


Introduction
A major obstacle in the translation of research findings into practice is the lack of representation of members of minority groups in research [Reference Smith, Agar and Delaney1–Reference Murthy, Krumholz and Gross4]. Research studies conducted with communities are often designed to reach underserved people in rural areas or those who lack access to care at academic centers where most research is conducted. Despite the intent of engaging these communities in research, there are multiple challenges, such as insufficient information about research, low health literacy, and language and cultural barriers [Reference Smith, Agar and Delaney1,Reference Ford, Howerton and Lai5 Reference Shavers, Lynch and Burmeister–7]. To help address these challenges, researchers have integrated Community Health Workers (CHWs) as part of the research team for their insight into social, economic, and cultural factors of underserved communities and their ability to meaningfully engage these populations, as they are often members of the same communities [Reference Cottler, Striley, O’Leary, Ruktanonchai, Wilhelm, Alving, Dai and Chan8]. This involvement has had positive effects. CHW-led interventions have enhanced chronic disease management [Reference Aponte, Jackson, Wyka and Ikechi9,Reference Hargraves, Ferguson, Lemay and Pernice10] and have increased health promotion practices like cancer screening [Reference Cosgrove, Moore-Monroy and Jenkins11,Reference Lohr, Ingram, Nuñez, Reinschmidt and Carvajal12]. The CHW/Promotora workforce has particularly played a key role during the COVID-19 pandemic [Reference Ballard, Johnson and Mwanza13,Reference Nawaz, Moon and Vazquez14]. Although they serve an important role in research, CHWs/Promotoras have not received much training and need to learn research best practices [Reference Hohl, Thompson and Krok-Schoen15,Reference Terpstra, Coleman, Simon and Nebeker17]. There is no standard training in research best practices for this important workforce, and training tends to be variable [Reference Lohr, Ingram, Nuñez, Reinschmidt and Carvajal12,Reference Kash, May and Tai-Seale18] since national competencies for research best practices for CHWs do not exist.
Our team developed training in research best practices for CHWs and Promotoras (hereafter referred to as CHW/Ps), their Spanish-speaking and for the most part, bilingual counterparts, using a community participatory approach with diverse stakeholders. Additionally, we previously reported CHW/Ps’ initial perceptions of an early version of the training [Reference Varma, Samuels and Piatt19] and revised and refined the materials based on feedback. This led to accessible, culturally- and linguistically appropriate training modules for CHW/Ps to better support research in the settings where they work. The training was designed to be administered either online, which is self-directed, or through facilitation with a trained group facilitator. The facilitator-led training utilizes trained peer “Champions,” but the structure and content of both versions of the training are the same. This article presents the findings of our evaluation of the online self-paced training course developed both in English and in Spanish. We outline the development of the course and the results of the evaluation of CHW/Ps’ self-rated abilities and perceptions of the online training.
Materials and Methods
Course development
A U01 award from the National Institutes of Health (NIH), National Center for Advancing Translational Sciences (U01TR003409), funded this team from three Clinical and Translational Science Award (CTSA)-funded institutions: University of Michigan (U-M), University of Florida (UF), and University of California, Davis (UC Davis). The three CTSA hubs include national leaders and experts in community-engaged research with underrepresented communities. Each site utilized previously established relationships with local community-based organizations that serve diverse racial and ethnic populations to select community partners for the project. From each hub, members of the team included researchers, research staff members, community-based organization leaders, and CHW/Ps.
The content and approach to course design were modeled after the Social and Behavioral Research Best Practices Course, which was developed for social and behavioral research professionals [Reference Murphy, Byks-Jazayeri and Calvin-Naylor20]. We first identified competencies for community-engaged research by CHW/Ps for research conduct, recognizing that CHW/Ps may have either a formal role on study teams or more informal roles, such as working at a site where research is being conducted. We began the development process with the understanding that this training was not a replacement for human participants protection training required for members of research study teams. This course was designed to provide basic introductory training in community-engaged research that focuses on the logistics of conducting research in partnership with communities. We did not provide training on different types of research studies such as interventional trials, observational or cross-sectional studies or the like, but the module did address what randomization is and why it is important for certain studies. We identified four modules for research conduct with a fifth module to cover the COVID-19 pandemic to address research with community members during a once-in-a-generation public health crisis. The modules are listed in Table 1.
Table 1. CHW/P research best practices course modules
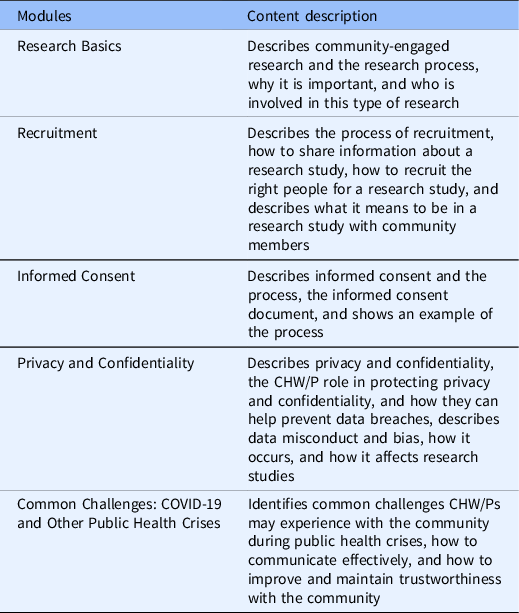
We collaborated closely with both an instructional design and a health literacy nonprofit organization for course development which took approximately 1.5 years to complete using a participatory process. The instructional designers regularly met and established processes for developing content based on competency-based learning objectives. They worked with us to engage our stakeholders and subject matter experts to create materials according to a development timeline. Subject matter experts consisted of team members and individuals who were employed as CHW/Ps or worked in community-based organizations. An outline of content was created, and the consultants helped provide details, such as relevant examples or scenarios to reinforce learning objectives. For example, to depict the process of how to discuss informed consent with community members in the informed consent module, the subject matter experts helped create the scenario and the dialogue used in the module based on their direct experience. Our partners from the health literacy nonprofit organization reviewed content for health literacy best practices, including plain language, and participated in creating animated vignettes that depicted what the informed consent process might look like within a community setting. We engaged our entire team to help ensure that these vignettes were as realistic and inclusive as possible. Our team met weekly to generate and review drafts of content and provide feedback and produce the finalized version for online evaluation with the CHW/P sample. After we developed the informed consent module, we conducted a qualitative study using focus groups to receive feedback on the look and feel of the course as well as the content [Reference Varma, Samuels and Piatt19]. In addition to these focus groups, we ensured that multiple stakeholders reviewed the content of each module as well as the presentation of the material online. Using the feedback, we adjusted all the course modules, adding short self-recorded video snippets in English and Spanish from CHW/Ps about their experiences in research.
Spanish course version development
The Spanish version of the course was developed in tandem with the English version. Consultants included native Spanish speakers who helped create content and vignettes. Our stakeholders supplied photos for the course to show settings where Promotoras work. All content was reviewed and translated into Spanish using native Spanish translators who had experience in communications and journalism, and the translation was adapted to the anticipated Spanish-speaking audiences. We used the World Health Organization process of translation and back translation with decentering [Reference Erkut21] and adaptation to ensure a high-quality translation of the Spanish version and one that will be understood by the intended audiences [22]. Any feedback from the group or participants regarding the translation of a particular word or phrase in the course content was reviewed by our expert translators, and a consensual decision was made based on knowledge of and experience working with the intended learners.
Recruitment
Participants were currently practicing CHW/Ps in either paid or volunteer positions. Recruitment for the English version of the online course evaluation launched in January 2023. One of the study’s principal investigators emailed requests to share the recruitment flyer and social media advertisement, including a study registration survey link, to the National Association of Community Health Workers (NACHW) and 10 state CHW/P associations across the country. Several organizations agreed to participate and shared the information with their networks. The initial recruitment response was high, with 248 individuals registering in the first week, forcing closure of registration because it far exceeded the recruitment goal of approximately 100 participants. Eligible participants were invited to take the course in the order that their registration forms were received. We offered a $25 e-gift card and certificate of completion to participants after completing the course. Due to the high number of registrations, particularly for the English version of the course, there were insufficient funds to compensate all those interested. Therefore, to give everyone who registered the opportunity to take the course, four additional options were offered: (1) completing the online English course with a certificate of completion but without a $25 e-gift card (12 participants chose this option), (2) completing the online Spanish course with a $25 e-gift card and certificate of completion (four participants chose this option), (3) enrolling in an upcoming facilitated course training (28 participants chose this option), and (4) not to take the course at all (six participants chose this option). Forty-nine individuals did not respond to any of the emails. Because not all people who expressed interest took the course, a second request for recruitment assistance was sent to the same CHW/P organizations in March 2023. Our team prioritized individuals interested in evaluating the Spanish language course, resulting in 36 additional registrations, yielding a total of 284 registrations. Fig. 1 shows details regarding CHW/P participation in the evaluation study.
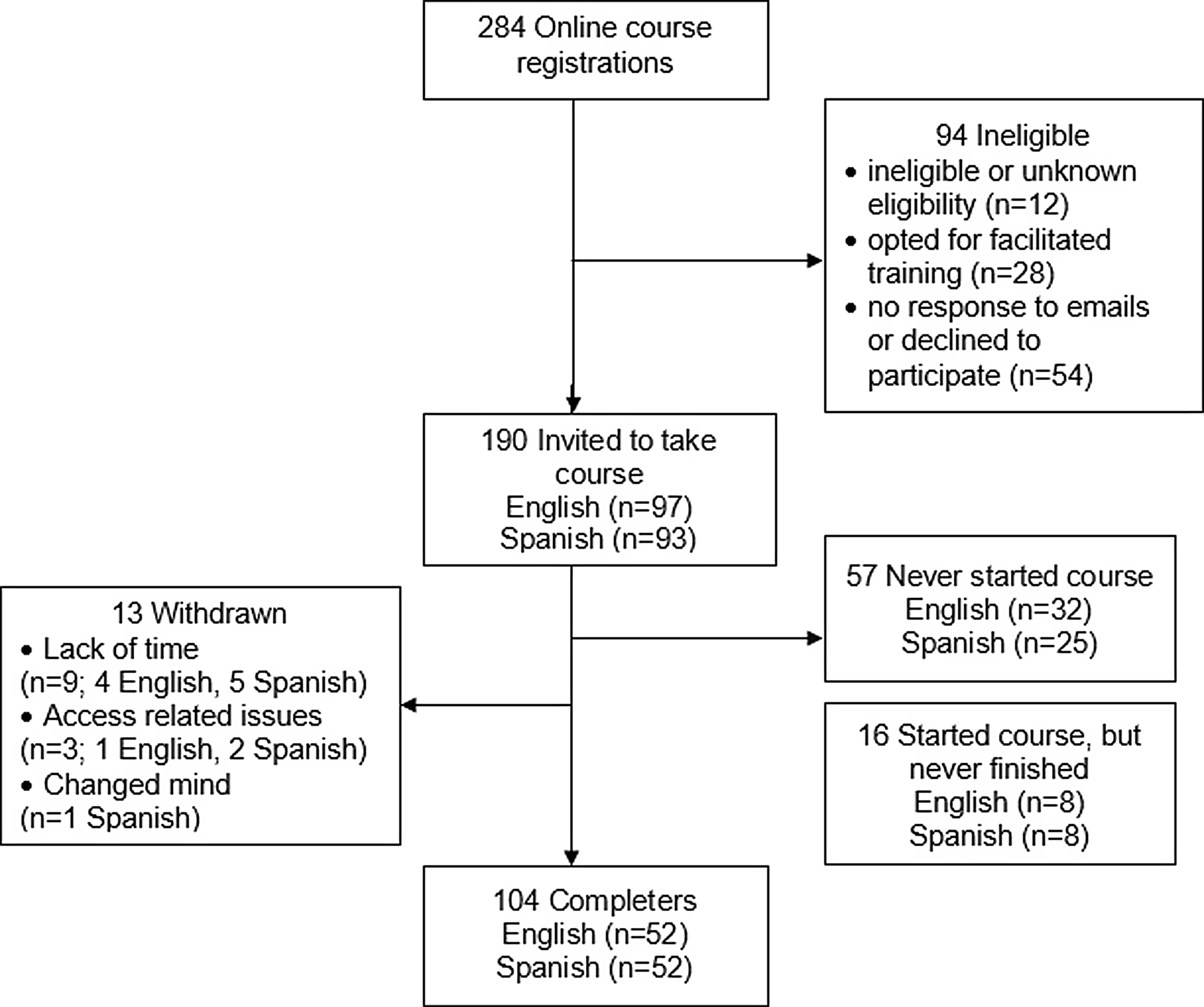
Figure 1. Participant flow chart.
Data collection
This study was determined exempt by the University of Michigan Institutional Review Board. The online registration form included the consent information, and all participants confirmed their understanding and interest in participating. To yield as broad a sample as possible, the only identifying information requested from participants in the registration form were names and email addresses.
We used Canvas, a web-based learning management system, to share the course with participants, which was accessible to them at any time. Participants were able to access materials at their convenience. Approximately once a week, the study team contacted participants who had registered but not started the course or those who started the course and become inactive for at least seven days. These participants were contacted up to three times to determine if they had questions and were still interested. The team communicated with participants who were responsive to the emails until they completed the course or chose to withdraw. Individuals who were nonresponsive to multiple email communications over several weeks were removed from the study.
After completing the online training, participants were sent a web link to the Qualtrics survey which was expected to take 5–10 minutes to complete. The survey included questions to self-rate abilities relevant to the training and perceptions about the usefulness of the training. The survey instrument was also reviewed by project stakeholders and translated into Spanish with the methodology previously described. Participants were also asked open-ended questions (with options to provide answers in English or Spanish) about how they might work more effectively because of the training and to provide any other comments on the course. Participant demographic data collected included age, gender, sex, race, ethnicity, work status, years of experience as a CHW/P, research experience, and educational attainment. All participants completed the online registration form before participating.
Data analysis
Descriptive analyses were performed to characterize the sample. Summary statistics were used to examine self-rated abilities and perceptions of the training. We then examined if self-rated abilities or perceptions varied by the English or Spanish version of the course using Chi-square tests as appropriate (p ≤ 0.05 indicating a significant difference). Finally, we conducted a qualitative latent content analysis [Reference Forman, Damschroder, Jacoby and Siminoff23,Reference Kleinheksel, Rockich-Winston, Tawfik and Wyatt24] to examine responses to the question, “How will you work more effectively as a result of this training?” We translated the Spanish transcripts into English, analyzed them, and developed codes based on words or short phrases, which we then categorized to create themes illustrating respondents’ perceived value of this training.
Results
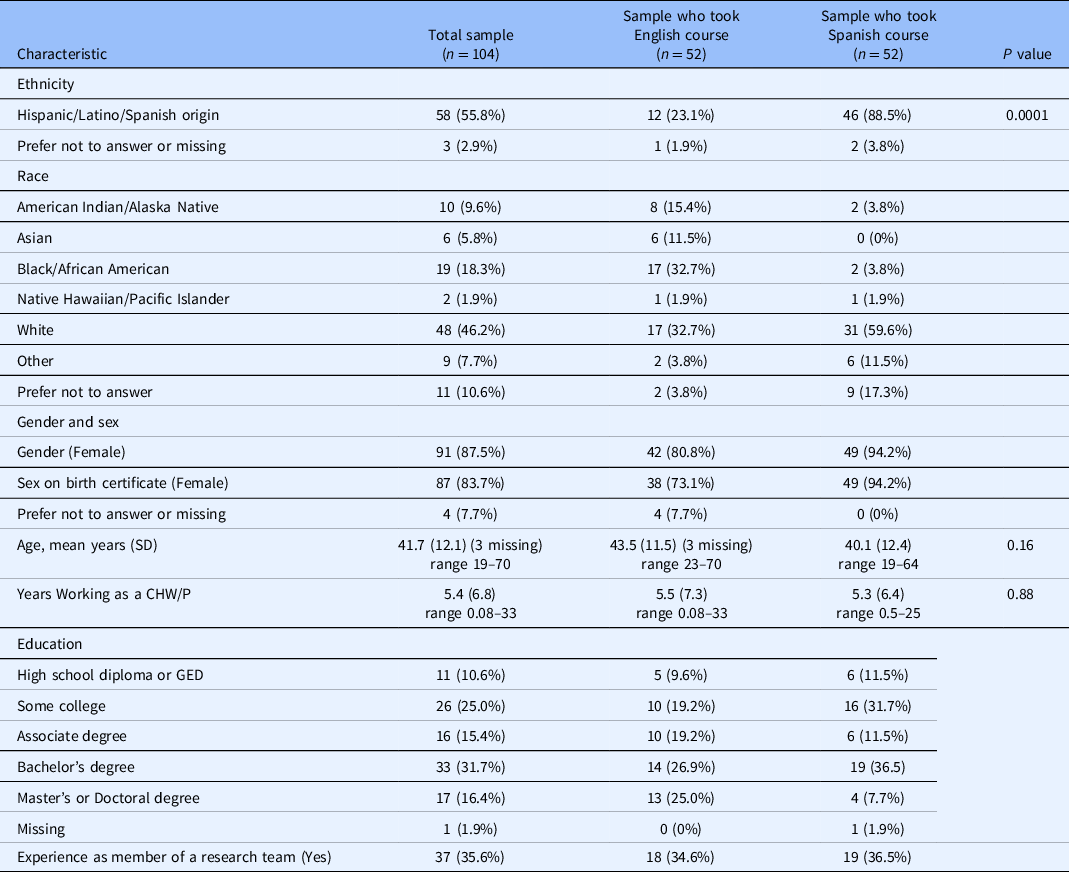
As shown in Table 2, 86% of the participants who completed the course identified as female with a mean age of 41.7 ± 12.1 years. Less than half identified as White (46%), with 18% who identified as Black, 10% who identified as American Indian/Alaskan Native, and 11% who declined to answer. More than half of the sample identified as Hispanic/Latino ethnicity (56%), of whom 79% completed the Spanish course. The majority of participants reported working as a CHW/P for five years or less (72%, range 1 month–33 years). There were 37 (35.6%) participants who reported having experience as a member of a research team.
Table 2. Sample characteristics (N = 104)
The median time it took to complete the online course was approximately 2 hours, with Spanish course takers needing 2 hours and 7 minutes on average, while English course takers needed, on average, 1 hour and 56 minutes. The course administration platform allowed people to take the course at their own pace. Of the course completers, 30% completed it in one day, an additional 32% completed it in one week, 14% in two weeks, 11% in three weeks, and the remaining 13% completed the course in four to seven weeks.
Between 96% and100% of respondents reported improvement (strongly or somewhat agreed) in self-rated abilities after the training (see Fig. 2). The most strongly agreed upon item was the ability to communicate how community-engaged research can address community health priorities. The least strongly agreed upon item was the ability to recognize adverse events and communicate about them with the study team. These ratings did not differ significantly across the English and Spanish versions of the course. Ratings also did not differ significantly based on whether they indicated having research experience as a member of a research team.

Figure 2. Self-rated abilities of CHW/Ps after training (N = 104).
Participants also had positive perceptions of the course overall (see Fig. 3). Most CHW/Ps (97%) agreed that the course was relevant to their work and felt the training was useful to their work (96%), which did not vary by which language version they completed. Those who completed the course in Spanish more strongly agreed that the training was useful to their work and that they would work differently because of the training. However, there were no significant differences in the overall patterns of agreement about perceptions of the course by group.

Figure 3. CHW/P perceptions of the course (N = 104).
We received responses to open-ended questions from 84 participants about how they thought they would work more effectively because of the training (see Table 3). Three themes emerged: (1) enhancing CHW/P skills, (2) expanding CHW/P resources, and (3) building bridges between communities and researchers. Regarding skills, the respondents most often reported that the training improved their communication with community members, including listening attentively and connecting responsibly. Some respondents also reported the course helped them to better understand the needs of the community. While some CHW/Ps reported that the course was a good refresher of their knowledge of research, others reported the course was helpful in learning about the role a CHW/P has in research.
Table 3. Content analysis of responses to: “How will you work more effectively as the result of this training?”

Responses from individuals could be in multiple categories.
Among a subset of those who completed the Spanish course, respondents mentioned that the course would help them better navigate how to create boundaries in communicating with people they interact with as part of research studies and who they also see in the community where they live. One person stated:
“El curso me dio apoyo que no sabia que necesitaba yo--el acuerdo que tener limites en medio del trabajo y mi vida privada son importantes y necesarios.”
“The course also gave me the support that I was not aware that I needed--the agreement to have limits between work and my private life, these are very important and necessary.”
Another participant mentioned that the course helped reduce the possible negative stigma about engaging in research. Regarding CHW/P resources, respondents mentioned that the course would be useful either as a tool to provide information to community members or as a personal resource that they could refer back to at a later time. A few respondents mentioned that having accurate information was important. For example, one person stated:
“As a Community Health Worker and with the many hats fellow CHW’s wear, if we’re not careful, items can go unchecked. (e.g., relying solely on social media and not being prepared to give accurate information). This user-friendly presentation study course can assist with circling back to many important factors which make CHWs resourceful, accessible, and important to their community.”
One person mentioned that the training could elevate the role that CHW/Ps have in the research process, thus helping to enhance the partnership between communities and researchers.
Although most respondents felt the course would help them work more effectively, eight participants reported that they would not work differently as a result of the training. Seven participants elaborated on this response. Three respondents reported they did not work directly with research in their jobs, two reported it was a review of information they already knew, and two felt information had been left out of the training. In particular, these participants mentioned that other topics about research and evaluation that CHW/Ps may be involved could be included. They also mentioned a lack of specific tailoring for the undocumented immigrant community, “whose needs and risk levels are somewhat unique within immigrant communities.”
Lastly, 41 people provided further feedback about the course. Most thanked us for developing the course, mentioned that they gained more knowledge or understanding because of it, or commented that they were eager to share the training with others. Areas for improvement identified were logistics related to course navigation, translation, closed captioning, and the use of videos.
Discussion
This article describes the development of a research best practices course for CHW/Ps as a step toward consistently preparing the CHW/P workforce to partner with researchers confidently and competently in conducting community-engaged research. The evaluation of the course revealed very positive responses in self-rated abilities to work more effectively as a result of the training and perceptions of the course’s relevance and usefulness. Given that the course evaluation did not differ by English or Spanish version, both appear to be highly acceptable to our intended learner groups. This may be a result of developing the course using a purposeful, highly participatory process with English- and Spanish-speaking members of the CHW/P community. Those who completed the course reported they gained skills, resources, and the ability to bridge between the community and researchers. The participants also offered examples that provide support for this course being attentive to cultural and linguistic tailoring for Promotoras. Specifically, only those who completed the course in Spanish highlighted the importance of lessons around setting boundaries between work and social settings when functioning in a research role as a CHW/P. Based on this feedback, instruction around this issue was added to subsequent versions of the course. This process highlights how the course was improved by embracing an inclusive strategy to course development.
While CHW/Ps are recognized for their value on research teams, this course was specifically developed to address practical information needed when CHW/Ps work with or as part of teams conducting research in community settings [Reference Terpstra, Coleman, Simon and Nebeker17]. This course specifically addresses recruitment, informed consent, and maintaining confidentiality, with the majority of participants agreeing that they gained skills in these areas. Importantly, participants reported the ability to better understand their role in research and to better communicate about research to community members.
The ability to understand one’s role on a research team as a CHW/P is crucial, as CHW/Ps often have unclear, multiple, or fluctuating job responsibilities [Reference Hohl, Thompson and Krok-Schoen15]. While the onus is on researchers to provide clarity and study-specific training of CHW/Ps in their job responsibilities, CHW/Ps need to have common, foundational knowledge in research and research training [Reference Hohl, Thompson and Krok-Schoen15 Reference Terpstra, Coleman, Simon and Nebeker–17]. In particular, the use of a standardized framework to train CHW/Ps for involvement in research teams is recommended [Reference Hohl, Thompson and Krok-Schoen15]. This course could potentially become the standardized training for CHW/Ps in research; however, there are a few considerations for optimal use. For this course evaluation, we did not establish a formal assessment of knowledge acquisition as a criterion for passing this course. Course completers only had to take a self-assessment to receive a certificate of completion. A more rigorous assessment of competency is recommended to ensure CHW/Ps’ perception of their abilities aligns with their actual skills. Nationally, there is no accepted standardized training for CHW/Ps [25], although there are efforts to define roles and the necessary competencies to fulfill those roles, including skills in better partnering for community-engaged research, assistance in program evaluation, and obtaining community consent in research [Reference Rosenthal E.L. and St. John26]. The course developed here does not map exactly onto these roles and competencies. Instead, this course provides more concentrated training on the role of CHW/Ps in a research study and how to communicate with community members about what being involved in research entails. We believe these skills are needed for the increasing role of CHW/Ps in research. The translation and adaptation of the modules into Spanish was an important step we took seriously. Half of the evaluation completers were Spanish speakers.
Strengths & Limitations
The CHW/P research best practices course was developed with a rigorous community-engaged participatory approach with careful attention to cultural and linguistic tailoring for Spanish-speaking communities. While this approach to course development was complex and lengthy, it yielded a course that is highly acceptable and relevant to both English and Spanish course takers. We had course takers from 26 out of 50 states, which supports some level of generalizability of the findings to a US sample of CHW/Ps. Because our translation and adaptation were only focused on developing a course for Promotoras in Spanish, further work is needed to develop culturally and linguistically appropriate training for CHWs working in other minoritized communities, such as the Chinese or Arabic communities. In this study, the course administration platform was a limitation. While it was chosen because it was determined to be the most accessible method for participants to access the course, Canvas had limited functionality and metrics to examine course experience, such as the time taken overall. Courses that function within dedicated learning management systems provide additional data that may be useful, such as tracked time in modules, and can support embedded knowledge checks and assessments.
Future Directions
As this course is also being offered using peer facilitators in English and Spanish, future evaluation work will be performed on the facilitated version of the course with CHW/P learners. This course will be broadly available via the website and through academic institutions supported by the Clinical and Translational Science Awards, and through our networks, such as PACER (Partners for the Advancement of Community Engaged Research of the Association for Clinical and Translational Science), but future studies will be needed to understand the implementation and sustainability of the online and facilitated versions of the course.
Conclusion
Given its highly reported relevance by both Spanish and English course takers, we believe this online course makes an important contribution to training resources available to CHW/Ps. Doing an appropriate translation and adaptation should be planned and budgeted from the go and not be an afterthought. This course may be useful as a standardized training for CHW/Ps nationally.
Acknowledgments
We thank our community stakeholders who participated in course development, those who translated the modules, and participants of this research project.
Funding statement
This project was supported by a grant from the National Center of Advancing Translational Sciences, National Institutes of Health (U01TR003409; MPIs Murphy, Aguilar-Gaxiola, Cottler) and supported by Clinical Translational Science Awards from the Michigan Institute of Clinical and Health Research (MICHR) (UL1TR002240), the University of California, Davis Clinical and Translational Science Center (UL1TR001860), and the University of Florida Clinical and Translational Science Institute (UL1TR001427). Dr. Alex Harper is a postdoctoral fellow funded by the University of Michigan’s Advanced Rehabilitation Research Training Award in Community Living and Participation (NIDILRR #90ARCP0003).
Competing interests
The authors have no conflicts of interest to declare.







 Open access
Open access