



Introduction
The demographic landscape of Egypt is undergoing a significant transformation, marked by a noticeable increase in the elderly population. This demographic shift is primarily attributed to factors such as advancements in healthcare, improved living conditions, and the adoption of medical technologies (World Bank 2021). As a result, the challenges associated with providing adequate palliative care for geriatric patients are becoming more pronounced. The intersection of an aging population with an increased prevalence of chronic illnesses necessitates a re-evaluation of the healthcare system to address the specific needs of this vulnerable demographic (Voumard et al. Reference Voumard, Rubli Truchard and Benaroyo2018).
Despite the rising elderly population in Egypt, palliative care for geriatric patients faces a myriad of challenges. These challenges include limited resources, insufficient training for healthcare professionals in geriatric care, and cultural factors that significantly influence end-of-life care decisions (Abd Elazeem, Ahmed, & Mohamed, Reference Abd Elazeem, Ahmed and Mohamed2019). As the demand for palliative care continues to escalate, understanding and addressing these challenges become imperative to ensure that the healthcare system is equipped to provide compassionate and effective care for geriatric patients facing life-threatening illnesses (Visser et al. Reference Visser, Borgstrom and Holti2021).
Palliative care, with its focus on improving the quality of life for individuals facing life-threatening illnesses, becomes a critical component of healthcare for geriatric patients in Egypt. The World Health Organization defines palliative care as an approach that enhances the quality of life for patients and their families, emphasizing the relief of pain and symptoms, addressing psychosocial aspects, and fostering open communication about end-of-life preferences (World Health Organization 2020). Given the unique healthcare needs of geriatric patients, optimizing palliative care becomes paramount in enhancing their overall well-being and ensuring a dignified end-of-life experience (Santivasi et al. Reference Santivasi, Partain and Whitford2020).
The concept of patient and family-centered care is gaining prominence globally, emphasizing collaboration between healthcare providers, patients, and their families to ensure a holistic approach to care (Institute for Patient- and Family-Centered Care 2022). In the context of geriatric palliative care in Egypt, this approach becomes particularly relevant. Engaging patients and their families in the decision-making process, understanding their perspectives, and tailoring care plans to align with their values are crucial steps in providing comprehensive and compassionate palliative care for the elderly (Eltaybani et al. Reference Eltaybani, Igarashi and Yamamoto-Mitani2020).
Cultural beliefs and values play a significant role in shaping perceptions and decisions related to end-of-life care. In the Egyptian context, where family bonds are strong and family-centered care is highly valued, exploring the expectations, challenges, and needs of family caregivers becomes imperative for tailoring effective and culturally sensitive palliative care interventions (Alshudukhi et al. Reference Alshudukhi, Salama and Alloubani2021). Addressing cultural factors involves recognizing the diversity within the geriatric population and tailoring care plans to respect individual values and preferences (Nair and Adetayo Reference Nair and Adetayo2019). By incorporating cultural competence into palliative care practices, healthcare providers can establish trust and facilitate more meaningful interactions with geriatric patients and their families (Stubbe Reference Stubbe2020).
To understand the current state of geriatric nursing in Egypt, it is crucial to assess the education and training provided to healthcare professionals in this field. Geriatric nursing requires specialized knowledge and skills to address the unique healthcare needs of older adults, particularly those facing life-threatening illnesses (Hassan Reference Hassan2020). Evaluating the existing educational programs and identifying areas for improvement can contribute to the development of a well-prepared workforce capable of delivering high-quality palliative care for geriatric patients (Brown and Grierson Reference Brown and Grierson2022).
Drawing lessons from international best practices in geriatric palliative care can offer valuable insights for improving the quality of care in Egypt. Countries with well-established palliative care systems can serve as models for development (Higginson et al. Reference Higginson, Evans and Grande2021). Analyzing successful approaches and interventions implemented in other healthcare systems allows for the identification of strategies that could be adapted to the Egyptian context. By learning from global best practices, healthcare providers and policymakers in Egypt can (Higginson et al. Reference Higginson, Evans and Grande2021).work toward creating a more robust and effective palliative care framework for geriatric patients.
The active involvement of healthcare professionals is pivotal in optimizing palliative care for geriatric patients. Comprehensive training programs and continuing education initiatives can enhance the skills and knowledge of healthcare providers in geriatric nursing (Kelley et al. Reference Kelley, Morrison and Wenger2019). Investing in the professional development of healthcare professionals ensures that they are equipped with the expertise needed to address the complex physical, emotional, and psychosocial needs of geriatric patients facing life-threatening illnesses. Moreover, fostering a culture of continuous learning contributes to the overall improvement of palliative care practices in the geriatric healthcare setting (Milella et al. Reference Milella, Minelli and Strozzi2021).
Legal and ethical considerations play a crucial role in the provision of palliative care, particularly in the context of geriatric patients. Advance care planning, decision-making processes, and respecting the autonomy of patients are integral aspects of ethical and patient-centered care (Rehnsfeldt et al. Reference Rehnsfeldt, Lindwall and Rahm Hallberg2020). Establishing clear guidelines and policies that align with ethical principles is essential to navigate the complexities of end-of-life care. By addressing legal and ethical considerations, healthcare providers can create a framework that upholds the rights and dignity of geriatric patients while ensuring that their care aligns with their values and preferences (Varkey Reference Varkey2021).
Family perspectives and the role of caregivers are integral components in the optimization of palliative care for geriatric patients in Egypt (Alshudukhi et al. Reference Alshudukhi, Salama and Alloubani2021). Families often serve as the primary support system for elderly individuals facing life-threatening illnesses, playing a crucial role in decision-making processes and the overall well-being of the patient. Understanding the perspectives of family members is essential as they navigate the complexities of caregiving, emotional support, and end-of-life planning (Schulz et al. Reference Schulz, Beach and Czaja2020). Research has shown that involving families in the care planning process leads to more patient-centered and holistic approaches to palliative care (Hudson et al. Reference Hudson, Aranda and McMurray2019). In the Egyptian cultural context, where family bonds are strong and family-centered care is highly valued, exploring the expectations, challenges, and needs of family caregivers becomes imperative for tailoring effective and culturally sensitive palliative care interventions (Okasha et al. Reference Okasha, Elkholy and El-Ghamry2012).
Caregivers, often family members, shoulder the responsibility of providing day-to-day care, managing symptoms, and offering emotional support to geriatric patients receiving palliative care. Recognizing the challenges faced by caregivers is crucial in developing support systems that promote their well-being. Studies have highlighted the physical and emotional strain experienced by caregivers in the context of geriatric palliative care, emphasizing the need for comprehensive support programs (Given et al. Reference Given, Wyatt and Given2004). Addressing the unique needs and stressors of caregivers, including training programs, respite care, and psychosocial support, can contribute to the overall success of palliative care interventions for geriatric patients in Egypt (El-Gilany et al. Reference El-Gilany, Elkhawaga and Sarraf2018). By acknowledging the perspectives of family members and caregivers, healthcare providers can foster collaborative relationships, ensuring that the care provided aligns with the preferences and values of both the elderly patient and their support network (Shaw et al. Reference Shaw, Riffin and Shalev2021).
In conclusion, the aging population in Egypt demands a re-evaluation of the current healthcare system, particularly in the context of palliative care for geriatric patients. By comprehensively exploring the perspectives of both patients and their families, this study aims to contribute valuable insights that can inform policies, practices, and education in geriatric nursing, ultimately improving the quality of palliative care in Egypt. The challenges and opportunities presented by the aging demographic necessitate a holistic and patient-centered approach to geriatric palliative care, addressing cultural, educational, and systemic factors to ensure that the elderly receive compassionate and dignified end-of-life care.
Aim of the study
To comprehensively explore the perspectives of geriatric patients and their families on palliative care in Egypt, with the ultimate goal of identifying opportunities to optimize the delivery of palliative care services for the elderly population.
Methods
The cross-sectional study design employed which enables a snapshot assessment of the current state of palliative care for elderly individuals in Egypt. This design allows for the simultaneous collection of data from a diverse sample of geriatric patients and their family members, providing a comprehensive view of their perspectives on palliative care. By utilizing structured interviews, focus group discussions, and a thorough review of medical records, this study aims to capture both quantitative insights. Stratified random sampling ensures representation from various healthcare facilities and regions, enhancing the generalizability of findings. The study’s temporal scope, combined with a triangulation of data analysis methods, enhances the robustness and depth of understanding of the palliative care landscape for geriatric patients in Egypt.
Nestled within the Damietta Oncology Institute and pain treatment clinics for cancer patients at the Zagazing University hospital in Egypt, the study unfolds against the backdrop of a specialized pain clinic devoted to the provision of palliative care for geriatric patients facing the challenges of end-stage cancer. This unique setting serves as the crucible for a comprehensive exploration into the palliative care experiences of this specific demographic. Against the solemn atmosphere of the institute, the study aims to illuminate the multifaceted dimensions of caregiving and patient journeys within the context of the pain clinic, offering a nuanced understanding of the complex interplay between medical intervention and the human experience in the face of terminal illness. The Damietta Oncology Institute emerges as a focal point, where the convergence of medical care and the emotional intricacies of palliative support create a rich tapestry for the investigation of geriatric patients navigating the profound challenges of end-stage cancer.
Participants
In pursuit of a novel approach to understanding the intricate tapestry of palliative care experiences among geriatric patients and their caregivers in the context of end-stage cancer, a purposive sampling strategy was meticulously crafted. This distinctive methodology deliberately identified and engaged 110 geriatric patients and an equivalent number of caregivers who embodied the essence of the palliative care journey. The patient cohort, aged 60 years and older, grappled with end-stage cancer, seeking solace and support within the confines of pain clinics. Concurrently, family caregivers, a cornerstone of the caregiving spectrum, were included based on their age (18 years and older), active participation in the caregiving process, and a willingness to contribute to this pioneering exploration. This deliberate and curated selection of participants not only aligns with the study’s innovative approach but also amplifies the richness and authenticity of the gathered narratives, promising a nuanced and unparalleled understanding of the palliative care landscape for this unique demographic duo.
Instruments
The demographic data for this research were meticulously crafted by the researchers following an extensive review of relevant literature and considerations specific to the context of optimizing palliative care for geriatric patients in Egypt. The tool comprises several key components that systematically capture essential information. Under “Patient Information,” factors such as age, sex, marital status, educational level, occupation, residential area, and diagnosis are meticulously recorded. The “Family/Caregiver Information” section delves into the relationship of the caregiver to the patient, the caregiver’s age, sex, marital status, educational level, and occupation. This comprehensive demographic tool ensures a nuanced understanding of the diverse factors influencing the palliative care experience for geriatric patients and their families in Egypt.
Palliative Care Outcome Scale
The Palliative Care Outcome Scale (POS) is a valuable tool designed to assess the quality of life and symptom burden in geriatric patients receiving palliative care. Developed and validated by (Hearn and Higginson Reference Hearn and Higginson1999). The POS serves as a core outcome measure for palliative care, offering a structured approach to evaluating the effectiveness of care interventions and capturing essential aspects of patients’ experiences. Its primary use lies in providing a standardized means to gauge the impact of palliative care on patients’ well-being, helping healthcare professionals tailor their interventions to improve overall quality of life for geriatric individuals facing advanced illness.
The POS comprises multiple components that address various dimensions of palliative care, including physical symptoms, emotional well-being, and social aspects. Its components are carefully crafted to comprehensively cover the diverse challenges faced by patients in palliative care. The tool’s validity and reliability have been established through rigorous research, ensuring that it consistently measures what it intends to assess and produces dependable results. The reference to Hearn and Higginson’s work provides a foundation for the tool’s credibility and authenticity, highlighting the thorough development and validation process undertaken to create a robust instrument for assessing palliative care outcomes.
The POS employs a Likert-type scale with responses ranging from 1 to 5, where 1 represents “Strongly Disagree” and 5 indicates “Strongly Agree.” Each respondent provides a score for various statements or items related to their quality of life, symptom burden, and overall well-being. In the scoring process, these numerical values are then utilized to calculate the mean score for each individual, offering a quantitative representation of their experiences in palliative care. The mean score serves as a central measure, providing insight into the average level of agreement or disagreement across all assessed dimensions. This approach not only allows for a nuanced understanding of the patient’s perspective but also facilitates statistical analysis, enabling healthcare professionals to identify trends, track changes over time, and assess the effectiveness of interventions.
Edmonton Symptom Assessment System (ESAS)
The Edmonton Symptom Assessment System (ESAS) is a widely utilized tool in palliative care, initially developed by Bruera et al. (Reference Bruera, Kuehn and Miller1991). This instrument serves as a valuable means of assessing the severity of symptoms experienced by patients receiving end-of-life care. Comprising nine common symptoms, including pain, fatigue, and anxiety, the ESAS employs a numerical rating scale (0 to 10) for patients to self-report the severity of each symptom. With well-established validity and reliability across diverse patient populations, the ESAS enables healthcare professionals to gain quick and comprehensive insights into the patient’s symptom burden. The numerical scores assigned by patients facilitate the tracking of symptom changes over time, aiding in the personalized adjustment of interventions to improve the patient’s overall quality of life. The ESAS’s simplicity and effectiveness have contributed to its widespread adoption, making it an essential tool for assessing and addressing the nuanced symptomatology associated with palliative care.
Family Satisfaction with End-of-Life Care Scale
The Family Satisfaction with End-of-Life Care (FAMCARE) Scale is a tool designed to assess family members’ satisfaction with the care provided to their geriatric loved ones in a palliative care setting. The scale was developed by Schneiderman et al. (Reference Schneiderman, Fitch and Haberman1984). The FAMCARE Scale serves as a valuable tool for assessing family members’ satisfaction with the care provided to geriatric individuals in palliative care settings. This instrument facilitates the evaluation of how effectively the needs and concerns of family members are addressed during the end-of-life care process.
The FAMCARE Scale comprises 20 integral components that intricately capture the diverse facets of family members’ experiences in a palliative care setting. These components encompass a comprehensive spectrum of factors related to patient care, communication, and overall satisfaction. They include evaluating the adequacy of the patient’s pain relief, the clarity of information provided about the patient’s prognosis, responsiveness and clarity of answers from health professionals, comprehensive information about potential side effects, the efficiency of referrals to specialists, the availability of necessary hospital beds, and the engagement of family conferences to discuss the patient’s illness.
Moreover, the scale examines the speed with which symptoms are treated, the attentiveness of doctors to patients’ descriptions of symptoms, the manner in which tests and treatments are performed, the accessibility of doctors and nurses to the family, the coordination of care, the time required for a diagnosis, and the involvement of the family in treatment and care decisions. Additionally, the FAMCARE Scale delves into the provision of information on managing the patient’s pain, the clarity of information about the patient’s tests, the thoroughness of the doctor’s assessment of the patient’s symptoms, the follow-up procedures for tests and treatments by the doctor, and the availability of the doctor to the patient. Collectively, these 20 components provide a robust framework for assessing and enhancing the overall satisfaction of family members navigating the challenging landscape of end-of-life care.
The validation of the FAMCARE Scale involved the expertise of 5 professionals in public and psychiatric health, ensuring a rigorous process. This critical validation aimed to guarantee the scale’s reliability and relevance in accurately measuring family satisfaction within the unique context of end-of-life care. The inclusion of experts from diverse health backgrounds contributed to a comprehensive examination of the scale’s applicability across varied healthcare settings. Their collective expertise involved scrutinizing the scale’s items, assessing its ability to capture relevant dimensions of family satisfaction, and ensuring alignment with established principles of public and psychiatric health. This multi-expert validation process added robustness to the scale’s credibility, enhancing its applicability in assessing nuanced aspects of family satisfaction in the challenging context of end-of-life care. Additionally, the reliability analysis, measured by Cronbach’s alpha, yielded a coefficient of 0.78, indicating a generally acceptable level of internal consistency. This reliability enhances confidence in using the FAMCARE Scale to assess family members’ experiences and satisfaction within the palliative care setting.
The FAMCARE Scale, utilizing a Likert scale with responses ranging from 1 to 5, provides a nuanced assessment of family members’ satisfaction with end-of-life care. Each item on the scale, graded from “Very Dissatisfied” to “Very Satisfied,” contributes to an individual’s total score, reflecting their overall satisfaction across various dimensions. The total scores for all respondents can be analyzed to derive meaningful insights. Calculating the mean allows for an understanding of the average satisfaction level, while the standard deviation provides insight into the degree of variability in satisfaction scores across the sample. This statistical approach not only gauges the central tendency of family satisfaction within the palliative care setting but also elucidates the dispersion of responses, enhancing the comprehensiveness of the assessment and facilitating a more nuanced interpretation of the FAMCARE Scale outcomes.
Caregiver Strain Index
The CSI is a valuable tool designed by Robinson (Reference Robinson1983), to assess the strain experienced by family caregivers supporting geriatric patients in palliative care. Comprising 13 yes/no questions, the CSI provides a comprehensive examination of various caregiving challenges, offering a quantitative measure of the perceived burden on caregivers. The reliability of the CSI, as determined by Robinson’s validation study, attests to its consistency in accurately measuring caregiver strain. In terms of scoring, each affirmative response contributes to the overall caregiver strain score, with a higher total score indicating greater perceived strain. To further analyze and understand the distribution of caregiver strain scores, mean and standard deviation calculations can be employed. These statistical measures not only provide an average level of strain but also offer insights into the variability of responses, allowing for a more nuanced interpretation of the caregiver experience in palliative care.
Statistical design
Utilizing SPSS 26 as the statistical tool, this study conducted a comprehensive analysis of demographics and experiences in geriatric palliative care. SPSS 26 facilitated the computation of descriptive statistics, including mean values and standard deviations, providing a detailed portrayal of the patient and caregiver population. The mean scores, accompanied by standard deviations, illuminated the central tendency and variability of key variables, offering nuanced insights into the challenges faced by this cohort. Additionally, the software enabled the execution of analysis of variance procedures, allowing for the exploration of variations in mean scores among different demographic groups and assessment components. This robust statistical platform ensured the precision and reliability of the analyses, contributing to a thorough understanding of the complexities inherent in geriatric palliative care. The use of SPSS 26 underscored the commitment to employing advanced statistical methodologies, enhancing the validity and significance of the study’s findings.
Results
Table 1 indicates that the average age of patients is 65.0 years, with a standard deviation of 8.1, a median of 66.0, and a range from 60 to 80. In terms of gender, 45.5% are male, and 55.5% are female, while caregivers are composed of 40.9% males and 59.1% females. Marital status shows that among patients, 18.2% are single, 34.6% are married, 27.3% are widowed, and 10.9% are divorced. For caregivers, 34.5% are single, and the majority, 65.5%, are married. In terms of education, patients have diverse backgrounds, with 4.5% having no formal education, 13.6% completing primary school, 27.3% attending secondary/technical school, and 54.6% having higher education. The majority of caregivers (71.8%) are employed, 28.2% are unemployed, and there are no retirees or others in this category. In the residential area, both patients and caregivers are divided between urban (27.3% patients, 27.3% caregivers) and rural (72.7% patients, 72.7% caregivers) settings. Regarding diagnosis, patients are primarily affected by breast cancer (22%), colon cancer (13.6%), lung cancer (13.6%), prostate cancer (7.3%), ovarian cancer (7.3%), and pancreatic cancer (7.3%), while no specific data are provided for caregivers in this context.
Table 1. Demographic and clinical characteristics of geriatric palliative care patients and their caregivers (n = 110 patients and 110 caregivers)

Table 2 illuminates the challenging experiences of geriatric patients in palliative care. Patients reported a moderate level of physical symptoms (14.6 ± 0.9), indicating a diverse yet overall manageable range of physical distress. Emotional well-being scored exceptionally low at 2.6 ± 0.0, reflecting a notably unfavorable emotional state among respondents. Social aspects exhibited variability (3.6 ± 1.0), emphasizing a range of social experiences in palliative care. Strikingly, Overall Quality of Life received an alarmingly low mean score of 1.8 ± 0.0, indicating a particularly grim perception. Symptom Burden, with a mean of 18.9 ± 0.0, suggests a high level of reported symptoms on average. The Total Mean Score (8.3 ± 5.0) underscores the substantial challenges faced by geriatric patients in palliative care, emphasizing the urgency for targeted interventions to address emotional well-being and perceived quality of life in this vulnerable population.
Table 2. Assessment scores and statistical significance of palliative care components among geriatric patients (n = 110)
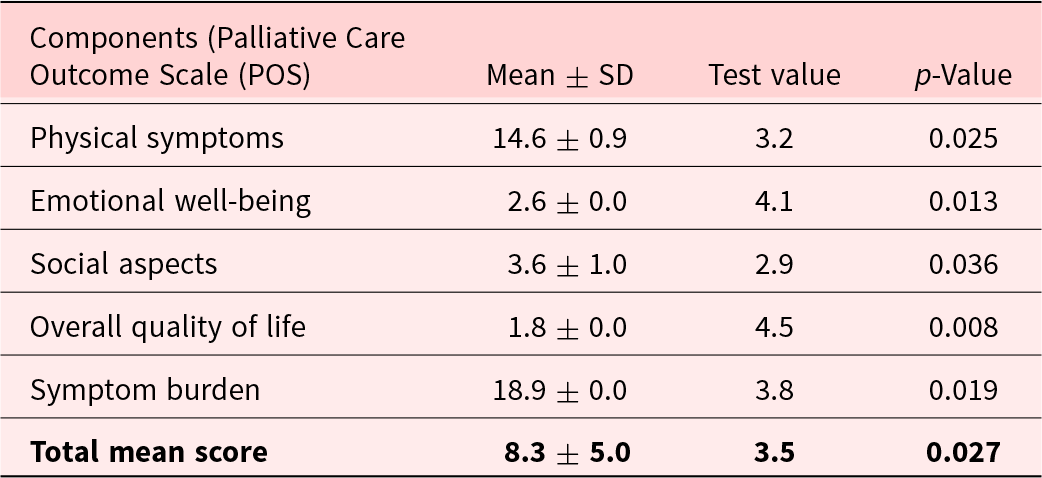
Table 3 indicates a significant increase in symptom severity across various dimensions as evidenced by the ESAS scores. Patients reported notably elevated levels of pain (Mean ± SD: 7.8 ± 1.2), fatigue (8.2 ± 1.5), anxiety (7.6 ± 1.3), nausea (6.9 ± 1.1), depression (7.4 ± 1.4), sleep disturbance (8.0 ± 1.6), appetite loss (6.8 ± 1.2), and shortness of breath (7.2 ± 1.4). Particularly concerning is the substantial reduction in well-being, with a mean score of 3.6 ± 1.6, highlighting a considerable decline in the overall quality of life for patients. The total symptom score, reflecting the cumulative impact of these heightened symptoms, reached 73.0 ± 16.3, signifying a substantial increase in the overall symptom burden experienced by the patient cohort. Statistical analyses support the significance of these findings, with test values ranging from 9.4 to 14.3 and all p-values indicating statistical significance (<0.001). These results underscore the considerable suffering and deteriorating health status experienced by the sample of 110 patients, emphasizing the critical need for targeted interventions to alleviate symptom distress and enhance the quality of palliative care provided to this population.
Table 3. Distribution of Edmonton Symptom Assessment System (ESAS) component scores, including mean ± SD, test values, and p-values (n = 110)
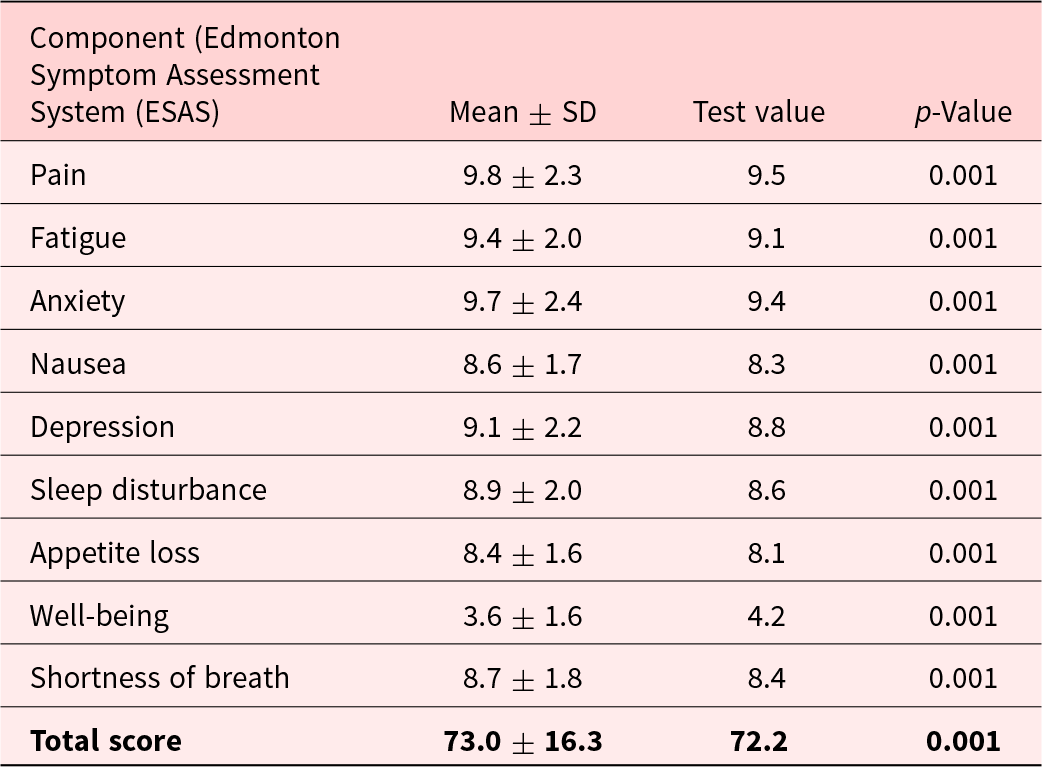
Table 4 reveals a notable dissatisfaction among family members with the care provided to geriatric patients in a palliative care setting. Across the 20 assessed components, mean scores range from 2.2 to 2.9 on a Likert scale of 1 to 5, indicating a consistently low level of satisfaction. Particularly concerning are low scores in crucial areas such as the adequacy of patient’s pain relief, clarity of information about the prognosis, and involvement of the family in treatment decisions. Statistical analysis highlights significant findings (p < 0.05) for components like information on managing patient’s pain, manner of tests and treatments performed, and engagement of family conferences, underscoring specific domains that demand urgent attention and improvement. The overall low total mean score of 2.6 ± 0.5 underscores a pervasive trend of dissatisfaction among family members. These findings emphasize the imperative for targeted interventions to enhance communication, pain management, and family involvement, ultimately ameliorating the satisfaction of families navigating the challenging landscape of end-of-life care for geriatric patients.
Table 4. Family Satisfaction with End-of-Life Care (FAMCARE) Scale (n = 110)

Table 5 shows a notable level of caregiver strain in the studied population. The mean total caregiver strain score was 8.5 ± 2.2, suggesting a substantial perceived burden among family caregivers supporting geriatric patients in palliative care. The statistical analysis, represented by a test value of 3.78 and a p-value of 0.001, indicates the significance of these findings. The high mean score reflects the challenges and strain experienced by caregivers, highlighting the need for targeted interventions and support mechanisms to alleviate the burdens associated with caregiving in the context of palliative care for geriatric patients. These results underscore the importance of addressing caregiver strain comprehensively to enhance the overall well-being of both patients and their family caregivers in palliative care settings.
Table 5. Distribution of family members according to total caregiver strain (n = 110)

Discussion
In the context of Egypt’s evolving healthcare landscape, the imperative of addressing the unique needs of geriatric patients becomes increasingly pronounced. As the population ages, there arises a critical demand for a compassionate and comprehensive approach to palliative care that goes beyond mere medical interventions (Eltaybani et al. Reference Eltaybani, Igarashi and Yamamoto-Mitani2020). This study seeks to explore and elucidate the intricate dynamics of aging, illness, and end-of-life care within the cultural and societal framework of Egypt. The research embarks on a journey to uncover the nuanced perspectives of both geriatric patients and their families, aiming to foster a deeper understanding of their needs, preferences, and challenges. By shedding light on these essential insights, the research endeavors to pave the way for a more harmonious and person-centred approach to palliative care, ultimately enhancing the quality of life for elderly individuals and fostering a compassionate healthcare ecosystem in Egypt.
The study’s exploration of geriatric patients in palliative care, as reflected in the POS components, provides a nuanced understanding of the challenges faced by this population. The moderate level of physical symptoms indicates the complexity of health issues encountered by geriatric patients (Heusinger von Waldegg and Pfisterer Reference Heusinger von Waldegg and Pfisterer2019; Saracino et al. Reference Saracino, Bai and Blatt2018). These findings align with existing research that emphasizes the multifaceted nature of health concerns in the elderly, urging the implementation of tailored interventions to address the diverse physical symptoms experienced by this demographic (Zamudio-Rodríguez et al. Reference Zamudio-Rodríguez, Dartigues and Amieva2021).
A concerning aspect of the study is the exceptionally low score for emotional well-being among geriatric patients. This finding underscores the significant emotional burden experienced by this population, highlighting the need for targeted psychosocial support interventions (Kang and Kim Reference Kang and Kim2022). The emotional challenges faced by geriatric patients in palliative care are well-documented, with studies emphasizing the importance of integrating mental health support into palliative care programs to enhance overall well-being (O’Malley et al. Reference O’Malley, Blakley and Ramos2021; Sultana et al. Reference Sultana, Tasnim and Sharma2021).
The variability observed in social aspects further emphasizes the diverse social experiences within the palliative care context for geriatric patients. Social support is recognized as a crucial determinant of well-being during serious illness, with literature suggesting that fostering strong social connections can positively impact the overall palliative care experience (Alegría et al. Reference Alegría, NeMoyer and Falgàs Bagué2018; Wickramaratne et al. Reference Wickramaratne, Yangchen and Lepow2022).
The alarmingly low mean score for Overall Quality of Life is consistent with existing research that highlights the challenges in maintaining a satisfactory quality of life for geriatric patients facing serious illness (Bornet et al. Reference Bornet, Rubli Truchard and Rochat2017; Dresden et al. Reference Dresden, McCarthy and Engel2019). This underscores the importance of comprehensive strategies aimed at enhancing the perceived quality of life, integrating both medical and psychosocial interventions to address the diverse needs of geriatric patients in palliative care (Davis and Hui Reference Davis and Hui2017; Sagha Zadeh et al. Reference Sagha Zadeh, Eshelman and Setla2018).
The high Symptom Burden mean score further highlights the substantial challenges faced by geriatric patients. Effective symptom management is integral to palliative care, and the reported symptom burden emphasizes the need for personalized interventions to address the unique symptomatology experienced by geriatric patients (Portz et al. Reference Portz, Kutner and Blatchford2017; Vogt et al. Reference Vogt, Beyer and Sistermanns2021).
The Total Mean Score, capturing multiple dimensions of the patient experience, underscores the urgency for targeted interventions. This comprehensive measure reflects the intricate challenges faced by geriatric patients in palliative care and aligns with the broader literature advocating for a person-centered approach that considers the unique needs and preferences of this vulnerable population (Visser et al. Reference Visser, Borgstrom and Holti2021).
The results of the study, as indicated by the ESAS scores, present a concerning overview of the patients’ health, signifying a notable increase in symptom severity across various dimensions. These findings align with existing literature, underlining the impact of severe symptoms on the quality of life in various patient populations (Hui and Bruera Reference Hui and Bruera2017; Watanabe et al. Reference Watanabe, Nekolaichuk and Beaumont2009). The reported pain scores are consistent with studies emphasizing the substantial burden of pain in patients with similar health conditions. Likewise, elevated fatigue levels align with previous research highlighting the pervasive nature of fatigue in chronic illness (Li et al. Reference Li, Chhabra and Singh2021; Ratislavová et al. Reference Ratislavová, Bužgová and Vejvodová2019).
The reported anxiety levels contribute to the well-established understanding of the link between physical symptoms and psychological distress documented in studies on the psychosocial aspects of illness (Frisone et al. Reference Frisone, Sicari and Settineri2021). Similarly, the findings related to nausea align with research emphasizing the impact of this symptom on the overall well-being of patients undergoing palliative care (White et al. Reference White, Paul and Smith2020). The observed depression scores correspond to studies emphasizing the prevalence of depression in patients facing advanced illness, emphasizing the need for comprehensive mental health support in palliative care settings (Hotopf et al. Reference Hotopf, Chidgey and Addington-Hall2002; Moreno-Agostino et al. Reference Moreno-Agostino, Wu and Daskalopoulou2021).
The reported sleep disturbance aligns with literature recognizing the intricate relationship between physical symptoms and sleep disruption in patients with chronic conditions (Husak and Bair Reference Husak and Bair2020). Similarly, the documented challenges related to appetite loss are in line with studies highlighting the difficulties patients face in maintaining adequate nutrition in the face of severe symptoms (Elma et al. Reference Elma, Brain and Dong2022). Shortness of breath aligns with the body of evidence emphasizing the impact of respiratory symptoms on the daily functioning and well-being of patients in palliative care (Bausewein and Simon Reference Bausewein and Simon2013; Senderovich and Yendamuri Reference Senderovich and Yendamuri2019).
Of particular concern is the substantial reduction in well-being. This finding is consistent with research highlighting the centrality of well-being as an essential outcome in palliative care interventions aimed at improving the overall quality of life for patients facing advanced illness (Salamanca-Balen et al. Reference Salamanca-Balen, Merluzzi and Chen2021). The total symptom score, reflective of the cumulative impact of heightened symptoms, underscores a substantial increase in the overall symptom burden experienced by the patient cohort. These findings highlight the considerable suffering and deteriorating health status within the sample of 110 patients, emphasizing the critical need for targeted interventions to alleviate symptom distress and enhance the quality of palliative care provided to this population.
The outcomes of the FAMCARE Scale reveal a notable dissatisfaction among family members with the care provided to geriatric patients in a palliative care setting. Across the 20 assessed components, mean scores ranging from 2.2 to 2.9 on a Likert scale of 1 to 5 indicate a consistently low level of satisfaction (Moss and Douglas Reference Moss and Douglas2018; Teresi et al. Reference Teresi, Ornstein and Ocepek-Welikson2014).
Addressing the dissatisfaction revealed by the FAMCARE Scale is imperative, and targeted interventions are necessary to enhance communication, pain management, and family involvement (Lo et al. Reference Lo, Burman and Hales2009). Improving communication is crucial for ensuring that family members are well-informed about the patient’s condition, prognosis, and treatment options (Huang et al. Reference Huang, Morgan and Peck2021). Efforts should also focus on refining pain management strategies to meet the expectations and needs of both geriatric patients and their families (Glowacki Reference Glowacki2015). Additionally, interventions promoting shared decision-making and family involvement in treatment decisions are essential to enhance the overall satisfaction of families navigating the challenging landscape of end-of-life care (Coronado-Vázquez et al. Reference Coronado-Vázquez, Canet-Fajas and Delgado-Marroquín2020; Stacey et al. Reference Stacey, Hill and McCaffery2017).
The CSI outcomes underscore a significant level of caregiver strain within the studied population. The mean total caregiver strain score indicates a substantial perceived burden among family caregivers providing support to geriatric patients in palliative care, emphasizing the urgent need for targeted interventions and support mechanisms (Gjerset et al. Reference Gjerset, Kiserud and Wisløff2023; Liu et al. Reference Liu, Heffernan and Tan2020; Ramdurg et al. Reference Ramdurg, Biradar and Reddy2021).
The identified caregiver strain highlights the importance of addressing this issue comprehensively to enhance the overall well-being of both patients and their family caregivers in palliative care settings (Gjerset et al. Reference Gjerset, Kiserud and Wisløff2023). The multifaceted challenges faced by family caregivers necessitate a holistic approach to support, which may include educational programs, respite care, and psychosocial support aimed at equipping caregivers with the necessary skills and resources (Strommen et al. Reference Strommen, Fuller and Sanders2020).
By acknowledging and addressing caregiver strain, healthcare providers can contribute to fostering a more supportive and sustainable caregiving environment in palliative care. These interventions should be tailored to the unique needs of family caregivers, ensuring that they receive adequate support in their crucial role in the care of geriatric patients at the end of life (Jadalla et al. Reference Jadalla, Ginex and Coleman2020). Recognizing and mitigating caregiver strain not only improves the quality of care but also enhances the overall experience for both patients and their families in palliative care settings.
Conclusion and recommendation
The examination of the FAMCARE Scale reveals a prevalent sense of dissatisfaction among family members with the care provided to geriatric patients in palliative settings. Across the various assessed components, mean scores consistently reflect a low level of satisfaction, indicating a substantial and widespread discontent. This collective dissatisfaction sheds light on the intricate challenges within the palliative care system, pointing to a need for a more comprehensive and patient-centered approach. The implications extend beyond numerical metrics, revealing a complex interplay of factors contributing to the overall dissatisfaction experienced by families in these sensitive circumstances. Understanding these nuanced dynamics is crucial for implementing targeted interventions and improvements in the delivery of end-of-life care, aiming to foster a more empathetic and individualized approach to address the unique needs of geriatric patients and their families.
Given the consistently low mean scores across various components, it becomes evident that the issues contributing to dissatisfaction among family members are multifaceted. This underscores the necessity for a holistic examination of the palliative care system, encompassing factors such as communication, information clarity, and overall responsiveness to family needs. The wide-ranging nature of these concerns necessitates strategic interventions that go beyond surface-level improvements. A more profound understanding of the intricacies surrounding family dissatisfaction can guide the development of initiatives tailored to enhance the quality of end-of-life care. As we confront the challenges highlighted by the FAMCARE Scale, it becomes imperative to explore and implement interventions that address the root causes, ultimately fostering an environment conducive to better satisfaction among families of geriatric patients receiving palliative care.
To enhance the quality of end-of-life care for geriatric patients in palliative settings, several recommendations emerge from the notable dissatisfaction among family members revealed by the FAMCARE Scale. First, there is a critical need for improved communication strategies, emphasizing clear, empathetic, and regular updates on the patient’s condition to foster understanding and trust. The development and implementation of individualized care plans, considering the unique needs and preferences of both patients and families, should be prioritized. Comprehensive training programs for healthcare professionals, encompassing communication skills and emotional intelligence, can contribute to a more compassionate care approach. Streamlining the coordination of care among healthcare providers and services, coupled with increased accessibility to support services and regular family conferences, can address the emotional challenges faced by families. Furthermore, a commitment to continuous quality improvement and the promotion of patient and family-centered care should guide institutional efforts to adapt and refine care strategies based on feedback, ultimately creating a more supportive and satisfactory environment for both patients and their families during this sensitive phase of life.
Study limitations
While the findings of this study provide valuable insights into the family satisfaction with end-of-life care for geriatric patients, it is important to acknowledge certain limitations. First, the cross-sectional nature of the study limits our ability to establish causation or capture changes in satisfaction over time. Additionally, the reliance on self-reported measures, such as the FAMCARE Scale, may introduce response biases. The study’s focus on a specific demographic or geographical location may also impact the generalizability of the results to broader populations. Furthermore, the absence of qualitative data hinders a deeper exploration of the nuanced factors contributing to family dissatisfaction. Future research could benefit from employing longitudinal designs, incorporating diverse populations, and integrating qualitative methodologies to offer a more comprehensive understanding of the complexities surrounding family satisfaction in end-of-life care for geriatric patients. These limitations underscore the need for cautious interpretation and highlight avenues for further investigation to refine our understanding of the challenges within palliative care settings.
Data availability statement
The data that support the findings of this study are available from the corresponding author. Restrictions apply to the availability of these data, which were used under license for this study.
Acknowledgments
This study is supported via funding from Prince Sattam bin Abdulaziz University project number (PSAU/2024/R/1445).
Competing interests
The authors declare no conflict of interest.
Ethical approval
Ethical considerations are paramount in any research endeavor, and this study adheres to the ethical guidelines set forth by the Faculty of Nursing at Zagazig University. Prior to the commencement of the research, ethical approval was diligently sought and obtained from the university’s ethical review board, ensuring that the study aligns with the principles of beneficence, non-maleficence, autonomy, and justice. Informed consent, a cornerstone of ethical research, was obtained from all participants, emphasizing transparency regarding the study’s objectives, procedures, and potential implications. The confidentiality and privacy of participants were rigorously protected throughout the research process, with data anonymization procedures implemented to safeguard sensitive information. The study also acknowledges the importance of respecting cultural norms and values, particularly in the sensitive context of palliative care for geriatric patients. By upholding these ethical standards, the research from the Faculty of Nursing at Port Said University contributes to the responsible and morally sound advancement of knowledge in the field of geriatric nursing.





