To the Editor—Hand hygiene is a core measure recommended for prevention of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission. 1,2 Hand hygiene is needed to eliminate SARS-CoV-2 acquired on hands during contact with infected patients or contaminated surfaces and fomites, including personal protective equipment. 1–Reference Li, Alhmidi and Scott3 In an in vitro model, SARS-CoV-2 inoculated onto human skin survived for 9 hours after inoculation versus 2 hours for influenza A. Reference Hirose, Ikegaya and Naito4 SARS-CoV-2 was rapidly inactivated on skin by 80% ethanol. Reference Hirose, Ikegaya and Naito4
Hand hygiene may also be beneficial in reducing the burden of SARS-CoV-2 on the hands of individuals with coronavirus disease 2019 (COVID-19), and bathing may reduce SARS-CoV-2 on other skin sites. However, the burden of SARS-CoV-2 on hands and other skin sites of COVID-19 patients is unknown. Here, we tested the hypothesis that SARS-CoV-2 RNA is frequently present on the hands and the chest/abdomen of patients with COVID-19, particularly those with a high viral burden in samples collected from the anterior nares.
The study protocol was approved by the Cleveland VA Medical Center’s Institutional Review Board. Between November 1, 2020, and April 26, 2021, a convenience sample of patients with symptomatic COVID-19 was enrolled. Patients were excluded if they had dementia or delirium, were admitted to the intensive care unit, and if >3 days had passed since their COVID-19 diagnosis.
Premoistened CLASSIQSwabs with universal transport medium (Copan Diagnostics, Murrieta, CA) were used to collect samples from the anterior nares, oropharynx, chest/abdomen (10×10-cm surface area), and the entire surface area of both hands. Swabs were also used to sample environmental surfaces in patient rooms, including 5×20-cm areas of the bed rail and bedside table; outpatients sampled a frequently used chair and tabletop. A medical record review was conducted to obtain information on age, sex, medical conditions, and COVID-19 treatments.
A detailed description of the methods for RNA extraction and reverse transcriptase quantitative polymerase chain reaction (RT-qPCR) is included as Supplementary Material (online). The Fisher exact test was used to compare the proportions of COVID-19 patients with positive chest/abdomen or hand SARS-CoV-2 RNA for those with anterior nares cycle threshold (Ct) values of ≤30 or >30. The cycle threshold cutoff of 30 was chosen based on evidence that individuals with higher nasopharyngeal swab Ct values are less likely to have a positive cultures or to transmit SARS-CoV-2 to contacts. Reference Lee, Rozmanowski and Pang5 Analyses were performed using R version 3.5.1 statistical software (R Foundation for Statistical Computing, Vienna, Austria).
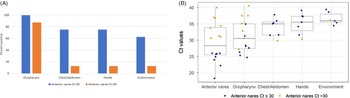
For the 16 study participants, the mean age was 60.8 years; 13 (81.3%) were male; 9 (56.3%) were receiving dexamethasone and supplemental oxygen at the time of enrollment; and 2 (12.5%) were outpatients. The anterior nares RT-qPCR result was positive for SARS-CoV-2 in all participants with an average Ct value of 29.2 (range, 18.2–40). Figure 1.A shows the percentage of other sites with positive RT-qPCR results for SARS-CoV-2 RNA, stratified by anterior nares Ct value ≤30 or >30. Of the 16 participants, the oropharynx, chest/abdomen, hand, and environmental samples were positive for SARS-CoV-2 RNA in 15 (93.8%), 7 (43.8%), 7 (43.8%), and 3 (18.8%) patients, respectively. All 7 patients with SARS-CoV-2 RNA on hands also had positive chest/abdomen samples. The percentage of chest/abdomen and hand samples that were positive was significantly higher in patients with anterior nares Ct values of ≤30 versus >30: 6 (75%) of 8 versus 1 (12.5%) of 8 (P = .04).

Fig. 1. Percentage of positive sites (A) and cycle threshold (Ct) values (B) by reverse transcriptase quantitative polymerase chain reaction (RT-qPCR), stratified based on anterior nares Ct values of ≤30 and >30.
Figure 1B shows a boxplot of the Ct values for SARS-CoV-2 RNA from all sites. Of the 7 patients with positive chest/abdomen RT-qPCR results for SARS-CoV-2, 1 patient (14.2%) had a chest/abdomen Ct value <30 and 3 patients (42.9%) had Ct values between 30 and 35. Of the 7 patients with positive hand RT-qPCR results for SARS-CoV-2, 3 patients (42.9%) had hand Ct values between 30 and 35. Only 1 (16.7%) of 6 positive environmental samples had RT-qPCR for SARS-CoV-2 with a Ct value <35.
Nearly half of COVID-19 patients had detectable levels of SARS-CoV-2 RNA on their hands and chest/abdomen. Contamination was significantly more common in patients with an increased nasal burden of SARS-CoV-2 based on an anterior nares Ct value of <30 (75% vs 12.5%). The burden of SARS-CoV-2 detected on the hands and chest/abdomen was relatively low, but approximately half had Ct values of <35 and 1 chest/abdomen sample had a Ct value of <30.
Our findings suggest that the hands and other skin sites of patients with COVID-19 could be an important source of transmission. Frequent hand hygiene should be emphasized for patients with suspected or confirmed COVID-19. Because presymptomatic patients contribute substantially to transmission of SARS-CoV-2, Reference Johansson, Quandelacy and Kada6,Reference Jones, Chan and Zabarsky7 hand hygiene is also essential in the absence of symptoms. Educational interventions can increase hand hygiene in hospitalized patients and long-term care facility residents. Reference Sunkesula, Kundrapu, Knighton, Cadnum and Donskey8 Because handshake and fist bump greetings efficiently transfer viruses, Reference Jones, Ha and Pinto-Herrera9 noncontact greetings should be encouraged. Finally, frequent bathing may be beneficial in reducing the burden of virus on skin. Chlorhexidine bathing is commonly used in healthcare facilities and has been shown to be effective against SARS-CoV-2. Reference Hirose, Bandou and Ikegaya10
Our study has several limitations. The swabs used for sampling the hands and chest/abdomen are designed for collection of nasopharyngeal specimens and were likely suboptimal for recovery of virus from skin. It is plausible that our results underestimate the burden of SARS-CoV-2 on skin. We did not perform viral cultures and cannot exclude the possibility that the SARS-CoV-2 RNA detected on skin represents nonviable virus. However, SARS-CoV-2 has been shown to survive for hours on skin. Reference Hirose, Ikegaya and Naito4
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/ice.2021.403
Acknowledgments
We thank the patients for their participation in the study.
Financial support
This work was supported by a Merit Review grant (no. CX001848) from the Department of Veterans’ Affairs to C.J.D.
Conflicts of interest
C.J.D has received research grants from Clorox, Pfizer, and PDI. All other authors report no conflicts of interest relevant to this article.