



Introduction
Due to aging populations and prolonging dying trajectories, many countries, including Sweden, are experiencing a growing demand for end-of-life (EOL) care. Consequently, EOL care provision has been identified as a public health challenge requiring a shift toward care provided by caregivers in the community (Cohen and Deliens Reference Cohen and Deliens2012). A critical prerequisite for increased civic involvement in EOL care, however, is competence and preparedness to engage with dying and death. There is therefore a steadily increasing interest for new public health approaches to EOL care focusing on competence building in the community (D’Eer et al. Reference D’Eer, Quintiens and Van den Block2022; Sallnow et al. Reference Sallnow, Richardson and Murray2016).
General EOL competence, beyond the purview of care professionals only, has recently been conceptualized as death literacy, that is, a multidimensional construct encompassing knowledge and skills needed to access, understand, and act on EOL care options (Leonard et al. Reference Leonard, Noonan and Horsfall2021) and preparedness for engaging with EOL-related issues (Hayes et al. Reference Hayes, Fabri and Coperchini2020). The concept of death literacy was developed in Australia from a research by Horsfall et al. (Reference Horsfall, Noonan and Leonard2012, Reference Horsfall, Yardley and Leonard2015) and represents how experiences of caring for and supporting a dying person at home had transformative effects on awareness, knowledge, and skills in relation to dying and death and attitudes to engaging in EOL care provision (Noonan et al. Reference Noonan, Horsfall and Leonard2016). Dimensions of death literacy are said to build on the construct of health literacy (Noonan et al. Reference Noonan, Horsfall and Leonard2016).
There are several motivations behind efforts to build death literacy. One is to balance the professionalization of EOL care by emphasizing the role of community support for dying people (Kellehear Reference Kellehear2013). Another is to promote and support proactive EOL care measures, such as advance care planning (Banner et al. Reference Banner, Freeman and Kandola2019). Furthermore, competence building is central to accommodate a shift toward community-based EOL care provision to address growing palliative care needs (Etkind et al. Reference Etkind, Bone and Gomes2017).
The death literacy construct is operationalized and measured in the Death Literacy Index (DLI), developed to measure levels of death literacy in adults and evaluate EOL-related educational initiatives (Leonard et al. Reference Leonard, Noonan and Horsfall2021). Unraveling factors associated with death literacy might be helpful for understanding the construct and how it develops. During the instrument development process, some sociodemographic variables, that is, older age, having children, relationship status, religious belief, and origin, were found to correlate with death literacy (Leonard et al. Reference Leonard, Noonan and Horsfall2021, Reference Leonard, Noonan and Horsfall2020). Older age has also been found to correlate with Bugen’s (Reference Bugen1981) seminal notion of “death competence,” which involves people’s self-perceived ability to cope with dying and death (Miller-Lewis et al. Reference Miller-Lewis, Tieman and Rawlings2019).
Gender and education level have also been identified as influential factors of the theoretically linked health literacy construct (Martin et al. Reference Martin, Ruder and Escarce2009; van der Heide et al. Reference van der Heide, Uiters and Sorensen2016). Furthermore, since death literacy encompasses experience-based competence, it is likely that interactions with the health-care system, either professionally or as a patient or relative, might contribute to death literacy, as indicated by findings from Graham-Wisener et al. (Reference Graham-Wisener, Toner and Leonard2022). However, research about death literacy is scarce, and its association with sociodemographic, health, and experiential factors has not yet been thoroughly examined. The aim of this study is therefore to explore factors associated with death literacy, as measured by the Swedish version of the DLI (henceforth: DLI-S). An additional research question was examined: What are the relationships between factors? We also present a model of posited explanatory pathways, which might guide future research.
Methods
Study design
This cross-sectional explorative study analyses data from an online survey. The study was approved by the Swedish Ethics Review Authority (reference 2021–00915) and adhered to the ethical principles of the Helsinki Declaration (World Medical Association 2013).
The Death Literacy Index
As illustrated in Fig. 1, the original Australian DLI encompasses 4 main scales: (1) Practical knowing, which consists of the subscales (1.1) Talking support (4 items) and (1.2) Hands-on care (4 items); (2) Learning from experience (5 items), (3) Factual knowledge (7 items), and (4) Community capacity, which contains the subscales (4.1) Accessing help (5 items) and (4.2) Community support groups (4 items) (Leonard et al. Reference Leonard, Noonan and Horsfall2020). The DLI contains 29 self-report items that are answered with ordered categories on a 5-point Likert-type scale, often ranging from “do not agree at all” to “strongly agree.” The DLI is scored by calculating transformed mean scores, ranging from 0 to 10, for the full instrument, each scale, and subscale. Higher scores indicate greater death literacy, and the total composite score represents overall death literacy (Leonard et al. Reference Leonard, Noonan and Horsfall2021). The validity of the factor structure has been supported, and the DLI has demonstrated good internal consistency reliability, for example, Cronbach’s alphas of scales ranging above 0.8, in the original Australian context (Leonard et al. Reference Leonard, Noonan and Horsfall2021). Similar psychometric properties were recently found with a sample in the United Kingdom (Graham-Wisener et al. Reference Graham-Wisener, Toner and Leonard2022). The original English-language DLI is provided in Supplement file 1.
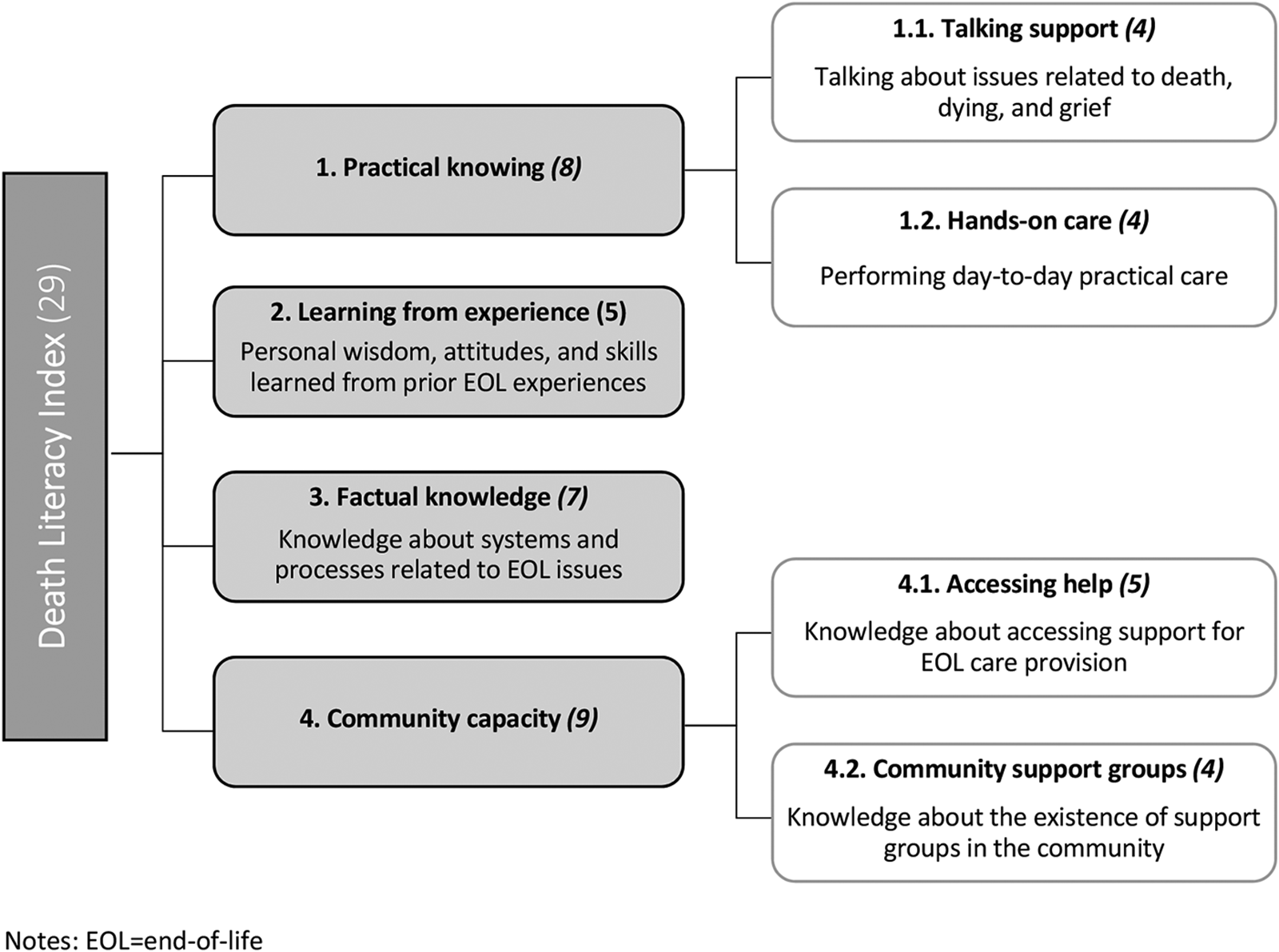
Figure 1. Overview of the dimensional scales and corresponding subscales of the Death Literacy Index (n of items). EOL = end of life.
The Swedish version of the Death Literacy Index
In 2021, the culturally adapted Swedish-language DLI was developed and tested in Sweden. The multistep translation and adaptation process is beyond the scope of this article but is described in detail elsewhere (Johansson Reference Johansson2022). The DLI-S was found to exhibit good validity in terms of content, response processes, and internal structure, with satisfactory psychometric properties for internal consistency (Cronbach’s α = 0.94, α for scales ranging 0.81–0.93), test–retest reliability, and factor structure (Johansson Reference Johansson2022). The DLI-S and its back-translation to English are provided in Supplement file 2.
Participants and procedure
Data were collected online during September–October 2021 through a survey distributed by a survey agency with an existing panel of approximately 100,000 adults in Sweden. The sampling plan is shown in Figure 2. Survey invitations were sent to a quota sample (n = 2911) from the panel, stratified by gender, age, and region, to consider the heterogeneity in the Swedish population. Panel members are compensated at the rate of 1 SEK (£0.08/€0.1/$0.12) per minute and can convert accumulated compensation to gift vouchers or charity donations.
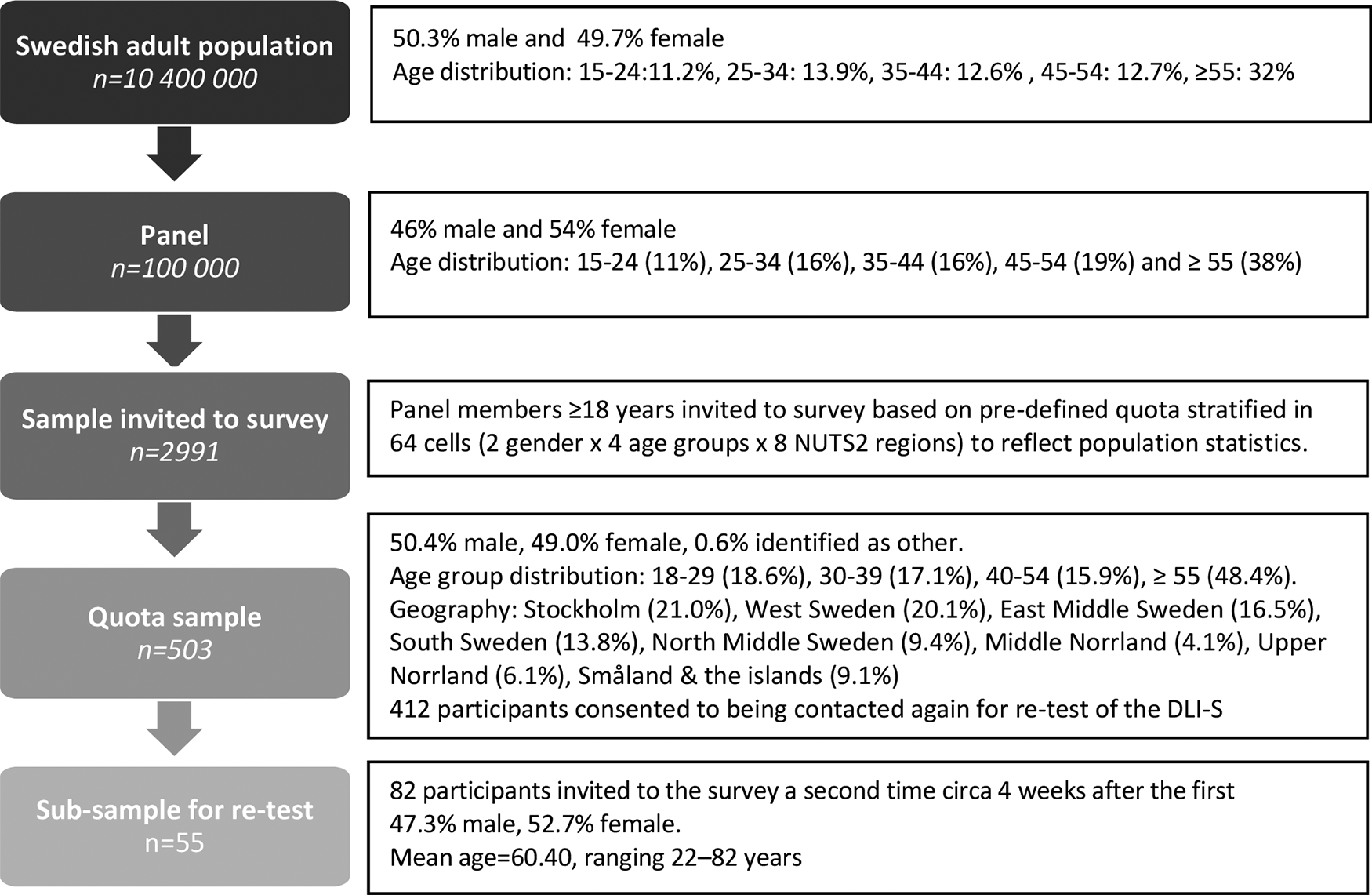
Figure 2. Sampling plan for the survey. Swedish population size in 2020, rounded off to the nearest 100,000.
Participants were informed about the study’s aim, topic, and procedure, and their right to withdraw at any time, and provided informed consent before being able to access the survey. In total, 503 (17%) participants completed the survey, which consisted of the DLI-S followed by questions about sociodemographic characteristics and EOL-related experiences. These questions are presented in Supplement file 3. Risk to participants was considered low; while survey questions about the EOL have been found to possibly affect immediate mood, cause of lasting harm is unlikely (Labott et al. Reference Labott, Johnson and Fendrich2013). All data were pseudonymized by the data collection agency prior to researcher access.
Data analysis
Statistical analyses were performed in SPSS (IBM, version 28), with statistical significance set as p ≤ 0.05. Participants’ total DLI-S score was used as the outcome measure of death literacy. Sociodemographic, health, and experience-based factors were used as explanatory variables. Country of origin was not included due to the low counts and heterogeneity within the foreign-born participant group. Direction and strength of bivariate associations between variables and death literacy were assessed using linear regression models. Polychotomous variables were dummy coded or combined to create mutually exclusive variables (see Supplement file 3). Only variables with statistically significant bivariate regression coefficients were retained for continued analysis.
Hierarchical regression analysis was used to estimate the collective and relative association of retained variables with death literacy. To select parameters for the regression model, a directed acyclic graph (DAG), also called causal diagram, was created using DAGitty (Textor et al. Reference Textor, van der Zander and Gilthorpe2016). In these graphs, explanatory and outcome variables are represented as nodes, with arrows between them indicating a causal relationship assessed on the basis of assumptions about temporality, face validity, and theory (Ferguson et al. Reference Ferguson, McCann and Katikireddi2020). Absence of an arrow indicates no suggested relationship. In this study, the DAG served as a template to postulate pathways, both direct and indirect, between explanatory variables and outcome. This process, summarized in Supplement file 4, enabled more informed decisions for constructing the regression model by distinguishing potential confounding and mediating variables to control for (Williamson et al. Reference Williamson, Aitken and Lawrie2014). Based on the DAG, a hierarchical regression analysis was conducted with 3 blocks. The model in the first block examined the influence of sociodemographic and health factors. In the second block, professional care background and EOL-related education or training were added to the model. In the third block, experiential factors were included in the model. Homoscedasticity of variables in the regression model, that is, whether residuals are equally distributed, was supported through visual inspection of P–P plots (Osborne and Waters Reference Osborne and Waters2002). Multicollinearity was evaluated using paired Spearman’s ρ correlation coefficients between variables and variance inflation factors (VIF) for each variable.
Results
Descriptive statistics
The 503 participants ranged in ages from 18 to 86 (x̄ = 49.95, SD = 17.92). Further participant characteristics are presented in Table 1. There were no missing values, as a mandatory response procedure was used, requiring all survey questions to be answered for participants to continue. Total DLI scores were normally distributed in the sample. The mean total DLI-S score in this sample was 5.15 (SD = 1.86, range = 0.61–10).
Table 1. Participant characteristics (n = 503)
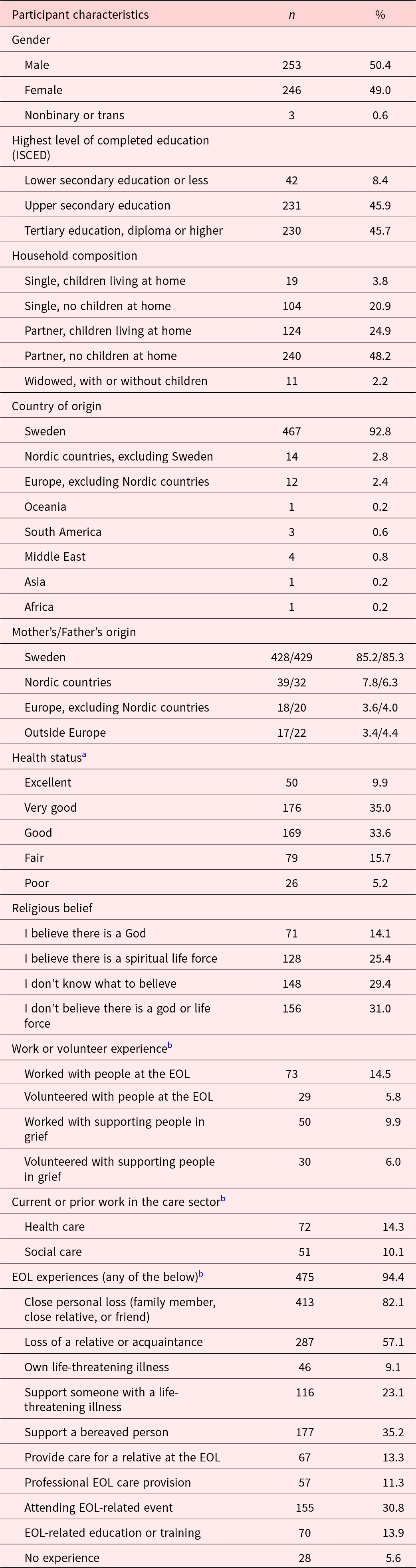
EOL = end of life; ISCED = International Standard Classification of Education;
a Do not wish to answer = 3
b Question with multiple response options allowed, that is, the variable denominator ≠ 503.
Bivariate regression analysis
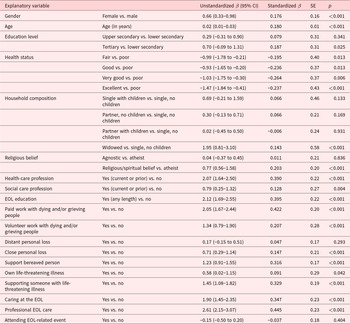
Results of bivariate linear regression analyses between death literacy and explanatory variables are shown in Table 2. Two variables, Distant personal loss and Attending end-of-life event, were excluded from further analysis as their correlations to death literacy were not statistically significant. Since only one category, being widowed, was significant from the variable Household composition, it was recoded as a separate dichotomized variable in the regression model.
Table 2. Results of bivariate linear regression analysis between explanatory variables and death literacy (total Death Literacy Index scorea)
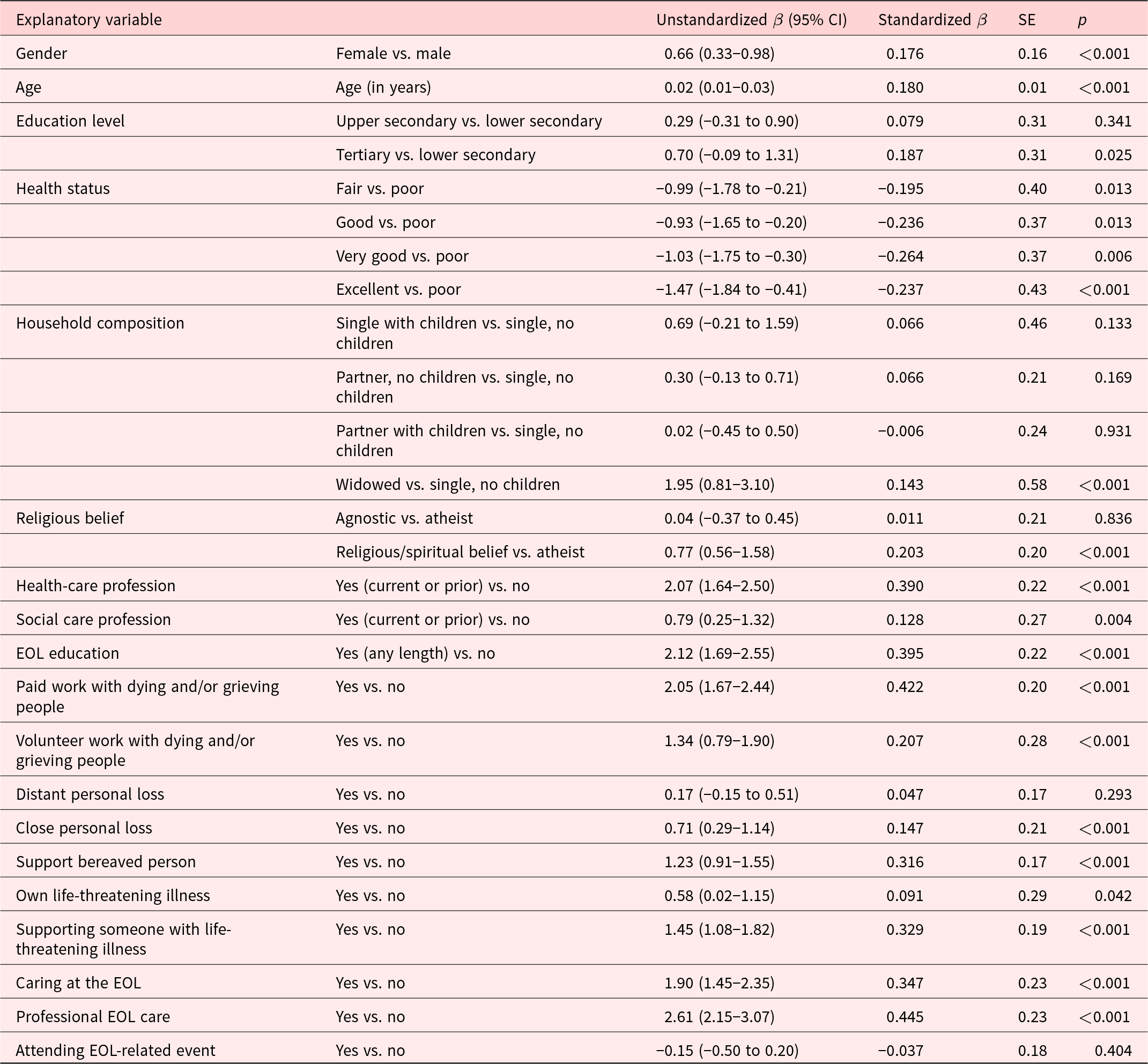
EOL = end of life.
a Ranging 0–10, with higher scores indicating greater death literacy.
Hierarchical regression analysis
Multicollinearity was found not to be problematic, with all variables having a VIF < 5. The matrix for pairwise correlation coefficients is presented in Supplement file 5. There was one strong correlation between widowhood and tertiary education, which likely resulted from the low number of widowed people (n = 11), making the percentual differences large even if the counts are not. All variables were therefore retained for continued analysis.
As depicted in Figure 3, the DAG illustrates an exploratory model of posited direct and indirect paths between death literacy and 16 explanatory variables. The results of the hierarchical model are shown in Table 3. The final model accounted for 40.5% of the variance in death literacy, F(22, 477) = 14.75, p < 0.001.
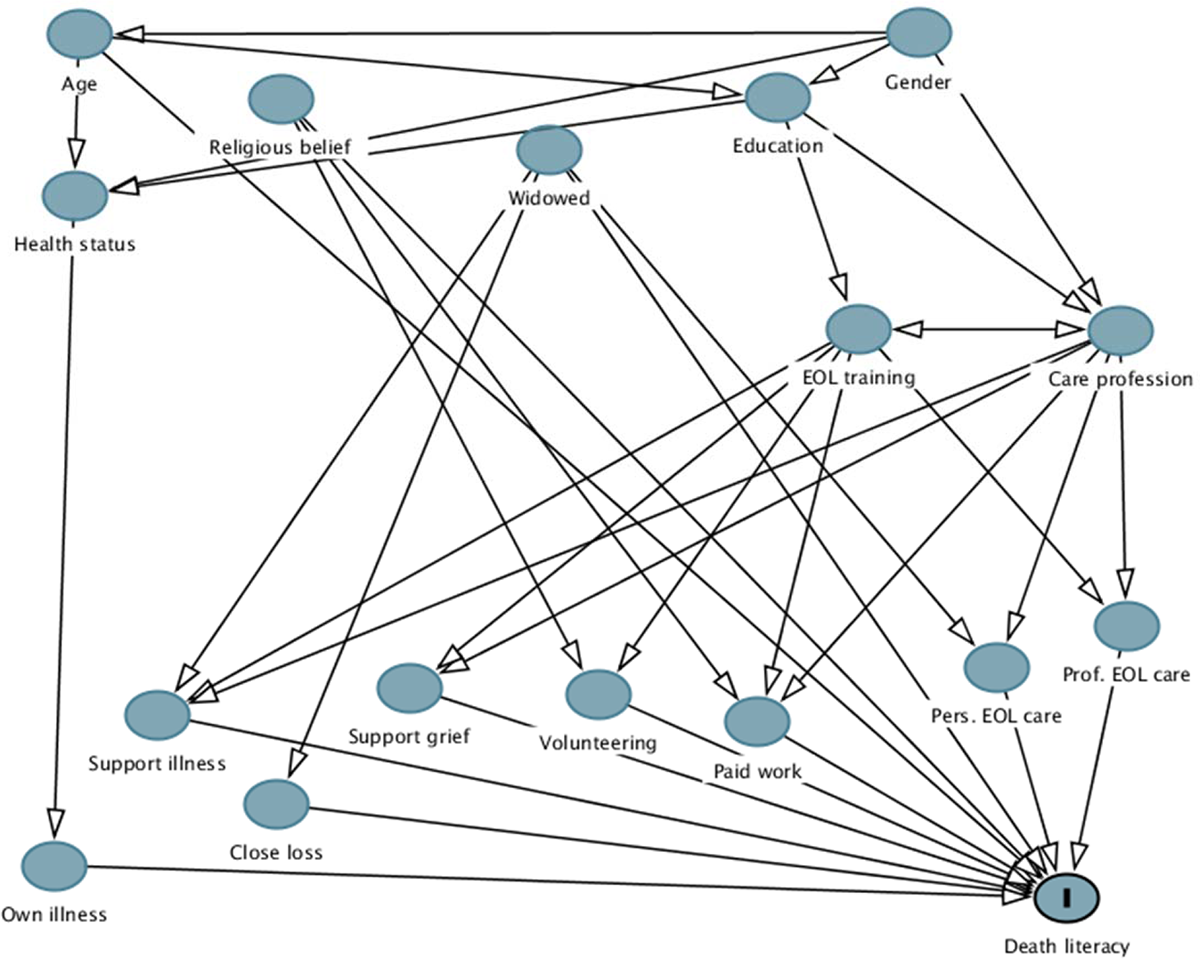
Figure 3. Directed acyclic graph of posited causal paths between sociodemographic, health, and experience-based variables and death literacy that informed the hierarchical regression model. EOL = end of life.
Table 3. Results of the three-step hierarchical regression model of relationships between explanatory variables and death literacya
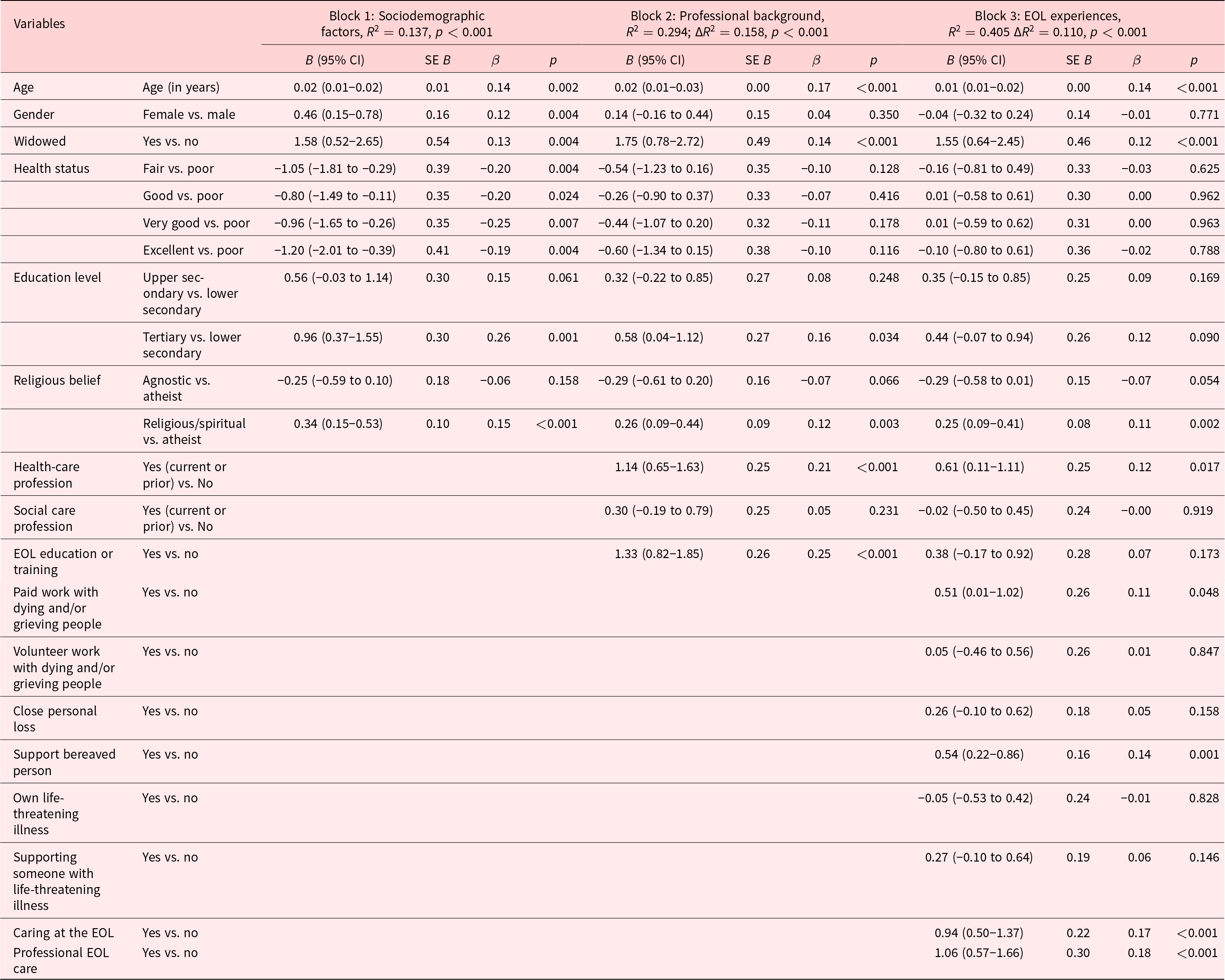
EOL = end of life.
a Total Death Literacy Index score, ranging 0–10, with higher scores indicating greater death literacy.
The first block included the sociodemographic factors age, gender, education, health status, widowhood (both men and women), and religious belief, which together accounted for 13.7% of the variance in death literacy. In the second block, professional care background and EOL education or training contributed an additional 15.8% of variance. In the third block, EOL-related experiences were included, accounting for another 11.0% of variance. In this final model, 8 variables were significantly associated with death literacy. Among the sociodemographic factors, widowhood (b = 1.55, p < 0.001), being older (b = 0.01, p = 0.001), and having a religious or spiritual belief (b = 0.25, p = 0.002) were positively correlated with death literacy, as was having worked in health care (b = 0.61, p = 0.017). Both professional (b = 1.06, p < 0.001) and personal (b = 0.94, p < 0.001) experience of EOL care provision, having supported a bereaved person (b = 0.54, p = 0.001), and having done paid work with dying and/or grieving people (b = 0.51, p = 0.048) were experiential factors significantly associated with higher death literacy.
Discussion
Main findings
Using bivariate and hierarchical multivariable regression analyses, this study shows associations between sociodemographic, health, and experiential factors and death literacy in a Swedish sample. Building on theoretical assumptions and Leonard et al.’s (Reference Leonard, Noonan and Horsfall2021) empirical research, our findings support the hypothesized relationship between direct lived experiences of EOL-related situations and death literacy, whether in formal or informal care contexts. Furthermore, this study highlights associations between a number of sociodemographic factors and higher death literacy, primarily older age, widowhood, and identifying as religious or spiritual. We did not, however, find a significant association to gender or education level, which have otherwise been shown to correlate with higher awareness of palliative care in the general public, internationally (Collins et al. Reference Collins, McLachlan and Philip2020; Patel and Lyons Reference Patel and Lyons2020) and in Sweden (Westerlund et al. Reference Westerlund, Tishelman and Benkel2018).
Being widowed, regardless of gender, showed the single strongest association with death literacy in our final model. While widowhood is theoretically linked to several direct EOL experiences, for example, supporting someone with life-threatening illness, providing care at the EOL, and loss, the effect was still strong after controlling for these factors. This suggests that there may be additional experiential aspects of widowhood that contribute to death literacy but were unaccounted for in this study. One such aspect could be that the closeness of the relationship with the dying person might influence the level of involvement as well as the salience of the experience. A close relationship likely entails greater involvement in care decision-making, which should, in theory, increase the Factual knowledge scale. Furthermore, a close relationship might heighten the emotional impact of an EOL experience, thereby potentially affecting a scale like Learning from experience. The suddenness of death and duration of illness might also alter the influence of widowhood. Such underlying aspects of widowhood and their association with death literacy remains a question to explore in future studies.
Overall, our study complements the existing literature by providing data from a new context that further support the assumption that death literacy is primarily associated with experiential factors. For example, there were several variables that were no longer statistically significant when experiential variables were entered into the hierarchical regression model. The significant negative association between health status and death literacy, that is, participants with poorer health had higher scores, did not remain when experiential factors were added. Curiously, the same tendency was found with experiences of life-threatening illness: neither experience of own illness nor supporting someone else remained significantly associated with death literacy when other variables were accounted for.
The significant, albeit weak, association between religious/spiritual belief and death literacy shown here support previous Australian findings (Leonard et al. Reference Leonard, Noonan and Horsfall2021). Religiosity has been shown to affect death attitudes in older people with chronic illness (Daaleman and Dobbs Reference Daaleman and Dobbs2010) and influence engagement in advance care planning (de Vries et al. Reference de Vries, Banister and Dening2019; Miyashita et al. Reference Miyashita, Shimizu and Fukuhara2021). Sweden, however, is known for being among the most secularized countries in the world (Hagevi Reference Hagevi2012). Nevertheless, Hagevi (Reference Hagevi2012) has showed that religiosity is more prevalent in Sweden when defined broadly as spirituality by including beliefs in some kind of life force. Our study supports this, although it should be noted that the sample is not representative of the Swedish population, for example, regarding proportion of foreign-born persons, and the proposed model may therefore underestimate the role of religiosity (Hagevi Reference Hagevi2017). One possible explanation for the association found could be that experiences of dying and death might awaken religiosity or spirituality. Alternatively, the association might be explained by more exposure to reflection and conversation about dying and death in religious or spiritual contexts, such as EOL-related volunteering. It should, however, be recognized that palliative care is generally publicly funded and run in Sweden, and there is relatively little public engagement in the form of volunteerism and charity work (Groeneveld et al. Reference Groeneveld, Cassel and Bausewein2017; Vleminck et al. Reference Vleminck, Paul and Reinius2022). Thus, potential mechanisms for these findings also demand further exploration.
Implications for practice
Self-perceived EOL competence is known to affect both professional (Grubb and Arthur Reference Grubb and Arthur2016) and family caregiver’s behavior and health (Henriksson and Årestedt Reference Henriksson and Årestedt2013). The death literacy concept encompasses several dimensions of knowledge and skills of importance for how EOL competence can be understood and developed both in the general public and organizations. The growth of community-based EOL care initiatives and increasing reliance on social care staff and family caregivers to support dying people (Bone et al. Reference Bone, Gomes and Etkind2018; Petrova et al. Reference Petrova, Wong and Kuhn2021) further emphasizes the necessity for competence-building efforts in these contexts, where increasing ability to access, understand, and act on EOL and death care options will be central objectives.
Experiential factors were found to influence the relationships between explanatory variables and outcome. Thus, lived EOL experience, rather than training in care provision (e.g., EOL education or having worked in a health-care profession), appears to be crucial for death literacy development. This finding raises questions about whether, and how, death literacy can be fostered through educational initiatives. For example, is it enough to encounter situations related to the EOL or is reflection or other forms of facilitated integration needed to build death literacy? Furthermore, what level of engagement in EOL situations is prerequisite and/or optimal for death literacy development? Leonard et al. (Reference Leonard, Noonan and Horsfall2021) argue that some of the skills that make up death literacy may not be easily translated into didactics. We have previously shown that exercises that promote reflection, introspection, and knowledge exchange supported development of EOL competence in eldercare (Johansson et al. Reference Johansson, Tishelman and Cohen2021). Overall, this study adds to prior literature, suggesting that death educational initiatives targeting EOL attitudes and preparedness benefit from focusing on experiential learning rather than information transfer. Our results suggest that a similar approach might be useful for death literacy development. There might also be other modes of engaging with dying, death, and bereavement with potential to enhance death literacy development. For example, prior research has highlighted the use of art and play (Kleijberg et al. Reference Kleijberg, Hilton and Ahlberg2021) and storytelling (Testoni et al. Reference Testoni, Ronconi and Palazzo2018) to help addressing EOL-related issues, which could aid knowledge exchange. In particular, this study suggests that volunteering might promote death literacy, which aligns with existing literature (Coleman and Walshe Reference Coleman and Walshe2021). Further research is needed to investigate what this might mean in practice.
Our findings contribute to an understanding of circumstances that foster death literacy and identify several influential variables that are amenable to change. This is useful to consider when designing future public health programs for EOL competence building. For example, as direct experiences were found essential for death literacy, this study indicates that inclusion of people with lived EOL experience, such as widows, may benefit knowledge exchange. There is growing international support for the validity of the DLI; to date, it has been validated in Australia, the United Kingdom, and Turkey, with studies ongoing in, for example, Belgium, the Netherlands, and China. While the cross-national validity of the DLI remains to be explored, its international spread provides opportunity of using it to evaluate and compare educational programs based on inclusive approaches to EOL care encompassing professional and lived experiences, such as the Scottish End-of-Life Aids Skills for Everyone (known as EASE) (Patterson et al. Reference Patterson, Gibb and Hazelwood2022) or Last Aid (Mills et al. Reference Mills, Rosenberg and Bollig2020). Such studies would add to the understanding of how death literacy might be developed on the individual and collective level. The DLI is also currently being used as one measure to evaluate an educational intervention about proactive EOL conversations in Swedish residential eldercare.
Strengths and limitations
Using established methods for exploring provisional causal inference from cross-sectional data, this study generated new knowledge about factors related to death literacy in the general public. Adhering to recommendations by Ferguson et al. (Reference Ferguson, McCann and Katikireddi2020), we constructed a DAG to conceptualize a model outlining the direction and strength of putative explanatory variables’ associations with death literacy, which were tested statistically. Using a hierarchical regression model was considered advantageous, as it controls for the effect of chosen variables, thereby enabling differentiation between total effect and changes in net effect. As the study’s aim was to explore possible associations between variables and death literacy and not generate population estimates, neither the use of non-probability sampling nor the low response rate was judged to pose a problem for the internal validity (Kohler et al. Reference Kohler, Kreuter and Stuart2019; Kukull and Ganguli Reference Kukull and Ganguli2012). The sample size was considered sufficient for adequate statistical estimation, given the number of variables in the model (Austin and Steyerberg Reference Austin and Steyerberg2015). Still, the results should be interpreted with caution, as the variable for widowhood had a very low count and therefore might have had a distorted influence in our model. Future studies might wish to use stratified sampling to explore the association between being widowed and death literacy further.
It is also possible that there may be unmeasured confounding variables (Williamson et al. Reference Williamson, Aitken and Lawrie2014). Our final model accounted for 40.5% of the variance, suggesting both that influential sociodemographic and experiential factors have been accounted for but that additional variables may also be of significance for explaining death literacy. The presented model thus constitutes a theoretical premise for future studies and requires further testing to assess both fit in other contexts as well as overall explanatory power. Furthermore, we have only investigated the effect of the variables on the overall DLI-S score and not on specific scales and subscales. It is possible that variables influence scales and subscales differently, resulting in distinct explanatory pathways to death literacy. Additional research is needed to disentangle the role of the different dimensions of death literacy. Longitudinal and experimental studies would be useful to address some of the remaining questions regarding causality in death literacy, such as residual confounding and temporality.
In addition, it is not clear how participants differentially interpreted questions about their experience of caring for or supporting someone at the EOL. Therefore, it is possible that some participants may have had EOL care experiences that were not conceptualized as such, for example, because they had not engaged in care provision directly or did not identify themselves as carers (Eifert et al. Reference Eifert, Dudley and Eddy2021). In future research, these questions may need adaptation to better distinguish between them.
Conclusions
The findings in this study demonstrate the individual, relative, and collective relationships between sociodemographic, health, and experiential factors and death literacy. Overall, our results support the notion that death literacy builds primarily from prior encounters with EOL care and death-related situations, such as caring for a dying person or supporting a grieving person. Specifically, the impact of working in health care and attending EOL education was shown to be influenced by direct experiences. This suggests that initiatives aiming to develop death literacy need to encompass components of both knowledge as well as reflection about lived experiences to adequately build competence and preparedness for EOL care. Still, further research is needed to account for the variance left unexplained by the model in this study, as there may be additional factors to consider to better understand the death literacy construct and how its development may be supported in both community and organizations.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1478951523000548.
Acknowledgments
The authors would like to acknowledge the valuable assistance of Sara Runesdotter in the statistical analysis. We also acknowledge Åsa Olsson’s contribution during study planning and data collection. Furthermore, we thank Rosemary Leonard and Kerrie Noonan for permission to use the DLI in this study and their input during the study process.
Author contributions
Joachim Cohen and Ida Goliath authors share last authorship.
Funding
This study was funded by Strategic Research Area Health Care Science (SFO‐V), Karolinska Institutet; the Doctoral School in Health Care Sciences, Karolinska Institutet; Swedish Research Council for Health, Welfare and Working Life (FORTE); Stockholm City Elder Care Bureau; and Stockholm Gerontology Research Center. The funders had no part in, nor influence on, the study design, data collection, analysis, interpretation, or writing of results.
Competing interests
The authors declare that there are no competing interests.








 Open access
Open access