



I. Background and Objectives: Why/How was the ARCH Project Commenced
In the Southeast Asia region, natural disasters frequently occur and the damage from those disasters is huge. Southeast Asia is the second biggest region in terms of the total number of natural disasters since 1900, led by South Asia and followed by East Asia. In addition, the total number of deaths by disasters during 2000-2017 in Southeast Asia was 350,000 for 1.2 million in the world.1 It means that deaths in the Southeast Asia region whose population is one-tenth of the world population accounted for one-third of the number of deaths by natural disasters in the world.
A massive earthquake of magnitude 9.1 occurred off the coast of Sumatra in Indonesia and resulted in the Indian Ocean Tsunami on 26 December 2004. More than 220,000 people were killed by the Earthquake and Tsunami in Indonesia and other countries, including many foreign tourists in coastal resort areas such as Phuket Island. After this unprecedented damage caused by the disaster, the Association of Southeast Asian Nations (ASEAN) launched regional initiatives toward strengthening regional collaboration for disaster prevention and response. The ASEAN Member States (AMS) signed the ASEAN Agreement on Disaster Management and Emergency Response (AADMER) on 26 July 2005 in Vientiane, Lao PDR.2 The Agreement sought to provide effective mechanisms to achieve substantial reduction of disaster losses in lives and the social, economic, and environmental assets of AMS, and to jointly respond to disaster emergencies through concerted national efforts and intensified regional and international cooperation. In April 2008, Myanmar was hit and severely damaged by Cyclone Nargis. At that time, Myanmar accepted medical teams from AMS by respecting the AADMER, although the Myanmar government refused many offers of assistance from the international community. The aforementioned AADMER came into effect on 24 December 2009 after all 10 AMS completed their internal process of ratification. Afterward, the ASEAN Coordinating Centre for Humanitarian Assistance on disaster management (AHA Centre) was established in Jakarta, Indonesia in November 2011.3 The AHA Centre has been strengthening its functions and capabilities to coordinate with AMS and relevant UN and international organizations for effective disaster response in the ASEAN region. After Typhoon Haiyan struck the Philippines in November 2013, momentum to strengthen the regional capacity for disaster response was further increased in ASEAN. The ASEAN Leaders finally signed “the ASEAN Declaration on One ASEAN, One Response: ASEAN Responding to Disasters as One in the Region and Outside the Region” at the 28th ASEAN Summit in Vientiane, Lao PDR on 6 September 2016 to increase the speed, scale, and solidarity of ASEAN’s response.4 The Declaration was inspired largely from lessons and experiences gained from ASEAN’s response to Typhoon Haiyan in 2013.
Disaster causes many injuries and sickness. Hospitals in the affected area are also damaged during a large-scale disaster, and it becomes difficult for these damaged hospitals to provide timely medical service or care for their patients and to respond to the surge of medical needs in the affected area.5 Therefore, Sendai Framework for Disaster Risk Reduction prioritizes the establishment of a disaster medical system at national and local levels.6 One of the key factors in the disaster medical system is to dispatch emergency medical teams (EMT) from outside of the affected areas. If the number of injured and sick by a large-scale disaster is beyond the medical capacity of the affected country, acceptance of international EMTs (I-EMTs) by the affected country must be considered.7 Many I-EMTs of other developed countries including Japan, Red Cross, and international NGOs have been dispatched to sites of large-scale disasters that occurred in the AMS in the past, and recently AMS themselves have begun to dispatch their EMTs to the affected area in other AMS as the case of Cyclone Nargis in Myanmar. Nowadays, AMS have come to consider more proactively to dispatch their EMT to disasters in the ASEAN region. The acute phase within the first week after disaster onset is very important for the deployment of I-EMTs to respond to the surging medical needs of the affected population. AMS I-EMTs are advantageous in terms of deployment time within the ASEAN region in comparison with I-EMTs outside of the ASEAN region. In addition, each AMS has some commonalities and similarities in their languages and culture as well as among different people of each AMS living in other AMS. In consideration of the aforementioned facts, AMS has come to recognize that it is necessary to accelerate the collaboration among themselves for emergency medical response in the ASEAN region as much as possible. However, ASEAN has not yet developed a robust regional mechanism and capacity to realize “One ASEAN, One Response,” especially for disaster medical response. Familiarizing the concept of disaster health management (DHM) in each AMS and realizing regional collaboration of medical response toward “One ASEAN, One Response” has been discussed. There are big differences and gaps among the 10 AMS countries in terms of their systems and capacities to implement DHM. The system and capacity for emergency medicine which must form a base for implementation of medical response operation in the acute phase of disaster have not been established yet in a few of the AMS. Based on these perceptions, ASEAN highlighted DHM as one of the priority areas in the ASEAN Post-2015 Health Development Agenda (HDA) adopted by the 12th ASEAN Health Ministers Meeting (AHMM) in September 2014 with a demand that ASEAN should strengthen regional collaboration and coordination mechanism and regional capacity on DHM.8
In December 2013, the Government of Japan committed to enhancing cooperation in disaster management with ASEAN as stated in the Vision Statement of the ASEAN-Japan Commemorative Summit by introducing “ASEAN-Japan cooperation package for enhancement of disaster management.”9,10 One of the components of this cooperation package in the above statement is to establish a network for disaster medicine between ASEAN and Japan. With the above context, Japan International Cooperation Agency (JICA) conducted a Survey on the Current Situation of Disaster/Emergency Medicine System in the ASEAN Region to collect necessary data and information on current status, potential needs, and challenges of disaster/emergency medicine in each AMS in order to examine a possible plan and way forward of establishing regional collaboration mechanism on DHM in the ASEAN region.11
Japan is also a disaster-prone country and has plenty of experience and knowledge in all aspects of disaster management. Through those experiences and efforts to build back better, Japan has developed Disaster Medical Assistance Teams (DMAT) for domestic disasters as well as the Japan Disaster Relief (JDR) Medical Team for international disaster response, both of which have been deployed many times for actual disasters.Reference Kondo, Koido and Morino12,Reference Homma13 JICA also conducted international training courses on Emergency Medicine and Disaster Medicine for 20 years from 1988, inviting a total of 207 participants from 53 developing countries.Reference Asari, Koido, Nakamura, Yamamoto and Ohta14,Reference Kondo, Seo and Yasuda15 Thailand established a Thai disaster medical team in 2008 by the leadership of the ex-participants of the JICA training courses referring to the Japanese DMAT system.
Under the above circumstances, Japan expressed its willingness to continuously support ASEAN for disaster medicine at the 6th ASEAN3 Health Ministers Meeting in September 2014.16 On the other hand, DHM was raised as one of the priority areas in the ASEAN Post-2015 HDA, and Thailand expressed to formulate the Project for Strengthening the ASEAN Regional Capacity on Disaster Health Management (ARCH Project) in cooperation with JICA to develop a regional collaboration mechanism and capacity on DHM in the ASEAN region.17 Then, the Thai National Institute for Emergency Medicine (NIEM) and JICA agreed to implement the ARCH Project which was a technical cooperation project under Japan’s Official Development Assistance (ODA) in February 2016. The Committee of Permanent Representatives (CPR) of ASEAN also approved the ARCH Project in January 2016 as an ASEAN official project which was listed for Health Priority 12; Disaster Health Management in the ASEAN Post-2015 Health Development Agenda 2016-2020.8 The ARCH Project has started in July 2016, led by three parties: NIEM, Thai Ministry of Public Health (MOPH), and JICA. The ARCH Project was implemented from July 2016 until July 2019 at first and was extended for 21 months until March 2021. Moreover, the Project has been extended again for another nine months from April 2021 to December 2021 in order to complete the planned activities which were not able to be conducted by March 2021 due to the outbreak of the coronavirus disease 2019 (COVID-19).
II. Structure and Contents of the Project
The main objective of the ARCH Project is to strengthen coordination on DHM for rapid and effective response to disasters occurring in the ASEAN region by utilizing regional resources, and also to enhance the capacity of each AMS on DHM and its basal emergency medicine. Finally, the Project aims to develop an ASEAN regional collaboration mechanism on DHM in the future, which could function effectively for medical response to actual disasters in the ASEAN region to realize “One ASEAN, One Response” so that it could mitigate the sufferings of the affected population.
In order to realize the objective and goal, the ARCH Project set five expected outputs and planned to conduct the following activities to achieve each output. The outline of the Project is indicated in Figure1.
Output 1: Coordination platform on DHM is set up.
Activity 1-1: Regional coordination committee (RCC) meetings are organized every year to share the progress and discuss the direction of the Project.
Activity 1-2: Discussion on the Work Plan of the Plan of Action (POA) 2019-2025 to implement the ASEAN Leaders’ Declaration on Disaster Health Management (ALDDHM)18 and the part of DHM under Work Programme for the next Health Development Agenda 2021-2025.
Output 2: “Framework of regional collaboration practices is developed.”
Activity 2-1: Develop and prepare the program of the regional collaboration drill (RCD) with the project working group (PWG).
Activity 2-2: Conduct the RCD every year in AMS.
Activity 2-3: Compile recommendations on regional collaboration on DHM based on the discussion and knowledge sharing through project activities.
Activity 2-4: On-site practice is conducted when a disaster occurs in the ASEAN region (or AMS) (if possible).
Activity 2-5; Collect and share Lessons Learned from responses for actual disasters in ASEAN.
Output 3: Tools for effective regional collaboration on DHM are developed.
Activity 3-1: Formulate PWG for regional collaboration tools at the beginning of the project.
Activity 3-2: Develop a draft regional Standard Operation Procedure (SOP) and minimum requirements (MR) for DHM with the PWG.
Activity 3-3: Prepare databases of EMTs of AMS.
Activity 3-4: Draft framework of health needs assessment (HNA) in emergencies with the PWG.
Activity 3-5: Facilitate the endorsement process of all regional collaboration tools that were developed in this phase by ASEAN Senior Officials Meeting on Health Development (SOMHD) or relevant ASEAN sectoral bodies.
Activity 3-6: Study on possibilities of ASEAN collective approaches.
Output 4: Academic network on DHM in AMS is enhanced.
Activity 4-1: Present outcomes of the Project activities at academic conferences such as the Japanese Association for Disaster Medicine (JADM), Asia Pacific Conference on Disaster Medicine (APCDM), and World Association for Disaster and Emergency Medicine (WADEM).
Activity 4-2: Hold an academic seminar.
Output5: Capacity development activities for each AMS are implemented.
Activity 5-1: Prepare training plan, curriculum, and materials on DHM and emergency medical system based on needs survey with the PWG.
Activity 5-2: Develop standard training curriculums.
Activity 5-3: Conduct training on DHM and emergency medical service for AMS.
Activity 5-4: Conduct monitoring survey and evaluation on capacity development on DHM in each AMS.
Activity 5-5: Conduct a study of systems and needs for the capacity development on DHM in each AMS.
Activity 5-6: Conduct a study tour in Japan for AMS.
Activity 5-7: Conduct a training program in Japan for the Thai counterpart personnel.

Figure 1. Outline of the ARCH Project.
III. Overall Progress and Evaluation of ARCH Project
A. Methodology and Criteria of Evaluation
The Project was reviewed in terms of: (1) The accomplishment of the Project, and (2) Five Evaluation Criteria which are outlined below.
1. Accomplishment of the Project
The accomplishment of the Project was measured in terms of the Outputs, the Project Purpose, and Overall Goal in comparison with the Objectively Verifiable Indicators of the Project Design Matrix (PDM) as well as the plan delineated in the Record of Discussions (R/D), which are the documents.
2. Evaluation based on the Five Evaluation Criteria
a. Relevance: The relevance of the Project was reviewed to see the validity of the Project Purpose and the Overall Goal in connection with the needs of the beneficiaries and policies of ASEAN and Japan.
b. Effectiveness: Effectiveness was analyzed by evaluating the extent to which the Project has achieved and contributed to the beneficiaries.
c. Efficiency: The efficiency of the Project implementation was analyzed focusing on the relationship between the Outputs and Inputs in terms of timing, quality, and quantity.
d. Impacts: Impacts of the Project were forecasted by referring to positive and negative impacts caused by the Project.
e. Sustainability: The sustainability of the Project was analyzed in institutional, financial, and technical aspects by examining the extent to which the achievement of the Project would be sustained and/or expanded after the Project is completed.
B. Result
1. Accomplishment of the Project
The accomplishments for each Output are described in Table1.18–Reference Kubo, Yanasan, Herbosa, Buddh, Fernando and Kayano20 All Outputs were accomplished.
Table 1. Evaluation of ARCH Project Accomplishment for Each Output

Output 1 (Set up of coordination platform on DHM) was accomplished. RCC was established as a coordination platform to oversee the implementation of the ARCH Project and was upgraded to an ASEAN official committee, namely Regional Coordination Committee on Disaster Health Management (RCCDHM).
Output 2 (Development of framework of regional collaboration practices) was accomplished. Regional collaboration drill (RCD) was developed as an occasion for regional collaboration practices and it was conducted five times in four AMS. RCD became a good test field of tools developed by Output 3. The EMT minimum data set (MDS) was verified to be effective in the RCDs, before it was officially adopted by WHO in February 2017 as an international reporting standard for EMTs. A template for the collection of lessons learned from responses to actual disasters in ASEAN was developed to integrate the knowledge and experiences.
Output 3 (Development of tools for effective regional collaboration on DHM) was accomplished. PWG 1 and PWG 2 were organized and SOP for coordination of EMTs in ASEAN, MR for members of EMTs, HNA for EMTs were developed. SOP, Medical Record, and HNA were finalized through testing those tools in the RCDs and were reviewed in the PWG1. These tools were tested both in table top and field exercises. EMT data in AMS were also collected. A Sub Working Group (SWG) on ASEAN collective approaches was established.
Output 4 (Enhancement of Academic network on DHM in AMS) was accomplished. Various presentations on the activities and outputs of ARCH were made by ARCH members on academic occasions stimulating and attracting practitioners and investigators.
Output 5 (Implementation of capacity development activities for each AMS) was accomplished. Several training programs and a study tour inviting participants from AMS were conducted in Thailand and Japan. SWG on Standard Training Curriculum was established. Questionnaire survey and the field study on capacity development in AMS were conducted.
The Project Purpose and its verifiable Indicators are indicated in Table2. Indicator 1 (Regular coordination meetings) was achieved. The RCC which is a coordinating platform to oversee the implementation of the ARCH Project was established immediately after the Project started. The RCC meetings were held five times. The RCC was upgraded to RCCDHM which is an ASEAN authorized committee to effectively and sustainably operationalize the Plan of Actions (POA) for the ALDDHM on time after the POA was adopted by the 14th AHMM on 29th August 2019 in Cambodia.18 The First Meeting of RCCDHM was also supported by the Project to be held in January 2020 in Bangkok.
Table 2. ARCH Project Purpose According to the Verifiable Indicators

Indicator 2 (Clarification of activities and approval) was achieved. Necessary activities and products of regional collaboration such as RCC, PWG, RCD, AMS training, SOP, and various templates for AMS I-EMT were clarified and approved in the RCC and PWG.
Indicator 3 (Recommendation to SOMHD) was achieved. The RCC and PWG discussed not only the directly related activities and outputs of the ARCH Project but also the drafting of ALDDHM and its POA in consideration of sustainability for regional collaboration after the Project. The text drafted through the discussion in the RCC and the PWG was submitted to the ASEAN Health Cluster 2 meetings and the SOMHD. Finally, the ALDDHM was adopted on the occasion of the 31st ASEAN Summit in the Philippines on 13 November 2017 and the POA was adopted by the 14th AHMM on 29 August 2019.18,19
Indicator 4 (Tool development and approval) was achieved. The regional collaboration tools such as the SOP and various templates for AMS I-EMTs were developed, reviewed, and endorsed by the PWG 1 and RCC. These tools have been submitted to the RCCDHM, ASEAN Health Cluster 2, and SOMHD for endorsement. Joint tabletop exercise by ASEAN Health Cluster 2 (TTX) and Working Group on Preparedness, Response, and Recovery (WG-PRR) under ASEAN Committee on Disaster Management (ACDM) with the AHA Centre was conducted to review the SOP for AMS I-EMTs to integrate it into ASEAN Standard Operating Procedure for Regional Standby Arrangements and Coordination of Joint Disaster Relief and Emergency Response Operations (SASOP).21
The overall goal and its verifiable indicators are indicated in Table3. Indicator 1 (Policy framework) was achieved. The ALDDHM was adopted on the occasion of the 31st ASEAN Summit in the Philippines on 13 November 2017.19 The POA to implement the ALDDHM (2019-2025) was drafted by the leadership of Thailand. The RCC and PWG of ARCH discussed improving the POA and a revised version based on those discussions was submitted to the SOMHD in April 2019. Finally, the POA was adopted by the AHMM on 29 August 2019.18
Table 3. The Overall Goal and its Verifiable Indicators
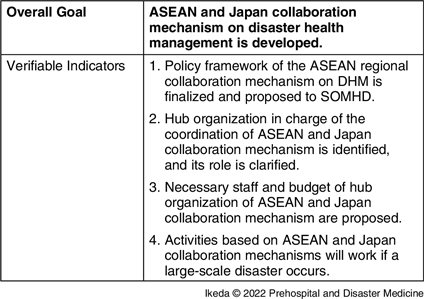
Indicator 2 (Identification of hub organization) was partially achieved. The RCCDHM was proposed to operationalize the POA. As a part of the POA, the Terms of Reference (TOR) for the RCCDHM were also adopted by AHMM, and the AMS representatives of the RCCDHM were nominated in December 2019. The first meeting of the RCCDHM was held on 22-23 January 2020. The establishment of the ASEAN Academic Network and ASEAN Institute on DHM (AIDHM) were also proposed to facilitate the academic part of the POA including research activities, education/training activities, and knowledge sharing. The drafts of the TOR for the ASEAN Academic Network and AIDHM were also discussed and polished in the Project and submitted to the RCCDHM. The RCCDHM and the AIDHM could be regarded as the “Hub organization in charge of the coordination of ASEAN and Japan collaboration mechanism” referred to in this Indicator. Although it is still necessary to continue negotiations and discussions among AMS on the ASEAN Academic Network and AIDHM, if the discussions are concluded, it can be said that this indicator would be satisfied. The ARCH Project has been conducted in close collaboration with the Japanese Advisory Committee, which consists of experienced and knowledgeable medical professionals on disaster medicine as well as the JDR Secretariat and JDR registered members. In addition, several opportunities have been provided for the ARCH AMS members to participate and make presentations in the conferences of JADM, APCDM, Radiation Emergency Medical Preparedness and Assistance Network (REMPAN), and WADEM. The network of practitioners and experts on DHM between AMS and Japan has been already strengthened through the ARCH Project. The ARCH Project took a very important role in the standardization of the EMT Minimum Data Set (MDS) which is the EMT reporting format for disease surveillance developed in collaboration between WHO and Japan (JICA and JDR members).
Indicator 3 (Staff and budget) was partially achieved. Thailand decided to serve as the secretariat of the RCCDHM. Thai MOPH appointed some staff of the Division of Public Health Emergency Management as the officers in charge of the secretariat of the RCCDHM.
Indicator 4 (Actual disaster response) was not evaluable. So far, cases in which activities based on ASEAN and Japan collaboration mechanisms were conducted for actual disaster response have not yet been reported.
2. Evaluation based on the Five Evaluation Criteria
Evaluation of the ARCH Project based on the Five Evaluation Criteria is listed in Table4.19
Table 4. Evaluation of the ARCH Project based on the Five Evaluation Criteria

Most of the activities have been implemented and the Outputs are almost achieved as planned. Regarding the indicators for the Project Purpose, the Project has already achieved or can be expected to achieve all of its targets in the near future. In addition, the Project has created a synergistic effect on the participants from AMS, resulting in accomplishments beyond the Project Purpose toward the Overall Goal, which should be achieved several years after the termination of the Project period.
Using the Five Evaluation Criteria, the ARCH Project has succeeded in generating a bigger Impact and securing higher Sustainability than those expected before starting. If the POA for the ALDDHM can be smoothly implemented, the Impact and Sustainability for ARCH could be ensured further. On the other hand, the Effectiveness and Efficiency had some space for improvement. The SOP and other tools can be better for actual international deployment, especially in the area of logistics for self-sufficient international deployment. The participants of the AMS training and the RCDs can utilize their acquired knowledge more for DHM in each AMS. From the Efficiency perspective, continuous commitment and cooperation of each government and relevant parties are necessary. To maintain consistency in the sequence of discussions, communication, and continuous education in each AMS are vital. It is necessary to continue testing the collaboration tools in the RCDs so that they can be functional and effective in an actual disaster. In addition, it is also necessary to improve the capacities of DHM in each AMS to fulfill capabilities necessary for disaster medical response, as well as to establish regional collective measures to support the affected AMS.
IV. Future Strategy
As a result of discussions between AMS and Japan during the project formulation stage before the ARCH Project was started, it was planned that the project should be continued for 10 years, saying more in detail, the first target in the first phase for three-four years is to initiate and strengthen the regional coordination on DHM in ASEAN and next target in the second phase for three-four years is to develop the collaboration mechanism on DHM and finally, in the last phase, ASEAN could complete acquiring the functional collaboration mechanism and regional capacity on medical responses for actual disasters and emergencies. Actually, the progress by the ARCH Project and its circumstances on DHM in ASEAN has moved on faster than expected. The ALDDHM was adopted on the occasion of the 31st ASEAN Summit in Manila on 13 November 2017.19 In addition, the POA 2019-2025 to implement the ALDDHM drafted through the ARCH Project was also adopted by the AHMM in August 2019.18 The POA included the activities that were initiated under the ARCH Project, such as RCC, RCD, SOP of AMS I-EMT, training programs on DHM, and ASEAN Academic conference. This means that the ARCH Project has already developed some extent of the collaboration mechanism on DHM and has entered into the final stage to complete toward acquiring the functional collaboration mechanism and regional capacity on DHM in ASEAN.
The POA is the plan till 2025, which has five priority areas and 21 targets (14 targets at the regional level and seven targets at the national level).18 Therefore, the next phase of ARCH should align with the POA to achieve the selected 19 targets among the 21 POA targets. ARCH 2 Project will start in 2022 after the ARCH extension phase completes at the end of 2021 and will last for four years and some months to realize the targets of the POA.
The 10-year plan for steps to an ASEAN collaboration mechanism on DHM is indicated in Figure2.

Figure 2. Mid-Term Plan for Steps for ASEAN Collaboration Mechanism on DHM.
ASEAN has set the ASEAN Post-2015 HDA in which DHM has been raised as one of the 20 health priorities, and the ARCH Project was listed as a project for the health priority on DHM.8 Now, ASEAN is preparing a new Work Programme for the next ASEAN HDA 2021-2025. DHM should be continuously one of the health priorities in the HDA. ARCH prepared a draft Work Programme on DHM through a series of discussions in the ARCH PWG and which was consistent with the implementation of the POA.18 The Work Programme on DHM has been already proposed to the ASEAN upper health bodies. Therefore, the ARCH 2 Project can contribute to implementing both the POA and the Work Programme on DHM in the ASEAN Health Development Agenda 2021-2025. Relations among the ALDDHM, POA, HDA, and ARCH can be illustrated in Figure3.

Figure 3. ASEAN Collaboration Framework for DHM.
The overall purpose of the ARCH Project is to contribute to the capacity development relating to the preparedness and response stages in the disaster management cycle. The first and extension phase of the ARCH Project has mainly concentrated on developing the regional capacity through the development of a regional collaboration/coordination platform, framework, and tools as well as training for the AMS personnel involved in regional collaboration/coordination on DHM. However, the ARCH 2 Project must tackle both regional capacity and national capacity in each AMS so that ASEAN could acquire sufficient capacity to strengthen its preparedness as a whole in the region and to effectively work together for disaster medical response. Therefore, the ARCH 2 Project should approach the seven targets at the national level as well as 12 targets at the regional level of the POA.18 Figure4 illustrates the outline and relationship of the ARCH and ARCH 2 Projects. The overall goal of the ARCH and ARCH 2 Projects is the health emergency and disaster-resilient ASEAN region with both improved regional capacity (ARCH Project) and national capacity (ARCH 2 Project) complementing each other.

Figure 4. Overall Purpose of ARCH and ARCH 2 Projects.
V. Conclusion
The ARCH Project is the first-ever regional cooperation mechanism and standardization of DHM in ASEAN. It was not possible without the multi-stakeholder commitment of AMS including the AHA Centre, relevant governmental and non-governmental bodies, and health and non-health clusters under the umbrella of “One ASEAN, One Response” in one of the most disaster-prone regions in this unprecedented time of complexity, aging, urbanization, and climate change. COVID-19 and social unrest are increasing the difficulties in DHM. The ARCH and ARCH 2 Projects will have a remarkable impact on the resilience and flexible medical response to disasters caused by any type of hazards, although continuous efforts of stakeholders to make this initiative sustainable are necessary.
Conflicts of interest/financial support
The ARCH Project was funded by JICA as part of the Official Development Assistance of the government of Japan in collaboration with NIEM/ MOPH Thailand as counterpart agencies. This publication was entirely funded by JICA as a part of the ARCH Project. Shuichi Ikeda is a member of the expert team dispatched by JICA. Authors do not have any conflict of interest to declare.
Author Contribution
Shuichi Ikeda and Phumin Silapunt equally conceptualized and wrote the manuscript.









 Open access
Open access