



This review aims to emphasise the impact of poor nutrition on children’s health and psychological well-being, urging those involved in childhood obesity or nutrition services to broaden their intervention approach. A range of evidence is presented which reviews: The importance of childhood nutrition; Childhood obesity and nutrition; The impact of obesity on psychological, psychosocial health and eating behaviour; A mention of mental health-psychiatric diagnosis; Empowering Voices: Children and Young People Living with Obesity; Childhood Obesity Interventions, and finally, a Conclusion which offers a summary of the key issues and calls for health professionals to consider various psychological factors relevant to supporting optimal child nutrition and obesity.
The importance of childhood nutrition
Childhood nutrition plays a crucial role in a child’s growth, physical and cognitive development and overall well-being(Reference Nyaradi, Li and Hickling1). Healthy eating patterns support disease prevention efforts by reducing the risks of nutritional deficiencies alongside the risks of developing obesity and other non-communicable diseases (such as certain cancers and metabolic disorders). UK evidence suggests that adherence to dietary guidelines during childhood is associated with better health outcomes (for example, improved cardiometabolic profile), suggesting that adopting a healthy diet has long-term benefits to child health(Reference Buckland, Taylor and Emmett2,Reference Ekbom and Marcus3) .
A healthy diet occurs when daily eating patterns include adequate nutrient and energy intake to meet individual energy needs. Optimal childhood nutrition provides ideal quantities of the essential nutrients and energy needed for physical growth and cognitive development. Nutrients such as proteins, vitamins, minerals and carbohydrates are essential for building strong bones, muscles and organs, particularly during rapid periods of growth(Reference Buttriss, Welch and Kearney4). Micronutrients like n-3 fatty acids, iron, iodine, zinc and B vitamins contribute to brain and cognitive development, memory and learning abilities(Reference Bourre5). Nutrient-rich diets positively influence cognitive function, concentration and academic performance(Reference Prangthip, Soe and Signar6).
However, evidence consistently shows that many children have suboptimal diets worldwide, resulting in limited adherence to national and international dietary guidelines(7–Reference Diethelm, Huybrechts and Moreno9). The WHO European Childhood Obesity Surveillance Initiative analysed over 132 489 diets of children across 23 European countries and reported that fewer than half (42·5 %) consumed fruit and less than a quarter (22·6 %) consumed fresh vegetables daily(Reference Williams, Buoncristiano and Nardone10). Similar findings have been reported in the UK, with data revealing poor compliance with the UK’s dietary recommendations(Reference Buckland, Northstone and Emmett11). Specifically, dietary analysis for implementation of child dietary recommendations is notably very low or low for consumption of free sugars, fish, saturated fat and fibre, as well as for fruit, vegetables and salt. These dietary intakes are suboptimal, and neglecting good nutrition could lead to serious short-term adverse impacts on children’s growth, development and future long-term health. For example, inadequate zinc intake during childhood can lead to detrimental effects on attention and short-term memory(Reference Monk, Georgieff and Osterholm12). Inadequate iron intake leading to iron deficiency in childhood can negatively impact overall intelligence and cognitive development(Reference McCann, Perapoch Amado and Moore13); there is growing evidence regarding the prevalence of brain disorders such as Attention Deficit Hyperactivity Disorder and iron deficiency during early life(Reference Abbas and Valli14,Reference Georgieff15) . Insufficient vitamin D during childhood has been linked to the onset of various conditions, including rickets, multiple sclerosis(Reference Gianfrancesco, Stridh and Rhead16) and prediabetes(Reference Ekbom and Marcus3). Moreover, a diet containing high levels of saturated fat, refined carbohydrates and processed food products is associated with poorer mental health in children and adolescents(Reference O’Neil, Quirk and Housden17). Furthermore, there is a significant association between mental well-being and diet, with lower fruit and vegetable consumption in adolescents showing lower mental well-being(Reference Hayhoe, Rechel and Clark18).
In addition to these health risks, a poor diet increases the chance of developing childhood obesity(Reference Ng, Fleming and Obinson19). Healthy eating and good quality nutrition are promoted as key elements in the prevention of childhood obesity(Reference Koletzko, Fishbein and Lee20,Reference Verduci, Bronsky and Embleton21) . The European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition published a position paper on the role of diet and food habits on childhood obesity(Reference Verduci, Bronsky and Embleton21). This position paper summarises a range of dietary and eating behaviours that may support the prevention of obesity (including for example: breast-feeding; parenting styles; dietary patterns; eating behaviours; meal frequency, composition and portion size)(Reference Verduci, Bronsky and Embleton21). A similar position paper on this subject is written by the Global Federation of International Societies of Paediatric Gastroenterology, Hepatology and Nutrition (FISPGHAN)(Reference Koletzko, Fishbein and Lee20). Whilst there are clear nutritional guidelines and position statements aimed at promoting healthy eating and preventing obesity, it is concerning to observe that children globally and in the UK are not consistently following these recommendations; this presents significant future public health risks as these children transition into adulthood. Interventions to encourage nutritious diets and healthier eating habits to date have yielded varying levels of success.
Key learning point
Nutrient deficiencies and poor diets have consequences which include various psychological and cognitive challenges (to recap: having a negative impact on brain and cognitive development(Reference Bourre5), cognitive functioning, concentration, memory(Reference Prangthip, Soe and Signar6), attention(Reference Monk, Georgieff and Osterholm12), intelligence(Reference McCann, Perapoch Amado and Moore13), poor mental health(Reference O’Neil, Quirk and Housden17) and lower mental well-being(Reference Hayhoe, Rechel and Clark18), links to Attention Deficit Hyperactivity Disorder(Reference Abbas and Valli14,Reference Georgieff15) and lower academic performance(Reference Prangthip, Soe and Signar6)). Hence, healthcare and public health professionals need to consider how they assess these psychological and cognitive needs, and how any challenges associated with such needs are integrated into population based or targeted interventions. The WHO(22) has recognised that healthy eating interventions, for example, in school settings, must go beyond measuring physical outcomes (i.e. diet) and include cognitive and academic outcomes as part of their evaluations. Despite ongoing efforts to promote healthy eating and prevent childhood obesity, the yearly increase in childhood obesity rates worldwide highlights the need for more effective strategies and interventions.
Childhood obesity
In 2015, 107·7 million children were living with obesity worldwide(23), and in 2018, the WHO reported that childhood obesity is one of the most serious challenges of the 21st century(24). Childhood obesity has profound and wide-ranging impacts on an individual’s health(Reference Pulgaron25). These effects can manifest both in the short term, have long-term implications into adulthood, and may significantly impact morbidity and mortality(Reference Simmonds, Llewellyn and Owen26–Reference Mirza, Yanovski, Mirza and Yanovski28). Specifically, children living with obesity are at higher risk of developing type 2 diabetes(Reference Hagman, Danielsson and Brandt29) and increased risk of developing cardiovascular diseases(Reference Baker, Olsen and Sorensen30) such as high blood pressure, high cholesterol levels and atherosclerosis later in life. Non-alcoholic fatty liver disease is more common in children living with obesity and can lead to inflammation and liver damage(Reference Marcus, Danielsson and Hagman31). Childhood obesity can affect bone development and increase the risk of fractures(Reference Lane, Butler and Poveda-Marina32). Excess weight places additional stress on the joints and may lead to osteoarthritis and musculoskeletal pain(Reference Antony, Jones and Venn33). Obesity can contribute to respiratory problems like asthma and sleep apnoea, further impacting a child’s overall health and quality of life(Reference Han, Lawlor and Kimm34). Oral morbidity is increased in children and adolescents with obesity. Conditions like gastroesophageal reflux disease and gallstones can be more common in children living with obesity(Reference Han, Lawlor and Kimm34). Childhood obesity also increases the risk for autoimmune diseases such as multiple sclerosis, Crohn’s disease, arthritis and type 1 diabetes(Reference Marcus, Danielsson and Hagman31). Obesity can disrupt hormonal balance, potentially leading to conditions like polycystic ovary syndrome in girls and may contribute to early puberty, which might carry additional physical and emotional challenges(Reference Han, Lawlor and Kimm34). Children living with obesity are more likely to become adults with obesity, further increasing the risk of chronic diseases, such as cancer(Reference Furer, Afek and Sommer35). The combination of obesity-related health issues can reduce life expectancy and overall quality of life.
Obesity and Nutrition: For those already living with overweight or obesity, promoting and supporting a healthy diet has been recommended as a priority(Reference Nishtar, Gluckman and Armstrong36). Specifically, for those living with obesity, dietary improvements such as reducing the consumption of energy-dense foods, processed foods and sugar drinks are among some of the modifiable behaviours recommended(Reference Baker, Farpour-Lambert and Nowicka37,Reference Appannah, Pot and Huang38) . Children living with obesity are reported to have low vitamin D(Reference Ekbom and Marcus3,Reference Alemzadeh, Kichler and Babar39,Reference Yanoff, Parikh and Spitalnik40) , low iron(Reference Nead, Halterman and Kaczorowski41,Reference McClung and Karl42) and various other deficiencies (and the impact of these deficiencies is described above).
Key learning point
In addition to the nutritional challenges facing the general population, children living with obesity are at much higher risk of current and future health issues. This should be considered with reference to the ‘double burden malnutrition’ phenomenon, defined by WHO as the ‘coexistence of under nutrition along with overweight, obesity or diet-related non-communicable disease’(43). Double burden malnutrition can exist at an individual, household or population level. Globally, children in low-income households are more likely to experience deficiencies of essential micronutrients (such as iron), alongside living with overweight and obesity. However, double burden malnutrition is more common in middle-income countries, experiencing rapid changes in economic circumstances and access to food(43). Promoting good nutrition and healthy eating habits must address all forms of malnutrition.
The impact of obesity on psychological, psychosocial health and eating behaviour
There is clear evidence highlighting the co-directional relationship between psychological well-being and childhood obesity(Reference Newson and Flint44). Children living with obesity are frequently exposed to psychological stress, such as stigmatisation, discrimination, teasing, bullying(Reference Ahmed, Hussein and Mohammed45,Reference Bacchini, Licenziati and Garrasi46) and other forms of social marginalisation. These and other psychological stresses expose children to additional emotional and physical impacts, such as reduced quality of life, lower self-esteem, lower self-worth, depressive symptoms, body dissatisfaction, functional impairment (for example, less agility, limited ability to engage in activities) adverse social functioning, social withdrawal, difficulties in forming and maintaining peer relationships(Reference Reilly and Kelly47,Reference Rankin, Matthews and Cobley48) , as well as difficulties communicating and lower academic achievement(Reference Thamotharan, Lange and Zale49,Reference Heshmat, Larijani and Pourabbasi50) , all of which may further affect their physical, psychosocial health, quality of life and well-being.
The impact of psychological factors on children living with obesity is highly variable. However, given the wide range of factors that could be impacted, further consideration, assessment and intervention should be integrated into childhood weight management and healthy eating interventions. For example, not all children living with obesity recognise their diagnosis or accept this as a negative view of their body image(Reference Newson, Povey and Casson51). However, negative body image can be evident for some children living with obesity. Cognitive factors such as self-identity, attitudes, beliefs and knowledge about obesity, food, nutrition and healthy behaviours can influence decisions, including food choice(Reference Newson, Povey and Casson51).
In a review of the link between stress and childhood obesity(Reference Wilson and Sato52), stress has been highlighted as a significant factor in contributing to and maintaining childhood obesity(Reference Hemmingsson53). Children living with obesity are more likely to experience stress at home, and daily stresses significantly impact their eating behaviours(Reference Debeuf, Verbeken and Van Beveren54). Food can be a coping mechanism for dealing with stress, anxiety or other negative emotions and can lead to a cycle where eating becomes associated with emotional coping. Stress can be defined as a ‘negative response that results from threatening stimuli, external events or conditions that adversely affect a person’s well-being’(Reference Wilson and Sato52) (for example, experiencing social discrimination, stigma, teasing or bullying for those living with obesity). Stress is considered in the context of chronic (ongoing prolonged) stress, and acute stress (brief stress), and its impact on childhood obesity risk. Stress can influence behaviour and affect psychological well-being; it can promote changes in sleep, cognition and perception of pain and may change biological responses such as endocrine, immune and metabolic functioning(Reference Christensen, Varney and Gupta55). The cause-and-effect debate regarding stress and obesity is still under investigation (as are many psychological variables), but stress and obesity are entwined. The Obesity Medicine Association (2022)(Reference Christensen, Varney and Gupta55) has produced a clinical practice statement which summarises the links between obesity, stress and psychiatric disease (focusing on adult literature). Which suggests that obesity and its negative health effects can heighten both physical and mental stress, potentially leading to unhealthy behavioural changes. These changes in biological functions, including the endocrine, immune and metabolic systems, contribute to a cycle of worsening obesity, a process known as an adiposopathic stress cycle(Reference Christensen, Varney and Gupta55) (i.e. ‘sick-fat’, see Bays et al.(Reference Bays56) for further information on this topic).
A possible link to the stress response is poor emotional regulation. In this context, the behaviours and actions of the child living with obesity are influenced by their emotions, how they experience these emotions and how they communicate them to others. Ineffective emotional regulation has been modelled to link stress and obesity, suggesting that stress and ineffective emotional regulation lead to unhealthy eating behaviours such as emotional eating and other maladaptive behaviours such as sleep difficulties or reduced physical activity(Reference Aparicio, Canals and Arija57). For example, adolescents who have higher levels of stress are more likely to engage in emotional eating(Reference Nguyen-Rodriguez, Chou and Unger58). Psychological factors can profoundly impact a child’s relationship with food, eating patterns and overall health. Additional emotional factors, such as boredom, sadness and happiness, can trigger eating behaviours(Reference Thaker, Osganian and deFerranti59). Children may turn to food for comfort or to cope with their emotions, which can lead to overeating or consuming unhealthy foods. Children living with obesity are reported to experience higher levels of emotional eating(Reference Wilson and Sato52). A clear summary of emotional-induced eating (emotional eating), dietary restraint, stress and eating behaviour and family, parental and environmental stress is identified as possible contributing factors to childhood obesity(Reference Wilson and Sato52).
There are biological (genetic/physiological) factors which are significantly associated with taste preferences and subsequent consumption of specific food types (for example, sweet, bitter and fat tastes(Reference Dioszegi, Llanaj and Adany60)). Children with higher BMI are reported to have bitter taste sensitivity, and girls may present with low sensitivity to sweet taste(Reference Rodrigues, Silverio and Costa61). Some of these biological mechanisms are apparent through the activation of various areas within the brain (including the frontal, parietal, occipital and temporal lobes, as well as the hypothalamus, thalamus, amygdala, hippocampus and ventral tegmental areas), all of which can be influenced and activated by specific foods, especially those rich in sugar, fat and salt(Reference Christensen, Varney and Gupta55). Activation of these areas in the brain, may directly impact eating behaviours, triggering cravings and initiating a cycle of seeking out specific foods for their pleasurable effects(Reference Christensen, Varney and Gupta55). For example, a cross-sectional study on adolescents living with obesity reported that nearly half (47·9 %) met a food addiction diagnosis(Reference Tas Torun, Icen and Gul62). Food addiction has been linked to impairment of the brain reward circuits(Reference Blum, Thanos and Gold63) and research into the field of obesity and food addiction in adolescents suggests that such occurrences increase the likelihood of adolescents reporting significant increased anxiety of gaining weight, dieting and thin body preoccupation(Reference Tas Torun, Icen and Gul62). Biological factors can change taste preferences and directly impact eating behaviour, and early experiences with food can also shape an individual’s food choice preferences(Reference Oliveira, Costa and Warkentin64). In addition, to biological, cognitive and psychological factors, eating patterns may also be influenced by social, environmental and cultural factors, such as group norms, peer pressure, parenting practices and the desire to fit in(Reference Newson, Povey and Casson51,Reference Russell and Russell65) . Children’s eating habits are influenced by their social circles, including family, friends, school teachers and peers. Psychological factors can play a role in forming and maintaining these habits, whether they are healthy or unhealthy.
Key learning point
Individual interventions to promote healthy eating or support weight management, in the case of those living with obesity, need to consider how they help children navigate all these possible influences. The underlying, complex and various biological mechanisms for the development (and maintenance) of childhood obesity need to be accounted for in future obesity prevention and treatment interventions. Understanding the interplay between various psychological factors and eating habits is essential for promoting healthy eating and achieving optimal weight management behaviours for those living with obesity. Strategies addressing emotional eating, promoting self-awareness and encouraging a positive relationship with food, which can contribute to more balanced eating habits.
A mention of mental health- psychiatric diagnosis
According to the Mental Health of Children and Young People in England survey(Reference Newlove-Delgado, Marcheselli and Williams66) in 2022, around 18 % of children aged 7–16 years had a probable mental health disorder leading to poor social and economic outcomes. These mental health diagnoses included clinical depression, clinical anxiety, eating disorders including binge eating and Attention Deficit Hyperactivity Disorder. The number of children seeking help for mental health concerns has risen in the UK. About 50 % of lifelong mental health issues start by age 14, making it crucial to explore the connection between childhood obesity and childhood mental health(Reference Hagell, Coleman and Brooks67). Negative experiences during childhood, such as abuse, parental stress, trauma and family discord, have been linked to behaviours that contribute to weight gain. The higher the exposure to psychological adversity, the greater the risk of developing obesity(Reference Hughes, Bellis and Hardcastle68).
Several reviews have evaluated research on the onset or co-morbidity of mental health and childhood obesity(Reference Rankin, Matthews and Cobley48,Reference Martin, Frisco and May69) . For example, a systematic review and meta-analysis evaluated data from 143 603 children and reported that the prevalence of clinical depression among children living with obesity was 10·4 %(Reference Sutaria, Devakumar and Yasuda70). The review suggested that children who perceive themselves as having obesity can develop negative body image, leading to depression. Moreover, the analysis found that females living with obesity had significantly higher odds of concurrent and future depression compared with females not living with obesity, but this finding was not the same for boys(Reference Sutaria, Devakumar and Yasuda70). In boys, the connection between body dissatisfaction and BMI is more complex; for example, boys may be more likely to underestimate their weight or not recognise obesity(Reference Martin, Frisco and May69). Another review evaluating the psychological consequences of childhood obesity(Reference Rankin, Matthews and Cobley48) highlighted that there is limited research that separates out gender and childhood obesity, but also that boys living with obesity are at higher risk of depression compared to boys of normal weight. The evidence for the direct association between clinical anxiety and childhood obesity is more uncertain, although children living with obesity are likely to be at increased risk of developing anxiety(Reference Rankin, Matthews and Cobley48).
There is further evidence to link obesity to co-morbidity of emotional and behavioural disorders (e.g. Attention Deficit Hyperactivity Disorder) and eating disorders. Adolescent girls living with obesity are more likely to engage in extreme weight-control behaviours, such as vomiting, using laxatives, fasting or other methods, which may lead to restrictive eating disorders(Reference Lebow, Sim and Kransdorf71).
The relationship between the cause and effect of childhood obesity and the various psychopathologies, however, remains inconclusive(Reference Rankin, Matthews and Cobley48). Evidence across this field can be contradictory, possibly due to analysing confounding variables differently, considering a variety of psychometric variables, or target populations (clinical v. community populations, overweight v. obese, etc.). It is noteworthy that mental health diagnosis or symptomology is not a given for those living with childhood obesity, and many children do not experience these issues.
Key learning point
It is important to understand and consider possible co-directional relationships between the mental health and psychological needs of children living with obesity(Reference Davies72). Given this varied evidence, prevalence, cause or consequence, children living with obesity should be assessed and monitored for mental health symptomology and screened for appropriate treatment (before, during and after any intervention for childhood obesity). If a child or adolescents meets pathway criteria for onwards referral to psychological support services, this should be supported. However, if an onwards referral is not made (for whatever reason), or the mental health challenges are not considered (prior to, or after onwards referral) at a level for psychological therapy, then those delivering weight management or nutrition interventions should remain aware of, and considerate of these individual psychosocial challenges.
Empowering voices: children and young people living with obesity
Despite the evidence that psychological challenges may impact children living with obesity, there is limited evidence regarding their reported experiences, perceptions and reflections on living with obesity and their emotional and psychological needs.
However, children and adolescents are insightful to their experiences of living with obesity and can offer valuable reflections on their experiences which we should learn from and integrate their opinions, experiences and needs back into our healthcare services and interventions. For example, in a UK study(Reference Curtis73), adolescents living with obesity reflected on their experiences of engaging in the national healthy school programme within their secondary school environment and how this general promotion of healthy eating to all school children reinforced their vulnerability to bullying, stigmatisation and social isolation within the school environment. It is important that strategies to engage in population-based health promotion activities, consider the impact (possibly negative) and prior to implementation, action is taken to mitigate possible negative impacts, in this case for those who may have difficulties engaging in healthy eating behaviours or who are living with obesity. Better still, it would be best practice to involve those living with obesity or experiencing challenges implementing healthy eating interventions, to be part of the co-design of any such population-based health promotion activities.
A recently published and significant study is the ACTION Teens global survey,(Reference Halford, Bereket and Bin-Abbas74) which evaluated various psychological factors and considered the lived experiences of adolescents living with obesity. Survey data were collected on 5275 adolescents living with obesity from 10 countries. The study reported that two-thirds of the adolescents living with obesity considered it comparable or more impactful than living with another serious health condition, such as cancer, heart disease, diabetes, depression and anxiety(Reference Halford, Bereket and Bin-Abbas74). Most of the adolescents perceived their weight as ‘above normal’, thus indicating they recognised their status as living with obesity; 85 % reported being worried about its impact on their health, and a significant number had attempted weight loss recently. Nearly half of adolescents indicated that their weight frequently or always caused unhappiness (44 %), and their body often or always made them feel insecure (37 %)(Reference Halford, Bereket and Bin-Abbas74). With reference to eating behaviour specifically, the adolescents acknowledged a lack of hunger control as the greatest difficulty in achieving weight loss, followed by a lack of motivation and enjoyment of unhealthy food as the most significant weight loss barriers. This study reported that over two-thirds of adolescents said they could lose weight if they ‘set their mind to it’ and that weight loss was entirely their responsibility. Finally, adolescents living with obesity defined successful weight loss as ‘feeling better about themselves’(Reference Halford, Bereket and Bin-Abbas74).
Adolescents living with obesity and attending weight management interventions have acknowledged the benefit of receiving support to improve their well-being and self-esteem and valued intervention input beyond focusing on weight-loss behaviours(Reference Morinder, Biguet and Mattsson75). Adolescents desire to lose weight has been motivated by a feeling of being proud and being normal, improving their social acceptance and activities, not wanting to be like other overweight people (especially family members), reflecting on past negative experiences and not wanting to experience bullying but to be happy(Reference Morinder, Biguet and Mattsson75). A qualitative systematic review(Reference Jones, Al-Khudairy and Melendez-Torres76) has summarised the perceptions and reflections of adolescents living with overweight or obesity attending lifestyle obesity treatment interventions, and one of the outcomes acknowledged that adolescents were greatly driven by the desire to enhance their body image and increase social desirability. This evidence explores adolescent’s experiences and highlights how psychological and emotional factors shape their perceptions, experiences and support needs while living with obesity. It also underscores the impact of these factors on their eating behaviours.
Younger children are also able to offer valuable insight into their experiences of living with obesity. A UK qualitative study(Reference Newson, Povey and Casson51) explored the beliefs and experiences of attending a multi-component family-based childhood obesity intervention. The analysis examined children’s (aged 5–15 years old) expectations of attending the weight management intervention and how this influenced subsequent behaviour (such as engagement in dietary change). Families who predicted that the intervention would have positive effects on their lives were more likely to attend, believing that it would help parents seek support from other parents, help children to make friends, improve their social relationships and self-confidence and facilitate the parents and children to gain new skills and knowledge. However, families who did not attend, emphasised their existing understanding of healthy eating and did not recognise the benefits of attending such a service. In comparison to the adolescents from the ACTION Teens global survey(Reference Halford, Bereket and Bin-Abbas74), in this study, the younger children and families made social comparisons to others with obesity, but primarily sought to downplay the severity of their obesity, and made social comparisons to distance themselves from other children living with obesity, and also compared obesity to more serious conditions, such as cancer.
Key learning point
This evidence highlights the importance of understanding the psychological perspectives and needs of those referred into a weight management intervention, and that healthcare professionals should help individuals acknowledge and reflect on their needs, that may include psychological changes (in addition to physical behaviour change, i.e. diet/ physical activity). Children and young people offer insight towards understanding the factors that influence their behaviours and decisions in attending, engaging and implementing the advice from weight management and healthy eating interventions. The psychosocial challenges and factors acknowledged from the young people are noteworthy, and they describe how these factors may or may not be addressed through the current interventions available.
Childhood obesity interventions
The current UK recommendations for children living with obesity are to attend a family-based multi-component weight management intervention(77). Multi-component refers to programmes that focus on a combination of behavioural outcomes such as achieving healthy eating, optimal nutrition, increased physical activity, reduction in sedentary behaviours and health outcomes such as reducing BMI or improving cardiovascular markers. The intervention may utilise a range of behaviour change techniques (BCT) aimed at impacting directly and indirectly (see mechanisms of action below) on these behavioural outcomes(Reference Michie, Richardson and Johnston78). A review(Reference Skinner, Staiano and Armstrong79) analysing 217 childhood obesity interventions found that most studies report weight change as the primary outcome. Despite offering a behavioural intervention, only half (48 %) of the studies reported behavioural outcomes, such as assessing changes to moderate-to-vigorous physical activity, reductions in television viewing and improvements in dietary intake(Reference Skinner, Staiano and Armstrong79). Notably, only 20 % of the studies systematically reported psychosocial outcomes, with the most common being quality of life, and only 5 % of the studies recorded mental health outcomes (such as depression)(Reference Skinner, Staiano and Armstrong79). Hence, psychological health (as outlined previously) is not typically the primary focus of childhood obesity, weight management or healthy eating interventions. However, self-esteem is included in UK National Institute of Health and Care Excellence (NICE)(77) clinical guidelines which recommends including self-esteem as a possible intervention outcome.
A more recent umbrella meta-analysis, reanalysed data from 26 other meta-analyses, and summarised the outcomes and various components of childhood obesity interventions(Reference Kobes, Kretschmer and Timmerman80). Across the studies, the components of the interventions were often categorised into different ‘types’ of support, such as diet-only, diet combined with physical activity, lifestyle-only, lifestyle combined with diet and diet combined with physical activity and sedentary behaviour. Typically, childhood obesity interventions tended to prioritise diet and physical activity, with the term ‘lifestyle’ encompassing other aspects. However, it can be argued that this approach does not adequately consider the psychological or emotional aspects of intervention types. Given the various psychological and emotional needs of children living with obesity (as previously described within this review), it is limiting that psychological components in the intervention design are rarely considered(Reference Kobes, Kretschmer and Timmerman80).
Numerous analyses and meta-analyses have assessed the effectiveness of childhood obesity interventions, but their success rates vary across studies(Reference Skinner, Staiano and Armstrong79,Reference Anderson and Ball81–Reference Oude Luttikhuis, Baur and Jansen83) . Evidence shows that participating in interventions promoting behaviour change outcomes, such as increased physical activity and good nutrition and implementing various BCT, is associated with improved psychological outcomes(Reference O’Neil, Quirk and Housden17,Reference Hayhoe, Rechel and Clark18) . This evidence appears to be echoed through some of the reflections given by children and adolescent’s perceptions of their lived experiences (See earlier considerations above). Furthermore, evidence suggests that participating in childhood obesity interventions may also improve psychosocial functioning(Reference Thomaseo Burton, Jones and Smith84). For example, attendance at weight management interventions for those living with obesity was found to reduce the prevalence and risk for eating disorder symptomology(Reference Jebeile, Gow and Baur85).
A systematic review(Reference Martin, Chater and Lorencatto86) of BCT (using an adapted CALO-RE BCT taxonomy(Reference Michie, Ashford and Sniehotta87)) assessed 9 childhood obesity weight management interventions and 8 obesity prevention interventions. Of the 9 childhood obesity management interventions, 6 were deemed effective in terms of achieving weight change and 4 out of 8 were effective for the preventative interventions Reference Martin, Chater and Lorencatto86 . The analysis of BCT utilised found that of the 41 BCT available, on average interventions used 7·5 BCT. Techniques commonly used in effective weight management interventions included: individual information; environmental restructure; role model; stress management; communication skills and practice. It is not known from the evidence base which BCT are effective, or which combination of BCT should or should not be included within a given intervention. However, it is noteworthy that there is limited focus on specific support to change psychosocial challenges, only two of the interventions reported using stress management/emotional control training and one reported using motivational interviewing as a specific BCT, though not effective. Whilst childhood obesity interventions focus on behaviour change outcomes, the consistency, application and effectiveness of using various techniques available is questionable in intervention design and implementation. Another review(Reference Matvienko-Sikar, Toomey and Delaney88), which focused on obesity prevention promoting feeding practices in children under 2 years of age, also reported the utilisation of BCT in the intervention implementation. This review found a limited number and range of BCT were adopted, and the review also questioned the theoretical underpinning and application of such theory in intervention delivery(Reference Matvienko-Sikar, Toomey and Delaney88).
If interventions do focus on behavioural outcomes and therefore apply behaviour change methods, understanding the concept of behaviour change and how BCT operate in such interventions is worth unpicking. BCT might include methods such as goal setting, problem-solving, knowledge and information or self-monitoring(Reference Michie, Richardson and Johnston78) and are directed towards a specific behavioural outcome, for example, achieving healthy eating. The BCT themselves are thought to directly impact the behavioural outcome (i.e. If a specific behaviour change technique (BCT), such as setting goals for dietary planning, is implemented, the intended behavioural change—in this case, dietary modification—will take place). However, given the varied success of interventions (which report implementing BCT), it is evident that the behavioural outcomes are not always achieved, or indeed may be achieved but are not sustained in the longer term.
BCT can also act on a behavioural outcome indirectly. This can be explained in terms of the BCT processes of change or mechanisms of action, which target predictors of behaviour (or determinants)(Reference Nielsen, Riddle and King89,Reference Michie, Thomas and Johnston90) . Determinants are psychological variables or regulatory processes that are causal antecedents of the target behaviour change and subsequently impact the behavioural or health outcomes(Reference Carey, Connell and Johnston91). In other words, the BCT may engage in a mechanism of action that triggers, enhances or engages various factors. It is here that BCT have the potential to influence psychological variables (such as some of those mentioned earlier, e.g. self-esteem, self-confidence). See example in Table 1.
Table 1 A simple illustration to understand mechanisms of behaviour change to impact on a behavioural outcome- dietary change (healthier eating)

*This is a very simple example, though an individual may be operating a number of mechanisms of action.
Although the contributing role of various psychosocial factors is known, there are few interventions which focus specifically on supporting the psychological needs of children living with obesity. However, some research has shown psychological approaches to be effective. For example, a multi-component intervention employed cognitive-behavioural techniques, together with nutrition education and the promotion of physical activity and demonstrated positive outcomes for children (aged 6–12 years old) living with obesity. These successful outcomes included BMI change, reduced energy intakes and improvements in lifestyle habits, emotional and social problems at 5 years follow-up(Reference Vignolo, Rossi and Bardazza92). Other interventions applying cognitive–behavioural /skill building techniques have also reported successful outcomes(Reference Boutelle, Kuckertz and Carlson93,Reference Moore, Borawski and Cuttler94) . UK Clinical guidelines, NICE(77,95) recommend using BCT, positive parenting skills, diet changes and physical activity routines. The intervention should be tailored to the need of the child and also include both the child and parents. NICE(95) acknowledges the role of BCT within interventions (such as self-monitoring, stimulus control and goal-setting) and calls for more evidence to explore the psychological interventions and methods, which may help improve outcomes for those attending weight management interventions. It is important to note that NICE recognises that adolescents living with obesity are more likely to experience emotional and behavioural problems, diminished quality of life and behaviours like binge eating compared to adolescents with a healthy weight(77,95) . However NICE guidance(95) does not provide healthcare professionals with specific instruction on how to recognise individual needs, or when or how to support their psychological, cognitive or emotional needs. Further NICE(95) suggests that consideration of psychological aspects is ‘beyond the scope’ of their guidance. It could be interpreted therefore that psychological needs of children living with obesity are considered beyond the scope of childhood obesity interventions, which would be a very narrow and limited view and may help explain the lack of inclusion and guidance for health professionals implementing psychological support into interventions.
To consolidate this evidence and establish a meaningful comprehension, we can utilise the behaviour science COM-B(Reference Michie, van Stralen and West96) (Capability, Opportunity, Motivation-Behaviour) model (as summarised in Table 2). This model allows us to dissect childhood obesity interventions, revealing potential gaps in achieving a personalised approach to treatment in not fully considering the psychological and emotional needs of children with obesity.
Table 2 An example of utilising the COM-B model(Reference Moore, Borawski and Cuttler94) to highlight weaknesses in current childhood obesity intervention, regarding lack of consideration for psychological and emotional support, embedded with the behaviour change mechanism of action
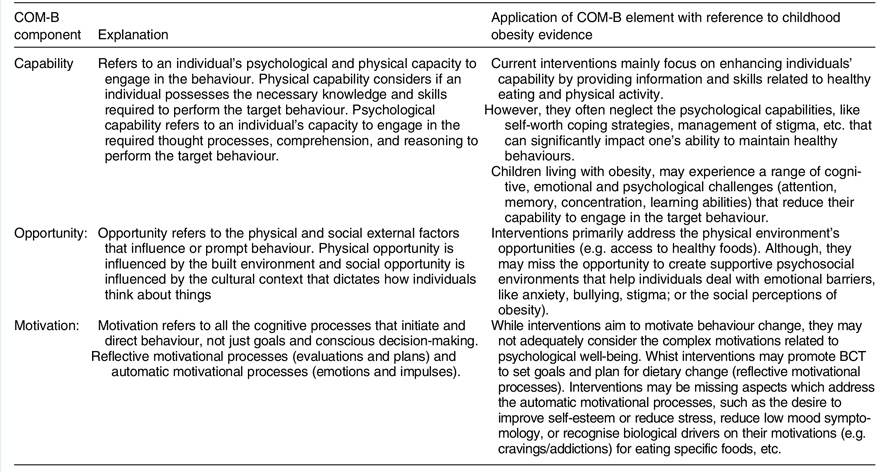
The COM-B model suggests that for a given behaviour to occur, an individual must have the capability and opportunity to engage in the behaviour, and the strength of motivation to engage in the behaviour must be greater than for any other competing behaviour(Reference Moore, Borawski and Cuttler94). Considering the psychological factors of childhood obesity becomes imperative in this context, as capability, opportunity and motivation play a crucial role in shaping behaviour and behaviour change for those living with obesity.
Conclusion
This review has highlighted various impacts of poor nutrition on clinical and psychological well-being. The impacts of childhood obesity on health and psychological well-being are also outlined. Significantly flagged by the WHO(43) is the double burden of malnutrition which is apparent, though little attention has been given to this in the childhood obesity literature(Reference Sahoo, Sahoo and Choudhury97).
Given the numerous and intricate health impacts linked to both the causes and consequences of obesity, it is crucial for health professionals to assess individual needs, inclusive of psychological and emotional needs and for the design and implementation of childhood obesity interventions to incorporate these varied needs. Childhood obesity interventions typically centre around BCT aimed at directly altering health behaviours, such as adopting a healthy diet. However, this approach may overlook the underlying mechanisms responsible for driving these behaviours and how these might be changed (see example described previously). Consequently, the success of adopting new behaviours tends to be limited and not sustained over time. BCT mechanisms of action operate indirectly, meaning that BCT should not only target the behavioural outcome itself but also engage these underlying mechanisms. For instance, it might involve addressing issues like low self-esteem, anxiety, low confidence or providing coping mechanisms to manage bullying. When addressing childhood obesity it is imperative that interventions address these psychological needs through the mechanisms of action. Unfortunately, this aspect is currently lacking in childhood obesity treatment interventions, and this is evident in the feedback from children and adolescents living with obesity in their reflections, evaluations and expectations of treatment interventions(Reference Newson, Povey and Casson51,Reference Halford, Bereket and Bin-Abbas74) .
Further research is required to explore the psychological and emotional mechanisms of action within the behaviour change interventions for treating and preventing obesity. It would be helpful to develop an assessment checklist or other resources to assist health professionals in considering the various health, psychological and cognitive needs of individual children living with obesity. However, in the absence of such tools, clinicians and other health professionals working within the field of childhood obesity, or indeed more broadly promoting health behaviours such as dietary change, should be mindful of these various causes and consequences of obesity, and therefore should evaluate their intervention offer, to ensure that it is personalised to meet the (changing) psychological and emotional needs of individuals, and thereby provide a comprehensive offer which may be more likely to change their health and lifestyle behaviours. Health professionals may find it helpful to utilise the COM-B model as an initial step to evaluate their intervention offer and consider if there are additional ways that they could tailor their intervention towards meeting individual needs.
It is important to note that the impact of psychological and psychosocial variables on a child or adolescent living with obesity can vary widely(Reference Jansen, Mensah and Clifford98). Some children living with obesity have no adverse psychological or psychological impairments. Others are significantly negatively affected with co-morbid mental health (e.g. depression, anxiety and eating disorders), whilst others are not. Some children and adolescents have lower self-esteem and confidence or experience higher levels of stress, stigma, bullying and teasing, with poor coping and communication skills, whilst others do not. Psychological factors, symptomology and mental health presentation, can change overtime(Reference Jansen, Mensah and Clifford98). There is a need to investigate and assess the individual needs and experiences of each child or adolescent living with obesity using objective measures. Once that assessment has explored these issues, an appropriate personalised intervention can be offered (recommendation to utilise a model such as COM-B to help assess and formulate an individual’s health behaviour change needs). However, assessment is not a one-time pre-intervention task. Children living with obesity should be monitored and supported as they engage in weight-management efforts, and consideration of their (changing) psychosocial and emotional needs should be part of the behaviour-change efforts, hence seeking to increase the likelihood of achieving the desired behavioural outcome (e.g. weight maintenance, healthier eating).
It is important to note that this review aims to encourage those working in the field of childhood obesity and nutrition to reconsider their intervention design and implementation when working directly with children and families seeking to improve their diet behaviour or engage in childhood obesity interventions. The review highlights various psychological and psychosocial factors that may be a cause or consequence of living with childhood obesity, though this review is not exhaustive and various other factors and mechanisms may be relevant. The review does not consider the wider context of childhood obesity, such as the obesogenic environment(99), including the environmental, economic, political and cultural factors that may also impact on the prevalence and indeed management of childhood obesity.
In summary, to enhance the effectiveness of obesity interventions, it is crucial to broaden the focus and include psychology fully into the design of childhood obesity interventions(100) and look beyond the physical behavioural outcomes as the only focus of the intervention. Those commissioning, designing and implementing childhood obesity interventions should therefore consider a more holistic approach that, considers the psychological and emotional needs, and incorporates the underlying mechanisms of action, which could lead to a more sustainable and effective treatment for childhood obesity.
Acknowledgements
The authors are thankful to the children and young people living with obesity (and their parents) who took part in online Patient and Public Involvement and Engagement discussions. These individuals from across the northwest and mid England played a key role in shaping the focus of Dr. Newson’s presentation at the Nutrition Society Conference (July 2023). Subsequently, in August 2023, follow-up online conversations with five young people living with obesity included feedback on the initial conference presentation, discussions about relevant research and agreeing key points for inclusion in this review. From their perspective, the aim of this review was to encourage other health professionals to understand why it is important to consider the psychological needs of children and young people living with obesity.
We would like to thank a number of academics who have engaged in research discussions relevant to this review: Dr Sides, Prof Pringle and Georgia Greenwood.
Financial support
No financial support was provided for this review.
Conflict of interest
There are no conflicts of interest.



 Open access
Open access