


Obesity is defined as a disease in which excess body fat has accumulated such that health may be adversely affected( Reference Kopelman 1 ), and is one of the most common medical diseases in dogs( Reference German 2 , Reference Holmes, Morris and Abdulla 3 ). Recent UK studies put the prevalence of overweight (OW) and obese dogs between 52( Reference Holmes, Morris and Abdulla 3 ) and 59 %( Reference Courcier, Thomson and Mellor 4 ), with a rising trend and worldwide problem suggested( Reference German 2 , Reference Courcier, Thomson and Mellor 4 ).
Owners commonly misperceive the body shape of dogs, and this is the most marked for OW dogs( Reference Courcier, Mellor and Thomson 5 – Reference Eastland-Jones, German and Holden 7 ). Thus, it is vital for veterinarians to provide guidance as to what constitutes ideal body condition, and support this with effective education and communication regarding obesity prevention( Reference Degeling, Rock and Toews 8 ). Despite this, a previous study demonstrated that veterinarians rarely perform body condition scores (BCS) on dogs in primary care practice, suggesting that they rarely discuss the issue of OW status with owners. There are a number of possible reasons for this, including more pressing medical problems( Reference Shaw, Adams and Bonnett 9 ), the fact that the owner is obese( Reference Morris 10 ) or time limitations( Reference Coe, Adams and Bonnett 11 ).
The main aim of the present study was to determine the frequency of veterinarians recording dogs as obese or OW in the first-opinion practice. The study used a larger, more representative population of dogs than previous studies, and utilised data obtained from veterinary practice management software. The aim of a further study was to identify factors that were associated with the likelihood of OW status being recorded.
Experimental methods
This was a retrospective, correlational case–control study. Data were collected from practices using a compatible version of practice management software (Premvet v03.02.12) following a positive response to a postal request. seventy-four practices were approached, recruiting 16/59, 3/7, 0/6 and 0/2 practices in England, Wales, Scotland and Northern Ireland, respectively (total nineteen practices comprising forty-two premises). Data were collected between 10 May 2010 and 8 August 2011. Data were stored in, and retrieved from, a relational database (MySQL, Oracle). In total, 73 000 small animal consultations were contained within the database, of which 49 488 related to dogs.
All client-identifying data (e.g. owner name, address, postcodes and practice details) were either removed or coded to maintain anonymity of participants. Information was then exported to a spreadsheet application (Microsoft Excel version 10.6871.6870, Microsoft Corporation) and included signalment data such as breed, date of birth, sex, microchipping and insurance status, as well as free text written by the veterinarian about the consultations and the date conducted. Consultation duplicates were identified and removed prior to data analysis.
Cases (e.g. consultations where the dog was identified as having an OW status (i.e. the text included a term that suggested the dog was either obese or OW)) were selected from the total 49 488 canine consultations by a search of the clinical record free text using words or phrases that correspond to likely diagnoses by veterinarians (Supplementary data). The number of initial case consultations identified was used to calculate the relative frequency of recording the OW status in dogs within the Small Animal Surveillance Network database. Consultations with missing information on date of birth, consultation date, breed, sex and neuter status were then excluded, since these variables were required for matching purposes. Furthermore, consultations with mixed-breeds and animals less than 2 years of age were excluded, since variance in weight within these categories might have affected valid selection of control animals. The free text for each consultation was then assessed, in order to confirm all details, and 231 consultations remained.
A matched group of controls (e.g. consultations where the dog was likely to be OW or obese, but this was not stated in the free text (i.e. none of the search terms were present)) was also identified). Given that BCS was recorded in <25 % of dogs, it was not possible to use this measure to identify OW or obese control dogs. Instead, OW control dogs were identified using body weight data: for each case, all similar dogs (e.g. with the same breed, age, sex and neuter status) were first identified in the database, and those with a body weight in the upper quartile of weight within this group were then selected (calculated by a formula in Microsoft Excel). For each case, three control dogs were selected from this group using the random series generator of a statistical software package (StatsDirect, version 2.6.8, StatsDirect Ltd.). If it was not possible to match a case to three controls, the case was removed. This method ensured that control dogs were matched to cases for breed and sex, and were among the heaviest dogs with the same signalment. Ultimately, there were 146 remaining cases and 438 matched controls. Signalment factors (age, sex, neuter status, breed (i.e. all breeds with more than ten dogs in the case group)) and body weight were compared between groups to confirm adequacy of group matching.
For all cases and controls, additional variables recorded were: vaccination appointment; parisiticide prescribed (including both endo- and ecto-parasiticides); non-steroidal anti-inflammatory drug (NSAID) prescribed; People's Dispensary for Sick Animals (a charity subsidising veterinary care for people receiving housing benefit or local government tax) registered; pet health club member; osteoarthritis present; lameness present; vomiting noted; diarrhoea noted; anal sacs expressed; aggressive behaviour noted; and abdominal palpation noted. Consultations were already defined in the database as ‘yes’ or ‘no’ for the further variables of microchipping and whether or not the animal was insured. The absolute frequencies of each variable for both cases and controls were recorded, and their relative frequencies calculated. Data were then exported to a statistical software package (StatsDirect, version 2.6.8) and binary logistic regression was used to calculate OR and P values for each variable. Initially, simple regression was conducted. Thereafter, a multiple regression model was constructed, which initially included all variables that were P ≤ 0·20. The model was subsequently refined by backwards-stepwise elimination of the least significant variable at each round. Variables were retained in the final model, either if they were significant in their own right, or if removal lead to a significant (>10 %) change in the effect of the other variables. The level of statistical significance was set at P < 0·05, for two-sided analyses.
Results
Relative frequency of veterinarians recording overweight status
Based upon the search terms, the OW status of a dog was recorded in 671 of 49 488 consultations, a relative frequency of 1·4 %.
Case and control group summaries
In the case group, median age was 7 years (range 2–15 years), and this was similar to the age of controls (median 7 years, range 2–16 years). In both groups, 49 % were male (cases 72/146; controls 216/438) and 51 % were female (cases 74/146, controls 222/438), while 75 % were neutered in both groups (cases 110/146, controls 330/438). In cases, median weight was 25·3 kg (range 4·1–57·0 kg), while the median weight of control dogs was 24·9 kg (range 4·1–54·4 kg). A total of twenty-two breeds were included, with Labrador Retrievers (thirty-three, 23 %), Jack Russell Terriers (twenty-one, 14 %), Staffordshire Bull Terriers (fifteen, 10 %), border collies (eleven, 8 %) and West Highland white terriers (ten, 7 %) contributing the most consultations.
Risk factors for recording overweight status
With simple logistic regression analysis (Table 1), factors associated with a veterinarian recording of OW status included discussing osteoarthritis, discussing lameness, being microchipped and being a member of a practice health scheme. The same factors remained significant in the final multiple regression model. No other factors examined were of significance, either with simple or multiple regression.
Table 1. Simple and multiple logistical regression analysis on factors associated with a veterinarian recording overweight status
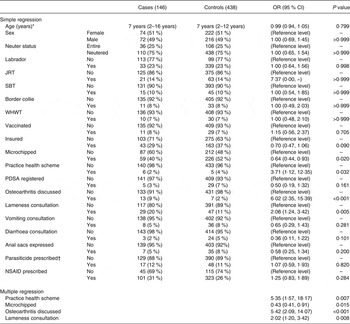
Frequencies and relative frequencies by case and control groups of dogs either positive or negative for each variable are displayed in the tabular format, with corresponding OR, 95 % CI and P values. JRT, Jack Russell terrier; SBT, Staffordshire bull terrier; WHWT, West Highland white terrier; PDSA, People's Dispensary for Sick Animals; NSAID, non-steroidal anti-inflammatory drug.
*Age data expressed as median (range).
†Parasiticide medication prescribed during the consultation, and included endoparasitic and ectoparasitic drugs.
Discussion
The present study has demonstrated that veterinarians in the first-opinion practice rarely record the OW status of dogs. In only 1·4 % of consultations, did the contemporaneous free-text entry indicate that dogs were either OW or obese. These data are consistent with those of a previous study, which demonstrated that veterinarians rarely perform weight measurements and body condition scoring( Reference German and Morgan 12 ). However, the present study expands upon the previous work because it was much larger (e.g. 49 488 v. 148 dogs), the study population more representative, data were taken directly from the veterinary practice management software, and it asked a different research question: the previous study asked how frequently body weight is measured and a BCS is performed in primary care practice; in contrast, the present study asked how frequently veterinarians record the OW status of a dog with their owner, and what prompts them to do this. Both studies also used different research methodology. In the previous study, the computer records sent to a second-opinion veterinary hospital were reviewed for evidence of body weight measurements and BCS. In the present study, data were obtained as part of a national surveillance project, and directly collected from the practice management software. This enabled patient records to be examined for evidence of terms associated with the OW status. Despite these differences, both studies confirm that veterinarians infrequently assess the OW status in dogs that they examine.
Given that BCS was uncommonly recorded, it was not possible to determine the prevalence of OW status in the present population. However, if prevalence is similar to the expected prevalence in UK dogs, based on the recent studies( Reference Holmes, Morris and Abdulla 3 , Reference Courcier, Thomson and Mellor 4 ), this suggests that the condition is markedly underreported. All such findings have wide-reaching consequences for the veterinary profession, since they suggest that many dogs are not treated despite the well-recognised health consequences, which include increased disease risk( Reference Lund, Armstrong and Kirk 13 ), shortened lifespan( Reference Kealy, Lawler and Ballam 14 ), metabolic dysfunction( Reference Tvarijonaviciute, Ceron and Holden 15 ) and decreased quality of life( Reference German, Holden and Wiseman-Orr 16 ). Interestingly, veterinarians have specified obesity as one of the main issues they could do more for as a profession( Reference Yeates and Main 17 ), indicating possible awareness of underdiagnosis. Finding the most appropriate means of communicating with owners regarding the topic of obesity( Reference Wheat, McMartin and Coe 18 , Reference Wheat, McMartin and Coe 19 ) might be a useful strategy in ensuring more veterinarians are prepared to actively engage owners with OW dogs.
Since only a few studies have examined veterinary decision-making for obesity, the reasons for the observed underreporting are not known. However, better understanding the reasons might allow strategies for change to be identified within the profession. One possible explanation for why the OW status was not recorded would be the time constraints encountered in general practice; in this respect, there might be other problems requiring more urgent attention. This is, perhaps, compounded by the fact owners rarely present their pet to the veterinarian because they are worried about excess body weight( Reference White, Cobb and Hammond 6 ), which itself might be related to the increased tendency for owners of OW dogs to underestimate their body condition, than owners of ideal weight dogs( Reference Courcier, Mellor and Thomson 5 – Reference Eastland-Jones, German and Holden 7 ). In addition, veterinarians might be reluctant to record the OW status if they perceive that they will encounter resistance from owners, or be concerned about offending the owner. This reluctance might arguably be greater when owners are themselves OW, and it is noteworthy that a positive association between BMI in owners and the body condition of their dog exists( Reference Holmes, Morris and Abdulla 3 , Reference Courcier, Thomson and Mellor 4 ).
A second aim was to determine what factors were associated with the likelihood of a veterinarian recording OW status, and this was explored in the case–control part of the study. The OW status was more often recorded when dogs presented with either osteoarthritis or lameness, which is logical given their known association in this species( Reference German 2 , Reference Lund, Armstrong and Kirk 13 ). It also emphasises that veterinarians more commonly highlight the OW status where they perceive either an association with a current health concern, or that weight management might benefit mobility. In contrast, there was no association between dispensing of NSAID and recording of OW status. While NSAID usage was common, being dispensed in 27 % of all consultations, they were given for osteroarthritis and lameness in only a minority of cases (3 and 13 %, respectively). Therefore, the lack of association between NSAID use and recording the OW status might reasonably be explained by the fact that NSAID have a wide range of indications, including analgesia for non-orthopaedic problems and post-operative analgesia. Furthermore, NSAID were commonly dispensed during repeat prescription consultations and, in such circumstances, the OW status is unlikely to be recorded.
The OW status was also more commonly recorded when dogs were enrolled in a practice health scheme (a scheme whereby complimentary routine preventive health care and some additional veterinary fees are provided an upfront fee). This would be expected, since OW dogs might have joined such a scheme because they were OW. In addition, since such schemes focus on preventive health care, and would include discussions regarding maintaining a healthy weight, greater recording of the OW status would be expected. In contrast to this, the OW status was less commonly recorded in dogs that were listed on the practice system as microchipped; however, the reason for this association is unknown.
The study has a number of limitations, which should be considered. Firstly, it was retrospective in nature, and used data gathered from practice software; as a result, and some information is incomplete or missing. For instance, occasionally basic signalment data were missing, such that some consultations were excluded which might have been relevant. Secondly, the study's search terms mainly utilised the free text entered during the consultation. This free text quality most likely varied between practices and veterinarians, and might not have represented the actual extent of the discussions between veterinarian and client. Thirdly, the use of key words to identify consultations within this free text, particularly when identifying case animals was another limiting factor. Although an effort was made to consider all possible complete word, and shorthand terms for the OW status, some might have been missed. Thus, the results obtained might be an underestimate of the actual situation. That said, it is unlikely that this point alone would account for the discrepancy between the current prevalence of dogs being OW and obese, and the frequency of recording the OW status.
A fourth limitation was the method by which OW status was recorded for control dogs. Unfortunately, we were unable to use BCS to identify controls, because this parameter was rarely recorded, a finding consistent with other published work( Reference German and Morgan 12 ). Such a problem is common to other studies of this nature( Reference Carina and Morris 20 ). Therefore, we chose to use bodyweight, stratified on breed, sex and neutered status, whereby dogs in the upper quartile were assumed to be OW. It is possible that this method incorrectly categorised some dogs as OW and vice versa.
Finally, there were limited breeds included in the present study due to excluding those without three matched controls and excluding all crossbreeds; results, therefore, cannot necessarily be applied to all breeds or to the crossbreed population. The three breeds of Labrador Retrievers, Jack Russell Terriers and Staffordshire Bull Terriers contributed proportionally the most consultations to the study. Owing to the Jack Russell Terrier not being recognised officially as a breed( 21 ), it appears overrepresented in the present study. Other than this, the breed spread is highly representative of the most commonly registered breeds( Reference Asher, Buckland and Phylactopoulos 22 ). We must also consider that, as dogs are often classified in the practice records based on the type they most represent and are not necessarily a pedigree of that breed, matching the breeds in the present study may not have overcome the actual variances in weight when calculating quartiles.
Conclusion
We conclude that there is a marked underreporting of OW status in pet dogs, but the reasons for this are not clear. Various factors were related to the likelihood of a veterinarian recording OW status, the most notable when the consultation was for osteoarthritis or lameness. While this suggests that veterinarians are aware of the association between the OW status and orthopaedic disease in dogs, lesser importance is placed on identifying obese dogs without such complications. This presents a challenge for strategies that aim to prevent the development of obesity, or to manage the condition when it arises. Further work is needed to understand the reasons behind decision-making in veterinarians, when faced with an OW or obese dog.
Acknowledgements
The authors would like to thank Small Animal Surveillance Network (SAVSNET) for providing the data to carry out the study. A. J. G.'s readership is financially supported by Royal Canin. This research received no specific grant from any funding agency, commercial or not-for-profit sectors. A. J. G.'s academic position at the University of Liverpool is financially supported by Royal Canin. The study was based upon a project conducted by N. C. R., as part of the requirements for the Degree of Bachelor of Veterinary Science. A. J. G. and P.-J. M. N. proposed the research question; P.-J. M. N. acquired the study data from the Small Animal Surveillance Network database; all authors assisted in study design; N. C. R. executed the study and analysed the data; N. C. R. produced the first draft of the manuscript, which was subsequently edited by both A. J. G. and P.-J. M. N. The work was performed at School of Veterinary Science, University of Liverpool, Leahurst Campus, Chester High Road, Neston, Wirral, CH64 7TE, UK.
This paper was published as part of the WALTHAM International Nutritional Sciences Symposium Proceedings 2013, publication of which was supported by an unrestricted educational grant from Mars Incorporated. The papers included in these proceedings were invited by the Guest Editor and have undergone the standard journal formal review process. They may be cited.
Supplementary material
The supplementary material for this article can be found at http://www.journals.cambridge.org/jns



 Open access
Open access