



Introduction
History shows that conspiracy beliefs often thrive in crises (van Prooijen & van Vugt, Reference van Prooijen and van Vugt2018). Fake information now spreads (digitally) faster and further than ever before (Ahmed, Vidal-Alaball, Downing, & Seguí, Reference Ahmed, Vidal-Alaball, Downing and Seguí2020). Beliefs in conspiracy theories (CTs) are commonly also referred to as conspiracy beliefs and can be understood as beliefs concerning patterns of causal connections involving intentional actions of conspirators acting in a group and secretly collaborating towards a harmful or deceptive goal (van Prooijen & van Vugt, Reference van Prooijen and van Vugt2018). As governments implement unprecedented measures affecting almost all aspects of life to contain the coronavirus disease 2019 (COVID-19) pandemic, conspiracy beliefs regarding the coronavirus – which mainly target the severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) – may arise even in people who would not normally endorse CTs. Consequently, both endorsement rates and negative consequences of coronavirus CTs – for example, less infection-conscious behaviors (Allington, Duffy, Wessely, Dhavan, & Rubin, Reference Allington, Duffy, Wessely, Dhavan and Rubin2020), more precautionary behaviors such as hoarding (Imhoff & Lamberty, Reference Imhoff and Lamberty2020), and inter-ethnic hostility (Schild et al., Reference Schild, Ling, Blackburn, Stringhini, Zhang and Zannettou2020) – may exceed negative outcomes of former CTs. It is therefore important to determine the endorsement rates of coronavirus-related conspiracy beliefs and the psychological risk factors underlying these beliefs to support policy makers in fostering guideline-observing behaviors (Freeman et al., Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b; Georgiou, Delfabbro, & Balzan, Reference Georgiou, Delfabbro and Balzan2020; Van Bavel et al., Reference Van Bavel, Baicker, Boggio, Capraro, Cichocka, Cikara and Willer2020).
High rates of ‘common’ CTs were reported before the coronavirus outbreak, with around 20% of the general population believing in CTs such as a faked moon landing, for example (Mancosu, Vassallo, & Vezzoni, Reference Mancosu, Vassallo and Vezzoni2017). In times of corona, a recent study by Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b) showed that of a British general population sample, around 15% endorsed coronavirus-related conspiracy beliefs at least strongly, another 25% agreed with them to some degree. This included both beliefs involving a broad, unspecific definition of actors or the conspirational goal (denoted as ‘general conspiracy beliefs’), as well as beliefs involving a specific conception of conspirators, a hidden goal or the measures taken to mislead others (denoted as ‘specific conspiracy beliefs’). In a related study, 28% of participants in a UK sample agreed with any coronavirus-related CT (Allington et al., Reference Allington, Duffy, Wessely, Dhavan and Rubin2020). Similar rates have been reported for the belief of a manufactured virus across countries (Roozenbeek et al., Reference Roozenbeek, Schneider, Dryhurst, Kerr, Freeman, Recchia and van der Linden2020). Similarly, one in three participants in a US-based survey believed that the coronavirus was created and spread intentionally (Uscinski et al., Reference Uscinski, Enders, Klofstad, Seelig, Funchion, Everett and Murthi2020).
Although beliefs in CTs are not a new phenomenon, psychological research has only relatively recently started investigating associated cognitive factors that may be linked to the occurrence of conspiracy beliefs. For example, greater endorsement of CTs has been observed in people who engage in less analytical and more intuitive reasoning modes (Barron et al., Reference Barron, Furnham, Weis, Morgan, Towell and Swami2018; Georgiou, Delfabbro, & Balzan, Reference Georgiou, Delfabbro and Balzan2019; Lantian, Bagneux, Delouvée, & Gauvrit, Reference Lantian, Bagneux, Delouvée and Gauvrit2021; Swami, Voracek, Stieger, Tran, & Furnham, Reference Swami, Voracek, Stieger, Tran and Furnham2014). Reasoning biases observed in delusions, which are distinct yet related phenomena, may also be relevant (e.g. Bronstein, Everaert, Castro, Joormann, & Cannon, Reference Bronstein, Everaert, Castro, Joormann and Cannon2019). While delusions involve a narrower definition of counterparties and are more personally targeted, what they share with CTs is combining seemingly unrelated phenomena into meaningful patterns even if there are none.
Delusion-associated biases such as jumping-to-conclusions (JTC bias; e.g. Dudley & Over, Reference Dudley and Over2003), liberal acceptance (LA bias, a lowered decision threshold; Moritz & Woodward, Reference Moritz and Woodward2004), bias against disconfirmatory evidence (BADE; Woodward, Buchy, Moritz, & Liotti, Reference Woodward, Buchy, Moritz and Liotti2007) and an excessive confidence in a belief with no ‘possibility of being mistaken’ (PM; Garety et al., Reference Garety, Freeman, Jolley, Bebbington, Kuipers, Dunn and Dudley2005; So et al., Reference So, Freeman, Dunn, Kapur, Kuipers, Bebbington and Garety2012) might be also associated with the endorsement of coronavirus-related CTs. To our knowledge, only two studies have investigated the association between reasoning biases and CTs and found that a more pronounced JTC is associated with more conspiracy beliefs (Moulding et al., Reference Moulding, Nix-Carnell, Schnabel, Nedeljkovic, Burnside, Lentini and Mehzabin2016; Pytlik, Soll, & Mehl, Reference Pytlik, Soll and Mehl2020). However, no study has yet tested the association between various reasoning biases and beliefs in CTs in a representative general population sample.
Aims of this study
Beliefs in coronavirus-related CTs are likely to result in less pandemic containment-focused behaviors. It is therefore important to provide estimates of the occurrence of such beliefs and to examine putative associated factors, such as reasoning biases, to attenuate CT-related negative outcomes. First endorsement rate estimates of coronavirus-related CTs have been provided, mostly for English-speaking countries (e.g. Freeman et al. Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b; Georgiou et al. Reference Georgiou, Delfabbro and Balzan2020). While common CTs seem less endorsed in German-speaking countries than in other Western countries, it is unknown if this extends to coronavirus CTs (Bruder, Haffke, Neave, Nouripanah, & Imhoff, Reference Bruder, Haffke, Neave, Nouripanah and Imhoff2013).
We aimed to estimate endorsement rates of existing coronavirus-related CTs in a German-speaking representative general population sample (Aim 1) and test whether reasoning biases and paranoia are associated with coronavirus-related CT beliefs (Aim 2). Regarding Aim 2, we hypothesized that endorsement of general and specific coronavirus conspiracy beliefs is associated with a greater jumping-to-conclusions bias (JTC; Hypothesis 1ab), a greater bias against disconfirmatory evidence (BADE; Hypothesis 2ab), a lower self-stated possibility to being mistaken (PM; Hypothesis 3ab), a greater liberal acceptance bias (LA; Hypothesis 4ab), and greater paranoid ideation (Hypothesis 5ab) (Aim 2). In subsidiary analyses, we expect that stronger endorsement of coronavirus-related conspiracy beliefs is associated with younger ages (Swami, Reference Swami2012) and lower levels of education (van Prooijen, Reference van Prooijen2017).
Methods
Participants
Participants were recruited via Respondi, an ISO-certified recruitment panel facilitating assessment of highly motivated participants via a double-opt-in registration process, fair incentives, and regular quality monitoring. Respondents were recruited via online campaigns of Respondi's panels. We aimed to collect data within a maximum of two weeks and a minimum of three days to also assess less-than-daily users of online services.
Inclusion criteria were an age of 18–69 years (due to platform characteristics), informed consent, permanent residency in Germany or the German-speaking part of Switzerland, and good proficiency in the German language. No further inclusion criteria were specified in order to obtain a rather representative general population sample. Participants who had responded to all questions uniformly were excluded.
We employed a non-probability quota sampling for both countries. Recruitment was conducted with regard to quota for gender and age groups for the German (Statistisches Bundesamt, 2020a, 2020b; women: 50.65%; of which 20.41% aged 18–29: 18.85% aged 30–39: 18.50% aged 40–49: 23.91% aged 50–59: 18.28% aged 60–69) and the Swiss (Bundesamt für Statistik, 2019; women: 49.63%; of which 21.01% aged 18–29: 20.72% aged 30–39: 20.54% aged 49–49: 21.86% aged 50–59: 15.88% aged 60–69) population of interest.
Procedure
This study was a cross-sectional online study performed using UniPark software (Questback GmbH). The study protocol was approved by the local ethics committee of the Department of Psychology, University of Basel. All assessments were completed in one web-based assessment: After providing basic demographic information, participants answered questions on their momentary perceived stress and their endorsement of general and specific coronavirus-related conspiracy beliefs. Reasoning biases and paranoid ideation were assessed through experimental paradigms and self-report items. Recruitment took place between 2 July 2020 and 7 July 2020, at a time when the first wave of COVID-19 infections had been overcome in both countries and a second wave had not started evolving yet.
Measures
We first assessed participants' demographic information and self-described political orientation to describe the sample profile in a way that it can be reasonably compared to other samples (e.g. Baier & Manzoni, Reference Baier and Manzoni2020; Freeman et al. Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b). Political orientation was assessed using one item (‘How would you rate your political orientation on the following spectrum?’) with a 7-point Likert scale ranging from 1 = ‘Left-wing’ to 7 = ‘Right-wing’.
General and specific coronavirus-related conspiracy beliefs
General and specific conspiracy beliefs targeting the coronavirus were assessed using items developed and used by Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b). The inventory comprises 30 items assessing endorsement of specific coronavirus-related conspiracy beliefs (e.g. ‘Coronavirus is a bioweapon developed by China to destroy the West’) and 18 items assessing endorsement of general coronavirus-related conspiracy beliefs (e.g. ‘The virus is a hoax’). The latter are subdivided into the sub-categories ‘skepticism about the government's response’ (3 items), ‘general conspiracy views about the cause of the virus’ (3 items), ‘general conspiracy views about the spread of the virus’ (7 items), and ‘general conspiracy views about the reasons for lockdown’ (5 items). All items were selected by Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b) to balance out political and religious influences. We added another specific conspiracy belief repeatedly stated on various media platforms (‘Bill Gates intends to use COVID-19 testing and a future vaccine to track people with microchips’). The items were translated into German via forward−backward translation (Supplemental Material).
All items in Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b) were answered using a 5-point-Likert scale. To obtain more fine-grained information, we applied a continuous scaling approach with a slider scale ranging from 0 to 100. The scale was labelled from left to right with the scale labels used in the original study: ‘do not agree’, ‘agree a little’, ‘agree moderately’, ‘agree a lot’, ‘agree completely’. The aim was to assess levels of degree of conviction in conspiracy beliefs in a manner clearly understandable by participants and easily interpretable (Freeman et al., Reference Freeman, Rosebrock, Petit, Causier, East, Jenner and Lambe2020a). The beliefs presented were extreme, with a simple, low cognitive load response option (‘do not agree’). Total scores of specific conspiracy beliefs and of general conspiracy beliefs were obtained by averaging all corresponding item scores (range for both total scores: 0–100). Cronbach's alpha for the general and specific belief subscales were excellent (α general = 0.97; α specific = 0.98).
Jumping-to-conclusions bias
The JTC bias was assessed with an established measure of JTC, the ‘fish task’ (e.g. Speechley, Whitman, & Woodward, Reference Speechley, Whitman and Woodward2010). Participants were shown two lakes containing orange and grey fish (lake A 80% orange : 20% grey fish; lake B reverse ratio). Ten fish were being successively caught and presented until participants were ready to decide from which lake the fish were being caught. Following each fish caught, participants were asked to indicate the probability with which the fish had been caught from Lake A or from Lake B (0–100%), and whether they had yet decided regarding the source of all the fish caught. All caught fish remained visible throughout the task to minimize demands on working memory. The JTC bias was measured by counting the number of ‘draws to decision’ (DTD; e.g. Andreou, Veckenstedt, Lüdtke, Bozikas, & Moritz, Reference Andreou, Veckenstedt, Lüdtke, Bozikas and Moritz2018; Moritz et al., Reference Moritz, Göritz, Balzan, Gawȩda, Kulagin and Andreou2017). If no final decision for either of the lakes had been made by the tenth catch, DTD was scored as 11. The higher the DTD score, the lower the JTC bias.
Liberal acceptance bias
A LA bias was assessed within the ‘fish task’ paradigm via the indicated probability (i.e. the ‘decision threshold’) upon making the final judgment. Consequently, the raw score for LA bias can range from 0 to 100, where a low score represents a greater LA bias in the form of a lowered decision threshold (e.g. Klein & Pinkham, Reference Klein and Pinkham2018; Moritz et al., Reference Moritz, Scheu, Andreou, Pfueller, Weisbrod and Roesch-Ely2016, Reference Moritz, Menon, Andersen, Woodward and Gallinat2018).
Bias against disconfirmatory evidence
BADE was assessed using the fictitious scenario task (e.g. Veckenstedt et al., Reference Veckenstedt, Randjbar, Vitzthum, Hottenrott, Woodward and Moritz2011), which is based upon the original BADE task (Eisenacher et al., Reference Eisenacher, Rausch, Mier, Fenske, Veckenstedt, Englisch and Zink2016; Woodward, Moritz, Cuttler, & Whitman, Reference Woodward, Moritz, Cuttler and Whitman2006). Participants were presented with initially ambiguous scenarios that became gradually disambiguated. Each trial began with an ambiguous statement, followed by two further statements providing disambiguating information. Four possible interpretations were given for each scenario (one true, one absurd, and two plausible lures). After each statement, the participant was asked to provide probability ratings for each of the four interpretations on an 11-step slider scale ranging from 0–100%. High scores corresponded to high confidence estimates. BADE was calculated by computing the mean change in confidence from sentence one to sentence three for the lure interpretations. In total, two randomly drawn scenarios (one with an emotional answer option, one with a neutral answer option as the true answer) were displayed. This decision was made in order to capture both an affectively charged and a neutrally charged outcome scenario, while minimizing study burden for participants. A total BADE score was obtained by averaging the BADE scores from both scenarios. A higher positive score represents a lower BADE; a higher negative score a higher BADE.
Possibility of being mistaken
Here, participants were presented with a random coronavirus-related belief and asked to rate the likelihood of being mistaken in their degree of endorsement of this particular belief. Participants used a slider scale ranging from 0 (=‘very unlikely’) to 100 (=‘very likely’). Several studies have used such a ‘one-item’ approach to operationalize PM (e.g. Dudley et al., Reference Dudley, Shaftoe, Cavanagh, Spencer, Ormrod, Turkington and Freeston2011; Jolley et al., Reference Jolley, Ferner, Bebbington, Garety, Dunn, Freeman and Kuipers2014; So et al., Reference So, Freeman, Dunn, Kapur, Kuipers, Bebbington and Garety2012).
Paranoid ideation
Paranoid ideation was assessed using the German version of the Paranoia Checklist (PCL; Lincoln, Peter, Schäfer, & Moritz, Reference Lincoln, Peter, Schäfer and Moritz2009; original by Freeman et al., Reference Freeman, Garety, Bebbington, Smith, Rollinson, Fowler and Dunn2005). The PCL contains 18 self-report items and is sensitive to dimensional non-clinical paranoia ideation in healthy individuals (Freeman et al., Reference Freeman, Garety, Bebbington, Smith, Rollinson, Fowler and Dunn2005). For each statement, participants rated how convinced they were it was true, using a 5-point Likert scale (1 = ‘not convinced at all’, 5 = ‘very convinced’). A total score for paranoid ideation was obtained by summing up all item scores.
Momentary perceived stress
For exploratory purposes and in order to control for potentially confounding effects regarding the assessment of both conspiracy related beliefs (Swami et al., Reference Swami, Furnham, Smyth, Weis, Lay and Clow2016) and reasoning biases (Moritz, Köther, Hartmann, & Lincoln, Reference Moritz, Köther, Hartmann and Lincoln2015), we assessed momentary subjective stress using a one-item scale (‘How stressed do you feel at the moment?’; e.g. Bollini, Walker, Hamann, & Kestler, Reference Bollini, Walker, Hamann and Kestler2004; Clamor, Koenig, Thayer, & Lincoln, Reference Clamor, Koenig, Thayer and Lincoln2016). A 10-point Likert scale was used (1 = ‘not at all stressed’, 10 = ‘extremely stressed’).
Analyses
Endorsement rates of conspiracy beliefs were computed descriptively. In order to estimate endorsement rates of single beliefs in a manner comparable to Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b), we post-hoc assigned raw values of the belief assessing slider scales to one of the five sections. Scores between 0 and 20 were assigned to ‘1’ (equaling ‘do not agree’), scores between 21 and 40 were assigned to ‘2’ (equaling ‘agree a little’), and so forth. We also calculated belief endorsement rates with ‘no degree of conviction at all’ (‘0’ scores). 95% confidence intervals of these endorsement rates were estimated using bootstrapping with 1000 samples. This procedure enables to draw comparisons, at least to some degree, with the endorsement rate estimates reported by Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b), while at the same time allowing to maintain a continuously scaled raw score for further analyses. To facilitate comparability, we computed Likert-based total scores per subscale by summing up Likert-scaled scores of corresponding items. We also calculated continuously scaled endorsements of single beliefs and belief subscales, always ranging from 0 to 100.
Addressing our hypotheses regarding the associations of conspiracy beliefs with reasoning biases and paranoia, we conducted multiple regression analyses to establish standardized and unstandardized regression coefficients. In each regression model, we controlled for demographic variables and momentary subjective stress, and for paranoid ideation in models for H1ab to H4ab. Exploratorily, we also tested whether quadratic relationships of these biases and conspiracy beliefs better explained the data at hand, as, for instance, CTs might be strongly endorsed both by individuals with low PM and individuals with high PM (who might think they may be misled by conspirators). Quadratic regression models each included a squared predictor. All hypotheses tests relied upon α = 0.05 and were performed using R (R Core Team, 2020). All data have been made publicly available and can be accessed via the Open Science Framework website (https://osf.io/qg89e/).
Results
In total, N = 1829 individuals were recruited, of which N = 1684 (92.07%; in the following denoted as ‘full sample’; N = 1130 German participants, N = 554 Swiss participants) individuals provided complete data. Of the excluded sample, most participants were excluded due to premature drop-out and two participants were dropped from analyses due to a uniform responding style across items. An overview of demographic information about the full sample is provided in Table 1. Quota of this group was consistent with population-based quota targets for age and gender by country.
Table 1. Demographic characteristics of the full sample

Note. N = 1684.
Endorsement rates of coronavirus-related conspiracy beliefs
Continuously scaled endorsement of beliefs
On average, conspiracy belief items were endorsed with rather low levels (M = 17.41, s.d. = 24.41, range: 0–100). Only 0.89% of participants did not endorse any conspiracy belief at all (i.e. M = 0.00). Similar results emerged when skepticism items were dropped (1.37% of participants with zero endorsement). Of all beliefs, conspiracy beliefs of skepticism (items sc2 and sc3) and those related to the cause of the virus (item c2) were endorsed with highest levels (Table 2). We found that endorsement of specific, but not of general, conspiracy beliefs differed slightly by country: Swiss participants indicated greater endorsement of specific conspiracy beliefs (MdnSwiss = 5.6, MdnGerman = 4.3; Table 3).
Table 2. Endorsements of coronavirus-related conspiracy beliefs
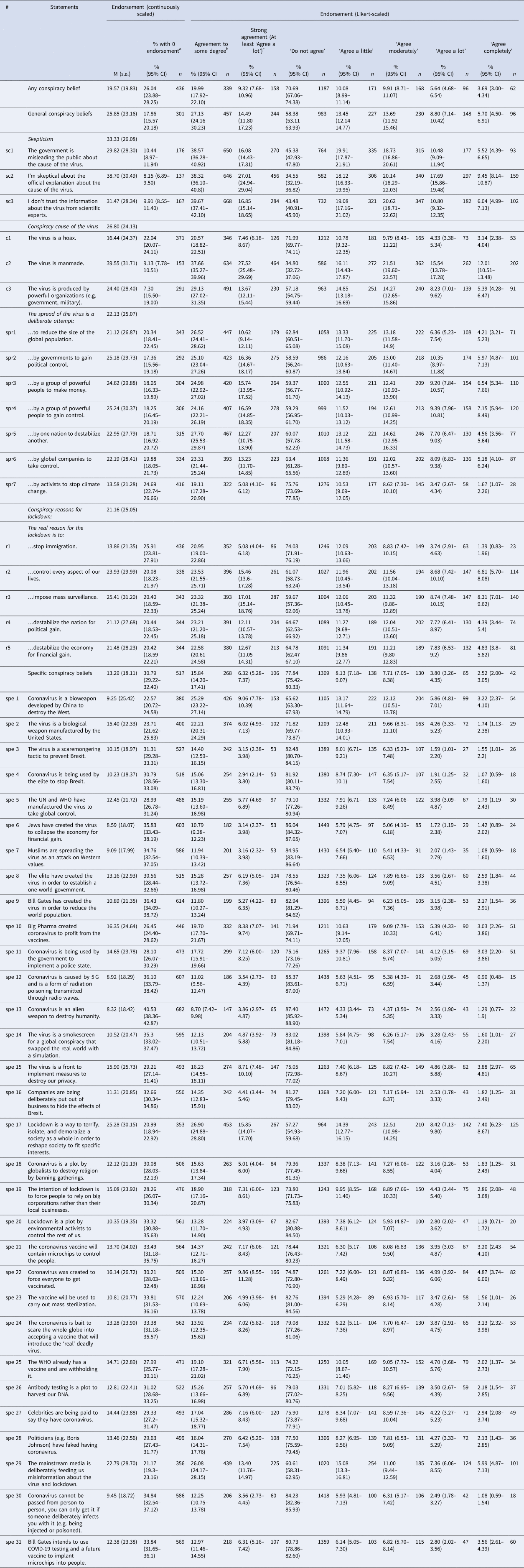
Note. All items reported here – except Item spe31 – were originally developed and published by Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b). Where scores which aggregate values from several columns are presented (e.g. percentage of ‘some degree’ endorsement), deviates from the estimated values of the unique columns are possible due to separate bootstrapping procedures. N = 1684.
a This denotes the percentage of participants who indicated a value of 0 of the respective slider scale.
b This rate was derived by summing up the rates of the third and fourth last columns, i.e. of the percentages of ‘Agree a little’ and ‘Agree moderately’.
c This rate was derived by summing up the rates of the two last columns, i.e. of the percentages of ‘Agree a lot’ and ‘Agree completely’.
Table 3. Differences in median endorsement of conspiracy belief categories and specific conspiracy beliefs, between Germany and Switzerland
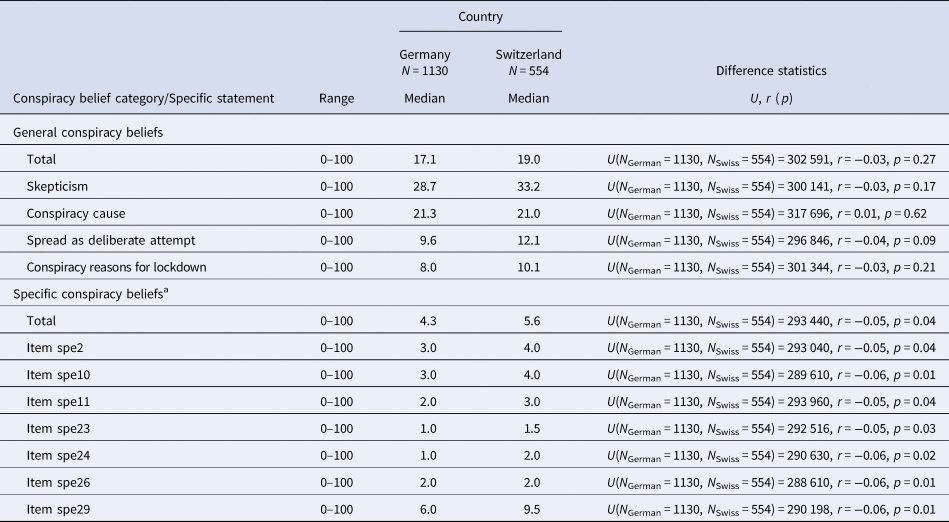
Note. Analyses were based upon continuously scaled endorsement (range 0–100). U refers to Mann−Whitney U test statistic.
a Only statements with significant differences (p < 0.05) in median endorsement between countries are presented here.
Likert-scaled endorsement of beliefs
The mean total specific conspiracy belief score for Likert-scaled endorsement was 44.96 (s.d. = 23.09), the mean total general conspiracy beliefs score for Likert-scaled endorsement was 34.20 (s.d. = 17.91). An average general and specific conspiracy belief was endorsed strongly (indicated by endorsement of at least ‘a lot’) by 14.49% (95% CI 11.80–17.23) and by 6.32% (95% CI 5.28–7.37), respectively (Table 2). Across both types of belief, 9.32% (95% CI 7.68–10.96) endorsed a conspiracy belief at least strongly. Another 19.99% (95% CI 17.92–22.10) endorsed a belief to some degree (indicated by endorsement of ‘a little’ or ‘moderately’). Similar percentages of Swiss [9.94% (95% CI 8.38–11.42)] and German [9.03% (95% CI 7.40–10.59)] participants endorsed any of the assessed conspiracy beliefs at least strongly.
Associations between conspiracy beliefs, demographics, and stress
As expected, we found evidence that both endorsement of general and of specific conspiracy beliefs was associated with younger ages [r s_gen (1682) = −0.07, p = 0.007; r s_spec(1682) = −0.10, p < 0.001] and lower levels of education [r s_gen(1682) = −0.21, p < 0.001; r s_spec (1682) = −0.18, p < 0.001]. Belief endorsement was not associated with gender [r s_gen(1682) = 0.01, p = 0.713; r s_spec (1682) = −0.00, p = 0.902], but with higher momentary stress [r s_gen(1682) = 0.16, p < 0.001; r s_spec (1682) = 0.19, p < 0.001]. Also, a tendency towards extreme political orientations predicted greater endorsement of both general [linear term: b = −36.26, t(1678) = −0.78, p = 0.433; quadratic term: b = 16.07, t(1678) = −2.70, p = 0.007] and specific [linear term: b = −77.34, t(1678) = −1.24, p = 0.315; quadratic term: b = 20.40, t(1678) = 2.55, p = 0.01] conspiracy beliefs in each regression model.
Associations between conspiracy beliefs, reasoning biases and paranoia
Confirming our hypotheses 1ab, 2b, 4ab and 5ab, a greater JTC bias (indicated by a lower DTD), a greater BADE (positive score indicating low BADE; only for specific beliefs), a greater LA bias (indicated by a lower decision threshold), and increased paranoia ideation predicted greater endorsements of general and specific coronavirus-related conspiracy beliefs in statistical models (Table 4). Hypotheses 2a and 3ab were not confirmed: results revealed that BADE did not predict endorsement of general coronavirus-related conspiracy beliefs and that a stated higher likelihood of being mistaken statistically predicted greater endorsements of general and specific conspiracy beliefs.
Table 4. Multiple regression analyses: Reasoning bias and paranoia outcomes predicting endorsement of general and specific conspiracy beliefs
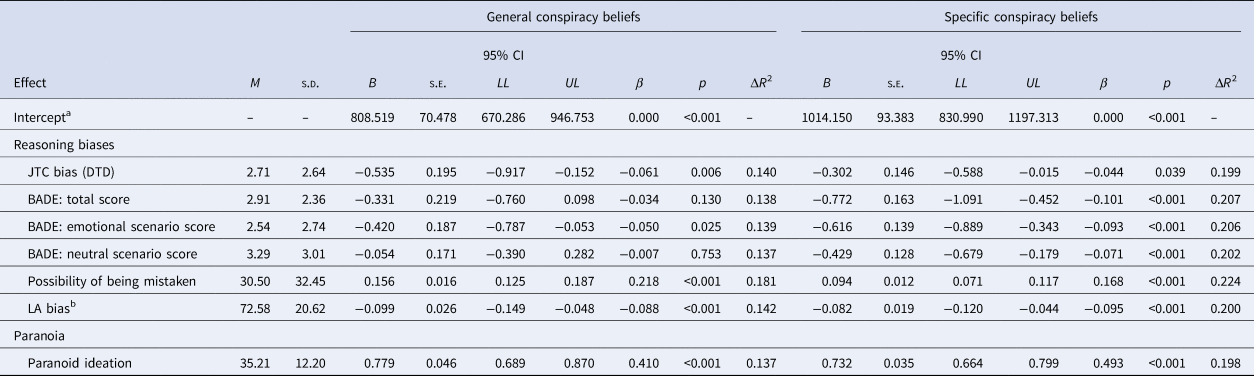
BADE, Bias against disconfirmatory evidence; CI, Confidence Interval; DTD, Draws to decision; JTC, Jumping-to-conclusions; LA, Liberal acceptance; LL, Lower limit (2.5%percentile); UL, Upper limit (97.5%percentile).
Note. For value ranges of reasoning biases, please see Method section. The change in R 2 represents the difference in R 2 between the corresponding multiple regression model (containing all control variables and the predictor of interest) and a reference regression model (containing only control variables). B refers to the unstandardized regression coefficient. β refers to the standardized regression coefficient. N = 1684.
a For reasons of parsimony, only intercepts for models involving JTC bias (DTD) as predictor are reported here.
b N = 1603, as participants who made no decision until the end of the fish task did not indicate a decision threshold and hence cause missing data.
To allow for other potential trajectories, we conducted exploratory investigations of quadratic associations for each hypothesis by adding the squared statistical predictor to regression models. Quadratic models improved model fit of each model significantly, and within each model, quadratic terms were significant predictors of the corresponding outcome (see Supplementary Materials). For example, both the linear [b = −3.65, t(1675) = −5.21, p < 0.001] and the quadratic term of DTD [b = 0.30, t(1675) = 4.63, p < 0.001] significantly predicted total endorsement of general conspiracy beliefs in the statistical model (the same pattern was observed for specific conspiracy beliefs). This means, for example, that individuals with very few DTD and individuals with many DTD endorsed these beliefs most strongly. Similarly, a negative linear term [b = −1.85, t(1675) = −3.78, p < 0.001] and a positive quadratic term [b = 0.24, t(1675) = 3.46, p < 0.001] of BADE predicted total endorsement of general conspiracy beliefs in our statistical model (again, the same pattern was observed for specific beliefs).
Discussion
The results of this study provide an extension of earlier studies, implying that a noticeable proportion of the German and Swiss German-speaking population endorse coronavirus-related conspiracy beliefs strongly or at least to some degree. Using self-report and experimental paradigms, we demonstrated that endorsement of these beliefs was associated with paranoid ideation and reasoning biases, the latter even when controlling for paranoid ideation. Our study contributes to a rapidly emerging body of literature acknowledging the relevance of such beliefs in the context of mental health (Chen et al., Reference Chen, Zhang, Jahanshahi, Alvarez-Risco, Dai, Li and Ibarra2020), pandemic-containing behaviors (Bertin, Nera, & Delouvée, Reference Bertin, Nera and Delouvée2020) and sociopolitical attitudes (Jutzi, Willardt, Schmid, & Jonas, Reference Jutzi, Willardt, Schmid and Jonas2020).
Compared to the British study by Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b), we observed a smaller percentage of participants with strong or absolute endorsements, which seems reasonable given the timing of our study. However, overall endorsement on a continuum scale was similar to that found by Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b), indicating that our participants more frequently endorsed conspiracy beliefs with moderate degrees. It should be noted, however, that endorsement rates observed in the two studies cannot be directly compared, as differences may have partly arisen from different scaling approaches, culture-specific factors, and different sample characteristics. Swiss participants endorsed specific beliefs only slightly more strongly than German participants, as indicated by small effect sizes. A part of these beliefs referred to the purpose and spread of vaccines, aligning with evidence that vaccination acceptance may be lower in Switzerland than in Germany (McAndrew, Reference McAndrew2020) and that, generally, generic conspiracy beliefs are endorsed less in Germany compared to other Western countries (Bruder et al., Reference Bruder, Haffke, Neave, Nouripanah and Imhoff2013). Corroborating prior studies, we observed that participants endorsing coronavirus-related conspiracy beliefs tended to be younger (Allington et al., Reference Allington, Duffy, Wessely, Dhavan and Rubin2020), less well educated (van Prooijen, Reference van Prooijen2017), politically more extreme (Krouwel, Kutiyski, van Prooijen, Martinsson, & Markstedt, Reference Krouwel, Kutiyski, van Prooijen, Martinsson and Markstedt2017), and more stressed (Swami et al., Reference Swami, Furnham, Smyth, Weis, Lay and Clow2016), while no gender differences emerged (Freeman et al., Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b).
Our hypotheses that reasoning aberrations and paranoia are associated with coronavirus-related conspiracy beliefs were largely supported. People endorsing such beliefs tend to collect less information before making a decision (JTC bias), make judgments with low-to-moderate certainty (LA bias), and adhere more to an already held specific belief, even if this turns out to be invalid (BADE) compared to people who endorse these beliefs to a lesser degree. Regarding JTC, our findings align with novel evidence suggesting that COVID-19 conspiracy beliefs are endorsed more strongly by people who are more impulsive (Alper, Bayrak, & Yilmaz, Reference Alper, Bayrak and Yilmaz2020), lending support to the assumption that a hasty reasoning process may be involved in the formation of such beliefs. Although effect sizes for reasoning biases were fairly small, reasoning aberrations may still represent a factor worth considering when investigating CT beliefs, especially since they may impact particularly on the persistence of beliefs (Freeman, Reference Freeman2016). Our results also imply that coronavirus-related CT beliefs may be an outgrowth of paranoid ideation and/or that paranoia and CT beliefs may favor each other (Darwin, Neave, & Holmes, Reference Darwin, Neave and Holmes2011). Further investigations to substantiate these relationships, particularly longitudinal studies, are needed.
Contrary to expectations, we found that BADE was not associated with endorsement of general beliefs, and that people endorsing conspiracy beliefs claim that they may be more likely mistaken in their beliefs (PM). While the latter finding seems somewhat surprising, it may reflect that individuals endorsing conspiracy beliefs consider themselves more prone to be deceived by conspiring parties in the details of the conspiracy, although not in the conspiracy itself. Alternatively, it seems also logical that particularly people who strongly reject such beliefs and defend official information consider themselves to be ‘right’ in their convictions. With respect to the BADE finding, it may be speculated that associations with conspiracy beliefs only arise if the disconfirmatory evidence is affectively charged and elicits emotional involvement, as is often the case in real life. Given that more research substantiates the associations reported here, public communication strategies targeting COVID-19-related CTs might consider addressing these biases and, rather than merely provide CT-contradictory information, raise awareness of reasoning styles and focus on other CT-relevant factors (e.g. transparent dissemination of virus-related information on social media; Allington et al., Reference Allington, Duffy, Wessely, Dhavan and Rubin2020).
Furthermore, our study implies that the relationship between reasoning biases and coronavirus-related conspiracy beliefs may be best described by non-linear relationships. It can, for example, be surmised that there is a subgroup of CT-believers who tend to oversample information until they have reached a medium-certainty threshold to satisfy a need of competence. There may also be a group of CT-endorsing individuals who successfully discard their invalid beliefs, but only based on information from official sources. This would align with findings that people endorsing coronavirus conspiracy beliefs mainly rely upon subjective, unregulated sources (Allington et al., Reference Allington, Duffy, Wessely, Dhavan and Rubin2020). Considering that CTs and delusions are related, these results also prompt the question whether the relationship between reasoning biases such as JTC or BADE and delusions might be better described by polynomial trajectories. This could partially explain the heterogeneous findings of the role of JTC in delusions.
Recent studies suggest that JTC may in fact be less pronounced in delusion-prone individuals (as opposed to healthy individuals; McLean, Balzan, & Mattiske, Reference McLean, Balzan and Mattiske2020a; McLean, Mattiske, & Balzan, Reference McLean, Mattiske and Balzan2020b) and question whether psychotic patients and healthy individuals differ as largely as previously assumed regarding JTC bias (Moritz et al., Reference Moritz, Scheunemann, Lüdtke, Westermann, Pfuhl, Balzan and Andreou2020; Pytlik et al., Reference Pytlik, Soll and Mehl2020). Our non-linear findings reconcile these results with seemingly contradictory results on the presence of JTC bias in strong convictions, and imply that there may be both a subgroup of highly convinced individuals with a pronounced JTC bias and a subgroup of equally strong convinced individuals gathering more as opposed to less information than healthy individuals. Null differences reported by recent studies may hence be partially founded in a non-linear association of JTC bias and delusions. Regarding a mechanism for the oversampling subgroup, it could be that these individuals' data gathering style is strongly driven by anxiety (e.g. McLean et al., Reference McLean, Balzan and Mattiske2020a), a factor which has been linked to higher endorsement of CT (Sallam et al., Reference Sallam, Dababseh, Yaseen, Al-Haidar, Ababneh, Bakri and Mahafzah2020) and delusions (Garety et al., Reference Garety, Freeman, Jolley, Bebbington, Kuipers, Dunn and Dudley2005). Further evidence supporting this hypothesis remains outstanding.
Our study has the following limitations: First, our cross-sectional design forbids drawing causal inferences on the relationship between reasoning biases or paranoia and conspiracy beliefs; we have investigated reasoning biases as correlates rather than (causal) risk factors (Kraemer et al., Reference Kraemer, Kazdin, Offord, Kessler, Jensen and Kupfer1997). Second, concerning our sample, we cannot eliminate the possibility of any type of selection bias (e.g. individuals with no online access or with profound conspiracy beliefs not being contacted or dropping out). While a majority of the general population is regularly online (Bundesamt für Statistik, 2020; DeStatis, 2020), it remains possible that not all targeted individuals had the same chance to participate (non-probability sampling), and, given our quota sampling for two characteristics only, the representativeness of findings is limited. Third, post-hoc assignment of continuously assessed scores to Likert-scaled categories may have yielded slightly different results from other studies using ordinal scales from the outset. We still believe that this approach was mostly valid, as we aimed to address links to reasoning biases as concisely as possible while attempting to compare our results to the methodologically related study by Freeman et al. (Reference Freeman, Waite, Rosebrock, Petit, Causier, East and Lambe2020b). Further, our study can only make a statement about the level of agreement, not of disagreement with the presented beliefs. As it was our rationale to quantify endorsement for these beliefs and participants had the possibility to choose a low and no-endorsement answer option, we consider this a valid format to address our aim. Also, we did not specifically assess COVID-19 (SARS-CoV-2) conspiracy beliefs, but coronavirus-related beliefs. However, we consider it highly likely that most people answered these items against the background of the current COVID-19 virus. Lastly, we did not assess data for individuals aged older than 69 years, thereby limiting the generalizability of results.
In conclusion, this study provides initial estimates of coronavirus-related CT belief endorsement within a demographically quota-representative and cross-national sample of two German-speaking countries. Although only a rather small proportion of the population strongly endorses coronavirus-related conspiracy beliefs, negative behavioral consequences of these beliefs necessitate the identification of putative risk factors such as reasoning biases. We presented first evidence that distinct reasoning biases relate to coronavirus-related CT beliefs and may be (non-linearly) associated with these beliefs, opening new avenues for empirical research into delusion and related areas. We also hope that this study paves the way for future investigations into cognitive and emotional risk factors promoting COVID-19-related CT beliefs and CT endorsement in general. If additional studies corroborate the specific role of reasoning biases in such beliefs, strategies addressing the modification of these biases may be formulated to prevent strong conspiracy beliefs from arising in the first place.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291721001124.
Acknowledgements
The authors would like to thank Ruth Veckenstedt for her support in providing study-relevant material, Ursula Drew for her support in the translation process of the conspiracy-belief items and editing, and Sarah Ulrich as well as Gregory Elbel for their support in study implementation and constructive discussions during the conceptualization period.
Financial support
This research received no specific grant from any funding agency, neither from commercial nor from non-profit sectors. This study was financially supported by the Division of Clinical Psychology and Epidemiology (Head: Prof. Dr Roselind Lieb), Faculty of Psychology, University of Basel.
SK and TZS are supported by an SNF Ambizione Grant (Grant No. 179897 awarded to Dr Thea Zander-Schellenberg).
Conflicts of interest
None.







 Open access
Open access