



Introduction
In October 2018, on the 40th anniversary of the Alma Ata Declaration, representatives from around the globe gathered in Astana, Kazakhstan to declare a renewed focus on primary health care (PHC) acknowledged in the Declaration of Astana (World Health Organization and United Nations Children’s Fund, 2018a). However, a mere 2 years later, the global COVID-19 pandemic exposed persistent and glaring gaps in global aspirations for well-integrated PHC (UHC2030 International Health Partnership, 2020).
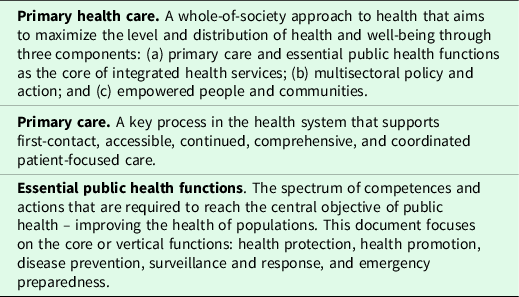
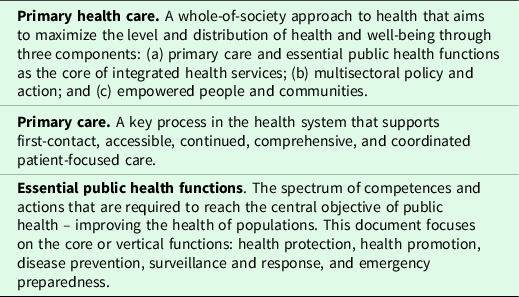
One of the commitments proclaimed in the Declaration of Astana is to ‘build sustainable primary health care’ which is further elaborated as enhancing ‘capacity and infrastructure for primary care (PC) – the first contact with health services – prioritizing essential public health functions’. The Declaration goes further stating, ‘We will benefit from sustainable PHC that enhances health systems’ resilience to prevent, detect and respond to infectious diseases and outbreaks’ (World Health Organization and United Nations Children’s Fund, 2018a). Hence, PHC includes both PC and essential public health (PH) functions (see Table 1) (World Health Organization, 2019). While much is written about the need to coordinate these two aspects, successful integration remains elusive in many countries (World Health Organization, 2018b; 2018c; 2019; Rechel, Reference Rechel2020).
Table 1. Definitions of primary health care, primary care, and essential public health functions according to the World Health Organization (World Health Organization, 2018b)
The World Health Organization Resolution on the PHC draft Operational Framework, approved by the World Health Organization Executive Board in January 2020 (World Health Organization, 2019), provides guidance on operationalizing the Astana commitments through strategic and operational levers. It encourages pursuit of ‘Models of care that promote high-quality, people-centred primary care and essential public health functions as the core of integrated health services throughout the course of life’ which seem vital to an effective pandemic response.
However, the intersection of PC and PH remains ill-defined and varies by setting (Rechel, Reference Rechel2020). In their Technical Series on PHC, the World Health Organization (WHO) outlines the benefits of coordinating PC and PH and identifies actions which could contribute to successful integration (World Health Organization, 2018c). The pandemic has provided an unexpected lens through which to gauge global readiness to take four key actions recognized as important for effective integration:
-
1) ‘Enabling primary care to deliver more protective, promotive, and preventive services to a defined population;
-
2) Improving communication and coordination between public health authorities and PC providers and managers;
-
3) Sharing knowledge and data to evaluate the impact of both individual- and population-focused services on health; and
-
4) Strengthening the surveillance function of primary care and more effectively linking this to public health surveillance’ (World Health Organization, 2018c).
This paper stems from a multi-national study on the perspectives of PC experts on their country’s response to the pandemic and aims to assess the degree to which PC and PH were integrated in national responses to the current coronavirus pandemic from the study’s free-text responses and learn from successes as well as failures.
Methods
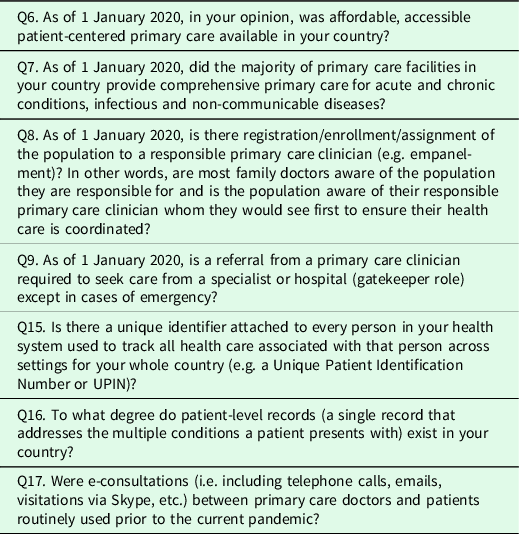
In an effort to better understand global PHC response to the pandemic, we conducted a survey from 15 April 2020 to 4 May 2020 using a convenience sample pulled from the World Organization of Family Doctors member network, WHO, and other global PHC organization contact lists. Respondents were encouraged to share the survey, so it is not clear how many total recipients received it. The 34-item survey assessed attributes of a strong PC system (see Table 2), national preparedness, and national response strategies to counter the COVID-19 pandemic. Further elaboration on survey methods, validation, and qualitative and quantitative analyses are presented in previously published papers (Goodyear-Smith, et al., Reference Goodyear-Smith, Kinder, Mannie, Strydom, Bazemore and Phillips2020, Reference Goodyear-Smith, Kinder, Eden, Strydom, Bazemore, Phillips, Taylor, George and Mannie2021).
Table 2. Attributes of primary care assessed in the PHC_COVID survey
Findings
A total of 1035 PC respondents (clinicians, researchers, policy-makers, and other global actors) from 111 countries completed the survey with good representation across all regions and economic levels (see Table 3). Participants’ text responses to open-ended questions in the survey were identified which underscored how each of the four key actions could have been strengthened in their country and are potential factors to why a strong PC system may not have guaranteed reduced mortality (Goodyear-Smith, et al., Reference Goodyear-Smith, Kinder, Mannie, Strydom, Bazemore and Phillips2020) (see Table 4).
Table 3. Summary table of count of respondents by country, World Bank economic tiers and World Health Organization region. Survey responses were captured between 15 April 2020 and 4 May 2020
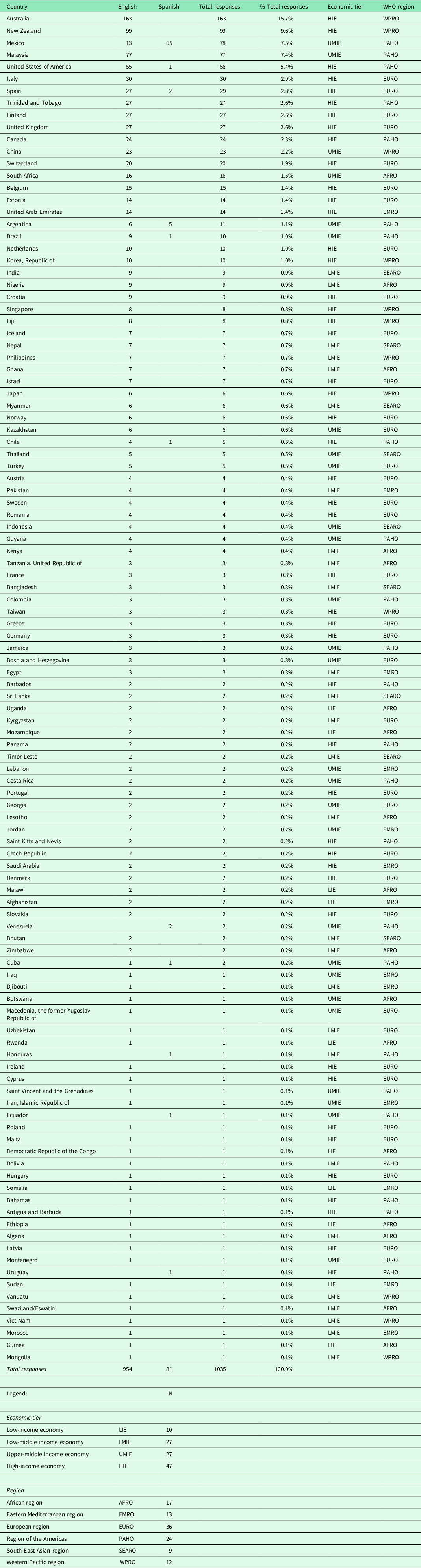
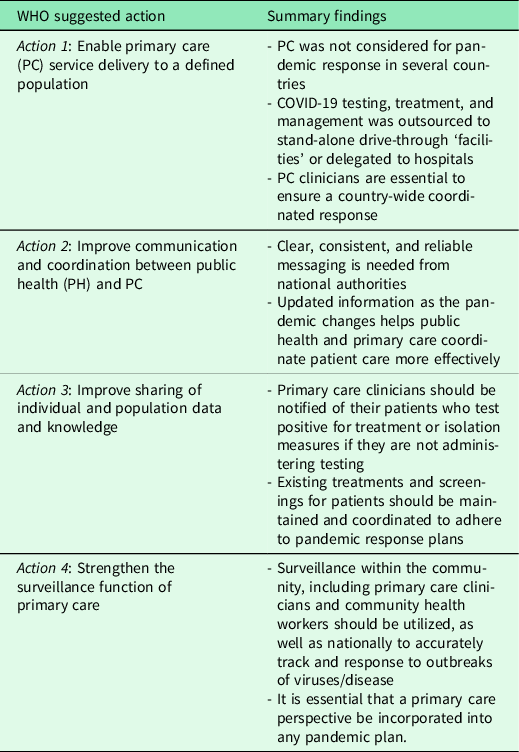
Table 4. Summary table of survey findings aligned with WHO suggested actions to integrate primary care and public health for pandemic response. Survey responses were captured between 15 April 2020 and 4 May 2020
Action 1: enable PC service delivery to a defined population
While good PC services may have been available, in some countries, these were not utilized or integrated. A respondent from Mexico wrote ‘A national response to COVID-19 has been focused on hospital services. PHC has not been taken into consideration’, and from Uzbekistan: ‘Our response is completely hospital/ER-centric. No one has talked about getting more testing and evaluation by the primary care sector’, The role of PC in triaging patients and only referring those in need of hospitalization can mitigate the overburdening of emergency and secondary care services.
Not all countries were perceived to have an existing and implemented pandemic plan. From Malaysia, one respondent mentioned ‘National guidelines for handling the COVID-19 needed to be formulated earlier’. Countries that had experienced previous pandemics were more prepared: ‘polyclinic doctors were well prepared and so were the 900 public health private GP clinics because Singapore had experience with SARs’.
Additionally, the degree to which PC was incorporated into the pandemic plan is unclear. We noted only a weak positive correlation (R = 0.1308) between respondents who thought a pandemic plan was utilized and believed their country had a strong PC system (Goodyear-Smith, et al., Reference Goodyear-Smith, Kinder, Mannie, Strydom, Bazemore and Phillips2020). The need to include PC clinicians in the crafting of such a plan was highlighted as critical to ensure a system-wide coordinated response. In addition, the disconnect between national- and state-level plans was evident in some federal health systems.
Action 2: improve communication and coordination between PH and PC
Absence of clear and consistent communication between national and local PH entities and the PC community was a theme clearly emergent in survey responses. Two Australian general practitioners noted ‘my information was received late in the overall evolution of the pandemic. Most … came through the media rather than reliable medical and infectious disease centres’ and ‘information was often passed on by word of mouth’. From a positive perspective, a respondent from Estonia conveyed ‘We organised a so-called committee of coronacrisis and the committee provided counselling and needed help for all family practices’ and in New Zealand ‘strong leadership jointly by the Prime Minister and by the Director-General of Health on medical & public health matters … [a] clear communication strategy’.
Several respondents identified poor communication from health authorities to health care delivery sites, such as a comment from an Indian respondent ‘Confusion in communicating whom we must see and whom we must not’, and a respondent from Germany stated, ‘The local administration with a crisis-committee is not aware of coordinating primary care services with hospitals’. Where there was insufficient governmental guidance ‘armchair experts filled the void of uncertainty’ which further added to the noise in Australia. A critical role of family doctors is to discern and dispel the plethora of false information, often promulgated through the internet, whether it be regarding the virus or under usual circumstances. As relayed from a respondent from Mexico ‘there is disinformation of the population spread x social networks’. One respondent from Trinidad and Tobago identified the importance of consistent communication, ‘Daily updates are given to the nation by the Ministries of Health, National Security, and Social Welfare’.
In a void of reliable information, clinicians were left to craft and convey clear messages to patients on the virus and self-care, a function built on the trust and relational continuity central to PC. This is particularly critical where a government response is missing or misguided. As conveyed by one Australian respondent, ‘We tried to do the right thing initially, moving chairs away from us, telling EVERYONE who came to see us how dangerous the virus was’. Another respondent noted ‘On the whole, the public’s response has been excellent but better and more timely information would have provided more trust between the public and politicians’.
Action 3: improve sharing of individual and population data and knowledge
The sharing of patient data and records between PC and PH is a long-standing touchpoint. When testing is conducted outside of PC practices, for example, at drive-through test centers, the test results must be communicated to PC clinicians. This enables the family doctor to follow up with the patient on treatment and isolation, as well as proactively assess the family’s situation and contact trace. It also ensures that non-COVID-19 PC services for patients and their families are maintained and coordinated (World Health Organization, 2019).
In many countries, the PH functions of testing, isolation, and tracing are not performed in PC facilities. In Hong Kong, ‘primary care is essentially private. Hospital care is government (public) and private. So initially no kits available for testing in private’. Many believed the lack of test kits exacerbated the problem with patients resorting to seeking care directly from hospitals. A Malaysian respondent identified PC testing as key, ‘if PC clinics do not screen, identify and isolate, COVID transmission will be out of control and increase exponentially’.
In some settings, integration of PC and PH may require additional training of PC staff in PH interventions, thereby expanding the comprehensiveness of the services PC clinicians are competent to deliver (World Health Organization; 2018b). Such a reorientation of PC to include a population health management approach, with a person-centered focus rather than an orientation toward diseases, can improve the health of an entire community (World Health Organization, 2018a; Rechel, Reference Rechel2020).
Action 4: strengthen the surveillance function of PC
In some countries, the role of PC in surveillance was emphasized. In India, it was noted that ‘the existing polio surveillance network and the chain of community health workers has definitely helped in better contact tracing’, and in Spain ‘primary care has played a very important role. All patients (except emergency) are attended initially in the health center, which acts as a filter, and applies a common protocol, and depending on the patient’s clinical situation, the patient remained at home with surveillance and follow-up by primary care professionals’. In Thailand, ‘government health facilities recruited professionals from private sectors to help with the increased need for surveillance/support at quarantine sites’.
However, in other countries, it was believed that the surveillance function of PC should be strengthened. From Afghanistan: ‘primary health care had the potential to have been used aggressively in community-level surveillance, contact tracing, health promotion and health protection as primary health care facilities are based closer to the community’.
Discussion
This pandemic is not over and there are lessons to extract from recent experiences in hopes of altering the trajectory of the next wave (UHC2030 International Health Partnership, 2020). Findings from this study highlight the inadequacy of existing PC and PH integration efforts, the need for including PC stakeholders in the planning process, the role of the PC clinician in communicating a clear message, as well as the necessity for PC clinicians to be involved in surveillance, triaging, and follow-up (see Table 4).
Despite the expressed frustration, there were reports of positive experiences of coordination of PC and PH. Ultimately, integration requires the leadership of PC clinicians and officials supporting PHC to actively inject themselves in the PH solutions which are being turned to.
Acknowledging that health systems vary and there is no ‘one-size-fits-all’ model for how best to integrate PC with essential PH functions, the WHO recommended actions which can facilitate inclusion of PC in the planning for pandemics, the response to mitigate the spread, the treatment and finally, the vaccination efforts to deflect future waves of the virus (World Health Organization, 2018c). The recognition of PC as ‘the first point of contact’ was bypassed by many countries during the pandemic as many initial responses were delivered by hospitals. By integrating PC and PH, greater capacity to respond to emergencies may be possible if the synergies gained by harmonizing the two are realized.
Acknowledgments
The authors would like to thank their international experts Prof Michael Kidd (Principal Medical Advisor, Australian Government), Dr Dionne Kringos (Amsterdam Public Health Research Institute, the Netherlands), Dr Ramiro Gilardino (Professional Society for Health Economics & Outcomes Research, USA), Assoc Prof Ben Harris-Roxas (University of New South Wales, Australia), Dr Priya Balasubramaniam Kakkar (Public Health Foundation of India), and Prof Kirsty Douglas, Dr Jane Desborough, and Dr Sally Hall (Australian National University) for providing advice and/or piloting of our survey. The authors would also like to thank Jose M Ramirez-Aranda (University of Nuevo León, Mexico) for the Spanish translation and Dr Viviana Martinez-Bianchi (Duke University in North Carolina, USA) for back-translation. Lastly, the authors would like to express their gratitude to all the primary health care experts who took time out of their busy lives to answer their survey.
Financial support
This study was unfunded. The corresponding author had full access to all the data in the study and is responsible for the decision to submit for publication.
Conflicts of interest
None.
Ethical statement
Ethical approval was granted for 3 years on 9 April 2020 by the University of Auckland Human Participants Ethics Committee (UAHPEC), Ref number 024 557.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation of the University of Auckland Human Participants Ethics Committee (UAHPEC) and with the Helsinki Declaration of 1975, as revised in 2008.
A written informed consent statement was included in the survey and was completed as a condition to submit the completed survey.




 Open access
Open access