


LeFevre-Levy et al., Reference LeFevre-Levy, Melson-Silimon, Harmata, Hulett and Carter2023) help bring neurodiversity at work to a wider audience, and we agree with much of what the focal article explores, particularly around removing the stigma associated with diagnoses under the neurodiversity umbrella. However, the authors miss some of the nuance around the historical roots of neurodiversity and how that could pose threats to neurodiversity research moving forward. Notably, a tension exists between the social model of disability, from which neurodiversity draws, and the medical model, which could result in harm to those considered neurodiverse (Haegele & Hodge, Reference Haegele and Hodge2016). To resolve this tension, we propose an adaptation of the biopsychosocial (BPS) model (Engel, Reference Engel1977) as a middle ground for scholars and organizations. We present this model as a person-centered approach to improving research and practice around neurodiversity.
Approach #1: A medical model of disability
At a time when research into disabilities may be more important to society than at any point in the past, researchers generally favor either the medical or social model of disability to frame their approach and findings. Both models have their advantages and disadvantages. The medical model of disability centers on the aim to treat or eliminate a condition (Pellicano & Houting, Reference Pellicano and Houting2022). In this tradition, and depending on the situation, doctors would use the Diagnostic and Statistical Manual of Mental Disorders (DSM) to make a diagnosis. Based on this identification, doctors would prescribe a treatment plan to reduce the symptoms associated with that diagnosis. In essence, the medical model pathologizes a diagnosis as though it were an illness to be cured (Baker, Reference Baker2011). Along with, and perhaps due to, this deficit-oriented approach, many people diagnosed under the medical model may face questions concerning their ability to make decisions for themselves, feel stigmatized, or experience other negative outcomes (Grinker, Reference Grinker2020). Further, the medical model focuses on the individual and does not consider the social/environmental factors that could negatively influence neurodiverse people (Engel, Reference Engel1977).
Approach #2: As social model of disability
The apparent alternative to the negatives associated with the medical model of disability has been the social model of disability. An emphasis for much of the social model of disability is that society excludes and diminishes individuals with a disability. The model and its supporters contend that disabled individuals should be included and accepted. The underlying tenet is that disability is caused by the environment not being able to accommodate individuals appropriately (Pellicano & Houting, Reference Pellicano and Houting2022). In line with this, neurodiversity tends to place an emphasis on the idea of the underlying conditions as being a part of normal human development and evolutionarily advantageous for humans over the course of human existence (Armstrong, Reference Armstrong2015). Relatedly, a controversial component of the social model of disability is the idea of accommodating, rather than treating, neurodiverse individuals.
The tension between the social and medical models
The focal article highlights that treatment, rather than accommodation, of neurodiverse people should occur under conditions of suffering but fails to define what types of suffering this treatment could include or under what conditions treatment is appropriate. For example, applied behavioral analysis (ABA) has been used as a method to help individuals on the spectrum increase language and communication skills (Yu et al., Reference Yu, Li, Li and Liang2020). However, ABA has also been characterized as traumatic and abusive (Milton, Reference Milton2018). Similarly, adult usage of attention-deficit/hyperactivity disorder (ADHD) medications have been praised for allowing some people to be productive at work and maintain a job, whereas elsewhere it has been maligned as an amphetamine widely abused in society (Schwartz, Reference Schwartz2016).
A possible solution: The biopsychosocial model
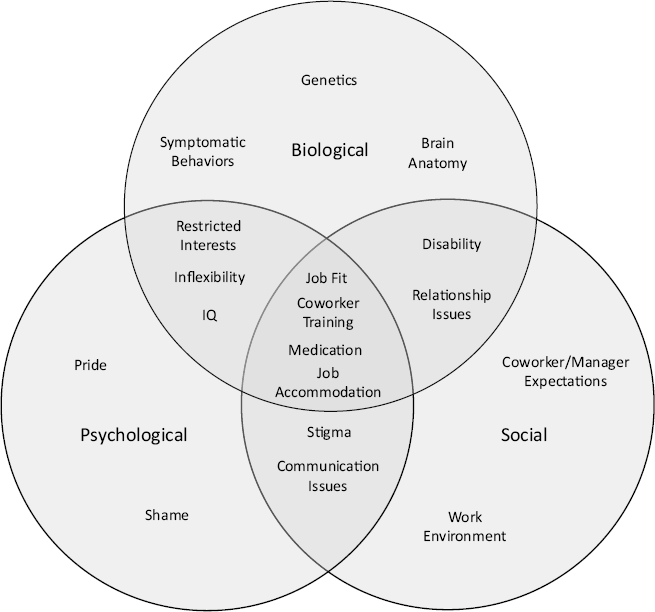
Given the tension that two people with similar conditions can react very differently to alternative approaches of intervention, we are left asking: How can companies embrace neurodiversity among employees and all of the benefits that come along with it? We propose one possible solution to this tension that advances a more person-centered approach. To do so, we draw on the BPS model that has been prevalent in the medical literature (Borrell-Carrio et al., Reference Borrell-Carrio, Suchman and Epstein2004; Engel, Reference Engel1977). The BPS model includes aspects of both the medical (biological domain) model and the social (social domain) model of disability while also simultaneously considering the individual’s beliefs and attitudes about their disability and how it influences their behaviors at work (psychological domain). The BPS model suggests that the three domains interact and overlap with each other; thus, considering all three domains leads to a stronger understanding of neurodiversity. Specifically, it allows for a more holistic and individualized approach to the study and application of neurodiversity at work because it incorporates a medical diagnosis but also accounts for variation in the individual and the contexts in which they live and work. This latter part is important because neurodiversity is an umbrella term that encompasses a wide variety of diagnoses, each with varying needs. The goal of using the BPS model is to ameliorate the aspects of disability that inhibit employment success while providing an environment that can emphasize the strengths of neurodiverse employees (Doyle, Reference Doyle2020). Below, we walk through each aspect of the BPS in the context of neurodiversity research and practice.
Psychological domain
The psychological domain consists of aspects like affect, motivation, stress, and cognitions/reflections about one’s unique condition (Lehman et al., Reference Lehman, David and Gruber2017). The psychological domain is frequently ignored in the social and medical models of neurodiversity; however, we view the psychological domain as essential for bringing the individual into how companies can approach neurodiversity. Nowhere may this be more obvious than the observation of autism as a spectrum. Where employees fall on the autism spectrum will influence a myriad of factors in the psychological domain, including one’s identities around neurodiversity and how being neurodiverse influences day-to-day activities. In turn, grouping autistic employees under a single neurodiverse umbrella may help some employees, whereas others could feel that their individual manifestations of the diagnosis are ignored. For example, some autistic employees prefer certain communication styles, such as written communication, whereas others might be more comfortable with oral communication (Howard & Sedgewick, Reference Howard and Sedgewick2021). This preference has implications for how an individual performs best at work. Further, autistic individuals may have very different reflections on their diagnoses in the greater social context (Johnson & Joshi, Reference Johnson and Joshi2016). These reflections could influence the individual’s choice to disclose their diagnosis or even seek accommodations and/or treatment (Whelpley et al., Reference Whelpley, Banks, Bochantin and Sandoval2021). This highlights the need for research to not only focus on the psychological domain but also to expand it into the social environment. In turn, any treatment or accommodation would need to be based around these psychological differences.
Social domain
The BPS model could lead practitioners to consider the unique social and normative environment that neurodiverse individuals find themselves in at work. In this sense, an individual’s identity concerning their neurodiversity is situated in the social environment. In turn, neurodiverse employees’ reflections about themselves will be influenced by others’ treatment and view of their condition. This so-called “looking-glass self” can strongly influence both negative and positive cognitions about oneself (marked by the overlap in the psychological and social domains illustrated in Figure 1). As noted, this can directly change behaviors, such as disclosure or asking for accommodation, but also creates the social dynamics that coworkers bring into their interactions with neurodiverse employees. For example, managers may decrease expectations for neurodiverse coworkers, against the wishes of those neurodiverse workers, believing that they are helping these workers succeed (Whelpley & Woznyj, Reference Whelpley and Woznyj2022). This type of interaction has the potential to reinforce the stigmatized stereotypes that are often applied to neurodiverse workers, which, again, influence the beliefs that people have about themselves.
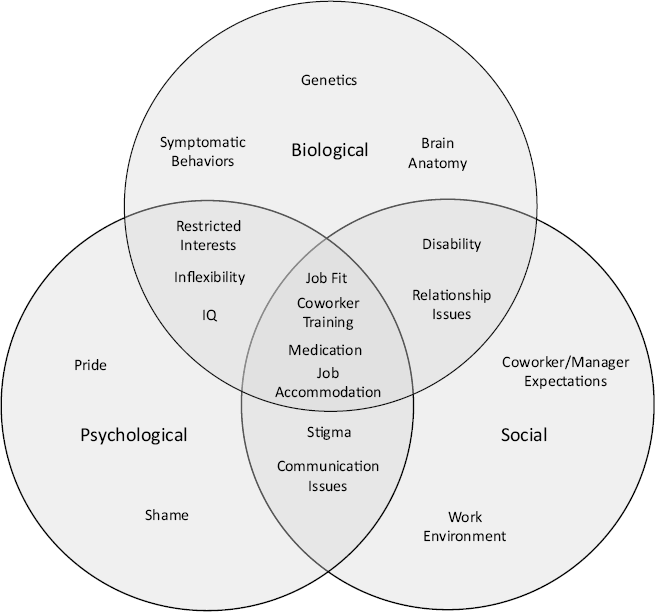
Figure 1. Autism and the BPS Model at work.
Biological domain
Not only are the psychological and social factors important for helping neurodiverse workers excel at work, but biological factors also play an important role. Consequently, the BPS model encourages practitioners to recognize the importance of appropriate treatment with respect to the biological aspects of neurodiversity. For example, even for individuals who share a medical diagnosis, appropriate treatment may vary based on genetic factors, presentation of symptoms, and the work environment. Sensory processing disorder (SPD) has some genetic roots, is attributable, in part, to differences in brain structure, and is a comorbidity with multiple neurodiverse identities (e.g., ADHD & ASD; Owen et al., Reference Owen, Marco, Desai, Fourie, Harris, Hill, Arnett and Mukherjee2013). But how SPD manifests at work can vary dramatically as research has found that noises, smells, lights, and so on affect people diagnosed with SPD differently. Consequently, employers should learn more about the context of the individual’s condition in addition to the kinds of treatment options available. Understanding what treatments have been successful for the individual in previous environments (i.e., in school or in prior employment), as well as how they have been implemented effectively (e.g., single-method treatment or combinations of medication, therapy, etc.) can provide a foundation for establishing options for job accommodation and treatment to promote the individual’s health, well-being, and success.
Illustrative example
To illustrate the benefits of the BPS model in neurodiversity research and practice, we draw on LeFevre-Levy et al.’s discussion of autistic employees (see Figure 1). The biological domain would be most similar to the medical model in that it underscores the diagnosis based on the criteria in the DSM IV manual (APA, 2013). For example, an autism diagnosis could include difficulty maintaining and understanding relationships or having extremely narrow interests. In the United States, the medical diagnosis entitles those on the spectrum to have reasonable job accommodations per the Americans with Disabilities Act (ADA). The psychological aspects of the BPS model at work include the reflections that an individual has—not only about their diagnosis (e.g., shame or pride in being autistic) but also aspects of personality, intelligence, and other individual differences. As noted, the psychological domain places more importance on the individual relative to the social or medical models of disability. As such, it is an important component for how the three BPS domains come together. Last, we acknowledge the role of the social environment. Research has found that many autistic individuals feel stigmatized by society, which influences self-cognitions (Johnson & Joshi, Reference Johnson and Joshi2016). However, some examples also paint the experience of autistic individuals at work as positive, with companies deliberately recruiting and hiring autistic individuals (Liu, Reference Liu2022).
How these three domains overlap is what makes the BPS unique and potentially fruitful in the work environment. As illustrated in Figure 1, we see that based on the overlap between the three domains, organizations can help to create an environment that is beneficial for both the employee on the spectrum and the organization. This can be achieved through job fit, coworker training, job accommodation, and, for those who want it, treatment. How might this unfold in organizations? In line with previous research, we see open communication between autistic employees and their organizations as central to the process. Specifically, the organization (or managers) should understand aspects of the condition (medical model, to some degree) but also recognize that each individual is unique (psychological domain) and that each person needs to be accepted and accommodated differently (social domain; Whelpley & Woznyj, Reference Whelpley and Woznyj2022).
The result is an instance in which the individual works with the organization to see what changes can be made to a role in order to facilitate a better fit that will make the employee more productive. Research indicates that both employees and managers support training interventions to improve understanding between autistic and neurotypical employees in organizations (Whelpley et al., Reference Whelpley, Banks, Bochantin and Sandoval2021). Such trainings could augment the social environment to create a more positive association with autism. Last, we view medical interventions (such as medication or applied behavioral analysis, also part of the medical model) as having more overlap between the biological and psychological domain, recognizing that the decision to seek treatment or medication is a personal choice embedded in a social environment. Some may feel medication is instrumental to their employment success, even with appropriate accommodation, whereas others may not. In sum, by using the BPS model we feel that organizations can build on the strengths of autistic—and other neurodiverse—employees as mentioned in the focal article.
Future directions and conclusion
LeFevre-Levy et al. issued a call for neurodiversity to take a greater role in industrial and organizational psychology research. However, the connection that neurodiversity has to the social model of disability could inhibit the inclusion of a variety of individuals at work because of the emphasis on accommodations rather than treatment. We contend that the BPS model is a more appropriate approach because it places the individual at the center of the situation and provides more flexibility in how employees approach being neurodiverse. This might include both treatment and accommodation as the individual sees appropriate. Our person-centered method is needed given the variety of diagnoses that the neurodiversity umbrella subsumes. For research and practice in the area to be truly effective, it is vital to consider each particular diagnosis and, more importantly, each individual person. For organizations, the BPS model allows for such consideration with the ultimate goal of ameliorating the negative influence that various diagnoses may have on an individual and promoting the success of employees. In turn, organizations could move further away from the label of disability by emphasizing the strengths and abilities of each employee. We hope that management research and organizations can use our approach to promote equity at work and to build environments that utilize all aspects of diversity for the improvement of organizations and the individuals working in them.

 Open access
Open access