



Introduction
Oncology clinics are environments where there are numerous factors that trigger both individual values and professional values. Oncology nurses face many ethical situations which trigger their values in daily practices, such as informed consent, managing pain or painful treatments, securing the quality of life, administering futile treatment at the end of life, resuscitation applications, and dealing with hopelessness, death, and preservation of dignity (Ameri et al. Reference Ameri, Safavibayatneed and Kavousi2016; Fruet et al. Reference Fruet, Dalmolin and Barlem2018; Hamric Reference Hamric2012; Sweeney Reference Sweeney2017). Although it has a much broader perspective, palliative care traditionally targets individuals with oncological problems and includes many situations in common with oncology nursing (Bradshaw et al. Reference Bradshaw, Dunleavy and Garner2022; Maffoni et al. Reference Maffoni, Argentero and Giorgi2019). In such cases, nurses’ emotions, thoughts, and actions will be unavoidably affected by their personal values (Schaefer and Vieira Reference Schaefer and Vieira2015). However, nursing is a profession built on certain human values. Although oncology nurses provide care within their own value systems, just as all other nurses and health professionals do, they are trained according to the professional values of nursing (Goris et al. Reference Goris, Kılıc and Ceyhan2014). The fact that nurses are faced with situations that cause conflict with their values and in some cases have to take actions that do not comply with their values is a risk for nurses experiencing moral distress (MD) (Wilson Reference Wilson2018).
MD, which is defined as the discomfort felt when an individual’s moral integrity is seriously compromised, when an individual fails to act according to core values and obligations, or when their actions fail to achieve the desired result (Hamric Reference Hamric2012; Jameton Reference Jameton2017), is affected by many factors, including the characteristics of the health-care worker and the group receiving the service. The literature includes various studies examining the sources of MD, related factors, and applications to reduce MD. There are 3 main theories on MD, but the one developed by Corley (Reference Corley2002) has been the most widely accepted, and therefore, this study uses Corley’s Moral Distress Theory (MDT) as its basis (Corley Reference Corley2002).
Corley (Reference Corley2002) emphasizes the nurses’ beliefs and values in his MDT, while MD looks at external factors in describing the experiences created through the conflict of these values and truths (Corley Reference Corley2002). The MDT is based on the following two hypotheses: “nursing as moral profession” and “nurses as a moral agent.” According to these hypotheses, nurses may experience MD in ethical situations they face while doing their job, and if they cannot demonstrate their moral effectiveness, they become vulnerable to MD. Some moral concepts have been used to explain the model developed by Corley (Reference Corley2002), who argues that these concepts that affect the development of moral action and moral competence are related to the concept of MD and interact with it. Corley’s model consists of 8 moral concepts, namely, commitment, sensitivity, autonomy, sense making, judgment, conflict, competency, and certainty. The interaction of these concepts with each other and the effects of these concepts may lead to MD or influence moral behavior (Corley Reference Corley2002).
It is known that the MDT is the source of much data related to the concepts, structure, emergence, and expressions of MD (Wilson Reference Wilson2018). However, ever since the theory was first developed, the conflict between the values of nurses and the values of others as the cause of MD has been emphasized, but the values of the nurses have not been sufficiently studied. Wilson et al. examined Corley’s model from this perspective in their MDT analysis study and reported that identifying the individual values that trigger MD in the model could contribute to gaining a better understanding of the concepts in MD (Wilson Reference Wilson2018). Therefore, it is believed that showing MD to be experienced when individual values are threatened will both provide a stronger grasp of the concept and shed light on preventive practices.
Another value system element that can be linked to the moral sensitivity theme and individual values in MDT is professional values. Although professional values in nursing vary slightly by society, there are internationally accepted basic professional values. However, it is important to note that although these values are more or less universal, it is known that these values are implicitly taught through the curricula of many institutions and cannot be measured (Sellman Reference Sellman2011). In this context, determining the professional values of nurses is also essential for gaining a better understanding of the concept of MD.
Therefore, examining the relationship between MD and the values of oncology nurses is very important to understand the situations they regularly faced and have the potential to trigger MD, individual values, and professional values. This study aims to examine the relationships between oncology nurses’ individual and professional values on MD. The tested hypotheses are that (1) oncology nurses with higher professional values will experience more MD and (2) oncology nurses with higher individual values will experience more MD. The data to be obtained from this study will contribute to providing clarification of the area related to the MDT values emphasized in the literature, which need to be examined in more detail.
Methods
Study design and sample
In this study, structural equation modeling (SEM) was used in a descriptive-relational design to determine the interrelationships between MD, individual and professional values. The population of the study consisted of two adult oncology hospitals located in Ankara, the capital city of Turkey. To carry out the study, oncology hospitals in this province were applied, but permission was obtained from one hospital. The hospital, for which permission was obtained, is the only training and research hospital in the country that provides services in the field of oncology and serves all cancer patients throughout Turkey. A total of 148 people work as oncology nurses for at least 6 months in the inpatient clinics of the 500-bed hospital. 119 oncology nurses agreed to participate in the study, and the study was completed with 116 nurses who filled out the scales completely. Results of the G-power analysis conducted for the sample size of 116 participants showed that the sample had 98% power.
Instruments
Research data were collected between September 2019 and July 2020 through participant information form, Moral Distress Scale-Revised Adult Nurses (MDS-R), Nursing Professional Values Scale (NPVS), and Values Scale (VS). The self-report method was used in data collection. The nurses were invited to participate in the study and answer the questionnaires during their work shifts. It took the nurses an average of 20 min to complete the questionnaires.
Moral Distress Scale-Revised Adult Nurses
The MDS-R was developed by Hamric et al. (Reference Hamric, Borchers and Epstein2012) in 2012 to determine the level of MD experienced by nurses who provide care to adults. The scale consists of 21 items, arranged on a 5-point Likert-type scale of two columns (0–4), and measures insensitivity and frequency. In the evaluation of the results, the frequency (f) and intensity (i) scores are multiplied (f × i) to obtain a general MD score in the range of 0–16. In this case, the total score obtained can range from 0 to 336. The scale does not have a cutoff point, and the higher the score, the greater the MD. The Turkish validity and reliability study of the scale was carried out by Karagozoglu et al. (Reference Karagozoglu, Yildirim and Ozden2017), who found it to be valid and reliable for use in the Turkish culture. The Cronbach’s alpha value, which was calculated as 0.88 for the original scale, was calculated as 0.85 for the Turkish adaptation.
Nursing Professional Values Scale
This scale, which reflects the American Nurses Association (ANA’s) code of ethics, was developed by Darlene Weis and Mary Jane Schank to reveal nurses’ values. It is a 5-point Likert-type scale consisting of 31 items. The scale’s subdimensions are human dignity (11 items), responsibility (7 items), activism (5 items), security (4 items), and autonomy (4 items). The total score can vary from 31–155, and a high score indicates that nurses place more importance on professional values and ethical issues. The Turkish validity and reliability study of the scale was carried out by Alpar and Orak (Reference Orak2012), who found it to be valid and reliable for use in Turkish culture. Nursing education in Turkey is planned in line with universal ethical codes and is carried out taking into account the ethical statements of ANA, International Council of Nurses, and Turkish Nurses Association. The Cronbach’s alpha value, which was calculated as 0.94 for the original scale, was calculated as 0.95 for the Turkish adaptation.
Values Scale
This scale was developed by Dilmac et al. (Reference Dilmac, Aricak and Cesur2014) to examine the psychometric properties of the values of adults. It is a 5-point Likert-type scale consisting of 39 items. The scale does not have a total score. Higher scores indicate that the individual has a greater degree of care for the respective subdimension. Cronbach’s alpha values were calculated as follows: 0.90 for “Social Values,” 0.80, for “Career Values,” 0.78 for “Intellectual Values,” 0.80 for “Spirituality,” 0.78 for “Material Values,” 0.61 for “Human Dignity,” 0.66 for “Romance Values,” 0.65 for “Freedom,” and 0.63 for “Generosity and Courage.”
Data analysis
IBM SPSS (Statistical Package for Social Sciences) version 23.0 was used for data analysis and IBM AMOS (Analysis of Moment Structures) version 23.0 statistical programs were used for structural equation analysis. Descriptive statistics were used to analyze sociodemographic data. Validation of SEM, using maximum likelihood estimation, and path analysis, chi-square (χ2)/degree of freedom (df) (χ 2/df < 2), adjusted goodness-of-fit index (AGFI ≥ 0.90), goodness-of-fit index (GFI ≥ 0.90), normed fit index (NFI ≥ 0.90), non-normed fit index (NNFI ≥ 0.90), comparative fit index (CFI ≥ 0.90), and root mean square error of approximation (RMSEA ≤ 0.08) fit indices were used (Kline Reference Kline2015). Pearson moment correlation was used to determine the relationships between the variables, and the level of significance was determined as p < 0.05.
Ethical considerations
The procedures followed were in accordance with the Helsinki Declaration of the World Medical Association. Permission to carry out the study was obtained from the Hacettepe University Ethics Commission (no: 5798623-300), and necessary permissions were obtained from the hospital at which the study was conducted. Participants were informed about all aspects of the study prior to receiving their informed consent to participate.
Results
Participants’ characteristics
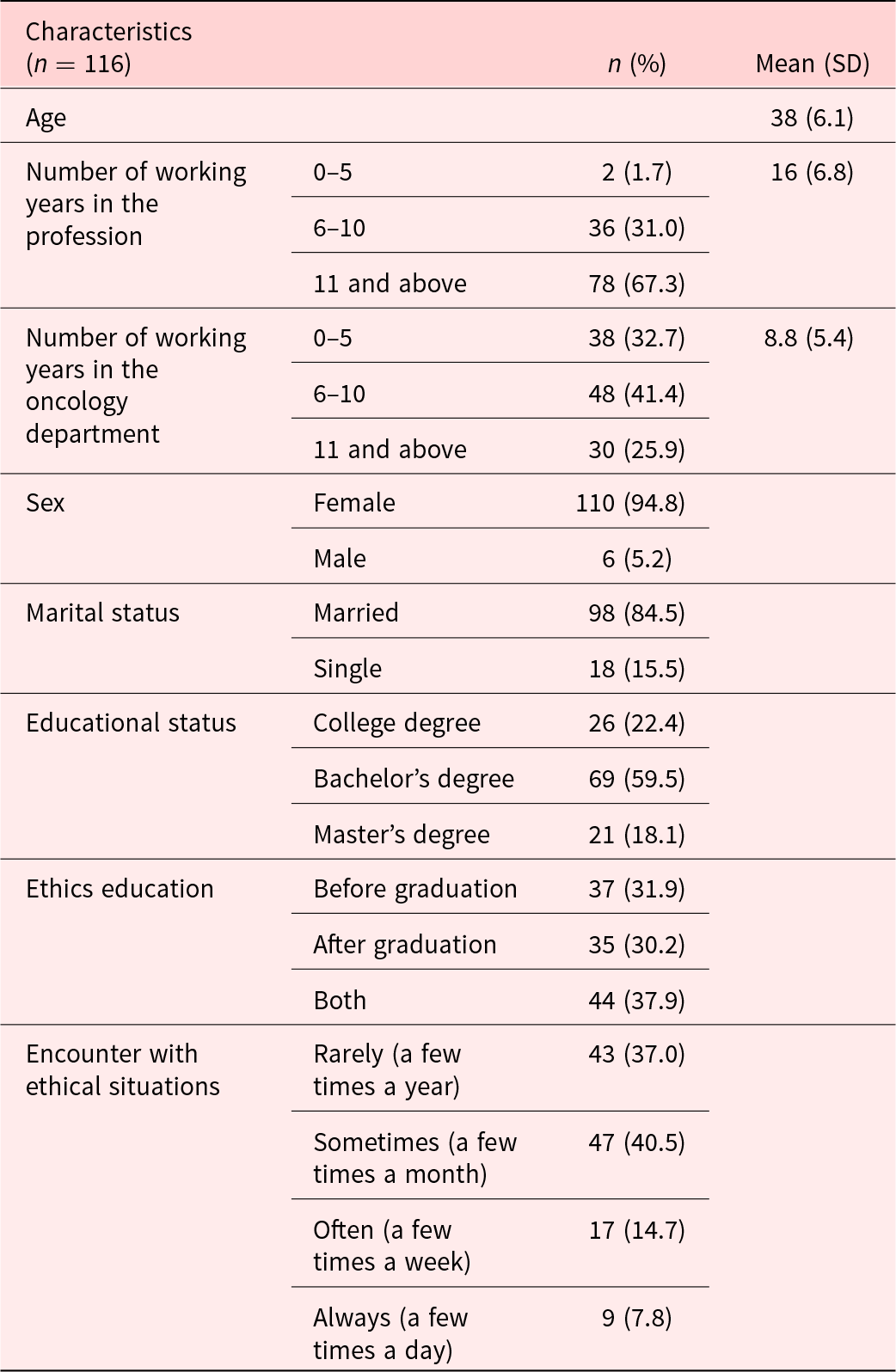
Table 1 shows the sociodemographic characteristics of the participants. The mean age of the participants was 38 ± 6.1 years, more than half (67.3%) had been working in the profession for over 11 years, and nearly half (41.4%) had been working in the oncology department for 6–10 years. Furthermore, nearly half of the participants (40.5%) stated that they encountered ethical situations at least a few times a month.
Table 1. Participants’ sociodemographic characteristics
Moral Distress Scale-Revised items means and standard deviations
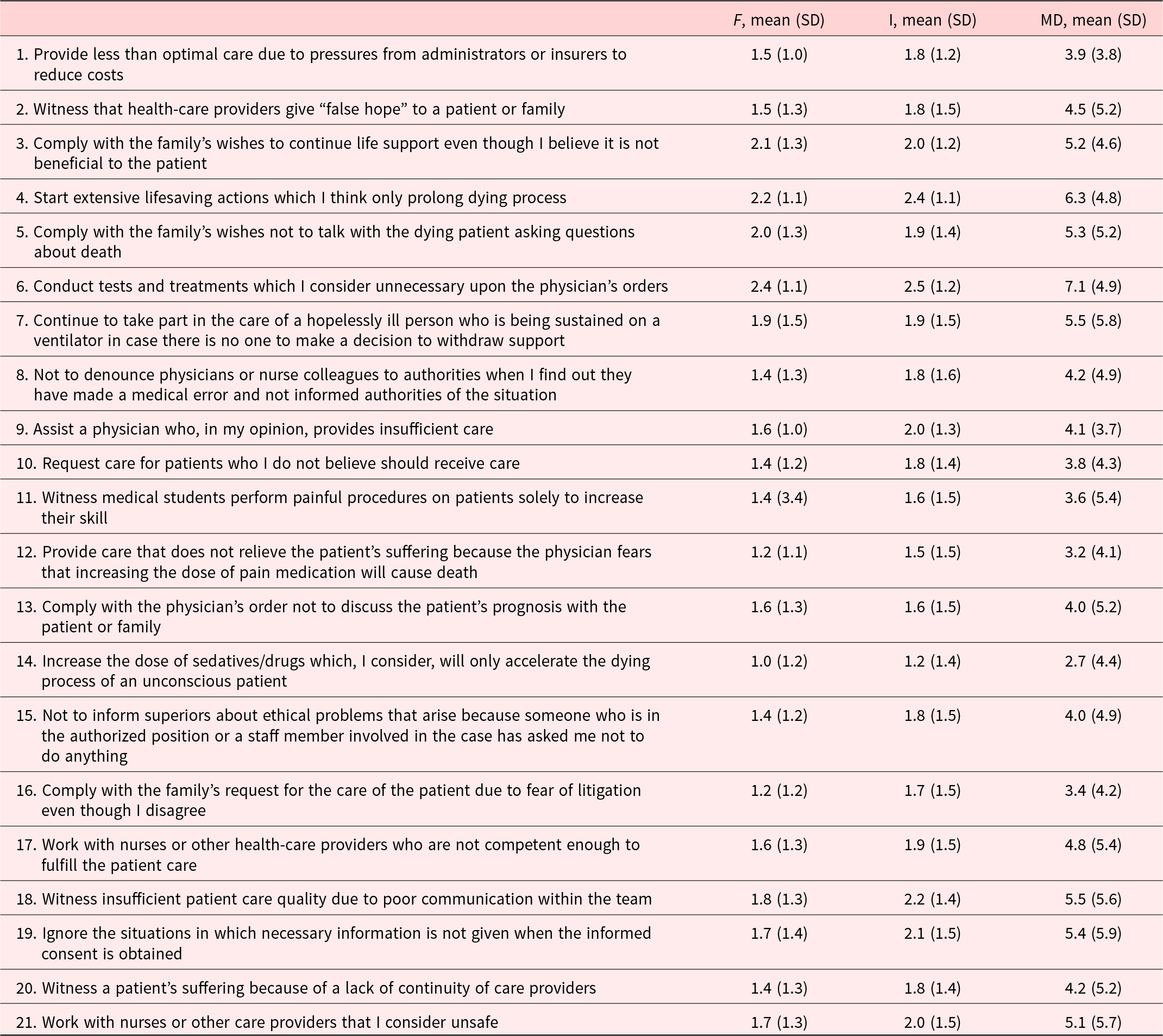
Table 2 shows the mean MDS scores of the participants, from which it can be seen that the scores for items 3, 4, 5, and 6 were moderately high in terms of MD frequency. The highest scores obtained in terms of MD frequency were on items 3, 4, 6, 18, 19, and 21.
Table 2. Participants’ MDS mean scores
Means, standard deviations, and correlations among the study variables
Means, standard deviations, and correlations among the study variables are presented in Table 3. Examination of the MDS mean scores showed that the mean score for MD frequency was moderately low (1.6 ± 0.7) and that the mean score regarding intensity was moderate (1.9 ± 0.8). Examination of the mean NPVS scores revealed that the obtained total mean score of the scale can be evaluated as high (4.1 ± 0.6). The NPVS subdimension mean scores were found to be quite close to each other. The “Responsibility” subdimension received the lowest score (4 ± 0.8), while the “Autonomy” subdimension received the highest (4.2 ± 0.7). The scores from all VS subdimensions were above average and could be evaluated as high. Similar to the NPVS, all VS subdimension scores were found to be close to each other. Finally, the “Social value” and “Human dignity” subdimensions received the highest scores (8.5 ± 0.7 and 8.6 ± 0.8), while the “Romance values” and “Materialistic values” subdimensions received the lowest (7.5 ± 1.4 and 7.3 ± 1.6). The total MDS mean score varied from 2.71 to 7.10.
Table 3. Means, standard deviations, and correlations among the study variables
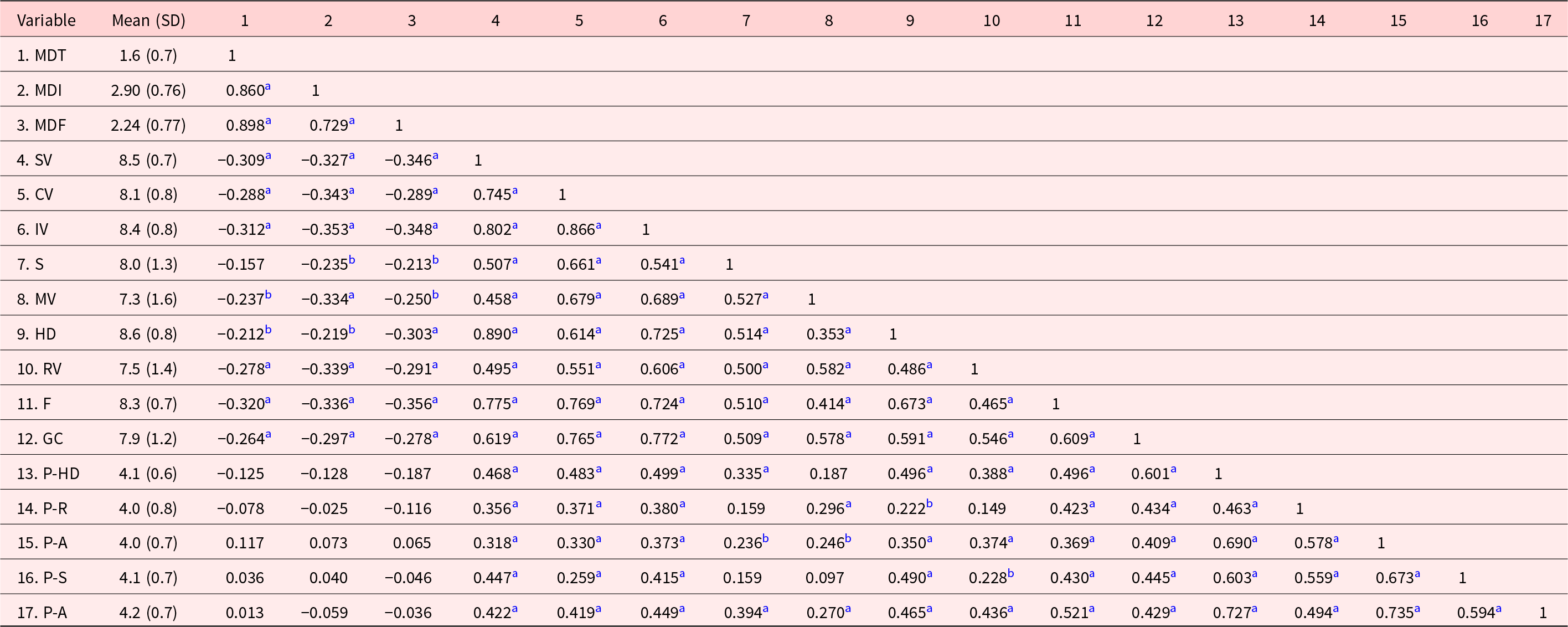
MD-T, moral distress total score; MD-I, moral distress intensity score; MD-F, moral distress frequency score; SV, social values; CV, career values; IV, intellectual values; S, spirituality; MV, material values; HD, human dignity; RV, romance values; F, freedom; GC, generosity and courage; P-HD, professional human dignity; P-R, professional responsibility; P-A, professional activism; P-S, professional security, and P-A, professional autonomy.
a p < 0.01.
b p < 0.05.
The examination of the relationship between the VS scores and MDS scores showed that there was a weak negative relationship between the MDS subdimensions frequency and intensity and all VS subdimensions (p ≤ 0.05). No relationship was found between the NPVS and the MDS subdimensions’ frequency and intensity scores and the total score (p ≤ 0.05). The same applies to all NPVS subdimension scores (p ≥ 0.05) (Table 3).
Structural equation modeling of the predicted model
In the study, hypotheses regarding the effect of individual and professional values on MD were tested with SEM analysis, and it was determined that the data were suitable for the model with 4 modifications. The fit indices for the model were found as follows: χ2/df value was 1.76 (<2; perfect fit), GFI value was 0.90 (good fit), and AGFI value was 0.87 (acceptable fit). The NFI value is 0.93 (good fit), the NNFI value is 0.95 (perfect fit), the CFI value is 0.96 (perfect fit), and the RMSEA value is 0.077 (good fit) (Kline Reference Kline2015).
The standardized path coefficients are shown in Figure 1. Individual values were found to have a direct and negative significant effect on the total score of MD (β = −2.37, p < 0.01), intensity (β = −0.70, p < 0.01), and frequency (β = −0.58, p < 0.01). This shows that the increase in individual values decreases the total score, intensity, and frequency of MD. Professional values, on the other hand, had a direct positive and significant effect on the total score (β = 1.40, p < 0.05), intensity (β = 0.37, p < 0.05), and frequency (β = 0.25, p < 0.05) of MD. These results show that the increase in professional values increases the total score, intensity, and frequency of MD.
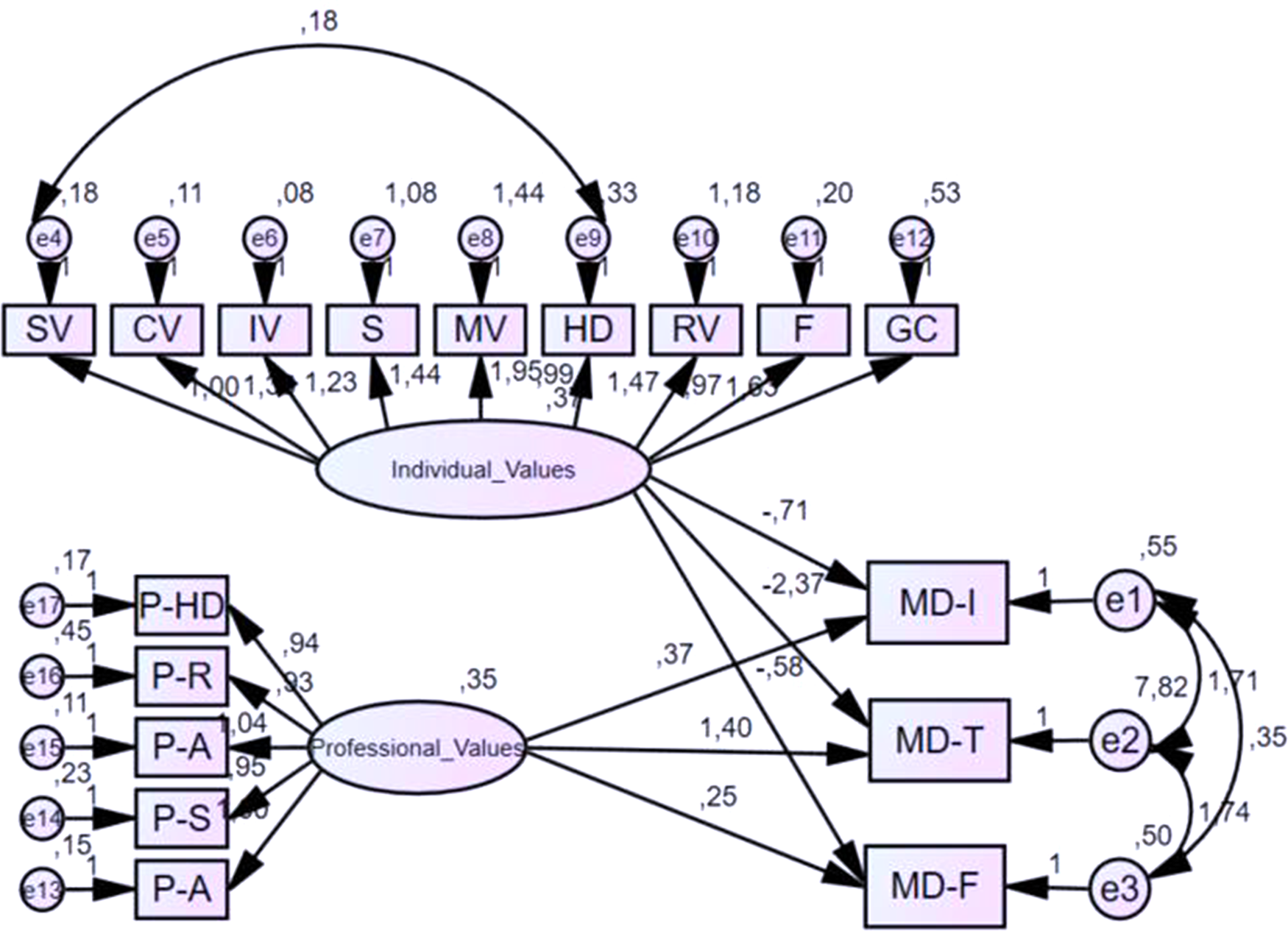
Fig. 1. The path coefficient of the effect of professional and individual values on moral distress.
MD-T, moral distress total score; MD-I, moral distress intensity score; MD-F, moral distress frequency score; SV, social values; CV, career values; IV, intellectual values; S, spirituality; MV, material values; HD, human dignity; RV, romance values; F, freedom; GC, generosity and courage; P-HD, professional human dignity; P-R, professional responsibility; P-A, professional activism; P-S, professional security; and P-A, professional autonomy.
Discussion
This study, which examined the relationship between MD and values in oncology nurses, obtained important data on the frequency and intensity of the MD experienced by oncology nurses and how these relate to their individual and professional values. This section will first discuss the descriptive statistical results of oncology nurses in terms of their MD experiences and then look at the relational results of the study.
The MD frequency of oncology nurses was found to be low (1.6 ± 0.7) and their intensity, moderate (1.9 ± 0.8). While most of the studies carried out in the fields of pediatrics, intensive care, surgery, emergency medical services, and similar departments have found low to moderate MD frequency and intensity (Burns et al. Reference Burns, Fox-Robichaud and Lorens2019; Karagozoglu et al. Reference Karagozoglu, Yildirim and Ozden2017; Lazzari et al. Reference Lazzari, Terzoni and Destrebecq2019; Meziane et al. Reference Meziane, Ramirez-Garcia and Fortin2018), a number of current studies conducted with oncology nurses have reported different results. For example, Fruet et al. (Reference Fruet, Dalmolin and Barlem2018), in their study conducted in Brazil, reported low MD frequency and moderate intensity among nurses, while Ameri et al. (Reference Ameri, Safavibayatneed and Kavousi2016) reported high MD frequency and intensity levels in their study with oncology nurses conducted in Iran.
It is known that the MD experienced by nurses can vary according to many variables, such as culture, values, current health system, and nature of the service provided (Soleimani et al. 2016). Studies conducted with oncology nurses also have reported there to be various factors responsible for MD (Fruet et al. Reference Fruet, Dalmolin and Barlem2018; Pergert et al. Reference Pergert, Bartholdson and Blomgren2018). In examining the results of studies on the causes of MD in oncology nurses, the study by Fruet et al. (Reference Fruet, Dalmolin and Barlem2018) reported the primary cause to be disregard for patient autonomy and the second cause to be having to work with incompetent team members in Brazil. Similarly, Pergert et al. Reference Pergert, Bartholdson and Blomgren2018 reported in their study conducted in Sweden that the chief causes were lack of competence and failure to provide continued care. These causes of MD as experienced by nurses can be combined to form a general category designated as “feelings of insufficiency to provide optimal care.” Ozbas et al. (Reference Ozbas, Kovanci and Koken2021) in a study which analyze MD causes of oncology nurses in Turkey found that oncology nurses face ethical problems in providing the quality and continuity of care they desire.
In the current study, the items “Conduct tests and treatments which I consider unnecessary upon the physician’s orders” and “Start extensive lifesaving actions which I think only prolong dying process” received the highest scores (Table 2). It was further seen that the item, “Continue to take part in the care of a hopelessly ill person who is being sustained on a ventilator in case there is no one to make a decision to withdraw support,” got a relatively high score compared to that of other items. It is noteworthy that these items are associated with the end-of-life issue, which is an important issue also in palliative care. The lack of do-not-resuscitate (DNR) practices in Turkey forces nurses to take part in the futile treatment and advanced life support applications, which explains the experience of MD in these situations. Dinçer, in his 2019 study, reported on the problems related to the lack of DNR practices and futile treatment, as experienced by health-care professionals working in the field of palliative care (Dincer Reference Dincer2019). Similarly, a study also found that futile treatment and lack of regulation for DNR are reasons for MD in oncology nurses (Ozbas et al. Reference Ozbas, Kovanci and Koken2021).
In the current study, it was seen that the nurses’ NPVS subdimension scores were very similar and relatively high (Table 3). In studies conducted with different groups in Turkey, the professional values of nurses were found to be at high levels (Cetinkaya-Uslusoy et al. Reference Cetinkaya-Uslusoy, Paslı-gurdogan and Aydınlı2017; Kaya and Kantek Reference Kaya and Kantek2016). Kaya and Kantek (Reference Kaya and Kantek2016) found in their study conducted in Turkey that while the professional values of the participants were high, no one value stood out from the others. It is believed that the similarity of professional values in the current study was due to the fact that the included nurses had a very homogeneous structure in terms of culture, religion, language, and socioeconomic level and had been working together in the same health system and institution for a long time. As emphasized in the literature, values can be learned directly or indirectly by observing the behavior of others (Poorchangizi et al. Reference Poorchangizi, Borhani and Abbaszadeh2019). The professional values of nurses also change after nursing education. In performing their profession after completing their academic education, nurses are affected by the health-care environments they are in, their colleagues, the values of the institution, and the unique situations they face (Poorchangizi et al. Reference Poorchangizi, Borhani and Abbaszadeh2019).
When the individual values of the oncology nurses were examined, it was observed that they achieved high, above-average scores in all the subdimensions of values, with the highest scores being in the subdimensions of human dignity, social values, intellectual values, and Freedom, in respective order (Table 3). Different results can be seen in studies conducted with nursing students and professional nurses. Hadid et al. (Reference Hadid, Malul and Khatib2019) reported in their study conducted in Israel that the participant’s individual values were benevolence, universalism, achievement, and security. It is believed that this difference seen in the studies from the literature is due to the nature of the concept of value, which differs according to culture, person, etc., and may change over the course of time within the same language, religion, and culture and be affected by individual factors.
The examination of the MD experiences and professional values of the oncology nurses showed there to be no relationship between the NPVS and MDS scores. A weak negative relationship was observed between MD experiences and almost all individual value subdimension scores and MDS scale scores. In the literature review, the only study examining the relationship between MD and values was one by Krautscheid et al. (Reference Krautscheid, DeMeester and Orton2017), which was conducted with nursing students. In this said study, a brief written narrative describing clinical situations contributing to MD was presented, along with content analysis to identify themes of distressing clinical situations, and from these, the conflict between individual values and professional values was emphasized. However, the only value to emerge as a theme was “human dignity.” In the current study, the subdimension with the highest score was also human dignity, but a relatively weaker relationship was observed between this value and MD (Table 3). This can be explained by the fact that human dignity emerged as 2 subthemes in the study by Krautscheid et al., namely, patient dignity and one’s own dignity. In the current study, the concept of human dignity, as part of the professional values of the participants, may have been perceived as disrespect for the dignity of the patient (incivility) and as disrespect to their own dignity in individual values (Krautscheid et al. Reference Krautscheid, DeMeester and Orton2017).
According to structural equation analysis, while individual values were found to have a direct and negative significant effect on MD, professional values had a direct positive and significant effect on MD. Consequently, while the first hypothesis of the study was confirmed, the second hypothesis was rejected. In the literature, there is not enough evidence-based data to discuss the results of the present study as they relate the relationship between professional and individual values and MD. Studies examining the relationship between the concepts possibly associated with MD are similarly very limited but could be interpreted as supporting the conclusion of our study that high professional values are associated with high MD. Kaya et al., in their study carried out in 2016 in Turkey, examined the relationship between the nurses’ values and the concepts of job satisfaction and intention to quit, both of which are known to be closely related to MD (Kaya and Kantek Reference Kaya and Kantek2016). Considering that information derived from the literature indicated there to be a positive relationship between MD and intention to quit, a negative relationship between professional values and MD was expected (Dyo et al. Reference Dyo, Kalowes and Devries2016). On the other hand, the other important result of the study is that high individual values have a direct and negative significant effect on MD. This result can explain the ethical competency concept of Corley’s MDT (Corley Reference Corley2002). In conflict situations where individual values come into play, nurses with higher personal values may experience less MD because they feel ethical competence (Schaefer and Vieira Reference Schaefer and Vieira2015).
Health care contains many ethical and moral factors that can trigger individual and professional values. It is not possible to completely eliminate these factors. However, there are solutions for healthcare professionals to be less affected by these situations. Moral resilience, which has been the center of interest in recent years, gains importance at this point as well. A theoretical framework for moral resilience has been developed by Rushton. The individual and relational integrity domains included in this theoretical framework directly point to value conflicts, individual and professional values (Heinze et al. Reference Heinze, Hanson and Holtz2021; Rushton Reference Rushton2018). It can be said that this theoretical structure developed by Rushton supports our study results. Therefore, individual and professional values can become a component that can affect individuals’ moral resilience capacities.
The relationship between MD and burnout and intention to leave has been revealed by various studies (Ajoudani et al. Reference Ajoudani, Baghaei and Lotfi2019; Carletto et al. Reference Carletto, Ariotti and Garelli2022; Karakachian and Colbert Reference Karakachian and Colbert2019). In the light of the findings of this study, it is recommended to focus on studies aimed at reducing MD in intervening with the sustaining nurse workforce problems, which is a global issue, which is gradually deepening with the effect of the Covid-19 pandemic, and to include individual and professional values in these studies.
Conclusion
To summarize, this study determined that the frequency of MD in oncology nurses was low and their insensitivity was moderate. The nurses received relatively high scores on both the individual and professional values scales, but there was no one value that stood out from the rest. While individual values were found to have a direct and negative significant effect on MD, professional values had a direct positive and significant effect on MD.
Based on these results, more national and international studies are needed to examine the relationship between MD concept and values. Given the highly subjective and personal nature of the concept of value, it is recommended that studies apply qualitative designs to examine this topic.
Limitations of the study
The fact that only one institution allowed the study to be conducted limited the sample size. Future studies may be conducted in a larger and heterogeneous study population and multicenter. In addition, study variables were measured using scales that tend to provide only limited information. Therefore, qualitative studies are needed to improve our understanding of the current findings. Moreover, study data were collected just before the Covid-19 pandemic emerged. Undoubtedly, the pandemic has had temporary and permanent effects on the values and lives of nurses.
Acknowledgments
The authors would like to thank all participants in this study.
Conflicts of interest
None declared.





 Open access
Open access