


Introduction
The global inequity in access to and availability of essential mental health services is well recognized and has been identified as a ‘grand challenge’ (Collins et al., Reference Collins, Patel, Joestl, March, Insel and Daar2011). The mental health treatment gap is approximately 50% in all countries, with up to 90% of people in the lowest-income countries lacking access to the mental health services they require (Saxena et al., Reference Saxena, Thornicroft, Knapp and Whiteford2007; Patel et al., Reference Patel, Maj, Flisher, De Silva, Koschorke and Prince2010). Inequity is also found within countries; vulnerable groups, including people with low socioeconomic status (SES), women and sexual minorities, young people and people residing in rural areas are often most affected by mental health problems and are least likely to receive care (Saxena et al., Reference Saxena, Thornicroft, Knapp and Whiteford2007). The global mental health (GMH) treatment gap is indicative of a historic inequity in the prioritization and response to mental health compared with other health conditions (Votruba et al., Reference Votruba and Thornicroft2016). The lack of essential treatment for many people suffering from mental illness in low- and middle-income countries (LMICs) has been described as a moral failure (Kleinman, Reference Kleinman2009).
In the last decade, however, GMH has emerged as a response to the treatment gap in mental illness. Increased investment in GMH has led to the development and testing of innovative approaches to mental health service delivery in LMICs. In turn, as the evidence for effective interventions grows, so too does the need for a deeper understanding of how to implement and scale-up mental health services so that they effectively reach those in need (Eaton et al., Reference Eaton, McCay, Semrau, Chatterjee, Baingana, Araya, Ntulo, Thornicroft and Saxena2011). Implementation science is a fundamental area of inquiry in GMH, representing a foundational component of sustained and effective interventions to diminish the treatment gap in LMICs (De Silva & Ryan, Reference De Silva and Ryan2016).
Implementation research in GMH examines how to ensure that evidence-based practices are integrated into routine clinical care and throughout health systems, by ‘understand[ing] and address[ing] the behavioural, managerial, economic and social barriers’ to implementation and scale-up (De Silva & Ryan, Reference De Silva and Ryan2016). Because it occurs within complex health systems, effective planning for implementation requires a deep understanding of context. Formative research, which ‘aims to determine how best to fit aspects of program design and/or implementation to the environmental and cultural context of its beneficiaries,’ (Bentley et al., Reference Bentley, Johnson, Wasser, Creed-Kanashiro, Shroff, Fernandez Rao and Cunningham2014) is, therefore, a critical component of implementation research. Situational analysis, a type of formative research, is ‘an assessment of the current health situation and is fundamental to designing and updating national policies, strategies and plans’ (World Health Organization, 2018). Situational analysis is used to understand, from the outset of a study, the multiple interacting factors within a system that might affect implementation (Martin et al., Reference Martin, Pauly and MacDonald2016). These might include, for example, human and financial resources, health policies and plans, social determinants of health, and other interacting factors. Situational analyses in GMH, where mental health services and systems are poorly developed and resourced, are essential when planning for research and implementation. However, little guidance is available to inform methodological approaches to conducting these types of studies.
Equity in health, defined as ‘the absence of systematic disparities in health (or in the major social determinants of health) between groups with different levels of underlying social advantage/disadvantage,’ (Braveman & Gruskin, Reference Braveman and Gruskin2003) is at the core of GMH (Patel & Prince, Reference Patel and Prince2010). The efforts of GMH to address inequity in mental health service delivery and access indicates a need for approaches to GMH implementation research that include equity as a key consideration (Rasanathan & Diaz, Reference Rasanathan and Diaz2016). Explicitly integrating equity considerations into the design of situational analyses, therefore, could help to ensure that implementation planning includes strategies to promote equitable access to interventions by the most vulnerable and underserved populations.
We aimed to provide a scoping review of methodological approaches to situational analysis in GMH. We also assessed the extent to which GMH situational analyses include equity in their study designs. This review would serve as an important resource for GMH researchers in implementation research and help identify gaps and areas for future development in GMH.
Methods
Scoping reviews are effective for summarizing and disseminating research findings and for identifying gaps in the literature (Arksey & O'Malley, Reference Arksey and O'Malley2005). They are particularly appropriate in fields with emergent findings and to ‘address questions beyond those related to intervention effectiveness’ (Levac et al., Reference Levac, Colquhoun and O'Brien2010). We used Arksey & O'Malley's (Reference Arksey and O'Malley2005) methodological framework for scoping reviews to conduct the review and met the criteria of the PRISMA-Scoping Review (PRISMA-ScR) guidelines (Tricco et al., Reference Tricco, Lillie, Zarin, O'Brien, Colquhoun, Levac, Moher, Peters, Horsley, Weeks, Hempel, Akl, Chang, McGowan, Stewart, Hartling, Aldcroft, Wilson, Garritty, Lewin, Godfrey, Macdonald, Langlois, Soares-Weiser, Moriarty, Clifford, Tunçalp and Straus2018). The objective of this review is to identify: (a) which methodological approaches for conducting situational analyses are commonly used in GMH; (b) the existing gaps and areas for further development in this area and, (c) to what extent, and how, equity considerations are captured in situational analyses in GMH.
We identified relevant studies through a search of PUBMED and PsychINFO databases using the search terms: Situational Analysis AND Mental Health AND Global, Situation Analysis AND Mental Health AND Global, and Formative Research AND Mental Health AND Global. The lead author (JM) initially conducted the database search in April and May of 2018. We also complemented our database search with a review of the reference lists of included articles to ensure we did not overlook relevant studies (Arksey & O'Malley, Reference Arksey and O'Malley2005). Based upon the broad definitions of situational analysis provided by the World Health Organization (WHO) (2018) and Martin et al. (Reference Martin, Pauly and MacDonald2016), we sought to include papers that involved an assessment of contextual factors in the mental health system of LMIC or regions in advance of implementing mental health interventions, programs, plans and/ or policies.
Inclusion criteria were studies that: (1) took place in an LMIC context as defined by World Bank criteria (The World Bank, 2018), (2) described situational analysis methodology, defined as approaches that assessed the environmental and cultural context of health services delivery to inform the design and/or implementation of mental health interventions, programs or plans (Bentley et al., Reference Bentley, Johnson, Wasser, Creed-Kanashiro, Shroff, Fernandez Rao and Cunningham2014; World Health Organization, 2018), and (3) focused on health systems and/ or service delivery research. We excluded studies that: (1) predominantly reported findings related to mental health epidemiology or intervention effectiveness or that did not otherwise constitute situational analyses or formative research (e.g. that took place after implementation, process evaluation, etc.), (2) were situated in high-income countries (HICs), and (3) were published in languages other than English. Figure 1 displays a PRISMA diagram of the search process. We began with an initial screening of the title and abstracts of records, followed by full-text screening. JM conducted the initial screening, which was then repeated and verified by co-author CW. Discrepancies were resolved by consensus with a third co-author (RWL).
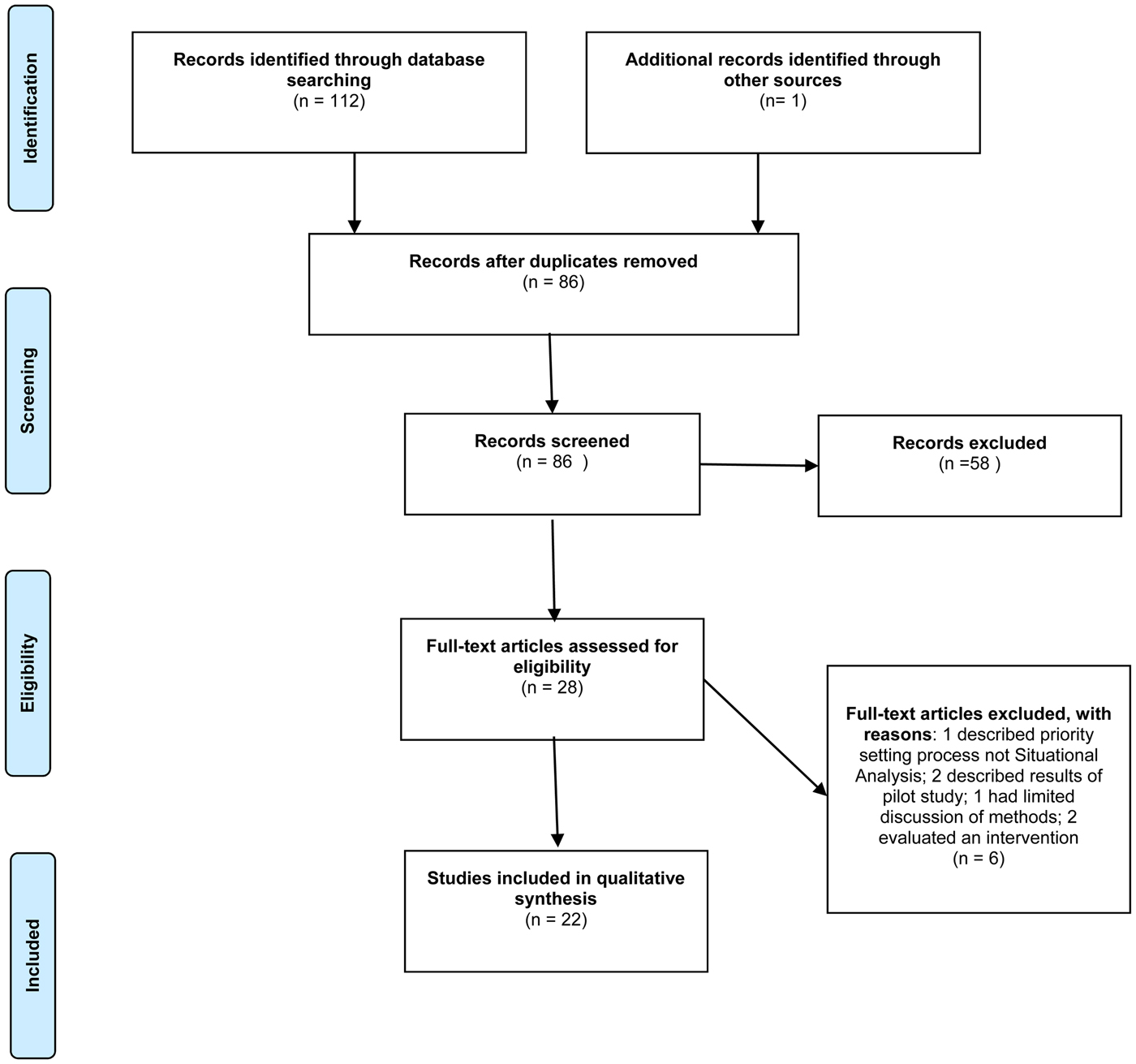
Fig. 1. PRISMA diagram of scoping review literature search and selection.
We extracted and charted the results of the review using the following categories: study scope (e.g. national, regional or district level, single or multi-country), purpose, country of origin, objectives, methods, situational analysis tool characteristics and use, inclusion of equity in study design, and limitations as described by the study authors. The inclusion and exclusion criteria and the data extraction categories were decided through discussion amongst authors JM, EEM and RWL, with further consultation with the full study team. We analysed the results using a combination of numerical descriptive summary and qualitative thematic analysis (Levac et al., Reference Levac, Colquhoun and O'Brien2010). This allowed us to collate the results, which are summarized below according to the study review categories.
Results
We identified 112 records through our database search and three additional records through a review of reference lists. A total of 27 duplicates were removed and another 58 were excluded after the title and abstract review. We excluded a further six records after reading the full text. A total of 24 papers were included in the review (see Fig. 1), representing 12 research programs s. Table 1 lists the studies that met inclusion criteria, the country or countries in which they took place, their objective(s), methods and limitations as identified by the study authors.
Table 1. Context and scope of included studies
a By World Bank region excluding North America which contains all High-Income Countries (Canada, USA, Bermuda).
b Numbers exceed total due to multi-country studies.
Scope and context of studies
Table 2 displays the regional distribution and scope of the studies: 70.9% (n = 17) of the 24 studies took place in Sub-Saharan Africa, 37.5% (n = 9) took place is South Asia and 8.3% (n = 2) two took place in East Asia. None were performed in Latin America, the Caribbean or Middle East and North Africa regions.
Table 2. Context and scope of included studies
a By World Bank region excluding North America which contains all High-Income Countries (Canada, USA, Bermuda).
b Numbers exceed total due to multi-country studies.
For this analysis, studies are counted as ‘single country’ if they reported results from only one country in a paper, regardless of their broader affiliation with multi-country research programs. Of the studies, 14 (58.3%) took place in multiple countries, with high representation in this review of papers published by consortia such as the Programme to Improve Mental Health Care (PRIME) (Jordans et al., Reference Jordans, Luitel, Tomlinson and Komproe2013; Hanlon et al., Reference Hanlon, Luitel, Kathree, Murhar, Shrivasta, Medhin, Ssebunnya, Fekadu, Shidhaye, Petersen, Jordans, Kigozi, Thornicroft, Patel, Tomlinson, Lund, Breuer, De Silva and Prince2014; Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015; Luitel et al., Reference Luitel, Jordans, Adhikari, Upadhaya, Hanlon, Lund and Komproe2015; Shidhaye et al., Reference Shidhaye, Raja, Shrivastava, Murhar, Ramaswamy and Patel2015; Baron et al., Reference Baron, Hanlon, Mall, Honikman, Breuer, Kathree, Luitel, Nakku, Lund, Medhin, Patel, Petersen, Shrivastava and Tomlinson2016; Hailemariam et al., Reference Hailemariam, Fekadu, Selamu, Medhin, Prince and Hanlon2016; Kigozi et al., Reference Kigozi, Kizza, Nakku, Ssebunnya, Ndyanabangi, Nakiganda, Lund and Patel2016; Angdembe et al., Reference Angdembe, Kohrt, Jordans, Rimal and Luitel2017) and the Emerging Mental Health Systems in LMICs (EMERALD) study (Abdulmalik et al., Reference Abdulmalik, Kola and Gureje2016; Upadhaya et al., Reference Upadhaya, Jordans, Abdulmalik, Ahuja, Alem, Hanlon, Kigozi, Kizza, Lund, Semrau, Shidhaye, Thornicroft, Komproe and Gureje2016; Mugisha et al., Reference Mugisha, Abdulmalik, Hanlon, Petersen, Lund, Upadhaya, Ahuja, Shidhaye, Mntambo, Alem, Gureje and Kigozi2017). Ten (41.6%) focused on a single country. Twelve (50.0%) of the studies focused on the district, provincial or state level, while 10 (41.6%) focused at the national level, and two (8.3%) took place at a municipal level.
Objectives of included studies
The broad objectives of the included studies are categorized by theme in Table 3. Twelve (50%) of the studies conducted situational analyses in advance of developing mental health policies or plans at national or regional levels. Of the 10 countries with the primary goal of informing mental health policy and planning, six were part of the PRIME study (Jordans et al., Reference Jordans, Luitel, Tomlinson and Komproe2013; Hanlon et al., Reference Hanlon, Luitel, Kathree, Murhar, Shrivasta, Medhin, Ssebunnya, Fekadu, Shidhaye, Petersen, Jordans, Kigozi, Thornicroft, Patel, Tomlinson, Lund, Breuer, De Silva and Prince2014; Luitel et al., Reference Luitel, Jordans, Adhikari, Upadhaya, Hanlon, Lund and Komproe2015; Shidhaye et al., Reference Shidhaye, Raja, Shrivastava, Murhar, Ramaswamy and Patel2015; Kigozi et al., Reference Kigozi, Kizza, Nakku, Ssebunnya, Ndyanabangi, Nakiganda, Lund and Patel2016; Petersen et al., Reference Petersen, Fairall, Bhana, Kathree, Selohilwe, Brooke-Sumner, Faris, Breuer, Sibanyoni, Lund and Patel2016), which aims to develop, test and scale-up mental health plans in selected districts of each of the study's participating countries (Ethiopia, India, Nepal, South Africa, and Uganda) (Lund et al., Reference Lund, Tomlinson, De Silva, Fekadu, Shidhaye, Jordans, Petersen, Bhana, Kigozi, Prince, Thornicroft, Hanlon, Kakuma, McDaid, Saxena, Chisholm, Raja, Kippen-Wood, Honikman, Fairall and Patel2012). Studies targeting policy and planning used situational analyses to understand the current state of mental health governance (Abdulmalik et al., Reference Abdulmalik, Kola and Gureje2016), to assess mental health resources (financial, human resource, infrastructure), to identify current practice and gaps in mental health service delivery, and to understand the broader health and socioeconomic context of the countries or regions of interest (Ofori-Atta et al., Reference Ofori-Atta, Read and Lund2010; Sikwese et al., Reference Sikwese, Mwape, Mwanza, Kapungwe, Kakuma, Imasiku, Lund and Cooper2010; Jordans et al., Reference Jordans, Luitel, Tomlinson and Komproe2013; Esan et al., Reference Esan, Abdumalik, Eaton, Kola, Fadahunsi and Gureje2014; Hanlon et al., Reference Hanlon, Luitel, Kathree, Murhar, Shrivasta, Medhin, Ssebunnya, Fekadu, Shidhaye, Petersen, Jordans, Kigozi, Thornicroft, Patel, Tomlinson, Lund, Breuer, De Silva and Prince2014; Luitel et al., Reference Luitel, Jordans, Adhikari, Upadhaya, Hanlon, Lund and Komproe2015; Baron et al., Reference Baron, Hanlon, Mall, Honikman, Breuer, Kathree, Luitel, Nakku, Lund, Medhin, Patel, Petersen, Shrivastava and Tomlinson2016; Kigozi et al., Reference Kigozi, Kizza, Nakku, Ssebunnya, Ndyanabangi, Nakiganda, Lund and Patel2016; Petersen et al., Reference Petersen, Fairall, Bhana, Kathree, Selohilwe, Brooke-Sumner, Faris, Breuer, Sibanyoni, Lund and Patel2016; Upadhaya et al., Reference Upadhaya, Jordans, Abdulmalik, Ahuja, Alem, Hanlon, Kigozi, Kizza, Lund, Semrau, Shidhaye, Thornicroft, Komproe and Gureje2016; Olofsson et al., Reference Olofsson, Sebastian and Jegannathan2018).
Table 3. Study objectives
Seven (29.2%) conducted situational analyses and formative research to inform the development or design of mental health programmes or services. Objectives included the development of a package of community-based mental health and mobile health services (Angdembe et al., Reference Angdembe, Kohrt, Jordans, Rimal and Luitel2017), supporting the integration of mental health services into primary health care (Bhana et al., Reference Petersen, Ssebunnya, Bhana and Baillie2010; Baron et al., Reference Baron, Hanlon, Mall, Honikman, Breuer, Kathree, Luitel, Nakku, Lund, Medhin, Patel, Petersen, Shrivastava and Tomlinson2016; De Kock & Pillay, Reference De Kock and Pillay2016; Mugisha et al., Reference Mugisha, Abdulmalik, Hanlon, Petersen, Lund, Upadhaya, Ahuja, Shidhaye, Mntambo, Alem, Gureje and Kigozi2017) and improving the availability and accessibility of treatment for specific mental health conditions (Hailemariam et al., Reference Hailemariam, Fekadu, Selamu, Medhin, Prince and Hanlon2016; Tekola et al., Reference Tekola, Baheretibeb, Roth, Tilahun, Fekadu, Hanlon and Hoekstra2016).
Finally, five (20.8%) papers used situational analyses and formative research before developing specific clinical mental health interventions. These sought to: inform the design of acceptable and feasible interventions for the study context (Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015; Davies et al., Reference Davies, Schneider, Nyatsanza and Lund2016; Maulik et al., Reference Maulik, Tewari, Devarapalli, Kallakuri and Patel2016; Yu et al., Reference Yu, Kowitt, Fisher and Li2017), assess contextual and implementation factors prior to pilot testing of interventions (Dos Santos & Wolvaardt, Reference Dos Santos and Wolvaardt2016), understand the sociocultural context of intervention delivery, including explanatory models of mental illness and stigma (Davies et al., Reference Davies, Schneider, Nyatsanza and Lund2016; Maulik et al., Reference Maulik, Tewari, Devarapalli, Kallakuri and Patel2016; Yu et al., Reference Yu, Kowitt, Fisher and Li2017) and to identify factors that might affect the scale-up and sustainability of interventions (Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015; Dos Santos & Wolvaardt, Reference Dos Santos and Wolvaardt2016).
Study methodologies
Methodological approaches used for situational analyses can be categorized into three themes: situational analyses using secondary data review, qualitative research and priority setting exercises. Table 4 displays the methodological approaches and the number of methods used by each study. Fourteen (58.3%) of the individual studies used one method, six (25.0%) used two and two (8.3%) combined three methodological approaches. Because many of the papers represent the PRIME and EMERALD research consortia, we also note studies that are associated with them and collated approaches used by each programme.
Table 4. Methodological approaches by study
Seventeen (70.8%) of studies included qualitative research, using key informant and in-depth interviews and/or focus group discussions (Bhana et al., Reference Petersen, Ssebunnya, Bhana and Baillie2010; Ofori-Atta et al., Reference Ofori-Atta, Read and Lund2010; Sikwese et al., Reference Sikwese, Mwape, Mwanza, Kapungwe, Kakuma, Imasiku, Lund and Cooper2010; Jordans et al., Reference Jordans, Luitel, Tomlinson and Komproe2013; Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015; Shidhaye et al., Reference Shidhaye, Raja, Shrivastava, Murhar, Ramaswamy and Patel2015; Davies et al., Reference Davies, Schneider, Nyatsanza and Lund2016; De Kock & Pillay, Reference De Kock and Pillay2016; Dos Santos & Wolvaardt, Reference Dos Santos and Wolvaardt2016; Hailemariam et al., Reference Hailemariam, Fekadu, Selamu, Medhin, Prince and Hanlon2016; Kigozi et al., Reference Kigozi, Kizza, Nakku, Ssebunnya, Ndyanabangi, Nakiganda, Lund and Patel2016; Maulik et al., Reference Maulik, Tewari, Devarapalli, Kallakuri and Patel2016; Petersen et al., Reference Petersen, Fairall, Bhana, Kathree, Selohilwe, Brooke-Sumner, Faris, Breuer, Sibanyoni, Lund and Patel2016; Tekola et al., Reference Tekola, Baheretibeb, Roth, Tilahun, Fekadu, Hanlon and Hoekstra2016; Angdembe et al., Reference Angdembe, Kohrt, Jordans, Rimal and Luitel2017; Yu et al., Reference Yu, Kowitt, Fisher and Li2017; Olofsson et al., Reference Olofsson, Sebastian and Jegannathan2018). Qualitative studies involved a range of participants, including: policymakers, mental health specialists, primary care providers, other healthcare providers (e.g. maternal health, HIV), community health workers, traditional healers, lay providers, service users, families and caregivers, police officers, teachers, community members and mental health experts. Many of the qualitative studies sought to understand existing mental health service availability in the study context, with qualitative methods providing a deeper understanding of current mental health practice, needs and gaps in service, and barriers to implementing policy, plans or interventions (Bhana et al., Reference Petersen, Ssebunnya, Bhana and Baillie2010; Ofori-Atta et al., Reference Ofori-Atta, Read and Lund2010; Sikwese et al., Reference Sikwese, Mwape, Mwanza, Kapungwe, Kakuma, Imasiku, Lund and Cooper2010; Shidhaye et al., Reference Shidhaye, Raja, Shrivastava, Murhar, Ramaswamy and Patel2015; De Kock & Pillay, Reference De Kock and Pillay2016; Dos Santos & Wolvaardt, Reference Dos Santos and Wolvaardt2016; Hailemariam et al., Reference Hailemariam, Fekadu, Selamu, Medhin, Prince and Hanlon2016; Kigozi et al., Reference Kigozi, Kizza, Nakku, Ssebunnya, Ndyanabangi, Nakiganda, Lund and Patel2016; Maulik et al., Reference Maulik, Tewari, Devarapalli, Kallakuri and Patel2016; Tekola et al., Reference Tekola, Baheretibeb, Roth, Tilahun, Fekadu, Hanlon and Hoekstra2016; Olofsson et al., Reference Olofsson, Sebastian and Jegannathan2018). Studies also used qualitative methods to understand acceptability, including the acceptability of integrating mental health care into existing services (e.g. primary care, HIV service delivery, community-based care) (Jordans et al., Reference Jordans, Luitel, Tomlinson and Komproe2013; Dos Santos & Wolvaardt, Reference Dos Santos and Wolvaardt2016; Petersen et al., Reference Petersen, Fairall, Bhana, Kathree, Selohilwe, Brooke-Sumner, Faris, Breuer, Sibanyoni, Lund and Patel2016; Angdembe et al., Reference Angdembe, Kohrt, Jordans, Rimal and Luitel2017), the acceptability of treatment options and interventions (Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015; Yu et al., Reference Yu, Kowitt, Fisher and Li2017) and gaps in human resources for mental health (Sikwese et al., Reference Sikwese, Mwape, Mwanza, Kapungwe, Kakuma, Imasiku, Lund and Cooper2010).
Sixteen (66.6%) of the studies reviewed secondary data; 14 used a specifically designed situational analysis tool and two studies did not use a tool. Tools used for situational analysis varied, with the majority (7) using the PRIME situational analysis tool, which was specifically designed for the PRIME study (Hanlon et al., Reference Hanlon, Luitel, Kathree, Murhar, Shrivasta, Medhin, Ssebunnya, Fekadu, Shidhaye, Petersen, Jordans, Kigozi, Thornicroft, Patel, Tomlinson, Lund, Breuer, De Silva and Prince2014; Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015; Luitel et al., Reference Luitel, Jordans, Adhikari, Upadhaya, Hanlon, Lund and Komproe2015; Shidhaye et al., Reference Shidhaye, Raja, Shrivastava, Murhar, Ramaswamy and Patel2015; Baron et al., Reference Baron, Hanlon, Mall, Honikman, Breuer, Kathree, Luitel, Nakku, Lund, Medhin, Patel, Petersen, Shrivastava and Tomlinson2016; Petersen et al., Reference Petersen, Fairall, Bhana, Kathree, Selohilwe, Brooke-Sumner, Faris, Breuer, Sibanyoni, Lund and Patel2016; Olofsson et al., Reference Olofsson, Sebastian and Jegannathan2018). Of these, one was not part of the PRIME consortium (Olofsson et al., Reference Olofsson, Sebastian and Jegannathan2018). In this case, the investigators adapted the PRIME tool for length and for relevance to children's mental health in the Cambodian context. Two additional teams developed their own situational analysis frameworks (Esan et al., Reference Esan, Abdumalik, Eaton, Kola, Fadahunsi and Gureje2014; Upadhaya et al., Reference Upadhaya, Jordans, Abdulmalik, Ahuja, Alem, Hanlon, Kigozi, Kizza, Lund, Semrau, Shidhaye, Thornicroft, Komproe and Gureje2016), while others used or adapted the WHO-Assessment Instrument for Mental Health (AIMS) tool, and WHO checklists for mental health policy, plans and legislation (Bhana et al., Reference Petersen, Ssebunnya, Bhana and Baillie2010; Ofori-Atta et al., Reference Ofori-Atta, Read and Lund2010; Sikwese et al., Reference Sikwese, Mwape, Mwanza, Kapungwe, Kakuma, Imasiku, Lund and Cooper2010; Abdulmalik et al., Reference Abdulmalik, Kola and Gureje2016). Details of the PRIME Situational Analysis Tool, the WHO-AIMS and the tools developed by Esan et al. (Reference Esan, Abdumalik, Eaton, Kola, Fadahunsi and Gureje2014) and Upadhaya et al. (Reference Upadhaya, Jordans, Abdulmalik, Ahuja, Alem, Hanlon, Kigozi, Kizza, Lund, Semrau, Shidhaye, Thornicroft, Komproe and Gureje2016) are provided in Table 5. Two studies (De Kock & Pillay, Reference De Kock and Pillay2016; Tekola et al. Reference Tekola, Baheretibeb, Roth, Tilahun, Fekadu, Hanlon and Hoekstra2016) did not use tools. All studies using secondary data review methodology reviewed documents that were available in the public domain, including health surveillance and census data, mental health legislation, policy and plans, academic publications, government reports from mental health, general health and related sectors, media reports and medical records. In the majority of studies, data were collected by members of study research teams and often supplemented with personal communication with local mental health experts and stakeholders. Sikwese et al. (Reference Sikwese, Mwape, Mwanza, Kapungwe, Kakuma, Imasiku, Lund and Cooper2010) and Ofori-Atta et al. (Reference Ofori-Atta, Read and Lund2010) involved key stakeholders in the completion of the WHOAIMS.
Table 5. Characteristics of situational analysis tools and measures
Four (16.7%) of the studies used priority setting exercises as part of their situational analyses and formative research. Three of these studies (Jordans et al., Reference Jordans, Luitel, Tomlinson and Komproe2013; Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015; Petersen et al., Reference Petersen, Fairall, Bhana, Kathree, Selohilwe, Brooke-Sumner, Faris, Breuer, Sibanyoni, Lund and Patel2016) used Theory of Change workshops, in which stakeholders are convened to ‘map a causal chain of pre-conditions (or preliminary outcomes), assumptions and interventions leading to an ultimate outcome’ (Jordans et al., Reference Jordans, Luitel, Tomlinson and Komproe2013 3). Theory of Change methodology is used by the PRIME program to map pathways to developing mental health plans and to encourage stakeholder engagement (Breuer et al., Reference Breuer, De Silva, Fekadu, Luitel, Murhar, Nakku, Petersen and Lund2014). Tekola et al. (Reference Tekola, Baheretibeb, Roth, Tilahun, Fekadu, Hanlon and Hoekstra2016) also used workshops for priority setting but did not use the Theory of Change methodology.
The priority-setting workshops were used to inform the development of an intervention (Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015) and mental health plans (Jordans et al., Reference Jordans, Luitel, Tomlinson and Komproe2013; Baron et al., Reference Baron, Hanlon, Mall, Honikman, Breuer, Kathree, Luitel, Nakku, Lund, Medhin, Patel, Petersen, Shrivastava and Tomlinson2016) and to capture stakeholder perspectives on the mental health situation, and challenges and opportunities for service improvement (Tekola et al., Reference Tekola, Baheretibeb, Roth, Tilahun, Fekadu, Hanlon and Hoekstra2016). Participants included community leaders, service providers and managers, policy makers, end users, families, mental health experts and representatives of local and international non-governmental organizations.
Equity considerations in study design
Three studies explicitly included equity considerations in their study designs (Abdulmalik et al., Reference Abdulmalik, Kola and Gureje2016; Hailemariam et al., Reference Hailemariam, Fekadu, Selamu, Medhin, Prince and Hanlon2016; Mugisha et al., Reference Mugisha, Abdulmalik, Hanlon, Petersen, Lund, Upadhaya, Ahuja, Shidhaye, Mntambo, Alem, Gureje and Kigozi2017). Abdulmalik et al. (Reference Abdulmalik, Kola and Gureje2016) used a framework (Siddiqi et al., Reference Siddiqi, Masud, Nishtar, Peters, Sabri, Bile and Jama2009) to guide the design of the qualitative component of their study that included an ‘ethics and inclusiveness’ component. They identified multiple factors related to equity in their study design and analysis, including stigma and discrimination, low prioritization of mental health, low mental health awareness by policymakers, financial coverage available to people accessing mental health care (e.g. public insurance coverage), and rights protection for people with mental health disorders.
The overall goal of Hailemariam et al.,'s (Reference Hailemariam, Fekadu, Selamu, Medhin, Prince and Hanlon2016) study was to ‘inform the development of equitable and accessible mental healthcare integration into primary mental health services for people with severe mental disorders in Ethiopia. That qualitative study identified barriers to equitable access to services, defining equitable access in terms of the possible effect of gender, physical disability, socioeconomic status and location of the residence on access to mental health care.
Mugisha et al.,'s (Reference Mugisha, Abdulmalik, Hanlon, Petersen, Lund, Upadhaya, Ahuja, Shidhaye, Mntambo, Alem, Gureje and Kigozi2017) situational analysis of the health system context for primary care integration across the EMERALD study countries (Ethiopia, India, Nepal, Nigeria, South Africa and Uganda) included the analysis of ‘issues of equity in relation to existing policies’ in the study design. This included examining if and how considerations of gender, poverty, disability and other vulnerable populations are considered in mental health policy and provision.
Five other studies implicitly addressed issues related to equity but did not incorporate it in their study design; that was addressed by discussing the impact of poverty on help-seeking (Angdembe et al., Reference Angdembe, Kohrt, Jordans, Rimal and Luitel2017), the relationship between poverty and mental health and gaps in social protection for people with mental illness (Ofori-Atta et al., Reference Ofori-Atta, Read and Lund2010), the implications of community mobilization for social inclusion, reduced stigma and improving economic status (Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015), the impact of poverty and living circumstances on women's mental health (Davies et al., Reference Davies, Schneider, Nyatsanza and Lund2016) and the role of mental health information systems in capturing equity in service distribution for women, people with low socioeconomic status, and rural inhabitants (Shidhaye et al., Reference Shidhaye, Raja, Shrivastava, Murhar, Ramaswamy and Patel2015).
Identified limitations
Seven studies did not describe limitations related to situational analysis methodology (Ofori-Atta et al., Reference Ofori-Atta, Read and Lund2010; Sikwese et al., Reference Sikwese, Mwape, Mwanza, Kapungwe, Kakuma, Imasiku, Lund and Cooper2010; Esan et al., Reference Esan, Abdumalik, Eaton, Kola, Fadahunsi and Gureje2014; Abdulmalik et al., Reference Abdulmalik, Kola and Gureje2016; Dos Santos & Wolvaardt, Reference Dos Santos and Wolvaardt2016; Kigozi et al., Reference Kigozi, Kizza, Nakku, Ssebunnya, Ndyanabangi, Nakiganda, Lund and Patel2016; Petersen et al., Reference Petersen, Fairall, Bhana, Kathree, Selohilwe, Brooke-Sumner, Faris, Breuer, Sibanyoni, Lund and Patel2016).
The most common limitation identified by those that did describe limitations of situational analyses related to use of secondary data (Hanlon et al., Reference Hanlon, Luitel, Kathree, Murhar, Shrivasta, Medhin, Ssebunnya, Fekadu, Shidhaye, Petersen, Jordans, Kigozi, Thornicroft, Patel, Tomlinson, Lund, Breuer, De Silva and Prince2014; Luitel et al., Reference Luitel, Jordans, Adhikari, Upadhaya, Hanlon, Lund and Komproe2015; Shidhaye et al., Reference Shidhaye, Raja, Shrivastava, Murhar, Ramaswamy and Patel2015; Baron et al., Reference Baron, Hanlon, Mall, Honikman, Breuer, Kathree, Luitel, Nakku, Lund, Medhin, Patel, Petersen, Shrivastava and Tomlinson2016; De Kock & Pillay, Reference De Kock and Pillay2016; Upadhaya et al., Reference Upadhaya, Jordans, Abdulmalik, Ahuja, Alem, Hanlon, Kigozi, Kizza, Lund, Semrau, Shidhaye, Thornicroft, Komproe and Gureje2016; Mugisha et al., Reference Mugisha, Abdulmalik, Hanlon, Petersen, Lund, Upadhaya, Ahuja, Shidhaye, Mntambo, Alem, Gureje and Kigozi2017). Many countries have mental health information systems that are developing, resulting in limited availability of documents related to the specific mental health contexts, or documents that were not up to date. Studies that described this limitation noted that they attempted to mitigate this issue, however, by supplementation with personal communications with local mental health stakeholders.
Several studies without a qualitative component identified an inability to include findings on knowledge, attitudes and beliefs of stakeholders as a study limitation. Some authors indicated that complementary qualitative studies were being or would be untaken to capture this information (Hanlon et al., Reference Hanlon, Luitel, Kathree, Murhar, Shrivasta, Medhin, Ssebunnya, Fekadu, Shidhaye, Petersen, Jordans, Kigozi, Thornicroft, Patel, Tomlinson, Lund, Breuer, De Silva and Prince2014; Luitel et al., Reference Luitel, Jordans, Adhikari, Upadhaya, Hanlon, Lund and Komproe2015; Upadhaya et al., Reference Upadhaya, Jordans, Abdulmalik, Ahuja, Alem, Hanlon, Kigozi, Kizza, Lund, Semrau, Shidhaye, Thornicroft, Komproe and Gureje2016) and one cited lack of resources to include a qualitative component in the study (Mugisha et al., Reference Mugisha, Abdulmalik, Hanlon, Petersen, Lund, Upadhaya, Ahuja, Shidhaye, Mntambo, Alem, Gureje and Kigozi2017).
The most commonly cited limitation of qualitative studies was the limited scope of the study area and of study participants, which could limit generalizability of findings (Jordans et al., Reference Jordans, Luitel, Tomlinson and Komproe2013; De Kock & Pillay, Reference De Kock and Pillay2016; Angdembe et al., Reference Angdembe, Kohrt, Jordans, Rimal and Luitel2017; Yu et al., Reference Yu, Kowitt, Fisher and Li2017). Other limitations included language barriers between researchers and study participants, requiring the translation of interview transcripts and the risk of loss of meaning or misunderstanding of findings (Angdembe et al., Reference Angdembe, Kohrt, Jordans, Rimal and Luitel2017; Olofsson et al., Reference Olofsson, Sebastian and Jegannathan2018).
For studies using priority-setting exercises, limitations included the risk of social desirability bias due to the study's affiliation with the national government (Asher et al., Reference Asher, De Silva, Hanlon, Weiss, Birhane, Ejigu, Medhin, Patel and Fekadu2015). The type of participants included, the use of purposive sampling and the priorities of participants were also acknowledged as potential limitations. Jordans et al. (Reference Jordans, Luitel, Tomlinson and Komproe2013) described a predominance of mental health experts from urban settings as a potential limitation. They also acknowledged that the priority setting outcomes themselves may have been biased by the experience and knowledge of participants; they were surprised to find that developmental disorders were given low priority and noted that this may have been due to the shortage of children's mental health experts in the country. Tekola et al. (Reference Tekola, Baheretibeb, Roth, Tilahun, Fekadu, Hanlon and Hoekstra2016) cite the lack of traditional healers as participants as a limitation given their important role in the Ethiopian context.
Discussion
This review identified a number of themes that are important to implementation research in GMH, pointing both to gaps and strengths in the field. Improving GMH depends not only on implementing evidence-based interventions, but also on modifying and implementing interventions that anticipate local implementation barriers across behavioural, managerial, economic, and social domains. Understanding these complex barriers, and ensuring that equity in health can be championed, requires sophistication in the situational analysis. Our review explored various methodological approaches to situational analysis as a guide to enhancing implementation strategies. We discovered that relatively few studies address situational analyses in GMH, with additional key findings noting the paucity of local mental health system data and an absence of consideration of equity. Fortunately, our review also identified the development of several situational analysis tools that can serve as key resources, and a methodological strategy—mixed methods—that can address challenges.
We found that the scope of published situational analyses and formative research in GMH is limited. Twelve of the studies included in the review were representative of the PRIME or EMERALD studies, which both include sites in Ethiopia, India, Nepal, South Africa and Uganda, while EMERALD also includes Nigeria (Lund et al., Reference Lund, Tomlinson, De Silva, Fekadu, Shidhaye, Jordans, Petersen, Bhana, Kigozi, Prince, Thornicroft, Hanlon, Kakuma, McDaid, Saxena, Chisholm, Raja, Kippen-Wood, Honikman, Fairall and Patel2012; Mugisha et al., Reference Mugisha, Abdulmalik, Hanlon, Petersen, Lund, Upadhaya, Ahuja, Shidhaye, Mntambo, Alem, Gureje and Kigozi2017). PRIME and EMERALD are providing leadership in GMH implementation research (De Silva & Ryan, Reference De Silva and Ryan2016) and currently make up the majority of the published literature in this nascent field. There is a gap, however, in research representing Latin America and the Caribbean and the Middle East and North Africa, and there is limited research from the East Asia and Pacific region. There is a need for expanded investment in and dissemination of situational analyses from other geographic regions and other programs. The importance of formative research has been recognized in other global health disciplines (Scott et al., Reference Scott, Vian, Kaiser, Ngoma, Mataka, Henry, Biemba, Nambao and Hamer2018), but neither methodological approaches to formative research nor its importance is yet sufficiently described in the literature (Bentley et al., Reference Bentley, Johnson, Wasser, Creed-Kanashiro, Shroff, Fernandez Rao and Cunningham2014).
Though outside the scope of this review, an informal search of situational analysis literature and tools from HICs also revealed a gap. There appears to be limited peer-reviewed literature detailing situational analysis tools and methods in mental health or the broader health sector in HICs, though some examples are found in the grey literature. For example, Alberta Health Services in the Canadian province of Alberta conducted a situational analysis of the use of impact assessments in the health sector (Alberta Health Services, 2017). The methodology for this situational analysis was informed by a planning and evaluation framework that was developed internally and was not extensively described in the report. Situational analyses using methods such as Strengths, Weaknesses, Opportunities and Threats (SWOT) analysis seem to predominantly appear in the business and marketing domain in HICs. This dearth of literature on situational analyses from both LMICs and HICs represents a considerable opportunity for GMH researchers to provide leadership in this area and to make a substantial contribution to implementation research in mental health and in global health more broadly.
Many of the studies included in this review used or developed situational analysis tools that provide a comprehensive and systematic template for the analysis of complex factors at multiple levels of a mental health system. The PRIME investigators developed their own tool, adapted from WHO-AIMS, to assess district-level mental health needs (Hanlon et al., Reference Hanlon, Luitel, Kathree, Murhar, Shrivasta, Medhin, Ssebunnya, Fekadu, Shidhaye, Petersen, Jordans, Kigozi, Thornicroft, Patel, Tomlinson, Lund, Breuer, De Silva and Prince2014). Esan et al. (Reference Esan, Abdumalik, Eaton, Kola, Fadahunsi and Gureje2014) developed a tool to assess mental health systems across Anglophone West African countries and included qualitative components to capture the cultural and historical context of mental health. These tools represent an important foundational resource that can be used by GMH researchers conducting situational analyses and can be adapted to meet the needs of specific contexts and study objectives (Olofsson et al., Reference Olofsson, Sebastian and Jegannathan2018).
While the tools represent a considerable asset to GMH researchers, their potential to contribute to robust situational analysis research relies on the quality of their implementation and on the availability of secondary data. A major limitation identified by study authors was the often limited availability of mental health system data. Mental health information systems in LMICs are at varying stages of development and may be disjointed and under-resourced. Their strengthening has been identified as a priority in GMH (Ryan et al., Reference Ryan, De Silva, Terver, Ochi and Eaton2015). Publicly available mental health data are essential for completing comprehensive situational analyses, but the limited or inconsistent availability of data will remain a considerable limitation as long as mental health systems are still advancing. Further, most situational analysis tools do not capture the knowledge, beliefs and attitudes of mental health system stakeholders, which are essential to understanding culture, context and potential barriers and drivers of implementation (Proctor et al., Reference Proctor, Landsverk, Aarons, Chambers, Glisson and Mittman2009; Aarons et al., Reference Aarons, Hurlburt and Horwitz2011).
Using mixed methods to conduct situational analyses could help to mitigate some of these challenges, along with the limitations of both qualitative research and priority setting exercises described above. Mixed methods approaches combine both quantitative and qualitative data collection, analysis and interpretation in order to provide a deeper understanding of phenomena (Johnson et al., Reference Johnson, Onwuegbuzie and Turner2007; Creswell & Clark, Reference Creswell and Clark2011; Ostlund et al., Reference Ostlund, Kidd, Wengstrom and Rowa-Dewar2011). Mixed methods approaches are effective for triangulating data, or using various data sources or methods to improve depth of understanding and validate research findings (Carter et al., Reference Carter, Bryant-Lukosius, DiCenso, Blythe and Neville2014) and for capturing the complexity of health systems (Tariq & Woodman, Reference Tariq and Woodman2013). Despite the potential utility of mixed methods research, only six of the included studies used more than one method. The PRIME study was represented by nine studies in this review and while not all studies used mixed methods, the combined studies did involve mixed methods and priority setting exercises. While mixed methods can be more resource intensive, they should be considered when conducting situational analyses in order to ensure a more robust and comprehensive analysis of mental health systems. Mixed methods studies should be encouraged and supported by GMH implementation funding agencies to promote rigorous implementation research from the inception of research studies to their conclusion.
Finally, only three of the 24 studies explicitly considered equity in their study design. While the PRIME situational analysis tool does include indicators related to equity, these were not explicitly discussed in the papers included in this review. Equity on a global scale is a fundamental concern of GMH, which aims to close the gap in treatment within and between countries, improving access to and availability of treatment and improving the lives of people suffering from mental disorders (Patel et al., Reference Patel, Collins, Copeland, Kakuma, Katontoka, Lamichhane, Naik and Skeen2011). Implementation science has the potential to improve equity in health service delivery (Rasanathan & Diaz, Reference Rasanathan and Diaz2016). Implementation research in GMH, beginning with situational analyses, can provide important insight into equity gaps and opportunities to improve mental health equity. Including frameworks for assessing equity considerations in situational analysis, including mixed methods approaches that help to mitigate challenges related to poor data availability, study designs would allow for equity to be considered in the design, implementation and scale-up of interventions, programs and policies and for equity outcomes to subsequently be monitored. Equity is a broad and complex concept, the dimensions of which should be explored in further depth in relation to GMH implementation.
Limitations
We only included English language studies in this review which may have led to the omission of relevant research in this area published in other languages. It is also likely that situational analyses and formative studies have been conducted in GMH using different terminology and were thus not identified with the search terms used in this scoping review. The use of MeSH terms in the search may also have yielded additional results. We are confident, however, that the review has captured a representative sample of the GMH literature on situational analysis methodology in GMH, and that it offers a useful overview of current practice and guidance on next steps in this important field of research.
Conclusions
Implementation research is an essential area of study in GMH and will help to promote improved availability of, access to and reach of mental health services for people living with mental illness in LMICs. Formative research, including situational analysis, is an essential first step in conducting robust implementation research. While strong leadership in this field exists, there remain significant opportunities for enhanced research representing different LMICs and regions.
This review of existing methodological approaches in situational analysis for GMH reveals limitations and opportunities that can inform the design of future studies. The field will benefit from prioritizing mixed methods approaches to implementation research and including equity considerations in the study design of formative research, including situational analyses.
Acknowledgements
This review was conducted as part of the formative phase of the Enhanced Measurement-Based Care Effectiveness for Depression (EMBED) study, funded by the Canadian Institutes of Health Research and the National Natural Science Foundation of China through the Global Alliance on Chronic Disease [CIHR/ Team Grant: GACD Mental Health, ref GAC-154985; Agreement #01709-000]. The first author is supported by the MITACS Postdoctoral Fellowship.
Conflict of interest
RWL has received honoraria for ad hoc speaking or advising/consulting, or received research funds, from: Akili, Allergan, Asia-Pacific Economic Cooperation, BC Leading Edge Foundation, Brain Canada, Canadian Institutes of Health Research, Canadian Depression Research and Intervention Network, Canadian Network for Mood and Anxiety Treatments, Canadian Psychiatric Association, CME Institute, Hansoh, Janssen, Lundbeck, Lundbeck Institute, Medscape, Mind Mental Health Technologies, Otsuka, Pfizer, St. Jude Medical, University Health Network Foundation, and VGH Foundation.
CNS has received funds from the Ontario Brain Institute (OBI) and the Ontario Research Fund- Research Excellence Program. He has acted as a consultant for Pfizer, Lundbeck, Bayer and Otsuka.
SHK has received research funding or honoraria from the following sources: Abbott, Allergan, AstraZeneca, BMS, Brain Canada, Canadian Institutes for Health Research (CIHR), Janssen, Lundbeck, Lundbeck Institute, OMHF, Ontario Brain Institute, Ontario Research Fund (ORF), Otsuka, Pfizer, Servier, St. Jude Medical, Sunovion and Xian-Janssen.
SVP has received honoraria for consulting from Assurex and Takeda, honoraria for speaking from CANMAT, research grants from Assurex, Takeda, the Ontario Brain Institute, the Canadian Institutes for Health Research, and the Ethel and James Flinn Foundation; and has shares in Mensante.







 Open access
Open access