



Impact statement
Refugee caregivers play a critical role in mediating the impacts of forced displacement on children. This study adds to a growing evidence base of promising interventions to strengthen caregiver mental health and associated parenting behaviors in the aftermath of war and displacement. Programs such as the journey of life have the potential to support displaced families and communities around the globe, increasing recognition of the importance of positive parenting and caregiver well-being in promoting the health and well-being of children in situations of adversity.
Introduction
The current global refugee crisis is unprecedented, with over 84 million individuals having experienced forced displacement (UNHCR, 2022a). Such displacement curtails access to necessary resources, such as food and shelter, and access to institutional supports including health and protective services. These barriers, along with the potentially traumatic impacts of conflict, can lead to immense psychosocial challenges and have compounding negative effects on the mental health of the most vulnerable, including children. Mental health and psychosocial support describes any type of local or outside support that aims to protect and promote psychosocial well-being and/or prevent or treat mental disorders for people in crisis situations, including having supportive social relationships, accessing basic survival needs and accessing economic and environmental resources and addressing physical, intellectual, emotional and development needs (UNICEF Uganda, n.d.). Common mental health conditions among displaced children and adolescents include post-traumatic stress estimated at 22.7%, depression estimated at 13.8% and anxiety disorders estimated at 15.8% (Blackmore et al., Reference Blackmore, Boyle, Fazel, Ranasinha, Gray, Fitzgerald, Misso and Gibson-Helm2020). Interventions are urgently needed that address the mental health and psychosocial well-being among forcibly displaced children and adolescents.
Caregivers play a critical role in mediating the impacts of forced displacement on children and adolescents, as they may either heighten or mitigate the compounding detriments of conflict and displacement (Masten and Narayan, Reference Masten and Narayan2012). A review of research on refugees and immigrants found that poor caregiver mental health was associated with heightened affect- or avoidance-related behaviors, which heighten the risk for harsh or emotionally absent parenting (Timshel et al., Reference Timshel, Montgomery and Dalgaard2017). In one study among refugees in Uganda, a one-unit increase in a caregiver’s depression score tripled the odds that the adolescent in their care would have high levels of anxiety symptoms, and caregiver depression and violence exposure were both positively associated with symptoms of adolescent depression (Meyer et al., Reference Meyer, Steinhaus, Bangirana, Onyango-Mangen and Stark2017). Various studies, including a recent systematic review by Eltanamly et al. (Reference Eltanamly, Leijten, Jak and Overbeek2019), have found that caregiver stress and distress negatively affect parenting by increasing harsh parenting and reducing parental warmth.
Parenting programs, which support the creation of safe and nurturing environments for children by improving parents’ wellbeing and bolstering the knowledge and skills they already possess, have shown some promising results related to improved parenting behaviors and caregiver well-being when delivered in humanitarian settings (Miller et al., Reference Miller, Arnous, Tossyeh, Chen, Bakolis, Koppenol-Gonzalez, Nahas and Jordans2020). A recent systematic review found that participation in caregiving programs led to improvements in parenting skills, attitudes, child psychosocial outcomes and caregiver mental health (Gillespie et al., Reference Gillespie, Banegas, Chan, Ali Saleh Darawsha, Wasil, Marsalis and Gewirtz2022).
This manuscript examines the effectiveness of one such intervention, the journey of life (JoL), on caregiver well-being and caregiving behaviors in Kiryandongo refugee settlement, Uganda (Cohen et al., Reference Cohen, Hermosilla, Knox, Agaba, Obalim, Kajungu, Mangen and Stark2021). The primary hypothesis of the study was that the community-focused psychosocial support intervention of JoL would confer measurable benefits to individual mental health and psychosocial well-being, social support and community efficacy. This study adds to the existing literature addressing caregiver psychosocial interventions in humanitarian settings and may inform future program scale-up activities.
Methods
Setting
Uganda is one of the largest refugee-hosting nations in the world, with over 1.5 million refugees and asylum seekers (UNHCR, 2022b). Upon arrival in Uganda, incoming refugees are entitled to a range of services and resources including the right to employment, education and healthcare. Despite these rights, refugees report difficulty in accessing many of these resources (Meyer et al., Reference Meyer, Meyer, Bangirana, Mangen and Stark2019). Food insecurity and difficulty in meeting basic needs have led to increased stress and violence against children (VAC; Meyer et al., Reference Meyer, Meyer, Bangirana, Mangen and Stark2019).
This study was implemented in the Kiryandongo settlement in western Uganda during the COVID-19 pandemic. Kiryandongo is home to approximately 76,765 refugees (UNHCR, 2022c), the large majority of whom are from South Sudan (99%), while a minority are from the Democratic Republic of Congo, Sudan, Kenya, Burundi and Rwanda. Approximately 63% of the Kiryandongo population is under 18 years of age (UNHCR, 2022c). Children and adolescents in Kiryandongo report high levels of distress, with 30–50% meeting the criteria for anxiety and depression (Meyer et al., Reference Meyer, Steinhaus, Bangirana, Onyango-Mangen and Stark2017).
Intervention
The JoL intervention was originally developed by the Regional Psychosocial Support Initiative, a pan-African organization that provides holistic psychosocial care and support to youth in East and Southern Africa, to increase community knowledge and skills about child protection and the needs of vulnerable children, especially children affected by HIV/AIDS (Cohen et al., Reference Cohen, Hermosilla, Knox, Agaba, Obalim, Kajungu, Mangen and Stark2021). JoL engages community members at multiple socioecological levels (Bronfenbrenner, Reference Bronfenbrenner1979) through individual and community reflection, dialog and action. These activities are intended to improve psychosocial factors to ultimately promote the well-being of children.
JoL has been credited with improvements in communities’ awareness of issues affecting children. In Malawi, Ethiopia and Namibia, qualitative evaluation found that the intervention led to an increased awareness of children’s rights alongside a decrease in corporal punishment, early marriage and school absenteeism. Furthermore, communities developed sustainable strategies to support children, leading to improvements in child mental health and psychosocial outcomes such as coping skills, meaning-making, social functioning and social capital (Lush et al., Reference Lush, Urgoiti, Naris and Indongo2012; Lanhuang and Adefrsew, Reference Lanhuang and Adefrsew2013; The Government of Malawi, 2016). For the purposes of this study, JoL was expanded and adapted for humanitarian contexts by the Transcultural Psychosocial Organization (TPO) Uganda and Washington University St Louis.
The 12 sessions in the adapted JoL include psychoeducation, self-care, positive parenting, understanding children’s needs, identifying children who need help, building on children’s strengths and developing a community action plan. Elements of problem management plus (PM+) were included in the first four sessions in order to enhance problem-solving skills (WHO, 2016). Developed by the World Health Organization, PM+ was developed to help people with mental distress and those exposed to adversity manage their stressors with the intention of improving mental health and psychosocial well-being (WHO, 2016). The four sessions that incorporated elements of PM+ were placed before the eight JoL sessions, based on the hypothesis that improvements in caregiver mental health would lead to improved parenting through skills developed in JoL.
The manualized protocol was implemented at a ratio of one facilitator and one translator to 10 participants in the mixed gender groups. Each facilitator held a minimum of a bachelor’s degree in social work, psychology or a related field and had experience in the humanitarian sector. Each facilitator completed 2 weeks of training on the JoL program, including practice sessions and role plays. Translators supported facilitators as needed. Each translator held a minimum of a high school diploma and had experience translating between English and their native languages. Facilitators were provided with a digital version of the manual, a tablet and paper files for record keeping. The files were reviewed weekly by a supervisor for attendance and fidelity.
The intervention was provided in common spaces agreed upon by all group members, including watering holes, churches, child-friendly spaces, near markets, beneath mango trees or outside participant homes, if this was deemed a suitable option by all group participants. Groups were primarily conducted outdoor in the open air for participant comfort and because of COVID-19 safety protocols. Participants brought their own chairs or borrowed them in order to comfortably attend sessions. Sessions were held weekly and lasted an average of 2 h. Implementation adaptations included staff COVID-19 testing and wearing face masks, including throughout training and program meetings. Moreover, the group size was reduced to 10 participants rather than the initial plan of 20 participants per group; the plan of two social workers co-facilitating was retained.
Study design and sample size
The study (trial registration: NCT04817098) employed a quasi-experimental design where participants were divided into treatment or ‘care as usual’ groups based on geographic location in order to reduce spill-over effects (Cohen et al., Reference Cohen, Hermosilla, Knox, Agaba, Obalim, Kajungu, Mangen and Stark2021). The ‘care as usual’ group received the intervention after the completion of the study (i.e., waitlist control). To ensure sufficient power, we conducted a sample size calculation for mental distress, measured through the Kessler-6 (K6). The proposed minimum sample size (n = 960; assuming 80% retention of an initial n = 1,200) was adequate for detecting an effect size of 11% with 80% power. R (base library, command power.prop.test) was used to conduct the power analysis. There was no blinding of participants employed during the study procedures.
Participants
Participants were recruited from the Kiryandongo Settlement. Study participants in both the control and intervention groups were 18 years or older. Individuals were eligible to participate provided they had caregiver responsibilities for someone in their home under the age of 18 years and spoke one of the languages included in the study. All study participants provided written consent, and data were collected in Juba Arabic, Dinka, Nuer and Acholi.
Recruitment and data collection
Participant recruitment was conducted in collaboration with the TPO Uganda and their community partners. TPO Uganda staff coordinated with village health teams (VHTs) to share information about the intervention and evaluation and mobilize community participation. VHTs worked with local leaders to recruit community members to meet in a central location where TPO Uganda staff could introduce the intervention and study, inform community members about the risks and benefits to participation and record information of interested persons (e.g., name, age, gender, household refugee ID number). All participants who enrolled in the program and met the eligibility criteria were invited to participate in data collection. Those who provided written consent to enroll in the study were assigned unique study IDs. Of the 1,354 individuals eligible to participate in the evaluation, 1,338 consented to participate (see Figure 1).

Figure 1. Trial profile
Twenty-seven data collectors were employed across the baseline (May–June 2021) and endline, (September–November 2021). Each data collector was from Kiryandongo and represented primary ethnic groups, namely Dinka, Nuer and Acholi. They received 2 weeks of data collection training, study methodology, consenting processes and ethics, tablet use for data collection purposes and appropriate handling of adverse events. Data collectors and participants were matched by language and gender. The survey was translated into each of the primary study languages by a professional translator and further validated through cognitive interviewing. Baseline and endline interviews were conducted in or close to the participants’ homes, based on participant preference. Data were uploaded to a secure server and routinely checked by the research team.
Ethics
All study procedures were approved by TASO Uganda’s Institutional Review Board (IRB) and Washington University in St. Louis’s IRB. Eligible participants were systematically screened to determine whether they met the inclusion criteria and were competent to be interviewed. Data collection staff were trained and available to respond to questions regarding the consenting process. Consent was explained to the participants verbally and in a written format, and the participants signed or fingerprinted written consent for participation.
Measures of interest
The outcomes of interest were six continuous measures of well-being and parenting practices (see Table 1). The primary outcome was mental distress (K6) (Kessler et al., Reference Kessler, Green, Gruber, Sampson, Bromet, Cuitan, Furukawa, Gureje, Hinkov, Hu, Lara, Lee, Mneimneh, Myer, Oakley-Browne, Posada-Villa, Sagar, Viana and Zaslavsky2010). The five secondary outcomes of interest included: social support (Medical Outcomes Study [MOS]) (Moser et al., Reference Moser, Stuck, Silliman, Ganz and Clough-Gorr2012), functioning (World Health Organization Disability Assessment Schedule [WHODAS]) (Federici et al., Reference Federici, Bracalenti, Meloni and Luciano2017), parental warmth and affection (warmth/affection subscale of the Parental Acceptance and Rejection Questionnaire [PARQ]) (Rohner and Khaleque, Reference Rohner and Khaleque2005), parental undifferentiated rejection (undifferentiated rejection subscale of the PARQ) and attitudes toward VAC (VAC subscale of the Child Protection Index [CPI]) (Meyer et al., Reference Meyer, Steinhaus and Stark2015). All outcomes, except social support and parental warmth/affection, were reverse coded to support scale development and ease analysis, whereby higher scores represent more desirable outcomes. The Cronbach’s alpha value for these baseline measures were 0.76 (K6), 0.86 (MOS), 0.87 (WHODAS), 0.83 (PARQ warmth/affection subscale), 0.56 (PARQ undifferentiated rejection subscale) and 0.76 (CPI VAC subscale).
Table 1. Measurement of primary study outcomes for journey of life

Categorical demographic variables included age, income source, school attainment, years in Uganda and the number of children in the respondent’s care. Dichotomous demographic variables included past 3-month experience of food insecurity, marital status, country of origin and gender. Demographic covariates for the partially and fully adjusted models included age, gender, marital status, school attainment, number of children in the respondent’s care and food insecurity.
Analysis
Descriptive statistics were assessed for all variables. To address the imbalance between intervention group baseline characteristics (see Table 2), several analytical techniques were examined to condition for potential confounders: propensity score matching (PSM) and inverse probability weighting (IPW). Two versions of these models were examined, conditioning for different sets of variables: 1) the respective outcome measure at baseline, as well as the baseline demographic variables of age, schooling, number of children in care, food security, ranch, gender and marital status; and 2) all outcome measures at baseline, as well as the baseline variables of age, schooling, number of children in care, food security, ranch, gender and marital status. Finally, each of these models were run using listwise deletion and multiple imputations. Findings were consistent to directionality and significance across all models using (i.e., IPW vs. PSM, partial vs. full conditioning and listwise deletion vs. multiple imputations). In a deference to the most conservative approach, findings from the PSM approach using listwise deletion and the more comprehensive conditioning approach are presented.
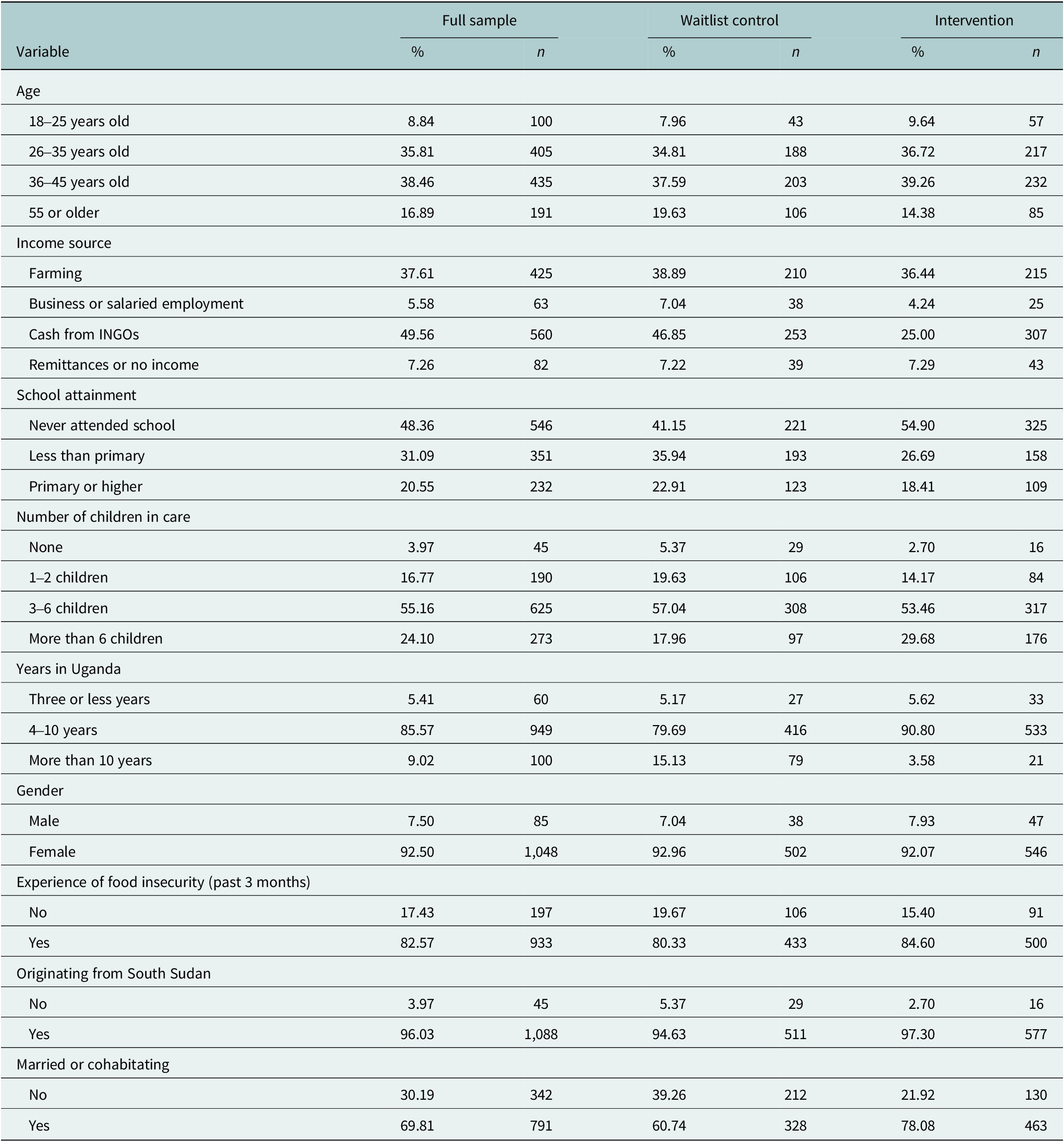
Table 2. Baseline descriptive statistics of the sample (n = 1,133)
Effect size was measured using Cohen’s d, or standardized mean difference, whereby a small effect is measured as at least 0.2, a medium effect as at least 0.5 and a large effect as at least 0.8. While not presented in the following tables, subgroup analysis was conducted to examine the varying effect for certain subgroups: each age category, females, and those with three to six children in their care. The only notable findings were for the subgroup of caregivers aged 18–25 years, with Cohen’s d values (including 95% CIs) consistently higher than those in the primary analysis. However, this finding should be viewed cautiously given the challenges of retaining intervention participants aged 18–25 years, with age being identified as not missing at random.
Intervention subgroup analyses were then conducted. After estimating the unadjusted effect of attendance, the models were adjusted for covariates of baseline demographics and the respective outcome (partially adjusted) and covariates of baseline demographics and all outcomes (fully adjusted). This subgroup analysis first examined the association between attending all 12 sessions and the six outcome measures, then examined the association between attending certain sessions (including all of the four first sessions with elements of PM+ and/or attending all of the eight subsequent sessions) and the six outcome measures. This analysis was conducted, in part, to assess whether the sessions with PM+ were driving any of the results or whether the full program model was responsible for the observed changes.
Analysis of missingness among the non-imputed sample (n = 1,133) indicated there were minimal demographic trends for missing observations at endline, aside from age and schooling. Participants aged 18–25 years and those who completed primary school were significantly more likely to be missing at endline (p < 0.001). All analyses were conducted using Stata15.
Results
Demographic characteristics
At baseline, almost all (96.03%) participants in the full sample originated from South Sudan. Most participants had spent 4–10 years in Uganda (85.57%), with only 9.02% living in Uganda for more than 10 years and 5.41% living in Uganda for 3 years or less (see Table 2). Most participants were married or cohabitating (69.81%) at baseline, and nearly all identified as female (92.50%). Participants often reported caring for multiple children, with 55.16% and 24.10% of participants reporting three to six and more than six children in their care, respectively. Another 16.77% of participants reported having one or two children in their care, and 3.97% reported having no children in their care.
Most participants were between the ages of 36 and 45 (38.46%) or 26 and 35 (35.81%) at baseline; only 16.89% of participants were 55 or older and 8.84% were between the ages of 18–25. Nearly half of the participants (49.56%) reported that cash from NGOs provided their primary income source; farming (37.61%) was also a commonly reported. The less common income sources included remittances or no income (7.26%) and business or salaried employment (5.58%). School attainment was low, as 48.36% of participants reported never attending school at baseline. Only 20.55% of the participants finished primary school, with the remaining 31.09% reporting to have attended school but not finished primary education. Food insecurity was common, as 82.57% of participants reported not having enough food because of limited resources within the 3 months prior to baseline data collection.
Effectiveness results
Findings from the PSM analysis demonstrate that JoL participation was strongly associated with each of the outcomes of interest (Table 3), with R-square values consistently around 0.11 (ranging from 0.1090 to 0.1115). In the fully adjusted models, JoL participation improved mental distress (coef.: 2.33; p < 0.001), social support (coef.: 1.45; p < 0.001), functioning (coef.: 2.64; p < 0.001), parental warmth/affection (coef.: 2.48; p < 0.001), undifferentiated rejection (coef.: 0.49; p < 0.001) and VAC attitudes (coef.: 1.98; p < 0.001).
Table 3. Propensity score matching analysis, treatment effect coefficients and Cohen’s d estimates
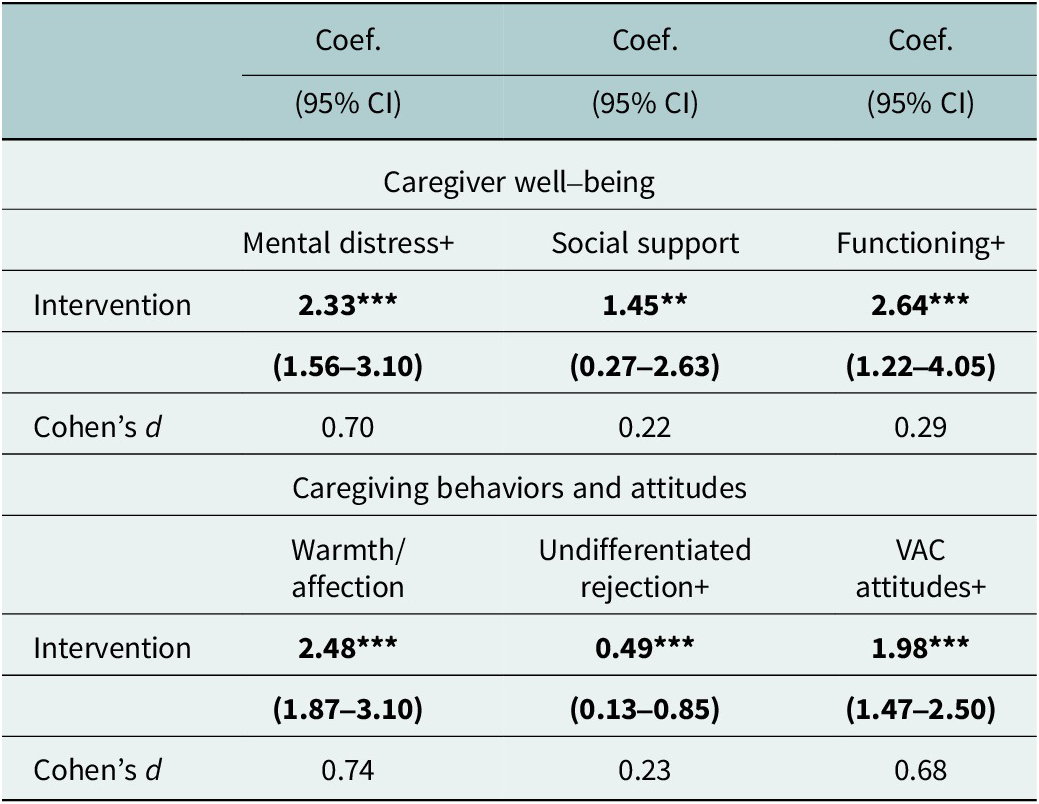
Note: A total of six models are presented in this table. All models are matched based on baseline variables of age, schooling, number of children in care, food security, ranch, gender, marital status and the baseline measures for all outcomes of interest. 95% CI: 95% confidence interval; All results with p < 0.05 are bolded. ***p < 0.001, **p < 0.01, *p < 0.05; + reflects an inverted score.
With varied scale ranges between outcome measures (e.g., 0–11 for VAC attitudes vs. 12–48 for functioning), PSM model coefficients cannot be directly compared. Thus, findings from the unadjusted Cohen’s d analysis bolster interpretation and comparability between outcome measures. A medium effect size was demonstrated for parental warmth/affection (0.74), mental distress (0.70) and VAC attitudes (0.68), whereas a small effect was demonstrated for functioning (0.29), parental undifferentiated rejection (0.23) and social support (0.22). In other words, the average parental warmth/affection score of the intervention group was 0.74 standard deviations greater than that of the waitlist control group.
Intervention attendance and subgroup effectiveness results
The majority of participants in the intervention group attended at least 9 of 12 sessions (i.e., 82.80% of the intervention group attended at least 75% of sessions). The remaining participants did not attend any session (6.74%) or attended between 1 and 8 sessions (10.46%). The skewed attendance distribution, including 33.56% attending all 12 sessions, limited the ability to examine the impact of attendance on outcomes in alignment with the 75% threshold determined in the study protocol paper (Cohen et al., Reference Cohen, Hermosilla, Knox, Agaba, Obalim, Kajungu, Mangen and Stark2021).
Instead, the subgroup analyses examined the association of attending certain sessions and the six outcome measures (see Table 4). The partially adjusted models that examined attending all of the first four sessions demonstrated that attendance was associated with improved social support (coef.: 1.35; p < 0.05) and worse undifferentiated rejection (coef.: −0.32; p < 0.05) compared to those who did not attend all of the first four sessions. The partially adjusted models that examined attending all of the final eight sessions demonstrated that attendance was associated with improved mental distress (coef.: 0.85; p < 0.05) and improved VAC attitudes (coef.: 0.54; p < 0.05) compared to those who did not attend all of the final eight sessions. There were no statistically significant associations in the fully adjusted models, except that attending all of the final eight sessions was associated with improved mental distress (coef.: 0.77; p < 0.05).
Table 4. Impact of PM+ and JoL attendance on mental health and caregiving, among intervention participants
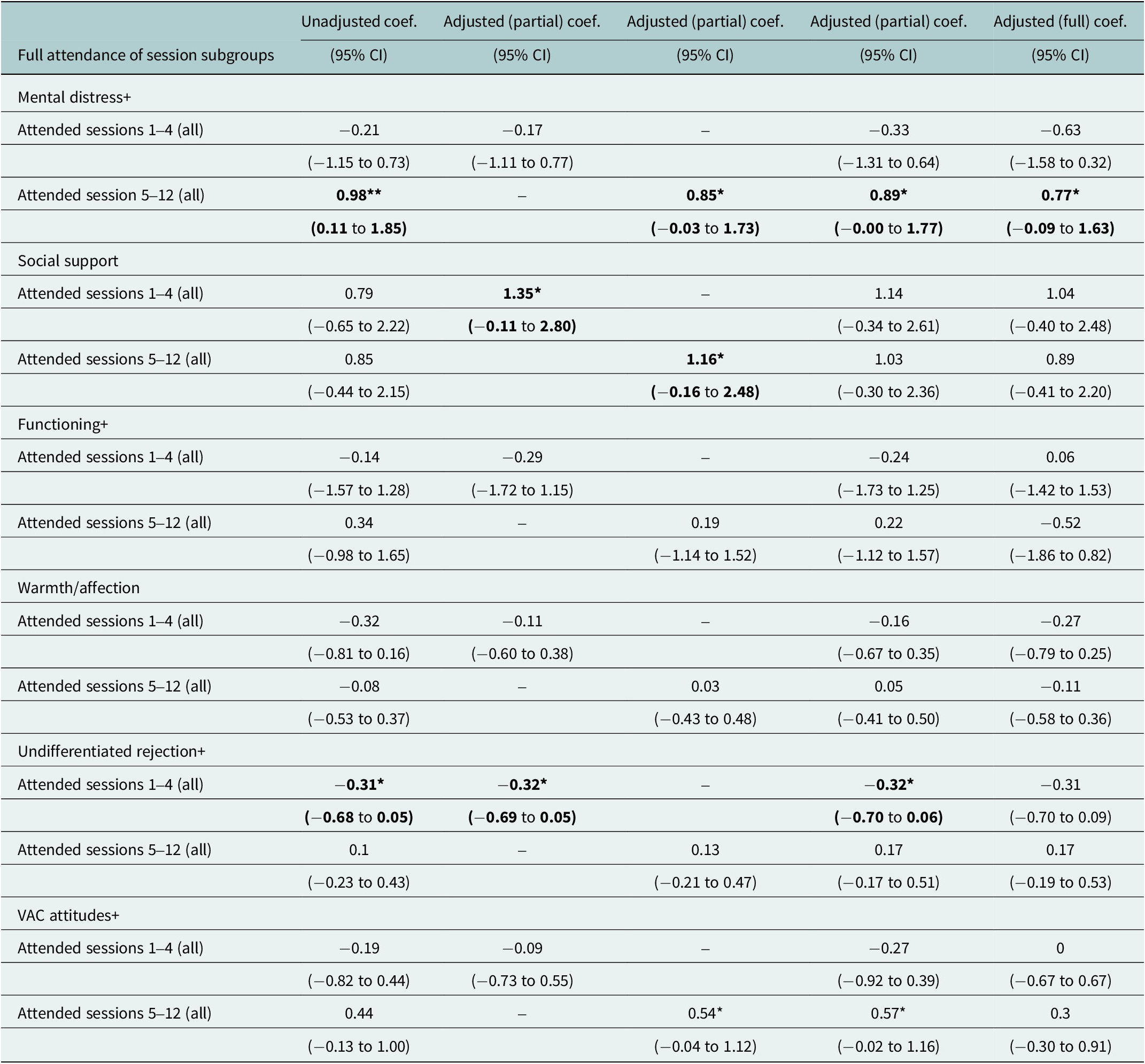
Note: Two binary independent variables of primary interest were examined: attending all of the first four sessions (sessions 1–4) vs. not and attending all of the final eight sessions (sessions 5–12) or not. A total of 36 models are presented in this table, whereby there are two unadjusted models per outcome, three partially adjusted models, and one fully adjusted model. Adjusted models (full and partial) include the respective outcome measure at baseline, as well as baseline covariates of age, schooling, number of children in care, food security, ranch, gender and marital status. Fully adjusted models also include all outcome measures at baseline. 95% CI: 95% confidence interval; ***p < 0.001, **p < 0.01, *p < 0.05; + reflects an inverted score.
Discussion
Examining the effectiveness of the JoL intervention among refugee caregivers in Uganda, this study highlights the value of integrating caregiver well-being and skill building as part of a holistic parenting programming in humanitarian settings. According to our primary PSM analysis, JoL led to significant improvements in mental distress (coef.: 2.33; p < 0.001), social support (coef.: 1.45; p < 0.001), functioning (coef.: 2.64; p < 0.001), parental warmth/affection (coef.: 2.48; p < 0.001), parental undifferentiated rejection (coef.: 0.49; p < 0.001) and VAC attitudes (coef.: 1.98; p < 0.001). Evidence from Cohen’s d analysis underscored the value of the intervention’s particularly pronounced effect on parental warmth/affection (0.74), mental distress (0.70) and VAC attitudes (0.68). Below, we explore the broader implications of these primary findings and opportunities to build upon the successes of this intervention.
Situating the primary findings within the existing evidence
Aligning with the family stress model, whereby chronic compounded stressors linked parental distress with threatening child well-being (Conger et al., Reference Conger, Ge, Elder, Lorenz and Simons1994; Meinhart et al., Reference Meinhart, Mangen, Hermosilla, Cohen, Agaba, Kajungu, Knox, Obalim and Stark2023), our findings suggest the potential for intergenerational impact from our mental health and psychosocial well-being findings alone. Previous research has already identified that parenting practices, attitudes and behaviors toward children can improve through enabling positive parenting (Ismayilova and Karimli, Reference Ismayilova and Karimli2020; McCoy et al., Reference McCoy, Melendez-Torres and Gardner2020). Mediation models from a randomized controlled trial of a caregiver support intervention among Syrian refugees in Lebanon found caregiver well-being accounted for 37% of the reduction in harsh parenting at the 3-month follow-up (Miller et al., Reference Miller, Chen, Koppenol-Gonzalex, Bakolis, Arnous, Tossyeh, Hassan, Saleh, Saade, Nahas, Abboud, Jawad and Jordans2022). Moreover, research among caregivers in Uganda identified a direct association between caregiver depression and anxious symptomology among their adolescent children (Meyer et al., Reference Meyer, Steinhaus, Bangirana, Onyango-Mangen and Stark2017). The well-being improvements among the JoL participants are particularly powerful because of the acute vulnerability of the study sample. Nearly half of the study participants never attended school (48.19%) and were reliant on cash from NGOs for income (49.47%). Moreover, the majority of participants (79.34%) had at least three children in their care. Our findings indicate intervention pathways to support the most vulnerable caregivers and, subsequently, their children.
Beyond these improvements in caregiver well-being, the intervention also showed improvements in pathways to positive parenting, both in terms of precursors to behavioral change (i.e., attitudes related to VAC) and also in terms of actual reported behavioral changes (i.e., parental warmth and acceptance and undifferentiated rejection). Existing intervention evidence demonstrates the positive child outcomes resulting from improved parenting skills and knowledge (Puffer et al., Reference Puffer, Green, Chase, Sim, Zayzay, Friis, Garcia-Rolland and Boone2015; El-Khani et al., Reference El-Khani, Maalouf, Baker, Zahra, Noubani and Cartwright2020; Miller et al., Reference Miller, Chen, Koppenol-Gonzalex, Bakolis, Arnous, Tossyeh, Hassan, Saleh, Saade, Nahas, Abboud, Jawad and Jordans2022). Recognizing the association between parental warmth and child well-being (Obando et al., Reference Obando, Wright and Hill2023), further investigation should examine the ways in which parental warmth and affection may mitigate the impact of stressors and/or directly improve well-being among children in humanitarian settings.
Intervention-specific considerations
The findings from the JoL study corroborate and build on the existing evidence base by suggesting that this intervention resulted in direct mental health and psychosocial benefits to caregivers in the form of reduced distress, improved functioning and improved social support. In our analysis of attendance data, we hypothesized that the majority of these direct improvements might be attributable to the first four sessions of the intervention that incorporated elements of PM+; however, these sessions did not fully account for the observed changes, suggesting that the remaining eight JoL sessions were also necessary for the observed improvements in caregiver well-being. Future studies would benefit from examining the mechanistic elements of sessions that may uniquely contribute to mental health psychosocial outcomes, as well as examining the dose–response of intervention sessions. These expansive considerations would help improve our understanding of whether it is the aggregate intervention or specific elements of the intervention that influence change.
We also note that parents who had completed primary school and those in the age range of 18–25 years were less likely to complete the endline survey. It is possible that younger participants and those with more basic education may have been more transient or difficult to reach, experienced more changes in life circumstances, or simply lost interest. Regardless of the reasons, this pattern suggests that additional work may need to be undertaken to consider particular demographic factors such as age and education level when designing and implementing parenting programming in humanitarian settings. Similarly, the large majority of participants in this study were female. Recognizing the challenge in recruiting male caregivers (Panter-Brick et al., Reference Panter-Brick, Burgess, Eggerman, McAllister, Pruett and Leckman2014), identifying alternate strategies for engaging men will better enable examination of the gendered impact of the JoL intervention in future studies. Similar considerations should be made for future studies in humanitarian settings that are interested in specific subgroups, such as groups based on country of origin or age.
Directions for future research
While the findings from this study are promising, future studies could helpfully answer important new questions. Our findings point to the potential benefits that would come from a third data collection point farther out from endline to look at sustained changes and to better understand mechanisms through which the program is affecting change. Future research might examine the moderating or mediating linkage between outcome measures. For example, an improvement in mental distress may enable caregivers to be more engaged in social networks. This social engagement might foster opportunities for caregivers to discuss their parenting experiences and challenges which, in turn, could influence parenting norms and behaviors in subsequently challenging situations.
Collecting data from children themselves could serve as means of triangulating reported caregiver behavioral outcomes and fostering a broader understanding the intervention implications for children. Research of parenting interventions has demonstrated positive influence on outcomes among children (Puffer et al., Reference Puffer, Green, Chase, Sim, Zayzay, Friis, Garcia-Rolland and Boone2015; El-Khani et al., Reference El-Khani, Maalouf, Baker, Zahra, Noubani and Cartwright2020; Miller et al., Reference Miller, Chen, Koppenol-Gonzalex, Bakolis, Arnous, Tossyeh, Hassan, Saleh, Saade, Nahas, Abboud, Jawad and Jordans2022); thus, similar examination into JoL would improve understanding of its potentially diverse implications within households and communities.
Limitations
The Cronbach’s alpha value for undifferentiated rejection was notably lower than the alphas for our other measures and should be carefully considered when interpreting findings. While the intervention’s undifferentiated rejection findings indicate the potential of JoL to impact caregiver behavior, we remain cautious in drawing firm conclusions due to the timing of the endline survey and the behavior measure itself. Another important limitation was the limited number of men recruited into the intervention and thus evaluated. The lack of randomization in the quasi-experimental design of the study is also important to consider; however, to the extent possible, baseline characteristics were controlled within the adjusted models. Finally, the COVID-19 pandemic introduced an additional stressor on refugee caregivers. While intervention adaptations were made as a result of the pandemic (see Intervention subsection), the study was unable to examine the extent that COVID-19 directly influenced intervention effectiveness.
Conclusion
Our results add to a growing evidence base around the role of caregiver mental health and parenting behaviors in the aftermath of war and displacement. With increasing recognition of the importance of positive parenting and caregiver well-being in promoting children’s health and well-being, programs like the JoL have the potential to support families and communities as the numbers of those displaced continue to rise worldwide.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2024.38.
Data availability statement
Data are available from PIs upon reasonable request.
Acknowledgments
The research team would like to acknowledge the research participants from Kiryandongo Settlement in Uganda and study team from the Transcultural Psychosocial Organization for their contributions throughout the study. This study is made possible by the support of the American People through USAID. The findings of this study are the sole responsibility of TPO Uganda and Washington University and do not necessarily reflect the views of USAID or the United States Government.
Author contribution
L.S. is the principal investigator and led manuscript development. R.S., G.S.A., J.O. and P.O.M. (co-PI) supported conceptual development and study implementation. F.C. managed oversight of data collection. S.R. and M.M. led data analysis, interpretation and supported manuscript development. All authors reviewed and approved the final manuscript prior to submission.
Financial support
This study was funded by the United States Agency for International Development (USAID) under the Health Evaluation and Applied Research Development (HEARD), Cooperative Agreement No. AID-OAA-A-17-00002. This study is made possible by the support of the American People through USAID. The findings of this study are the sole responsibility of TPO Uganda and Washington University and do not necessarily reflect the views of USAID or the United States Government.
Competing interest
The authors declare no conflicts of interest.
Ethics statement
All study procedures were approved by TASO Uganda’s Institutional Review Board (IRB) and by Washington University in St. Louis’s IRB. Consent was obtained from all participants.






 Open access
Open access
Comments
Dear editors,
Please find attached our manuscript, “Improving Psychosocial Wellbeing and Parenting Practices Among Refugees in Uganda: Results of the Journey of Life Effectiveness Trial” for consideration in Global Mental Health, special issue “Community-Based Psychosocial Support Interventions for Displaced and Conflict-Affected Populations.”
Our manuscript presents findings from an effectiveness trial of the Journey of Life (JoL) intervention to improve caregiver wellbeing and healthy parenting practices among refugees in Western Uganda. A quasi-experimental design was implemented in the Kiryandongo refugee settlement. Caregiver mental distress was the primary outcome, and secondary outcomes included functioning, social support, and caregiving attitudes and behaviors. Propensity score matching and Cohen’s D estimates were used to examine intervention effects. Per our primary PSM analysis, JoL led to significant improvements in measures mental distress (coef: 2.33; p<0.001), social support (coef: 1.45; p<0.001), functioning (coef: 2.64; p<0.001), parental warmth/affection (coef: 2.48; p<0.001), parental undifferentiated rejection (coef: 0.49; p<0.001), and VAC attitudes (coef: 1.98; p<0.001). Evidence from the Cohen’s d analysis emphasized the particular value of the intervention’s effect on parental warmth/affection (0.74), mental distress (0.70), and VAC attitudes (0.68). This trial adds much-needed evidence for the implementation of programming to improve the mental health of refugee caregivers to support positive parenting of refugee children.
As is customary, this letter should serve to certify that there are no prior publications or submissions with any overlapping information or study results, including studies and patients, and that there are no conflicts of interest among any of the authors. As the corresponding author, I confirm that the manuscript has been read and approved for submission by all named authors. If there is any other information you require, please do not hesitate to contact us. Thank you for your consideration.
Sincerely,
Dr. Lindsay Stark
Associate Dean of Global Programs
Professor of Public Health
Brown School at Washington University in St. Louis
Campus Box 1196, One Brookings Drive, St. Louis, MO 63130