



Introduction
As an important life event in the life cycle, reproductive behaviours triggered not only individual physiological changes but also brought about changes in role-playing, social networks, and the environment they live in. This was closely linked to their health, a topic that has attracted a great deal of attention from scholars both nationally and internationally. Previous studies have found that parity can have both positive and negative effects on people’s health (Parikh et al., Reference Parikh, Cnattingius, Dickman, Mittleman, Ludvigsson and Ingelsson2010; Umberson et al., Reference Umberson, Pudrovska and Reczek2010; Huijts et al., Reference Huijts, Kraaykamp and Subramanian2011; Bai et al., Reference Bai, Wang, Yang, Tang, Wang and Han2017; Peters et al., Reference Peters, Yang, Guo, Chen, Bian, Millwood, Wang, Yang, Hu, Liu, Wang, Chen, Peto, Li, Woodward and Chen2017), with a large body of literature focusing on the psychological impacts of pregnancy and parity (Grundy et al., Reference Grundy, van den Broek and Keenan2017; Djundeva et al., Reference Djundeva, Emery and Dykstra2018; Li et al., Reference Li, He, Sun, Li, Zhai, Wang, Zhang and Lin2019). In Chinese culture, more children and larger families were often considered to be a blessing (Lee et al., Reference Lee, Chan, Hui and Chan2009). In China, with the development of urban and rural areas and the liberalisation of fertility controls, what was the association between number of children and parental well-being in later life, and whether it was in line with the relevant international findings, needed to be further explored. Of course, this had important theoretical and practical implications for the institutional construction of population and health policies in various countries.
Reproductive behaviour and mental health in later years
A review of the relevant literature revealed inconsistent associations between the reproductive behaviour and mental health, which were complicated by factors such as physical functioning, socio-economics, and lifestyle (Ryan et al., Reference Ryan, Carrière, Scali, Ritchie and Ancelin2008; Perquier et al., Reference Perquier, Ryan, Ancelin, Mesrine and Clavel-Chapelon2013; Tsai et al., Reference Tsai, Lin and Koo2017; Djundeva et al., Reference Djundeva, Emery and Dykstra2018).
The event of childbearing brought the role of parents into a new life course and influenced by traditional culture, childbearing could improve the life satisfaction of older people (He, Reference He2002). Some studies have found that older adults with no children and those with four or more children had poorer psychological status and were more likely to experience depressive symptoms and cognitive impairment than those with two children (Read & Grundy, Reference Read and Grundy2017; Keenan & Grundy, Reference Keenan and Grundy2018). On the one hand, in terms of group differences between having and not having children, depressive conditions may be worse among older people without children. However, the relevant research was not rich enough. On the other hand, in those groups of older people with children, an increased number of children may be associated with depression due to the realities of impaired physiological functioning, heavy family burdens, and unbalanced resource allocation. A study of a sample of older people in the UK found that deteriorating mental health was associated with having more children (Grundy & Read, Reference Grundy and Read2015). In Eastern European countries, the association between an increased number of children and depression in later life also existed and was influenced by marital status and the country’s economic development (Grundy et al., Reference Grundy, van den Broek and Keenan2017).
However, there were studies that did not support this. Based on data from the E3N follow-up survey, the association was found between the larger number of children and lower risk of depression for French women (Perquier et al., Reference Perquier, Ryan, Ancelin, Mesrine and Clavel-Chapelon2013). This similar association was found in a sample of Taiwanese women in China (Tsai et al., Reference Tsai, Lin and Koo2017). One study selected 10 regions (five urban and five rural) and again found that more children were associated with better mental health of their mothers (Wang et al., Reference Wang, Chen, Xin and Tang2019). In addition, there have been studies that have found no link between the number of children and depression in later life (Ryan et al., Reference Ryan, Carrière, Scali, Ritchie and Ancelin2008). Some studies have also concluded that parenthood did not affect the life satisfaction of either fathers or mothers (Keizer et al., Reference Keizer, Dykstra and Poortman2010). The association between number of children and fathers’ mental health appeared to be a little weaker than that of mothers, and inconclusive. In general, the combination of motherhood and work roles made mothers more susceptible to the ongoing stress of childbearing compared to fathers, and having children or even more children increased mothers’ negative emotions (Kim et al., Reference Kim, Lee, Shin, Choi and Park2015; Meier et al., Reference Meier, Musick, Flood and Dunifon2016; Roeters et al., Reference Roeters, Mandemakers and Voorpostel2016). Other studies have further sought to support the above view (Savolainen et al., Reference Savolainen, Lahelma, Silventionen, Gasuthier and Helence2001; Meier et al., Reference Meier, Musick, Flood and Dunifon2016).
Some scholars have also pointed out that the sex of children was an important variable when studying the relationship between reproductive behaviour and mental health. For mothers, having a son may consume more energy than having a daughter (Jasienska, Reference Jasienska2009). As male foetuses grew faster in utero, they were larger at delivery (Marsal et al., Reference Marsal, Persson, Larsen, Lilja, Selbing and Sultan1996; Loos et al., Reference Loos, Derom, Eeckels, Derom and Vlietinck2001) and had a higher need for breastfeeding (Hinde, Reference Hinde2007). Number of sons was positively associated with the rate of inflammation in the mother’s later years (Marttila et al., Reference Marttila, Nevalainen, Kananen, Jylhava, Jylha, Hervonen, Ilonen and Hurme2015). Epidemiological studies have shown that the number of sons was associated with shorter life expectancy (Helle & Lummaa, Reference Helle and Lummaa2013).
Number of children and sex of children had different effects on the mental health of older people, suggesting that both biological and social effect mechanisms were possible.
Mechanism of biological effect
The impact of reproductive behaviour on the health of parents in later life was mainly realised through biological effects and social effects. Biological effects were manifested in the impact of biological scars or physical imprints produced during pregnancy on health in later life. Obviously, this was for the mothers. Social effects emphasised the impact of children support, family resource distribution, and parenting burden.
In terms of biological mechanism, reproductive behaviour affected the maternal organism differently (Jasienska, Reference Jasienska2020), and poor physical health directly contributed to the onset of depression in later life (Fiske et al., Reference Fiske, Wetherell and Gatz2009). This was due to the trade-off between investing energy resources in reproduction and other metabolic functions (e.g. growth, somatic maintenance, and so on) (Kirkwood & Rose, Reference Kirkwood and Rose1991). If resources were limited, allocation to one function can only be at the expense of other functions (Zera & Harshman, Reference Zera and Harshman2001). One mechanism that allowed more resource energy to be allocated to reproduction was to reduce maternal basal metabolism (Peacock, Reference Peacock1991; Prentice et al., Reference Prentice, Poppitt, Goldberg and Prentice1995). A Chinese study chose hormone levels as mediating the link between high parity and depression in later life (Li et al., Reference Li, He, Sun, Li, Zhai, Wang, Zhang and Lin2019). Allocating resources for reproduction may make the supply to other metabolic functions inadequate, leading to impaired physiological function and increased risk of disease (Jasienska, Reference Jasienska2009). This was consistent with the Disposable Soma Theory that reproduction competed with resources for organismal maintenance and that high parity was associated with health disadvantage (Kirkwood, Reference Kirkwood1977). In addition, unlike mothers with sons, mothers with daughters consumed relatively little energy during pregnancy and delivery (Galbarczyk & Jasienska, Reference Galbarczyk and Jasienska2013).
Specifically, the biological response to the reproduction can lead to an increased risk of coronary heart disease and obesity in later life (Lawlor et al., Reference Lawlor, Emberson, Ebrahim, Whincup, Wannamethee, Walker and Smith2003; Bastian et al., Reference Bastian, West, Corcoran and Munger2005), and the repeated pregnancies may also affect lipid and glucose metabolism over time, leading to health problems such as obesity and atherosclerosis (Skilton et al., Reference Skilton, Serusclat, Begg, Moulin and Bonnet2009). Epidemiological studies have shown that pregnancy has a direct impact on women’s health in the long term. Women with high parity had poorer health status (Kington et al., Reference Kington, Lillard and Rogowski1997) and were also at higher risk of chronic diseases such as cardiovascular disease, endocrine disease, and certain cancers (Parikh et al., Reference Parikh, Cnattingius, Dickman, Mittleman, Ludvigsson and Ingelsson2010; Peters et al., Reference Peters, Yang, Guo, Chen, Bian, Millwood, Wang, Yang, Hu, Liu, Wang, Chen, Peto, Li, Woodward and Chen2016).
In addition, birth interval has also been shown to be associated with maternal health. Short birth intervals meant that the mother had not yet effectively recovered from the previous act of childbearing, while they also faced a higher stress level from sleep deprivation, postnatal depression, and financial burdens. In the analytical framework of life course epidemiology, these stressful events exposed to mothers themselves had a cumulative impact on mental health in later life.
Mechanism of social effect
For social mechanism, social factors such as socio-economic resources, partnerships, and social networks were also associated with depression in the late-adulthood (Fiske et al., Reference Fiske, Wetherell and Gatz2009; Virtanen et al., Reference Virtanen, Ferrie, Batty, Elovainio, Jokela, Vahtera, Singh-Manoux and Kivimäki2015). Pregnancy and parenting consumed parents’ energy, while bringing some financial strain and crowding them out of their social roles (Grundy & Read, Reference Grundy and Read2015). Social support theory suggested that individuals with more social support and close relationships had better health and lower mortality rates (Berkman & Syme, Reference Berkman and Syme1979; House et al., Reference House, Landis and Umberson1988).
Both personal beliefs (Lehrer et al., Reference Lehrer1995; Giavazzi et al., Reference Giavazzi, Schiantarelli and Serafinelli2013) and cultural practises (Antecol, Reference Antecol2000; Fernandez, Reference Fernandez2007; Almond et al., Reference Almond, Edlund and Milligan2013) had significant explanatory power for reproduction-related outcomes. In the context of traditional Chinese culture, the impact of having children on parents’ health in later life showed different cultural effects. On the one hand, there were positive cultural effects. Specifically, due to the presence of upward inter-generational support provided by children, older adults were able to obtain timely and adequate financial support, spiritual comfort, daily care services, and so on, which, in turn, were beneficial to their physical and psychological health. Inter-generational support in the late stages may have a greater impact on mothers’ health in later life than the cost of reproduction itself (Thomas & Thomeer, Reference Thomas and Thomeer2019). On the other hand, there were negative effects. Chinese parents often took on the task of starting a family and career development for their children. The life and financial pressure may continue until old age. In the elderly stage, they still worried and cared for their children and even continued to work, thus enduring greater stress both physically and mentally. Thus, the impact of having children on parental health was multi-directional due to cultural effects. For example, in rural China, both the financial support of children on whom they relied in later life and the spiritual consolation that came from family emotions were effective in alleviating the mental stress of parents in later life. Studies have shown that parents with large families were more likely to have regular face-to-face contact than parents with no or few children and that this higher level of face-to-face contact in turn reduced the risk of depression (Grundy & Read, Reference Grundy and Read2012; Tomassini et al., Reference Tomassini, Kalogirou, Grundy, Fokkema, Martikainen, Broese van Groenou and Karisto2004).
Among other socio-economic and lifestyle factors, region influenced the relationship between parity and depression. In urban areas, more children had a significant protective effect against depression, but in rural areas, this protective effect disappeared for both men and women (Wang et al., Reference Wang, Chen, Xin and Tang2019). This urban-rural difference may stem from different economic status and health levels (Tang, Reference Tang2010). Previous studies have shown that older people in rural areas were at higher risk of depression than those in urban areas (Wen et al., Reference Wen, Ren, Korinek and Trinh2019; Song, Reference Song2017).
In addition, many factors have an important moderating role in the association between reproductive behaviour and health in later life, such as marital status, socio-economic status of children (Yang et al., Reference Yang, Martikainen and Silventoinen2016), religious beliefs, reproductive culture, and so on. When discussing the health of older people in the context of Chinese society, grandchild care was a very important factor. On the one hand, grandchild care as an act of domestic labour created a physical burden on older adults and increased the risk of chronic disease (Minkler & Fuller-Thomson, Reference Minkler and Fuller-Thomson2005). Heavy caregiving also crowded out a great deal of older adults’ time and energy, leaving them with fewer opportunities to exercise and go to the hospital for treatment (Baker & Silverstein, Reference Baker and Silverstein2008), and thus they often did not have time to engage in self-health management (Burnette, Reference Burnette1999). In addition, grandchild care can also be directly detrimental to the mental health of older people, raising depression level (Whitley et al., Reference Whitley, Kelley and Sipe2001). Some studies have shown that intensive care made older adults’ socialization narrow, which negatively affected mental health. On the other hand, caring for grandchildren can alleviate the loneliness and dreariness of older people and increase their enjoyment of life (Goodman & Silverstein, Reference Goodman and Silverstein2002). Some studies have found that grandchild care significantly reduced depression levels and increased life satisfaction and subjective well-being in older people (He et al., Reference He, Tan and Xie2020).
Research contribution
The literature review indicated that most of the studies have been conducted in Western countries, while studies on Chinese samples were very few, especially for depression in older women. Considering that there were still a large number of farmers in China, it was of significance to select a sample of Chinese rural older people for this study. From data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS) in 2018, this study selected rural older women who have experienced pregnancy (i.e. at least one child) as the sample to investigate the effects of the number of children on depression and attempted to analyse the transmission channels involved. The major contribution of this study was to explore the effects of the number of children born early in life on mothers’ mental health in later life. Differences in the association between the sex of children and mothers’ late-life depression were explored by introducing cultural factors. In particular, cutting through the social perspective, this study attempted to explore the mechanisms, including the social activity effect, the child-feeding effect, and the health effect.
Method
Data
The data for this study were obtained from the 2018 CLHLS, which was a tracking survey of older people initiated by the Centre for Healthy Ageing and Development of Peking University and the National School of Development, and was the earliest and longest-running social science survey in China. This survey project conducted a baseline survey in 1998 and has been followed up eight times. It covered 23 provinces, municipalities, and autonomous regions across China. There were two types of questionnaires, one for surviving respondents and one for family members of the deceased. The former included basic information about older people and their families, financial status, cognitive function, and ability to perform daily activities. The latter focused on the death time and death cause of older people. This study mainly used the data provided by the surviving respondent questionnaire.
Combining the content and purpose of the study, older rural women aged 65 years and above with pregnancy experience (i.e. at least one child) were selected as main study population. Figure 1 illustrates the screening process for inclusion and exclusion of the study sample. After excluding irrelevant samples and missing values, a final sample of 3759 was obtained, including 1901 rural women and 1858 urban women (sample information was shown in Table 1). Figure 2 illustrates the distribution of the number of children in the urban and rural female samples.

Figure 1. Flow Chart of the Study Population Selection Process.
Table 1. Descriptive Statistics for Variables in the Female Sample
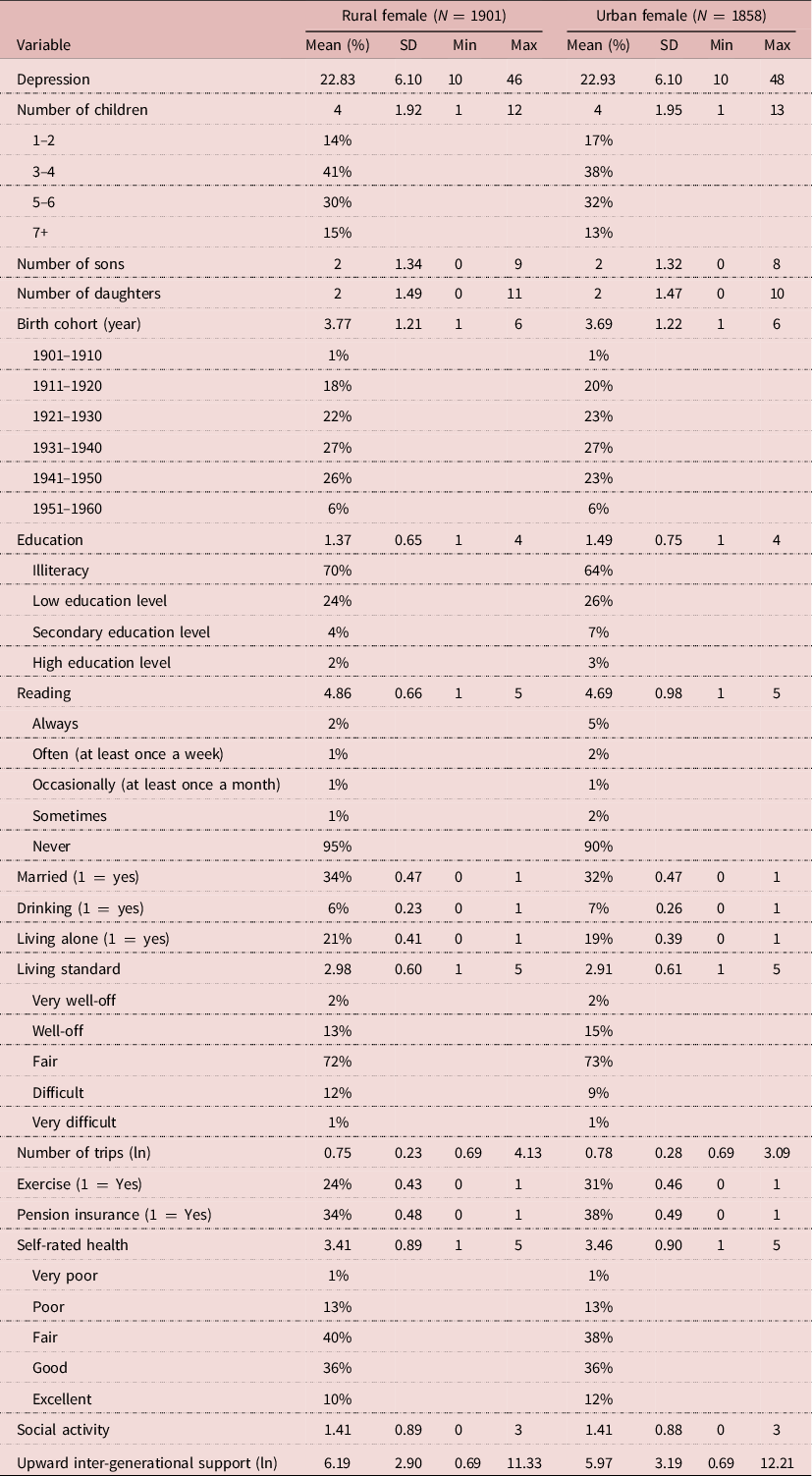
Note: Social activities included visiting friends, watching TV, listening to radio, and playing cards and mahjong. Upward inter-generational support mainly refers to the financial support provided by sons, daughters-in-law, daughters, and sons-in-law.

Figure 2. Distribution of the Number of Children of Urban and Rural Women.
In addition, to further test the representativeness of the study sample to the original database sample, we chose to compare the distribution of the number of children in the original database and the study sample. Figures 3 and 4 showed that this study sample was representative, and the study design was continued next.

Figure 3. Distribution of the Number of Children in the Study Sample.

Figure 4. Distribution of the Number of Children in the Original Database.
Variable design
Dependent variable
In the study, the dependent variable was the level of depression. The impact of the number of children on depression in rural older women was mainly in the areas of emotional state, loneliness, and sleep quality. In the 2018 CLHLS, participants were asked the related questions that measured an individual’s depression level, including ‘are you worried about some small things?’, ‘are you feeling sad or depressed?’, ‘are you full of hope for future life?’, ‘do you feel lonely?’, and so on. These questions made up the Center for Epidemiological Studies Depression scale that contained ten items (CES-D10). The CES-D scale, developed by Radloff (Reference Radloff1977), contained 20 items and was widely used to measure depressive symptoms in individuals. Here, the brief form containing three negative items and seven positive items used in this study had the same reliability and validity for the measurement of depressive symptoms in the Chinese population (Zhang & Li, Reference Zhang and Li2011; Ren et al., Reference Ren, Ma and Liu2014; Feng et al., Reference Feng, Guo and Liu2016).
Referring to existing literature (Lei et al., Reference Lei, Sun, Strauss, Zhang and Zhao2014; Zhang et al., Reference Zhang, Giles and Zhao2015; Zhou et al., Reference Zhou, Qin and Liu2018), each response under the negative item was assigned an integer between 1 and 5, and the response under the positive item was reverse-assigned a value. Finally, the scores were summed to obtain the individual’s depression score, with a range of 10–48. Higher scores represented more severe depression and poorer physiological health of the participants.
Independent variable
The independent variable was the number of children and did not include adopted children, using the question ‘how many children have you had in your lifetime (including those who have died)?’. It was important to clarify that the number of children in this study referred to the number of pregnancies that occurred early in the sample of older women and that have been delivered normally that is equivalent to going through the full course of pregnancy. Data from this study showed 86% of respondents who answered that they have six children or less, which was in line with the reality of the situation. Also, number of sons and daughters were added to the analysis to further explore the association between sex of children and depression level.
Mediating variable
In exploring the transmission channels through which the number of children affected with depression level, this study specifically selected three different channels for in-depth exploration: health effect, social effect, and feedback effect.
The first was the health channel, choosing self-reported health to test. Self-reported health was one of the commonly used indicators to measure the health status of the population. It was a comprehensive evaluation of people’s subjective feelings and objective health information about their physical, psychological, and social adaptation, which could reflect their health status in an intuitive and comprehensive way (Zhang & Fu, Reference Zhang and Fu2022). In the questionnaire, the responses to the question ‘how do you feel about your own health now?’ were assigned a value between 1 and 5, with higher value indicating poorer self-rated health of participants. The second was the social channel, choosing social activities to test. Participants were asked to answer the question ‘do you currently do or participate in the following activities?’, including ‘series, interact with friends’ ‘play cards/mah- jongg’, and ‘watch TV or listen to radio’. If the response was to participate, it was assigned a value of 1, otherwise it was assigned a value of 0. Social activity status was obtained by summing all responses and had a value range of 0–3. Higher value indicated a greater variety of activities participated in. The third was the feedback channel, choosing upward inter-generational support to test, mainly referring to financial support. Participants were asked ‘how much did you receive from your son(s) or daughter(s)-in-law last year?’ and ‘how much did you receive from your daughter(s) or son(s)-in-law last year?’. Responses were logarithmically processed to measure the support provided by the children.
Control variables
Referring to the studies of other scholars (Galbarczyk et al., Reference Galbarczyk, Klimek, Nenko and Jasienska2019; Grundy et al., Reference Grundy, Read and Väisänen2019; Wang et al., Reference Wang, Chen, Xin and Tang2019; Yang et al., Reference Yang, Wu, Zhang and Zhang2021), birth cohort, education, reading, married, drinking, living alone, living standard, number of trips, exercise, and pension insurance were selected as control variables from multiple perspectives, including individual characteristics, lifestyle, and family status. The specific definitions and assignments of variables are shown in Appendix Table A1.
Model Setting
Based on the specifics of this study, we set up the following models. Here, models were estimated and analysed in this study using Stata 15.0 software.
Ordinary least square
In this study, the depression score was treated as a continuous variable (Lei et al., Reference Lei, Sun, Strauss, Zhang and Zhao2014; Zhou et al., Reference Zhou, Qin and Liu2018). Therefore, the ordinary least square (OLS) was used to estimate the association between number of children and depression. The specific model was set up as follows:
 $${\rm{Depressio}}{{\rm{n}}_{it}} = {\alpha _0} + {\alpha _1}{\rm{Nu}}{{\rm{m}}_{it}} + {\alpha _2}{X_{it}} + {\varepsilon _{it}},$$
$${\rm{Depressio}}{{\rm{n}}_{it}} = {\alpha _0} + {\alpha _1}{\rm{Nu}}{{\rm{m}}_{it}} + {\alpha _2}{X_{it}} + {\varepsilon _{it}},$$
where
 ${\rm{Depressio}}{{\rm{n}}_{it}}$
denoted the participant’s depression score;
${\rm{Depressio}}{{\rm{n}}_{it}}$
denoted the participant’s depression score;
 ${\rm{Nu}}{{\rm{m}}_{it}}$
denoted number of children born to the participant, including the total number of children, number of sons, and number of daughters;
${\rm{Nu}}{{\rm{m}}_{it}}$
denoted number of children born to the participant, including the total number of children, number of sons, and number of daughters;
 ${\alpha _1}$
was the core coefficient to be estimated in the study;
${\alpha _1}$
was the core coefficient to be estimated in the study;
 ${X_{it}}$
were other control variables;
${X_{it}}$
were other control variables;
 ${\alpha _2}$
indicated the coefficients of a set of control variables, respectively;
${\alpha _2}$
indicated the coefficients of a set of control variables, respectively;
 ${\alpha _0}$
denoted the constant term; and
${\alpha _0}$
denoted the constant term; and
 ${\varepsilon _{it}}$
denoted the random error term.
${\varepsilon _{it}}$
denoted the random error term.
Mediating mechanism
The possible mediating effects in Equation (1) were tested by referring to the practises of other scholars (Judd & Kenny, Reference Judd and Kenny1981; Baron & Kenny, Reference Baron and Kenny1986; Wen et al., Reference Wen, Chang, Hau and Liu2004; Lv & Liu, Reference Lv and Liu2020). First, all selected mediating variables were put into the same model to make a preliminary judgement on their transmission effects. Then, number of children was regressed on each of the mediating variables separately. Finally, the relative contribution of each channel was obtained. Based on this, the following models were established.
 $${M_i} = {\beta _0} + {\beta _1}Nu{m_{it}} + {\theta _{it}} + {\omega _{it}},$$
$${M_i} = {\beta _0} + {\beta _1}Nu{m_{it}} + {\theta _{it}} + {\omega _{it}},$$
 $${\rm{Depressio}}{{\rm{n}}_{it}} = {\gamma _0} + {\gamma _1}{\rm{Nu}}{{\rm{m}}_{it}} + {\gamma _2}{M_i} + {\gamma _3}{X_{it}} + {\delta _{it}},$$
$${\rm{Depressio}}{{\rm{n}}_{it}} = {\gamma _0} + {\gamma _1}{\rm{Nu}}{{\rm{m}}_{it}} + {\gamma _2}{M_i} + {\gamma _3}{X_{it}} + {\delta _{it}},$$
where
 ${M_i}$
denoted the mediating variables, including self-reported health, social activity, and upward inter-generational support;
${M_i}$
denoted the mediating variables, including self-reported health, social activity, and upward inter-generational support;
 ${\beta _1}$
was the coefficient of the effect of number of children on mediating variables;
${\beta _1}$
was the coefficient of the effect of number of children on mediating variables;
 ${\beta _0}$
and
${\beta _0}$
and
 ${\gamma _0}$
were the constant terms of Equations (2) and (3), respectively;
${\gamma _0}$
were the constant terms of Equations (2) and (3), respectively;
 ${\theta _{it}}$
denoted the control variables;
${\theta _{it}}$
denoted the control variables;
 ${\gamma _1}$
denoted the coefficient of effect of number of children on depression after the inclusion of mediating variables, indicating the direct effect after accounting for mediating effects; and
${\gamma _1}$
denoted the coefficient of effect of number of children on depression after the inclusion of mediating variables, indicating the direct effect after accounting for mediating effects; and
 ${\gamma _2}$
denoted the coefficient of the effect of mediating variables on depression after the including of number of children.
${\gamma _2}$
denoted the coefficient of the effect of mediating variables on depression after the including of number of children.
 ${\gamma _3}$
also indicated the coefficients of a set of control variables, respectively. Both Equations (2) and (3) were estimated using OLS model. In the decomposition of the mediating effect, Equation (2) was substituted into Equation (3) to obtain Equation (4).
${\gamma _3}$
also indicated the coefficients of a set of control variables, respectively. Both Equations (2) and (3) were estimated using OLS model. In the decomposition of the mediating effect, Equation (2) was substituted into Equation (3) to obtain Equation (4).
 $${\rm Depression}_{it} = \gamma _0 + \gamma _2\beta _0 + (\gamma _1 + \gamma _2\beta _1){\rm Num}_{it} + \gamma _2\theta _{it} + \gamma _3X_{it} + \varepsilon'_{it},$$
$${\rm Depression}_{it} = \gamma _0 + \gamma _2\beta _0 + (\gamma _1 + \gamma _2\beta _1){\rm Num}_{it} + \gamma _2\theta _{it} + \gamma _3X_{it} + \varepsilon'_{it},$$
where
 ${\gamma _1}$
denoted the direct effect of number of children on depression and
${\gamma _1}$
denoted the direct effect of number of children on depression and
 ${\gamma _2}{\beta _1}$
denoted the indirect effect of number of children on depression through mediating variables. It can be seen that the relative contribution of each transmission channel was as follows:
${\gamma _2}{\beta _1}$
denoted the indirect effect of number of children on depression through mediating variables. It can be seen that the relative contribution of each transmission channel was as follows:
 $${\sigma _1} = {{{\gamma _1}} \over {{\gamma _1} + {\gamma _2}{\beta _1}}},$$
$${\sigma _1} = {{{\gamma _1}} \over {{\gamma _1} + {\gamma _2}{\beta _1}}},$$
 $${\sigma _2} = {{{\gamma _2}{\beta _1}} \over {{\gamma _1} + {\gamma _2}{\beta _1}}}.$$
$${\sigma _2} = {{{\gamma _2}{\beta _1}} \over {{\gamma _1} + {\gamma _2}{\beta _1}}}.$$
Results
Basic descriptive analysis
Table 1 presents the descriptive results of the variables for the female sample. In this study, there were 1901 rural women and 1858 urban women, accounting for approximately half each. Depression scores ranged from 10 to 46 among rural women and 10 to 48 among urban women. The mean value of the former was 22.83 and the latter was 22.93, indicating that the average depression level would be a little higher in the urban female group. For number of children, the mean value was 4 for both rural and urban women, with the maximum value of 12 for rural female sample and 13 for urban female sample, which was consistent with the family structure in our national context. Specifically, the sample of women with three to four children had the highest percentage in both rural (41%) and urban areas (38%), followed by five to six children (30% and 32%, respectively). The mean value for both number of sons and daughters was about 2.
According to the birth cohorts, it could be found that 1921–1930, 1931–1940, and 1941–1950 birth cohorts had higher percentages of samples. The mean age of the rural and urban female samples was 85 and 86 years, respectively. 70% of rural women and 62% of urban women were in a state of illiteracy, meaning they had no education, and the vast majority said they did not usually read. About one-third of the samples was married with a spouse status. Most samples considered their standard of living to be average compared to other local people. Less than one-third of samples exercised regularly. The vast majority do not have pension insurance.
Baseline regression results
Regression analyses were conducted based on a sample of rural older women who had children, and the results are shown in Table 2.
Table 2. Estimates of the Effect of Number of Children on Depression in Rural Older Women

Note: Older rural women with at least one child were used as study population; the ordinary least square (OLS) is used to estimate above models; *, **, or *** indicated a significance level at 10%, 5%, and 1%, respectively; standard errors are reported in parentheses.
The results of Model 1 showed a coefficient of 0.272 (p < 0.01) for a number of children before the inclusion of control variables, indicating that an increase in the number of children led to higher depression scores. Adding the control variables to the model to obtain Model 2, it was found that the regression coefficient for number of children decreased to 0.177 (p < 0.05) and still passed the significance test, indicating that an increase in the number of children does lead to poorer health and increased levels of depression. Specifically, each additional child was associated with an increase in depression score of 0.177 units. Further, in Model 3, the number of children was treated as four groups. When the one to two children groups were used as the reference group, the regression coefficients for three to four, five to six, and seven or more children were all positive, and the coefficient was especially larger and more significant for the seven and more children group, suggesting that older women with more children would show higher depression level.
Models 4 and 5 showed the association between number of sons or daughters and depression level. In addition, to try to avoid bias in the effect of sex of child on the regression results, when exploring the association between number of sons on depression level, the number of daughters was simultaneously controlled, and vice versa. Model 4 demonstrated that an increase in the number of sons or daughters was significantly associated with increased levels of depression in rural older women. After adding the control variables, Model 5 indicated that the regression coefficient for the number of sons was 0.135, although insignificant, while the coefficient for the number of daughters was 0.208 (p < 0.05) and passed the significance test. It could be found that an increase in the number of sons or daughters could be detrimental to the mental health of rural older women and aggravate their depression levels. By comparing the absolute value and significance of the coefficients, it was clear that the positive association between number of daughters and depression levels was stronger. In other words, an increase in number of daughters may lead to a higher level of depression.
The results in Table 2 showed that most control variables were significantly associated with depression level. For living arrangement, there was a stronger association between living alone and depression level in older women. Family support theory suggested that older adults who lived with their children received more support in all areas, which enhanced physical and mental health. One study using Chinese older adults found that living alone worsened their mental health and significantly increased their depression levels (Jiang & Sun, Reference Jiang and Sun2022). Similar findings have been found in foreign studies, for example, a study of older adults in Singapore showed that older adults who lived alone and had poor social networks had higher depression levels than those who lived with their children (Chan et al., Reference Chan, Malhotra, Malhotra and Stbye2011). Older women with the lower standard of living may feel higher depression level compared to other locals. Self-assessment of the standard of living was often done with reference to their income level and household economic status, among others. In a study by O’Neil et al. (Reference O’ Neill, Sorhaindo, Xiao and Garman2005), 40% of residents reported that their health was affected to some extent by economic problems and that they had mental health problems such as depression and anxiety. It was found that high-income earners had more positive emotions, while low-income earners had more negative emotions (Bradburn, Reference Bradburn1969). Further, the effect of income was relative. Easterlin (Reference Easterlin1974) found that subjective perceptions of economic level played a greater role than income itself. In addition, compared to those not having pension insurance, the association between having pension insurance and lower level of depression in older women was stronger. In 2012, China’s social pension insurance achieved full system coverage. Taking China’s New Rural Social Pension Insurance policy as an example, many existing studies have found that the pension income under this policy has reduced poverty and increased subjective well-being to some extent and that older people in poorer health were more affected by the policy (Pei & Pillai, Reference Pei and Pillai1999; Zhang & Chen, Reference Zhang and Chen2014; Zurlo et al., Reference Zurlo, Hu and Huang2014). It was found that this pension insurance significantly increased the financial independence of older rural people. Similarly, Galiani et al. (Reference Galiani, Gertler and Bando2016) found that the Mexican pension system improved the mental health of older adults and reduced depression values.
Mediating effect analysis
Combined with the above analysis, after referring to other studies (Wen et al., Reference Wen, Chang, Hau and Liu2004; Lv & Liu, Reference Lv and Liu2020), this study sought to explore the mediating transmission mechanisms between number of children and depression level in rural older women, as shown in Tables 3–5 of the specific results.
Table 3. Estimation Results of Mediating Effect
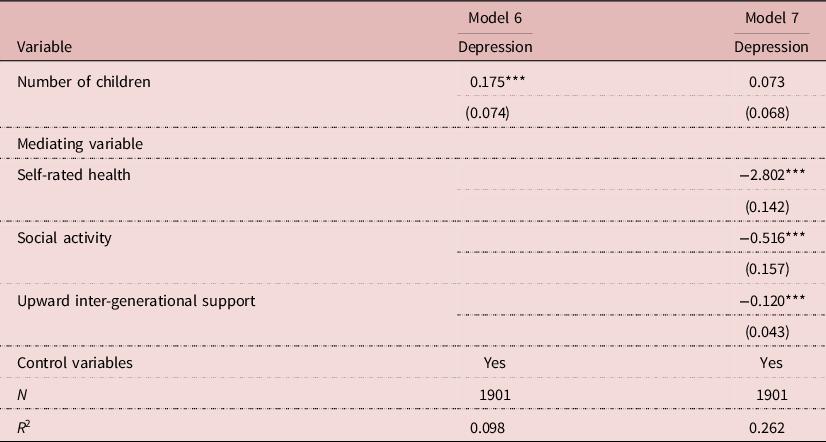
Note: Older rural women with at least one child were used as study population; birth cohort, education, reading, married, drinking, living alone, living standard, number of trips, exercise, and pension insurance are under control; *, **, or *** indicated a significance level at 10%, 5%, and 1%, respectively; standard errors are reported in parentheses.
Table 4. Regression Estimates of number of Children on the Mediating Variables
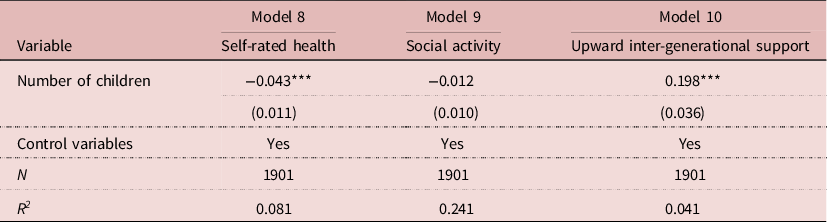
Note: Older rural women with at least one child were used as study population; birth cohort, education, reading, married, drinking, living alone, living standard, number of trips, exercise, and pension insurance are under control; *, **, or *** indicated a significance level at 10%, 5%, and 1%, respectively; standard errors are reported in parentheses.
Table 5. Results of Effect Decomposition
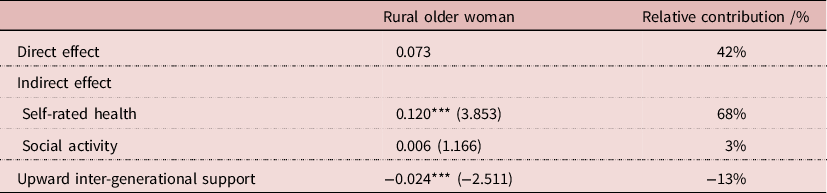
Note: Older rural women with at least one child were used as study population; *, **, or *** indicated a significance level at 10%, 5%, and 1%, respectively; the Z-sobel statistic is reported in parentheses.
In Table 3, Model 6 reported the results of estimating the effect of the number of children on depression level when the control variables were added to the model but mediating variables were not included. Model 7 was obtained by adding mediating variables, and it was found that the regression coefficient of the number of children decreased from 0.175 to 0.073, although the latter was not significant. From this, it could be found that indirect channels through self-reported health status, social activity status, and inter-generational support of children could explain to a greater extent the effect of the number of children on depression. Specifically, self-reported health, social activity, and upward inter-generational support were all significantly associated with depression levels in older women (p < 0.01). Poorer self-reported health, fewer social activities, and less inter-generational support from children were significantly associated with higher depression scores, that was, they showed higher depression levels.
Table 4 reports the estimation results of the effect of the number of children on mediating variables. Model 8 demonstrated the regression coefficient of −0.043 (p < 0.01) for a number of children, indicating a significant negative association between number of children and self-reported health. In Model 9, the coefficient of the number of children was 0.012, indicating a negative but insignificant association between number of children and social activities. The results of Model 10 showed a coefficient of 0.198 (p < 0.01) for a number of children, indicating that the number of children showed a significant positive association with inter-generational support.
To ensure the reliability of mediating effect test results, this study used the Bootstrap sampling method to test the mediating effect, which was a coefficient product test, and the specific Z-statistics were reported in parentheses in Table 5. In addition, Table 5 reported the results of specific effect decomposition.
The results showed that the |Z| for both self-reported health and upward inter-generational support were greater than 1.65, indicating that the number of children had a significant effect on their depression levels through these two channels among the study population. However, the |Z| for social activity was less than 1.65, indicating that the mediating effect of this variable was not significant in this study. Considering that the social activities in this study only included three categories: hanging out with friends, playing cards and mahjong, and watching TV and listening to the radio, it did not define this variable more comprehensively, which in turn may have influenced the test results. Not surprisingly, 58% of the effects of the number of children on depression were generated through mediating variables, with the rest showing a direct effect. Specifically, poorer self-reported health and fewer social activities exacerbated the depression level, with relative contributions of 68% and 3%, respectively. More financial support from children reduced the level of depression with a relative contribution of −13%.
Further analysis
Through a review of relevant literature, the association between number of children and depression level in older women may show differences in urban and rural samples (Dew & Wilcox, Reference Dew and Wilcox2011; Wang et al., Reference Wang, Chen, Xin and Tang2019; Yang et al., Reference Yang, Wu, Zhang and Zhang2021). Therefore, the study population was replaced with urban older women with children for further analysis in an attempt to explore the urban–rural differences. Also, to ensure the completeness and reliability of the regression results, a simple comparative analysis was conducted by analysing the full women sample and urban women sample. The specific results are shown in Tables 6 and 7, respectively.
Table 6. Estimates of the Effect of Number of Children on Depression in Total Older Women

Note: Total older women with at least one child were used as study population; the OLS is used to estimate above models; birth cohort, education, reading, married, drinking, living alone, living standard, number of trips, exercise, and pension insurance are under control; *, **, or *** indicated a significance level at 10%, 5%, and 1%, respectively; standard errors are reported in parentheses.
Table 7. Estimates of the Effect of Number of Children on Depression in Urban Older Women

Note: Older urban women with at least one child were used as study population; the OLS is used to estimate above models; birth cohort, education, reading, married, drinking, living alone, living standard, number of trips, exercise, and pension insurance are under control; *, **, or *** indicated a significance level at 10%, 5%, and 1%, respectively; standard errors are reported in parentheses.
The regression results for the full sample of females are shown in Table 6. It was not difficult to find that the regression results for the full sample and rural female sample remained consistent. In other words, there was a significant association between an increase in the number of children and an increase in depression score, i.e., more children increased the depression level in older women. According to Model 13, when one to two children groups were used as the reference group, it was found that women with three to four, five to six, or seven or more children had higher depression scores. By comparing the magnitude of the coefficient values, the higher the number of children (especially seven and above), the higher level of depression in older women. For the sex of children, an increase in number of either sons or daughters was significantly associated with higher levels of depression. The coefficient size and significance results suggested a greater exacerbating effect of number of daughters on depression in older women.
Table 7 presents the regression results in the urban women sample with children as the study population. In Model 17, the regression coefficient of the number of children was positive, indicating that there was an association between more children and an increase in depression level among older urban women, which was consistent with the results for the rural women sample. There were two differences worth noting. One of them was shown in Model 18. It was found that when the one to two children groups were used as a reference, the coefficients for all other child subgroups were positive, but older urban women with five to six children may show higher depression level, followed by the group with three to four children. Another point was expressed in terms of sex of children. Model 19 showed an association between an increased number of either sons or daughters and increased depression in urban older women, which was consistent with the results for the rural women sample. When control variables were added, Model 20 showed that the coefficient on number of sons became negative, but its absolute value was smaller. This suggested that the effect of increasing number of sons on depression in older urban women was different across settings. Context-specific analysis was required.
Discussion
More children significantly associated with depression in older rural women
In rural China, for older women with children, an increase in the number of children significantly exacerbated their depression levels. In the group of women with children, compared with one to two children, having more children was often associated with more severe depressive conditions. It was consistent with most existing research results.
On the one hand, this was due to the existence of the trade-off between reproduction and health. Specifically, women had limited resources in their bodies, and when allocating energy resources to reproduction, this inevitably reduced the supply of energy for their other metabolic functions (Peacock, Reference Peacock1991; Prentice et al., Reference Prentice, Poppitt, Goldberg and Prentice1995; Jasienska, Reference Jasienska2009). The Disposable Somatic Theory suggests that reproduction competes with resources to sustain organismal growth and that high parity can cause health problems (Kirkwood, Reference Kirkwood1977). Most studies have found that as the number of children increased, women may be at increased risk of cancer and chronic diseases, including stomach, brain, and cervical cancers, as well as heart disease and diabetes (Parikh et al., Reference Parikh, Cnattingius, Dickman, Mittleman, Ludvigsson and Ingelsson2010; Peters et al., Reference Peters, Yang, Guo, Chen, Bian, Millwood, Wang, Yang, Hu, Liu, Wang, Chen, Peto, Li, Woodward and Chen2016; Bai et al., Reference Bai, Wang, Yang, Tang, Wang and Han2017; Peters et al., Reference Peters, Yang, Guo, Chen, Bian, Millwood, Wang, Yang, Hu, Liu, Wang, Chen, Peto, Li, Woodward and Chen2017). The presence of depressive symptoms was associated with certain physical health disadvantages, and the cumulative health disadvantages associated with high parity can lead to a high incidence of depression in later life.
On the other hand, the different family divisions of labour tended to make Chinese women take on more family caregiving responsibilities, leading to a lack of social support, which hindered career development and reduced personal leisure and consumption. Mirowsky (Reference Mirowsky1988) noted that women who had difficulties in caring for their children had higher levels of depression. However, older people could also receive more financial support, spiritual comfort, and daily care from more children in their later years, which increased their subjective well-being and thus benefited their mental health (Mu & Xie Reference Mu and Xie2014; Zhang et al., Reference Zhang, Lin and Zhang2018). Thus, from a social point of view, the impact of the number of children on mothers’ mental health in later life is multi-directional and varies across regions and groups.
In the context of Chinese society, especially in rural areas, grandchild care and traditional cultural practises (supporting parents, respecting older people, and so on) were important factors that had to be taken into account. Specifically, grandchild care could increase the physical burden on older people, increase the risk of chronic disease, and take up time and energy. Grandchild care can also be directly detrimental to the mental health of them, increasing levels of depression. At the same time, grandchildren care could alleviate the loneliness and dreariness of old age and add to the enjoyment of life. In order to raise more children, parents were under greater life and financial pressure and expended more energy. At the same time, adult children often fulfil their obligation to support their parents by providing them with financial support and daily care.
It needed to be made clear that reproductive behaviours such as the number of children were only one of the influences on mothers’ mental health in later life. In addition to the above, healthy habits, adequate security in old age, and a rich life in old age all have an impact.
Differences in the association between sex of children and depression in older rural women
An increase in the number of daughters significantly exacerbated depression among older rural women, while the worsening effect of an increase in the number of sons on depression was much smaller and the result was not significant.
When discussing the sex of children and health in old age in the context of Chinese rural society, among all the influencing factors, traditional cultural customs cannot be ignored.
In terms of having daughters, the positive cultural effects were mainly manifested in the excellent traditional culture of respecting older people, and children have the obligation to support their parents. In other words, older people would receive financial support, spiritual comfort, and daily care services from their children, which were beneficial to their physical and mental health. Negative cultural effects were more often seen in the traditional concept of reproduction that favours sons over daughters, especially in rural areas of China. Under the influence of this fertility culture, a family would choose to continue to have children until they had a son, which meant more daughters. A family was keen to have more sons than daughters. More daughters meant that the mother may be under more pressure to bear children, which in turn was detrimental to her physical and mental health. With the combination of these different effects, in the sample of rural elderly women in this study, the negative cultural effect of daughters outweighed the positive effect, indicating that the more daughters there are, the more depression in later life will worsen. Thus, to some extent, the positive feedback effects of daughters were much smaller than the negative effects such as impaired physical health and reduced social support.
In terms of having sons, in addition to the positive cultural effects mentioned above, under the influence of traditional concept of having more children and more blessings and preferring sons to daughters in rural China, having sons directly increased older people’s sense of well-being. In addition, family care remained the choice of the vast majority of older people. In the social context of the time, daughters left their families through marriage when they reached adulthood, and sons were often the main source of financial support and spiritual comfort for parents in their later years (Yang, Reference Yang2019). As a result, under the concept of raising sons for old age, sons usually took on the responsibility of caring for them, and parents preferred to have more sons to ensure their old age (Ebenstein & Leung, Reference Ebenstein and Leung2010). The negative effect was mainly manifested in the fact that Chinese parents often took on the task of family and career for their children, especially sons. Life and financial pressure continued into old age. They still worked hard for their children in the old age and even continued to work, resulting in significant physical and mental stress. Based on this, the positive feedback effects of sons were somewhat offset by negative effects such as impaired physical health and reduced social support. In summary, compared to sons, daughters had a greater negative effect on the health of mothers.
Number of children was associated with depression in older rural women through both biological and socio-economic mechanisms
First, an increase in the number of children decreased self-rated health, which in turn increased depression levels. This was consistent with the Disposable Soma Theory, where high parity led to poor physiological health (Kirkwood, Reference Kirkwood1977), accumulating a poor health base for the onset of depression. As the reasons for poor self-rated health, there were bound to be other relevant factors in addition to the accumulation of physical health disadvantages that may have resulted from early reproductive events. Specifically, the increased stress of life associated with raising more children may continue into later life, and grandchildren care may affect their physical and mental health, and so on. This study did not explore the specific reasons in detail. Thus, in terms of the biological effect mechanism, the larger the number of children born, the greater the negative impact on the physical health of mothers, and thus on the mental health in later life.
Second, more children exacerbated depression by reducing the mother’s social activities. This was because more children bring with them a greater burden of nurturing and caregiving, crowding out personal leisure time, and leading to reduced social participation. At the same time, long-term family roles would affect other social roles, thus limiting access to social support, which led to depression.
Finally, more children brought with it an increase in inter-generational support in later life, an effect that inhibited the onset of depression in older women. In rural China, older people often choose family care. They could receive more financial support, spiritual comfort, and daily care from a larger number of children, which reduced the stress of later life and thus contributed to physical and mental health.
Negative association between number of children and depression of older urban women
There was also a correlation, although not significant, between the increase in the number of children born and depression in older urban women.
This may be due to the dual urban–rural structure in China, which has led to an imbalance in development between urban and rural areas, as reflected in differences in the economic level, social development, public health service, and so on. In terms of physiological factors, most urban women were mandated to enrol in maternity insurance, which provided them with basic reproductive health care. This has, to a certain extent, improved the accessibility of health-care services, thereby ensuring the maintenance of better physiological health. In terms of social factors, regional development may bring high-economic income and available childcare services. The former can to some extent alleviate the pressure of raising children in daily life. The latter was conducive to weakening the crowding-out effect of taking care of children on the personal development of mothers, thereby having more time and energy for social participation and obtaining more social support. This will all be beneficial to their health in later years. In addition, economic development inevitably led to higher health consciousness as well. This was consistent with Maslow’s Hierarchy of Needs theory. There was no doubt about the influence of scientific and correct health concept on individual health, such as exercising, eating a balanced diet, and seeking timely medical treatment. Therefore, under the combined influence of various factors, compared to rural older women, more children may exacerbate depression in urban older women, but this impact was smaller and not significant.
Conclusion
The traditional notion of ‘more children and more blessings’ has always been deeply rooted, and a large family with more children was often regarded as a symbol of happiness. In China’s current rapidly developing society, the link between more children and health in later life deserves a serious answer.
Based on data from the 2018 CLHLS, older women with children were included in the study. It was found that there was a significant adverse effect of the number of children on depression in rural older women. This effect was also present in the urban mother samples, though not significant. There were differences in the association between the sex of children and maternal depression in later life. The worsening effect of an increased number of daughters on depression was stronger compared to sons. The direct effect of the number of children exacerbating depression levels accounted for approximately 42%. In terms of indirect effects, self-rated health and social activity explained about 68% and 3% of the exacerbating effects of depression, respectively, and upward inter-generational support explained approximately 13% of the reducing effect of depression.
In order to cope with aging, China has now begun to adjust its fertility policy. However, while relaxing fertility control, the potential impact of reproductive behaviour on women, as the direct bearers of fertility, deserves in-depth study. In this study, the test of relationship between the number of children born early in life and mothers’ mental health in later life illustrated its importance.
On the one hand, it is recommended to accelerate the improvement of supporting policies related to fertility and develop a healthy and scientific fertility culture. Strengthen policy supply in public services, improve maternal and child health services in rural areas, and improve women’s reproductive health. On the other hand, it is recommended that a sound family development support programme be gradually established. Women should be helped to balance their family and social roles and minimise role conflicts, and in particular, the pressure of caring for children should be shared appropriately. At the same time, targeted efforts have been made to increase old-age protection for older people.
There were many limitations to this study. First, there is insufficient control for confounding variables. In addition to the confounding factors such as individuals and families, low socio-economic status, health status before having children, fertility, and other social policies should be taken into account. Second, this study is not theoretically explanatory enough in terms of regional differences. Factors such as religious beliefs, social development, and traditional culture are all important reasons for the heterogeneity of its findings. Finally, there are few measures of reproductive behaviour and health in later life. This study only focuses on the number of children and child sex and does not take into account information such as age at childbearing and birth interval. At the same time, this study measures mental health only by depression, which may have also overlooked other important health information.
Acknowledgements
The authors wish to acknowledge the invaluable work of participants in the study. For the data used in this study, the authors thank Peking University of China for providing Chinese Longitudinal Healthy Longevity Survey.
Author contribution
ZS and YHL conceived this research. YHL was responsible for the methodology. ZS and WYY conducted software analyses. ZSQ and LZY conducted necessary validations. WYY conducted a formal analysis and managed the investigation. ZS, WYY, and LZY gathered resources, curated all data, wrote/prepared the original draft, and were responsible for project administration. ZS and YHL reviewed and edited the manuscript, were responsible for visualisation, supervised the project, and acquired funding. All authors contributed to the article and approved the submitted version.
Funding statement
This work was supported by the Later funded projects of National Social Science Foundation (Grant numbers: 21FRKB003).
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethics approval
The CLHLS study was approved by the research ethics committee of Peking University (permission: IRB00001052 – 13074), and all participants or their proxy respondents provided written informed consent after thoroughly explaining the research contents and results involved.
Appendix
Table A1. Variable Definition and Assignment













