



Introduction
Breast cancer is a dominant threat to global public health. In the United States, the incidence of breast cancer has been increasing over the past 4 decades. At the same time, mortality due to breast cancer is decreasing, thanks to advances in therapeutic treatments and diagnosis at earlier stages. Thus, in this country, there is an ever-increasing population of breast cancer survivors (Giaquinto et al. Reference Giaquinto, Sung and Miller2022). A similar situation is observed in other regions of the developed world, such as Europe (Zielonke et al. Reference Zielonke, Gini and Jansen2020). At the same time, in regions of the developing world where life expectancy has traditionally been very low, such as some undeveloped regions of Asia, the increase in life expectancy in recent decades has also led to an increase in the total number of breast cancer patients (Youn and Han Reference Youn and Han2020). Therefore, for reasons that differ between the developed and the developing world, there is a significant increase in the total number of women with breast cancer.
In addition to the emphasis on the therapeutic needs of breast cancer patients, considerable emphasis has also to be given on their psychosocial needs. Since the breast is identified with femininity, breast cancer and painful treatment procedures, such as mastectomy, radically impact the patients’ representation of themselves (Berterö and Wilmoth Reference Berterö and Wilmoth2007). It is undeniable that the self-esteem of women with breast cancer is affected as a function of the change in their body image (Carpenter et al. Reference Carpenter, Brockopp and Andrykowski1999). The lower levels of self-esteem of women with breast cancer are found through comparative analyses with healthy women. For example, a related study in Poland comparing 170 patients who had undergone mastectomy 5 years ago and 149 women who had never been diagnosed with breast cancer found that the former group had lower self-esteem scores (Tarkowska et al. Reference Tarkowska, Głowacka-Mrotek and Nowikiewicz2020). Therefore, improving self-esteem is considered a primary goal of interventional mental health enhancement programs in women with breast cancer (Pelekasis et al. Reference Pelekasis, Zisi and Koumarianou2016).
More generally, perceptions about the self change significantly due to the disease. Women with breast cancer often feel low pride, significant guilt, and intense shame (Solikhah et al. Reference Solikhah, Matahari and Utami2020). The belief that neglect of necessary health behaviors contributed to the development of the disease is significantly associated with these feelings (LoConte et al. Reference LoConte, Else-Quest and Eickhoff2008). Managing these perceptions becomes imperative as they are associated with more intense anxiety and depression for women with breast cancer (Hill et al. Reference Hill, Holcombe and Clark2011).
As a function of the above, and the general experience of the disease, the quality of life of women with breast cancer appears to be significantly affected. Quality of life levels are affected in the phase immediately after diagnosis due to the intense mental and physical burden on women (Chen et al. Reference Chen, Ma and Zhao2022; Oh and Cho Reference Oh and Cho2020). Moreover, even 5 years after the end of the relevant treatment regimens, it appears that there are still significant quality of life-related issues, for example cognitive decline, sleep disturbances, and issues related to sexuality (Schmidt et al. Reference Schmidt, Wiskemann and Steindorf2018). Therefore, breast cancer generally affects women’s quality of life.
Given the significant negative impact of the disease on patients and the long period of time over which they now survive the disease, it is necessary to study the relationship between treatment regimens and disease outcome (Culbertson et al. Reference Culbertson, Bennett and Kelly2020). Immediate reconstruction appears to have a beneficial effect on the quality of life, as based on a related study in Sweden, the quality of life levels of women undergoing immediate reconstruction are the same as those of the general population of women 1 year after completion (Elder et al. Reference Elder, Brandberg and Björklund2005). However, on the one hand, constantly updated data and recent studies are needed to draw relevant conclusions, and on the other hand, with regard to certain mental health parameters, the difference between immediate and later reconstruction has not been examined, but the difference between reconstruction and no reconstruction. For example, a related study in Brazil found that women who had undergone breast reconstruction had higher self-esteem scores compared to those who had not undergone reconstruction (Gomes and Silva Reference Gomes and Silva2013). Yet, it is not clear whether a similar pattern occurs for women who proceeded with immediate and later reconstruction. Also, research to date has not studied the relationship between the time to reconstruction in women who did not undergo concurrent reconstruction in relation to parameters of mental health and quality of life. In general, research on the psychosocial effects of reconstruction in women with breast cancer is characterized by considerable heterogeneity between studies and has also led to several contradictory findings, factors that highlight the need for further research (Heimes et al. Reference Heimes, Stewen and Hasenburg2017).
Based on the above, the objectives of this study were as follows:
1) to examine the difference in quality of life, self-esteem, pride, shame, and guilt between women who had and had not undergone breast reconstruction
2) to examine the relationship between the time to reconstruction for women who had not undergone simultaneous reconstruction and the above parameters
Methods
Study design
The present study was quantitative and cross-sectional. Thus, all assessments were carried out without prospective assessment of the patients. A comparative design was utilized for the first objective of the study, in order to search for differences based on immediate/later reconstruction. In addition, a correlational analysis was utilized for the second objective since both variables were numeric.
Participants
The inclusion criteria for this study were the following:
(1) Having received a breast cancer diagnosis
(2) Having received mastectomy
(3) Having received breast reconstruction
The exclusion criteria were the following:
(1) Diagnosis of dementia or any other syndrome affecting the patients’ ability to complete the study assessments
(2) Limited knowledge of Greek language, debarring the participants’ ability to complete the assessments
The inclusion and exclusion criteria were assessed by the participants’ medical records. The two exclusion criteria were also orally assessed prior to study recruitment.
Measures
Sociodemographic and medical data
Participants’ sociodemographic data included age (years), marital status (unmarried/married/divorced/widowed), employment status (employed/unemployed/retired), previous in vitro fertilization (IVF) (yes/no), number of children, parents’ place of origin (open question), country or city where they grew up (open question), previous treatments (chemotherapy/radiotherapy/hormone therapy/immunotherapy), date of completion of treatment (year and month), whether they are currently receiving any treatment (yes/no), type of treatment currently received (hormone therapy/immunotherapy/other), time since first diagnosis of the disease (years), family history of cancer, of any type, in a member of the extended family (yes/no), concomitant diseases (none/hypertension/diabetes/musculoskeletal/cardiovascular/other), and whether mastectomy and reconstruction have been performed together or at a later time (open question).
Breast-Q version 2.0
Breast-Q version 2.0 is a category of questionnaires that assess individual aspects of satisfaction and well-being of cancer patients through questions that take values from 1 (not at all) to 5 (all the time) (Memorial Sloan Cancer Center 2017). The subscales used in this study and the associated Cronbach’s level in this study were as follows:
1. psychosocial well-being (0.97)
2. sexual well-being (0.96)
3. Satisfaction with breasts (0.96)
4. Satisfaction with implants (0.94)
5. Physical well-being: chest (0.91)
6. Satisfaction with nipple reconstruction (Cronbach was not calculated as it consisted of only one question)
7. Patient experience: satisfaction with information (0.96)
8. Satisfaction with surgeon (0.97)
9. Satisfaction with the medical team (0.95)
10. Satisfaction with office staff (0.97)
The Rosenberg Self-Esteem Scale Questionnaire
The Rosenberg Self-Esteem Scale (RSES) is a self-report instrument with 10 questions answered on a Likert scale of 1 (strongly agree) to 4 (strongly disagree). Half of the questions are positive and half are negative. The scores of the individual questions are summed to a total score that reflects the respondent’s overall self-esteem. High scores mean high self-esteem and low scores mean low self-esteem (Rosenberg Reference Rosenberg1965). The standardized Greek version of this instrument (Galanou et al. Reference Galanou, Galanakis and Alexopoulos2014) was used in the present study. In this study, the α level was 0.84.
The State Shame and Guilt Scale
The State Shame and Guilt Scale consists of 15 questions that assess levels of shame and guilt on a Likert scale ranging from 1 (not at all) to 5 (absolutely) (Marschall et al. Reference Marschall, Sanftner and Tangney1994). This scale was translated into Greek using the back-forward method, in congruence with guidelines from previous literature (Maneesriwongul and Dixon Reference Maneesriwongul and Dixon2004). In this study, the Cronbach’s α was 0.71 for shame, 0.75 for guilt, and 0.86 for pride.
Procedures
The data collection of the study was carried out by the General Oncology Hospital of Kifissia “Agioi Anargyroi” in Greece, following a relevant decision of the hospital’s Ethics Committee (15912/01.10.2018). In particular, participants were informed about participation in the study by a medical specialist, who also administered the study measurement. The information took place following their hospital visits for health reasons related to breast cancer (e.g., preventive follow-up). Subsequently, women who wished to participate signed a written consent form and were given the study measurements. Participants were stressed on the anonymity and confidentiality of their participation, told that the data would be used solely for research purposes, and told that they could terminate their participation in the study even if they had initially agreed to participate in the research. Subsequently, they either completed the measurements on the spot or returned them on another day, following an agreed appointment. In addition, since some participants were from rural areas, they returned the measurements by post for convenience. Data collection lasted from October 2018 to October 2020. After this period, the data were entered into an SPSS database to be analyzed.
Statistical analysis
Statistical analysis of the survey data was carried out using the SPSS statistical program for Windows. Initially, descriptive statistics were used to calculate the sociodemographic characteristics of the study sample. Subsequently, a study of the normality of the distribution of the dependent variables was carried out to determine whether or not the normality of the distribution was violated. Subsequently, the relationship between simultaneous or not reconstruction and time since reconstruction and the values of the 3 self-report questionnaires was studied, based on an inductive statistical analysis. The relationship between immediate vs. later reconstruction and the questionnaires’ score was analyzed through Independent Samples T-test, when normality was not violated, and through Mann–Whitney U test, when normality was violated. The association between time till reconstruction and the questionnaires’ score was analyzed through Pearson’s Correlation, when normality was not violated, and Spearman’s Correlation, when normality was violated. The p value was set at 0.05 for all the analyses.
Results
The sociodemographic data of the participants are presented at Tables 1 and 2. As indicated by Table 1, most of the study participants were married (67.3%), employed (56.7%), had not undergone IVF (92.7%), had not had a protective mastectomy (74%) and were not currently receiving treatment (51.3%). Of those receiving treatment, the vast majority were receiving hormone therapy (83.6%). The majority of participants had another family member who also had cancer (63.3%), did not have a comorbidity (62.2%), and had gone into reconstruction at a later time (54%). Further details are shown in the table below.
Table 1. The qualitative sociodemographic data
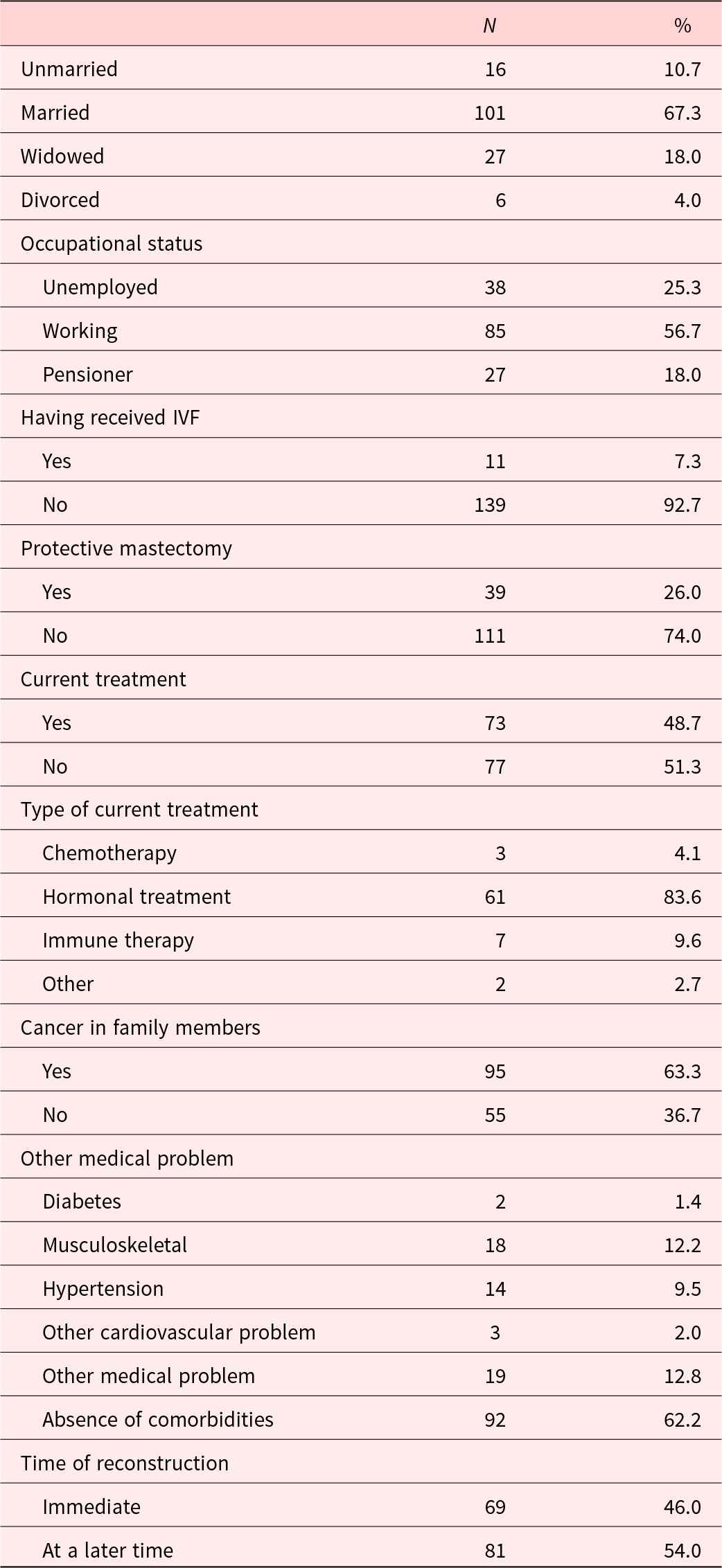
Table 2. The quantitative sociodemographic data
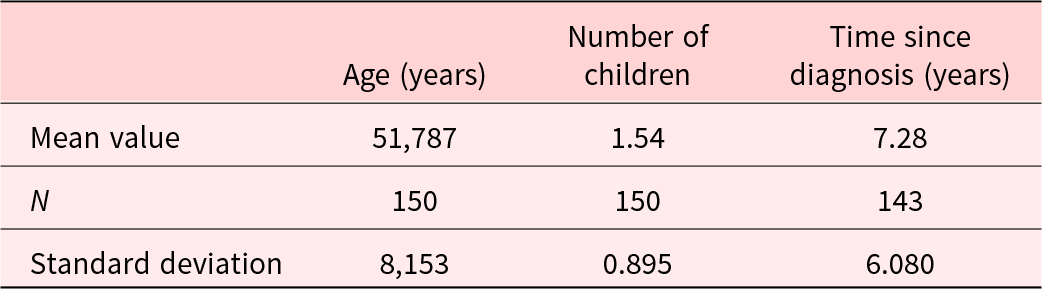
The following table presents the quantitative sociodemographic variables of the study. As can be seen, the participants had a low mean age, a small number of children, with a considerable standard deviation, and 7.28 years since diagnosis, also with a very large standard deviation.
The difference between those receiving immediate and later reconstruction on the questionnaires of the study is presented in Table 3. As indicated by the table, those receiving immediate reconstruction had higher scores in psychosocial well-being (p = 0.014) and sexual well-being (p = 0.016). No further significant differences were noted.
Table 3. The difference in questionnaire scores based on simultaneous or subsequent reconstruction
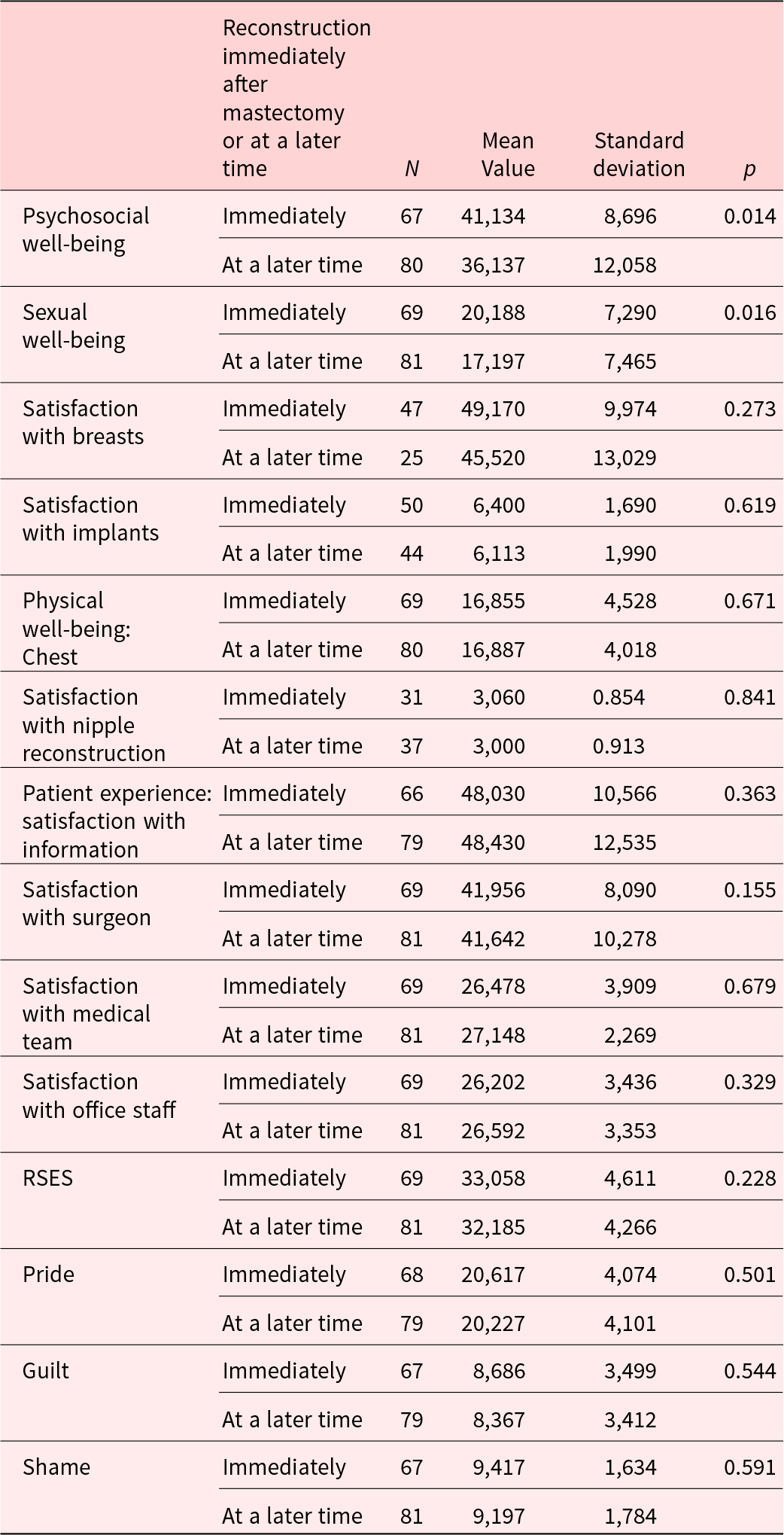
RSES; Rosenberg Self-esteem Scale.
Table 4 presents the analysis between the instruments’ score and time between mastectomy and reconstruction surgery. As indicated in the table, no significant associations were noted.
Table 4 The association between instruments’ score and time between mastectomy and reconstruction surgery
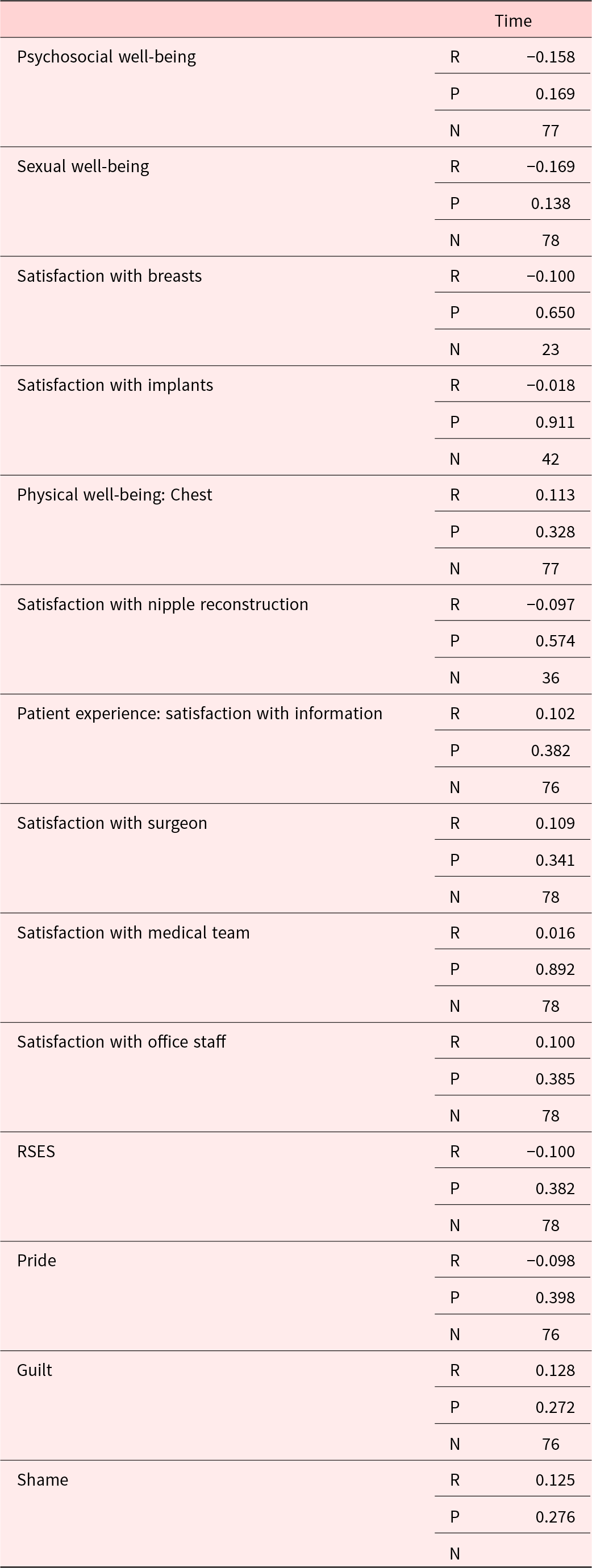
RSES; Rosenberg Self-esteem Scale.
Discussion
Without a doubt, breast cancer is a chronic disease that significantly affects the mental health of patients (Fortin et al. Reference Fortin, Leblanc and Elgbeili2021). Changes in body image have a central role in these negative effects (Helms et al. Reference Helms, O’Hea and Corso2008). In this context, this study examined parameters of breast reconstruction in relation to patients’ quality of life, self-esteem, feelings of shame, guilt, and pride. Based on the statistical analysis performed, the following central findings can be drawn:
1. Immediate reconstruction is associated with higher psychosocial and sexual well-being
2. No other parameters of quality of life, but neither self-esteem, nor feelings of guilt, shame, and pride, are associated with having a mastectomy and reconstruction at the same time or not
3. For women who did not undergo simultaneous reconstruction, the time elapsed until reconstruction is not associated with quality of life, self-esteem, , feelings of guilt, shame, and pride.
Based on the above, some theoretical attributions are possible regarding the parameters in relation to which statistically significant relationships were found and not found. With regard to self-esteem, in relation to which no statistically significant relationships were found, it is possible that the final outcome, meaning the existence or nonexistence of reconstruction, is the one affecting the self-esteem levels of women, irrespective of the course till that outcome. Indeed, Gomes and Silva (Reference Gomes and Silva2013) found that the existence and absence of reconstruction affected self-esteem levels of women with breast cancer, while this study found that the time of reconstruction did not have a significant effect on their self-esteem. Hence, it could be supported that self-esteem levels are affected by the current state of breast reconstruction not by the course of the patients till that final aesthetic outcome.
As for women’s feelings of guilt, shame, and pride, these may not differ because these feelings develop following the overall dynamics that arise as a function of the disease. For example, the feelings of guilt that currently arise are a function of the health behaviors that women had developed prior to the development of breast cancer (Shaver and Drown Reference Shaver and Drown1986). Based on this theoretical positioning and the findings of this study, it appears that no mechanism for linking these feelings to the differentials that might arise following breast reconstruction emerges.
As mentioned above, one of the findings of this research concerns the link between reconstruction and sexual well-being. In this case, it is possible that higher quality of life is not a function of women’s own representation of their body image but of the interaction with their sexual partners (Sheppard and Ely Reference Sheppard and Ely2008). Therefore, simultaneous breast reconstruction may possibly lead to a more rapid restoration of balance in relationships with the sexual partner after cancer diagnosis and treatment, thus leading to higher sexual well-being in the long term. Indeed, the higher psychosocial well-being scores on the part of women who proceeded to reconstruction at the same time may be explained by higher sexual well-being scores, given that the sexuality of women with breast cancer directly affects their psychosocial well-being (Kornblith and Ligibel Reference Kornblith and Ligibel2003).
In any case, the finding of higher psychosocial quality of life on the part of women who had undergone concurrent reconstruction should be considered highly significant. It is a fact that stress is significantly involved in the development of breast cancer (Antonova et al. Reference Antonova, Aronson and Mueller2011) and its recurrence (Palesh et al. Reference Palesh, Butler and Koopman2007). Therefore, the contribution of concurrent reconstruction in improving the psychosocial well-being of women with breast cancer can be considered as particularly important not only for their mental but also for their physical health.
Based on the above, it becomes clear that facilitating access to concurrent reconstruction for women with breast cancer is quite important. Among the main barriers identified at the international level is the lack of coverage of reconstruction by insurance funds, with the result that many women, especially those belonging to more vulnerable groups, cannot afford the cost of reconstruction (Retrouvey et al. Reference Retrouvey, Solaja and Gagliardi2019). However, given the significant impact of simultaneous reconstruction on women’s psychosocial and sexual well-being, it may be that it should take place at the same time as treatment. Health systems should take actions to this direction.
In any case, this study faces a number of limitations, which should be mentioned. A key limitation of the research relates to the size of the sample considered. This limitation lies not so much in whether the sample was small or large, but in whether it was sufficient to avoid the relevant error. From a methodological point of view, the inclusion of samples without a formula for calculating the required sample size can lead to Type I and Type II error, that is, incorrect rejection and acceptance of the null hypothesis, respectively (Campbell and Machin Reference Campbell and Machin1999). The absence of the use of such a formula in this research is a relative limitation of this research.
Another limitation relates to the taking of measurements during the COVID-19 pandemic. Based on the data from a recent study during the quarantine period in Greece, it seems that in mental health parameters of patients with chronic diseases, such as stress and somatization, there were higher values compared to healthy individuals, while in others such as depression and anxiety, there were not (Louvardi et al. Reference Louvardi, Pelekasis and Chrousos2020). Another study in China during the early phase of the pandemic found that a significantly high proportion of women with breast cancer, specifically 20.8%, experienced high levels of stress (Li et al. Reference Li, Santa-Maria and Feng2020). More generally, the impact of the current pandemic on the mental health of women with breast cancer is unclear, and it is unclear whether the results reflect a general picture of their mental health or a situation that was dynamically shaped under the effects of the COVID-19 pandemic.
Another limitation of this study concerns the quality of the participants’ responses as a result of the number of measurements administered. As Robson (Reference Robson2002) states, the more questionnaires administered in a survey, the lower the likelihood of accurate and qualitative responses from participants. Therefore, as a large number of questionnaires were used in this research, which required a large time commitment, this limitation cannot be ignored.
Based on the aim, results, and limitations of this research, it is possible to make a number of recommendations for future research. A first suggestion is to conduct qualitative studies to examine the same subject under consideration. From a methodological point of view, qualitative studies are appropriate for in-depth exploration of participants’ attitudes, perceptions, and beliefs about a researched issue (Babbie Reference Babbie2013). In the present study, the study was correlational, thus not being able to study in depth the formation of relevant phenomena. Consequently, a qualitative approach could lead to the study of “unseen aspects” of the issue under study, providing an opportunity for in-depth exploration of parameters such as shame.
A second suggestion would involve the investigation of additional parameters related to women’s mental health in relation to breast cancer reconstruction. In this study, parameters of quality of life and mental health not related to psychopathological manifestations were studied. However, it is widely accepted that breast cancer may potentially lead to significant trauma-related psychopathological manifestations. Thus, it is quite common for women to develop post-traumatic stress disorder as a consequence of the particularly intense traumatic event of breast cancer and its treatments, as well as the inability of women to cope with this trauma (Cordova et al. Reference Cordova, Riba and Spiegel2017; Parikh et al. Reference Parikh, Ieso and Garvey2015). It could therefore be studied whether breast reconstruction is associated with differences in post-traumatic stress disorder, given that women who proceed directly to reconstruction may also be distinguished by lower levels of post-traumatic stress.
Another suggestion for future research has to do with examining the possible differentiation of the effects of reconstruction based on the cultural context. In this study, given the sample size, no analyses were conducted to investigate a possible differential effect of reconstruction by cultural group. However, it is widely accepted that representations of breast cancer and body image change have a cultural bias, that is, they depend on the way in which the cultural group in question deals with these issues based on the norms they have formed. This finding emerges from multicultural countries and societies, such as that of the United States, where different representations of breast cancer and reconstruction are found among individual cultural groups (Soon et al. Reference Soon, Ruban and Mo2019). Consequently, a similar study could be conducted in our country to investigate whether breast reconstruction leads to different effects on the quality of life of women of different ethnic and cultural groups.
In addition, a third related suggestion has to do with investigating parameters of the relationship with health professionals involved in reconstruction treatment, which may potentially differentiate women’s subsequent quality of life. It is widely accepted that the relationship with health professionals when carrying out treatment interventions significantly modulates patients’ mental health, both immediately and in the long term (Di Matteo and Martin Reference Di Matteo and Martin2002). Therefore, another proposal has to do with conducting a study to examine the relationship with health professionals involved in breast reconstruction with women’s subsequent quality of life.
Conclusions
This study highlights the importance of simultaneous mastectomy and breast reconstruction, as it is associated with higher psychosocial and sexual quality of life. Therefore, simultaneous breast reconstruction should be promoted in health systems’ level.
Funding
This research received no specific grants from any funding agency in either the public, commercial, or not-for-profit sector.
Competing interests
The authors hereby state that they have no potential conflicts of interest to declare.





 Open access
Open access