



Introduction
Family caregivers are essential partners in the care of relatives with palliative care needs. Often, they are heavily involved in providing the physical, social, emotional, and practical needs of the relative who becomes gradually more dependent at the end of life (Glajchen Reference Glajchen2004; Martín et al. Reference Martín, Olano-Lizarraga and Saracíbar-Razquin2016). Dignity is perceived as a basic human right involving being esteemed, valued, and respected (Chua et al. Reference Chua, Quah and Lim2022). Conserving a patient’s dignity while providing care is a fundamental concern regardless of the patient’s age, diagnosis, or place of care as loss of dignity may lead to worsening perception of selfhood, demoralization and triggering the wish to hasten death (Chochinov et al. Reference Chochinov, Hack and Hassard2002; Rodríguez-Prat et al. Reference Rodríguez-Prat, Balaguer and Booth2017). While dignity is an inherent human trait, it is also a relational concept influenced by the caregiver’s tenor, communication style, provision of support, and acts of empathy or indifference (Chochinov 2006 {Obispo, 2022 #9507}). Dignity may be violated when a person is vulnerable especially in situations of relational conflict, isolation or disharmony with the counterpart (Chua et al. Reference Chua, Quah and Lim2022; Franco et al. Reference Franco, Donato and Carvalho2019). Concurrently, dignity may be promoted when the ill person feels socially connected, receives good care from the family caregivers, and enjoys genuine family engagement paving the way for meaningful relationships (Andorno Reference Andorno2009; Chua et al. Reference Chua, Quah and Lim2022; Guo and Jacelon Reference Guo and Jacelon2014; Jacobson Reference Jacobson2009).
In Lebanon, family caregivers are deeply engaged and take charge in the caregiving role to ensure their ill relatives receive quality care (Dumit et al. Reference Dumit, Abboud and Massouh2015). The family unit is a basic social structure in the Arab world, much of Asia, and Latin Americas, often playing a key role inthe delivery of informal care, decision-making, and communication with health care providers (Osman and Yamout Reference Osman, Yamout, Al-Shamsi, Abu-Gheida, Iqbal and Al-Awadhi2022). Dignity preserving care, maintaining the values and worth of the patient, occupies a central ground in palliative care principles, and is an imperative standard in health care policies, and human rights’ laws (Brennan Reference Brennan2014). Although dignity perceptions or dignity conserving interventions are often explored from the patient’s or health care providers’ perspective (Chua et al. Reference Chua, Quah and Lim2022), the evidence from the family caregivers’ views is limited (Guo and Jacelon Reference Guo and Jacelon2014). Providing a safe psychological and physical environment, sense of belonging, and social support have been identified by caregivers as promoting patient dignity (Liang et al. Reference Liang, Xie and Pan2023). Whereas, abandonment, acts of omission, physical or psychological humiliation have been associated with dignity loss (Nåden et al. Reference Nåden, Rehnsfeldt and Råholm2013). Exploring family caregivers’ perceptions of dignity, and unfolding the strategies they adopt to preserve it, is vital to understand their role in enhancing the dignity of the ill relative with palliative care needs.
This study is part of a larger study that aimed to explore dignity perceptions from patients’ and family caregivers’ perspective within palliative care setting in Lebanon (Sailian Sap et al. Reference Sailian Sap, Preston and Salifu2022). This paper presents the perceptions of dignity and the practices that family caregivers adopt to preserve the dignity of their ill relative.
Methods
This is a qualitative study adopting the social constructivist paradigm. A social constructivist lens assumes that perceptions of dignity and practices that enhance or demean it are the outcome of a social reality, co-constructed between the participant and the researcher within existing sociocultural norms (Burr Reference Burr2015). The findings are reported in accordance with the Standards for Reporting Qualitative Research guidelines (O’Brien et al. Reference O’Brien, Harris and Beckman2014).
Setting
The study was conducted in Beirut, Lebanon, during the COVID-19 pandemic and political uprising (Chulov Reference Chulov2019). The settings were 2 sites providing care to patients with chronic, advanced or terminal illnesses: a health clinic and a hospital ward of a tertiary hospital. The hospital offers in-patient palliative care services to around 400 patients per year but has no support program to the family caregivers.
Participants
Participants were adult caregivers of relatives with serious illness related as the parent, spouse, son, daughter, or a sibling. Caregivers provided unpaid assistance with personal, psychological, household needs as well as financial support and arranging for the acquisition of health services (Roth et al. Reference Roth, Fredman and Haley2015). Participants needed to be actively involved in their care for at least 6 months, willing to be interviewed and capable of communicating either in English, Arabic, or Armenian. Family care givers needed to be caring for a relative at home or supporting someone in hospital. The relative with serious illness is any individual with advanced chronic or terminal illness such as cancer, organ failure, or neurodegenerative disease who has been hospitalized at least once in the past year (World Health Organization 2020). The receipt of palliative care services is not a criterion for selection.
Sampling
Fifteen participants were sampled purposefully (Patton Reference Patton2015) seeking specific variation in relationship to the relative, diagnosis, age, gender, and religion to enhance transferability. When information power, relevant to the aim of the study, was achieved, no further sampling was necessary (Malterud et al. Reference Malterud, Siersma and Guassora2016).
Recruitment
The family caregivers were recruited from the health clinics or the hospital wards through the patients or staff. The potential participants were contacted and informed about the study details through sending the Participant Information Sheet and the informed consent document via WhatsApp, which is widely used in Lebanon, for familiarization before data collection.
Questions about the research were addressed at the beginning of the interviews. The voluntary nature of participation and the right to withdraw was discussed before oral consent was secured and recorded for all the interviews due to the inability to interview all patients in person.
Data collection
Eight semi-structured interviews were conducted via telephone by SDS due to COVID-19 compulsory social isolation, 1 in person in a hospital setting and 6 in the participants’ homes in person. The interviews were conducted between September 2020 and April 2021 and audio recorded. They lasted a median of 30 minutes. Field notes were taken to capture initial impressions and thoughts of the researcher. The topic guide (online supplemental appendix 1), utilized during the interviews was prepared based on clinical experience and a review of the literature (Guo and Jacelon Reference Guo and Jacelon2014). Questions included: How would you define the concept of dignity? In what ways did your relative’s illness impact their sense of dignity? How did interactions with health care providers affect your relative’s dignity? What actions do you take to support and uphold your ill relative’s dignity? What factors or practices may either decrease or enhance the dignity of your relative? Probes were used to clarify interviewees’ answers as needed.
Reflexivity
Given the context of conducting this study in Beirut, Lebanon, during the COVID-19 pandemic and political uprising, reflexivity was crucial to acknowledge the primary researcher’s (SDS) position as a female nursing instructor of Lebanese Armenian origin who is trained in patient interviewing. Reflexivity was employed throughout the interviewing and analysis phases to mitigate this positionality and ensure a balanced interpretation of the data. Being mindful, continuous appraisal of the context, and note-taking at different phases of the research process helped in being thoughtful and harness reflexivity.
Data analysis
The interviews were translated from Arabic to English, transcribed verbatim by SDS, so they can be uploaded to NVivo qualitative software for data management. To protect confidentiality, the interview texts were de-identified for each interview. Reflexive thematic analysis was employed to ensure a thorough and nuanced understanding of the data, involving continuous engagement and immersion by the primary researcher, SDS (Braun et al. Reference Braun, Clarke, Hayfield and Liamputtong2019). This process included coding data line by line to identify over 200 codes, and inductively developing and refining themes that faithfully reflected the participants’ language and experiences. The data and the analysis were discussed among the researchers until the themes were refined in consensus. The open, flexible, and iterative nature of this analysis allowed for the identification of 4 main themes, ensuring the findings were substantiated with the participants’ perspectives while acknowledging the researcher’s influence (Braun Reference Braun2024).
Results
The 15 participants were from diverse religions and ethnic backgrounds (see Table 1). The majority were female (n = 11) reflecting the high involvement of women in caregiving. While many male caregivers supported the care financially, some of those interviewed also served as hands-on caregivers. Most participants lived in Beirut, except 2 in the suburbs.
Table 1. Demographics of the participants

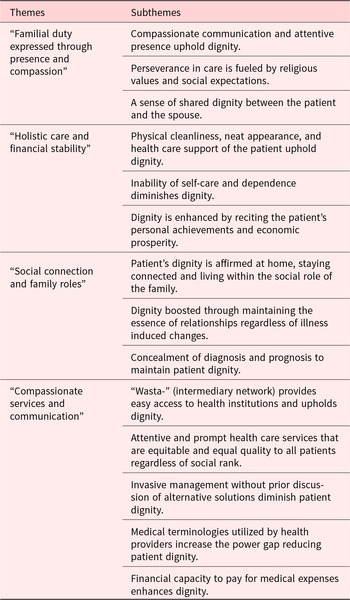
The participants shared their understanding of dignity and discussed their efforts in preserving the dignity in their ill relatives. Four themes on dignity were developed: (a) familial duty expressed through presence and compassion; (b) holistic needs and financial stability; (c) social connection and family roles; and (d) compassionate services and communication. These 4 themes and their subsequent subthemes described in Table 2 are interconnected as they collectively address the multifaceted nature of dignity in caregiving, encompassing emotional support, comprehensive care, social structures, accessibility of resources, and communication, all of which are crucial for maintaining the dignity of ill person. The themes are described below, supported with quotations.
Table 2. Themes and subthemes

Theme 1: Familial duty expressed with presence and compassion
This theme highlights that family caregivers enhance dignity through compassionate communication and an attentive presence. Their perseverance is fueled by religious values, duty and social expectations, with time leading to a sense of shared dignity between the ill person and the spouse.
According to family caregivers, kind, compassionate communication, and staying close to the patient, especially during times of acute illness, lay the foundation for dignified care. They perceived caregiving as a familial duty and a commitment that affirms their devotion to religious beliefs, faith, and fulfills social expectations. Soothing communication, use of gentle words, and maintaining respect were regarded the basis for nurturing a dignified life for the ill relative.
So, since my aunt is now passing through this hard situation, so… we need to be by her side. “Ma feena nofrot kelna” (we can’t break down all of us), we can’t be weak or divided, she is passing through a tough period, and we have to help her. (P08)
Despite sometimes the heavy burden of caregiving, preserving the ill relative’s dignity was of utmost importance as it enhanced their reputation and social status in the community. Family caregivers spent days and nights with the ill relative during hospitalizations, bearing sacrifices to ensure presence, support, and safeguard dignity. Caregiving was a collective family responsibility and a social obligation, exhibited by the division of tasks amongst each other.
As I accepted the sweet days …., I must accept the bitter or the bad, because this can be the path to spiritual salvation from many things in our lives. So, I accept it’.…So, preserving his dignity is by not using bad language, but only kindness and sweetness is my duty towards him (P02)
Dignity was perceived as a shared concept between spouse caregivers and their partners with the state of one’s dignity affecting the other. For instance, a wife feels happy when her husband is well dressed, or washed clean because his wellness reflects on her own well-being and dignity.
But I am doing this (caregiving) for God’s sake and for my own honour. I must do this.… If someone came and saw his pyjamas and underwear dirty, his feet dirty, they would say, ‘what is this woman? She doesn’t take care of her husband’. (P04)
Family caregivers considered the dignity of their ill relative a valuable matter to attend to through practicing kind and compassionate talk, and by being next to the ill person throughout the illness.
Theme 2: Holistic needs and financial stability
Physical cleanliness, neat appearance, health care support, reciting the patient’s personal achievements and ensuring economic prosperity uphold dignity, while inability to self-care, physical dependence, and limited purchasing power diminishes it. Family caregivers expressed that dignity is maintained through attending to the physical, psychological, emotional, and health needs of their relatives. They provided essential support like physical care, social entertainment, feeding, and securing health care supplies such as medicine and oxygen. Family caregivers aimed to ensure their ill family members are content, comfortable, clean, well fed, and symptom free at home.
One time he was begging for oxygen… so I think he felt bad, hmmm because of the illness of course, and the scarcity of resources. So yes, the illness, the pain, the shortness of breath, hm shake his dignity. (P07)
Of course, of course. My mother’s dignity is a priority to me, that she doesn’t feel upset. I make sure that all her needs are met, that she has nothing to complain about. (P09)
Losing functionality and the ability to take charge of basic personal care compromises relative’s dignity. Family caregivers offer personal assistance only after receiving the relative’s approval to reduce feelings of incompetence. For example, a daughter asks her mother’s permission before giving her a bath to preserve her dignity.
I tell her that, I just want to help and see if she wants, she accepts my help. I ask her first “can I do this?” “Let me help you with this.” “Do you want somebody to be with you?” (P14)
When she can’t reach the toilet in time, this affects her badly. (P12)
Most family caregivers expressed that recalling and celebrating the life experiences and accomplishments of the relative boost dignity and respect. Hence, they tend to recite those achievements during social encounters such as gaining high-community status, accumulated wealth, or a good reputation at work to affirm their capabilities and dignity. A male caregiver explained that he lifts his mother’s dignity through affirming and praising her cooking skills.
-
If I am around, I pass by for a cup of coffee, you know, these things will make her always happy …. and I always try to eat something from her kitchen, and I remind her that her food is the best, this makes her smile and then everything will be fine. (P09)
Economic prosperity is also seen crucial to assure all needs of the ill relative is met and dignity preserved. Asking for monetary assistance may imply weakness and diminish dignity of both the ill relative and family caregiver potentially leading to social isolation. Poverty and the inability to secure a good quality life do not resonate with dignity as it signifies low social status and vulnerability.
Don’t ask for monetary assistance from anyone. If you ask for assistance people will run away from you and gossip … they will isolate you, and not relate to you. (P04)
Preserving the physical needs of the relative through maintaining cleanliness, securing daily basic and medical needs, ensuring functional control over personal activities and providing moral support were strategies adopted by family caregivers to enhancing dignity in the ill relative.
Theme 3: Social connection and family roles
This theme affirms that relative’s dignity is acknowledged at home by staying socially connected and maintaining their role within the family hierarchy. Dignity is boosted through preserving relationships regardless of illness induced changes and concealing diagnosis and prognosis when necessary.
Maintaining their ill relatives’ role within the family, society, and community were seen as important. Dignity does not exist in isolation but is deeply seated within the collective societal values and connectedness of the family fostering identity and meaning through sharing personal stories, experiences, laughter, and dreams. It is within this communicative network that an individual establishes dignity.
For me, his dignity is above all dignity, so that he stays as he was before, productive, father of his children, and a giving human being, so his role is not finished in his life. (P03)
Family caregivers explained that although the relative’s character often changes with the illness, such as becoming more childish or impatient, this is overcome with humor, gentle communication, reinstating the individual’s inherent family role, safeguarding dignity.
He is still the caretaker and the head of the family; he says to us “do this … do that” he wants to be in control of us that makes him feel better. And this is true for my father and my mother. (P12)
Due to the stigma of the illness, some family caregivers did not disclose the truth about a poor diagnosis or prognosis to the relative to avoid psychological distress. Instead, they used softer words to explain the condition such as “infection” or “growth of a lump” to replace “cancer.” Some family members avoided spreading the news of the illness in the community to protect the relative’s dignity through concealment.
I won’t tell her (patient) about the metastasis… I will tell her that there is some residual ‘lump’ showing from the old thyroid … I will tell her but not everything at once…. Early morning, I was down at the pier crying … I don’t want the news to be spread. (P10)
However, family caregivers of relatives with non-cancer conditions, and those who experienced a sense of preparedness towards their death, had no problem in disclosing the medical condition.
I want them to fix her heart. They fixed it, may be temporarily, I think … I still don’t know when her heart will.. do that rhythm again. …there is always a question mark on her heart. (P06)
The ill relative’s dignity was unescapably seen as enhanced within the family setting that provided support and reinforced familial identity. Disclosing a poor prognosis was a sensitive issue to some family caregivers as it was perceived to jeopardize relative’s dignity.
Theme 4: Compassionate services and communication
This theme illustrates features of health care services that enhance or diminish patient dignity, from the perspective of the family caregivers. Economic stability, easy access to quality health care services, ability to pay, and attentive and prompt care regardless of social rank are critical elements to maintain dignity during acute phases of illness. On the other hand, invasive medical management without prior discussion of alternative solutions, and unclear medical terminologies utilized by health providers increase the power gap reducing patient dignity.
Family caregivers found that personal contacts, “wasta-” (intermediary network), were key human acquaintances that enabled patient access to health services especially during times of limited resources. “Wasta” is a common social norm in Lebanon that consists of an informal network that facilitates in reconciling a conflict or achieving a goal. Those who were not connected to a political party or an influential leader or did not have “wasta” suffered from delayed hospital admissions or did not receive care due to limited resources.
Doctors should give equal time to everybody, not that because X person works in a famous company, they give him more time and talk to him leisurely, on the other hand they pass by quickly on a patient who is poor or from low class. (P13)
Family caregivers sought health providers who genuinely understood and addressed their relative’s needs. A health care provider who is approachable, listens, and shows readiness to provide care regardless of social rank was regarded to be fostering dignity. Practices that demeaned dignity were staff being unresponsive to call bells, unavailability of health professionals, poor coordination among health disciplines, and inconsistent care standards. Gentle humor, amiable and positive conversations were perceived to be empowering and uplifting dignity.
So, my father needed to walk. One time, two nurses came in and started joking with my father. They said let’s go have some fun, let’s have a walk around, and they took him by his hand, for a stroll and then brought him back … hmmm … and he was doing it with a smiling face. Yep. I think they really cared about him, and they were very cautious that he doesn’t get angry or upset and feel safe with them. (P08)
Family caregivers expected health care providers to explore alternative measures before resorting to artificial or invasive interventions. Applying hand restraints or inserting a nasal feeding tube without negotiating with the family, were regarded as imposing, violating patient dignity.
The doctor told me we want to insert a tube from her nose for her feeding, because she is not eating (upset), but a friend, …. told me that I can get a syringe instead and put the smashed food inside it, and then I can feed her like that. I did that and it worked. I am grateful for her. (P12)
It was unnecessary (the restraints). We could have resolved it if they had called us, and that made it worse for her. (P01)
Family caregivers also requested clear, simple explanations of the health condition without medical jargon. A prescriptive language that holds no space for dialogue and employment of multiple medications was not welcomed and sometimes was seen as criticism.
When doctors don’t say everything about the case or use language we don’t understand, as if he has more power, this is bad. (P01)
Look sometimes my father has very poor compliance in his diabetic journey, when his physician gave him various instructions and comments about his lifestyle, inferring that he (my father) is not compliant and that he should do something about it eh … he got annoyed of it, he didn’t accept, and it felt offensive to him. (P04)
Family caregivers described distress over hospital expenses, which increased the burden and affected the dignity of both the relative and themselves. Financial strain was a significant barrier to dignity.
Last time, my daughter told me I paid the bill of the hospital, but they called me again asking for another payment. I told them my daughter had ‘closed’, paid the bill and paid all our dues, they told me no, you need to pay for the exit charge and the cost of the documents we used. I didn’t have the amount, I had only …., this is my day’s money (for daily living), I told them if you accept take it or else keep the patient with you. This is the worst thing that has ever happened (angry). (P11)
Health care services that were affordable, accessible and person-centered were regarded to be necessities that enhanced dignity in the ill relative during health care encounters. Family caregivers needed to be aware of the patient condition and the plan of care before its implementation.
Discussion
Family caregivers enhance patient dignity in multiple ways. Addressing patient’s holistic needs, preserving the social role of the relative within the family, maintaining financial stability, and following up on medical needs and consults, are all strategies adopted by family caregivers to ensure their ill relative remains dignified. As elaborated in other studies of dignity in serious illness, accessible health services, compassionate caring culture, social inclusion and fellowship, relational interactions, and clear communication were identified as essential to preserve patient dignity during acute illness (Sailian et al. Reference Sailian, Salifu and Preston2024; Tranvåg et al. Reference Tranvåg, Petersen and Nåden2015).
Commitment and loyalty in caregiving means that family caregivers in Lebanon uphold patient dignity through being present and providing support with kindness and a gentle approach. Lebanon’s cultural values, rooted in tradition and religion, underscore the significance of close family ties and moral obligation shaping the caregiving process (World Values Survey 2020). Caregiving in Lebanon shares common values to countries in northern Europe like Lithuania, where it is underpinned by familial duty, to sustain the ill relative physically, emotionally, and economically during illness (Kuznecovienė et al. Reference Kuznecovienė, Butkevičienė and Harrison2022). Also, in eastern cultures like China and Indonesia, family caregiving is a social and cultural tradition, fueled with the desire for mutual family support, sharing tasks, making sacrifices, and emotional connectedness, to invoke peace of mind and attain moral comfort and social approval (Chan et al. Reference Chan, Ho and Leung2012; Kristanti et al. Reference Kristanti, Effendy and Utarini2019).
The need for affirmation of the social role of the ill person in the family as a father, a mother, and ascertaining its entrenched value was often practiced by the family caregivers to preserve dignity. The concept of social connectedness and informal networks was central in reassuring, consoling and restoring the ill relative’s self-esteem, enhancing dignity comparable to other Middle Eastern countries like Iran (Babaei and Abolhasani Reference Babaei and Abolhasani2020) and Asian cultures (Lou et al. Reference Lou, Lou and Ridley2021). Similar to the findings of the meta-synthesis (Liang et al. Reference Liang, Xie and Pan2023), ill relatives are supported at home connected with family members to enhance feeling of “belonging” maintaining their role in the family and wider society, as the home environment serves as a source of dignity where their achievements, personal qualities and pride are acknowledged.
Family caregivers need accessible health care services that are equitable and affordable to all without political interference or intermediaries. They desire to have compassionate and genuinely engaged health care providers who are approachable and skilled in effective communication. Similar to European or other Middle Eastern countries, giving clear information, explaining the plan of care or future expectations in simple words, providing psychological support are deemed critical to a person’s dignity as well as for a sense of security to family caregivers (Babaei and Abolhasani Reference Babaei and Abolhasani2020; Robertson et al. Reference Robertson, Hjörleifsdóttir and Sigurðardóttir2022). In contrast, as reported in Middle-Eastern studies, communication limited to merely medical details or prescriptions, without addressing the psychosocial needs of the patient, was regarded to be too technical, bewildering, and unsatisfactory (Sailian et al. Reference Sailian, Salifu and Saad2021). Medical terminologies increased the power gap between the patient and health provider reducing patient dignity. It is worth noting that the evidence on patient dignity with palliative needs is comparable to that of ill relatives as expressed by the family caregivers.
Family caregivers in the United Kingdom, Canada, New Zealand, and Indonesia experienced challenges when combining employment and caregiving (Gardiner et al. Reference Gardiner, Taylor and Goodwin2022; Kristanti et al. Reference Kristanti, Effendy and Utarini2019). The demands of both roles often necessitated giving up their jobs or the introduction of significant changes for accommodation. Family caregivers wanted to remain employed to guarantee an income and secure financial capacity to have access to health services needed to the well-being of the ill relative (Gardiner et al. Reference Gardiner, Taylor and Goodwin2022; Kristanti et al. Reference Kristanti, Effendy and Utarini2019). This is similar to the Lebanese context where financial stability was crucial to safeguard patient dignity especially in times of economic crisis and shortage as the case in Lebanon. As access to quality health care services is often limited to the socially privileged, economic stability becomes essential to secure a dignified care for people with serious illness (Sailian et al. Reference Sailian, Salifu and Preston2024).
Similar to Asian and Arab cultures, family caregivers prefer not to disclose the diagnosis or poor prognosis to their relatives to decrease psychological distress and hence enhance dignity (Alzahrani et al. Reference Alzahrani, Alqahtani and Alhazmi2018; Sailian et al. Reference Sailian, Salifu and Saad2021; Ghoshal et al. Reference Ghoshal, Salins and Damani2019; Kristanti et al. Reference Kristanti, Effendy and Utarini2019). Cancer is still stigmatized in Lebanon, associated with negative discourse and misperceptions of incurability (Bou Khalil Reference Bou Khalil2013). In this regard, discussions about an individual’s deteriorating health are regarded as dishonorable and damaging to a patient’s dignity.
Implications to practice/policy
Supporting family caregivers: Since family caregivers hold a crucial and considerable role in the care of the ill relative across multiple countries globally; they have to be enabled and supported by health care professionals to maintain good caregiving that in turn preserves the dignity of their ill relative. Ensuring comprehensive support to family caregivers such as helping them retain paid employment, includes the involvement of various stakeholders like governmental policies, and community or employer initiatives, that in turn is beneficial to the ill relative, the caregiver and the society in general (Gardiner et al. Reference Gardiner, Taylor and Goodwin2022; Kuznecovienė et al. Reference Kuznecovienė, Butkevičienė and Harrison2022). This may be accomplished through needs assessment and support programs such as direct caregiver support, timely advice and referrals, assurance, communication with health care providers, and financial allowances to relieve caregiving burden (Aoun et al. Reference Aoun, Deas and Howting2015; Gardiner et al. Reference Gardiner, Taylor and Goodwin2022).
Clear communication from health care providers: Health care providers need to be aware and trained to employ compassionate communication using simple and clear language when conversing with family caregivers of ill relatives. Discussing interventions, particularly intensive ones, prior to their implementation is critical to ensure the ill person and the family caregivers receive care that is concordant to their wishes and perceived as dignified.
Financial stability and equal accessibility of health services: Family caregivers express the need for financial stability to follow up with the medical needs, supplies and services required for the care of their ill relatives. Having a national coverage of health services or adequate palliative care services and financial reimbursement will relieve family caregivers from some of the economic burden. Quality health services need to be accessible equally to all who are in need without discernment or discrimination. These changes would involve changes at the systems and governmental level.
Strengths and limitations
This study provides rich insights from family caregivers’ perspectives on how dignity is enhanced in relatives with various serious illnesses, illuminating differences about dignity from the Eastern Mediterranean region. It emphasizes the key role of family caregivers in maintaining dignity both at home and during hospitalization. However, it did not address dignity from a health care provider or policy maker perspective as well. The findings provide contextual insights which highlight the needs of family caregivers, particularly that of financial security, the need for support, and clear communication from health providers, during the caregiving journey in maintaining their relative’s dignity.
The COVID-19 health crises as well as severe economic crash of Lebanon could be a limitation of this study since the study was conducted during this period. Thus, participants’ views could be influenced by the unprecedented period of socio-political uncertainty and health care shortage. Nonetheless, these findings provide an initial understanding of the role and perceptions of family caregivers in enhancing dignity in a context where collective family decision-making is valued. Further research such as longitudinal studies could unveil how the role of family caregivers changes with the intensity and trajectory of the illness and how they shape end of life of their relatives.
In conclusion, dignity is upheld by family caregivers through their support and attendance to the holistic well-being they provide to their ill relatives. Preserving dignity is perceived as a duty and a moral obligation for the family caregiver and the family, is an important social unit, and a source of comprehensive support for the person who is unwell. However, family caregivers find it challenging in maintain this culturally desirable duty when faced with challenges of financial support, access to health services, and effective communication with health providers. It is important to ensure that family caregivers are supported so they continue in safeguarding the dignity of their relatives.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1478951525000100.
Acknowledgments
We would like to thank the staff of the health clinics and hospital wards for their assistance in recruitment. Also, we appreciate all the participants who were willing to take part in the interview during times of high stress and instability in the country.
Author contributions
SDS conceptualized the idea and developed the protocol with input from NP and YS; SDS conducted the interviews and led the analysis of the data with support from all authors. SDS wrote the first draft of the paper. NP and YS contributed to its critical revision and refinement. All authors read and approved the final manuscript before submission.
Funding
No funding was received for conducting this research, its authorship, and/or publication of this article. This study is part of the first author’s PhD thesis at Lancaster University, UK.
Competing interests
The authors declare no competing interests with respect to the research, authorship or publication.
Ethical approval
An ethical clearance was obtained from the American University of Beirut Institutional Ethics Committee (IRB- ID: SBS 2020-0033) and from the Lancaster University Faculty of Health & Medicine Research Ethics Committee (FHMREC19139) as the study was part of a larger PhD thesis that included patients and family caregivers as participants. Pseudonyms were applied to preserve the anonymity of the participants.




 Open access
Open access