



Introduction
In December 2019, the novel coronavirus pneumonia (NCP) first appeared in a city and rapidly spread [Reference Hui David1]. Coronavirus disease 2019 (COVID-19) is a new disease that can be transmitted by humans. It is highly infectious and has a high incidence. Currently, there is no effective treatment targeting its aetiology [Reference Li2]. Patients are still uncertain about whether they can fully recover, whether there are side-effects and whether the infection will relapse or infect others. Uncertainty in illness refers to a state of doubt and uncertainty caused by the lack of effective cognition of a disease and the lack of control over disease-related situations. It can lead to psychological states such as fear, and an increase in the psychological burden of patients, which can then affect the process of treatment [Reference Zhang3, Reference Shun4]. Coping is a kind of cognitive behaviour that patients may use to relieve their psychological stress. It is one of the important mediating factors in the process of dealing with psychological stress, which affects physical and mental recovery. Coping can be divided into three types: facing, avoiding and yielding. Generally speaking, facing is a positive coping style, while avoiding and yielding are negative coping styles [Reference Feifel5]. Some researchers have confirmed that adopting a positive and effective coping style can reduce a patient's uncertainty in illness, thus reducing the psychological pressure on them [Reference Bao6]. Currently, there is no research study on the correlation between disease uncertainty and coping style of severe COVID-19 patients in the world.
This study aimed to investigate the characteristics of uncertainty in illness and coping styles in patients with severe COVID-19, and explore the relationship between them, so as to guide patients towards adopting an appropriate coping style, which could reduce uncertainty in illness, and promote physical and mental health and well-being.
Subjects and methods
Study subjects
A cross-sectional survey was used. A total of 56 severe COVID-19 patients, admitted to a designated hospital in Wuhan between February 2020 and March 2020, were selected as the research objects. The inclusion criteria were as follows: (1) patients diagnosed with the severe type of COVID-19, according to the standard of COVID-19 prevention and control programme released by the National Health and Health Committee [7]. According to any of the following: (1) respiratory distress, RR ≥ 30 beats/min; (2) resting state, finger oxygen saturation ≤93%; (3) arterial partial pressure of oxygen (PaO2)/oxygen concentration (FiO2) ≤ 300 mmHg (1 mmHg = 0.133 kPa); (4) patients who were conscious and able to read and write; (5) patients who gave informed consent. The exclusion criteria were as follows: (1) patients with mental and psychological illnesses; (2) patients who were critically ill and could not complete the questionnaire.
Survey tools
General information questionnaire
The questionnaire was designed by the research team after they had reviewed the literature and consulted experts so that it could be used to evaluate the demographic and disease-related data of the patients. The following were included in the questionnaire: age, educational background, marital status, occupation, family residence, family economic situation and the existence of family infection.
The Mishel Uncertainty in Illness Scale for Adults (MUIS-A)
The MUIS-A was developed by the American nursing expert Mishel [Reference Mishel8] and translated into Chinese by Chinese researchers [Reference Xu9]. It can be used to measure the uncertainty level of patients with various diseases. The scale has 33 items, which fit into four different aspects: uncertainty, lack of information, complexity and unpredictability. All the items in this study were scored by the Likert 5 method. The total scores ranged from 32 to 160, 32.0–74.7 being low, 74.8–117.4 being moderate and 117.5–160.0 being high. The higher the score was, the higher the uncertainty in illness was. MUIS-A has good validity and reliability. The content validity index (CVI) of this study was 0.92, and the internal consistency reliability coefficient of Cronbach's α was 0.865.
The Medical Coping Style Questionnaire (MCMQ)
There were 20 items in the MCMQ [Reference Shen10] assigned to three coping styles: confrontation (eight items), avoidance (seven items) and acceptance/resignation (five items). The four-level scoring method (1–4 points) was used. The higher the score for each style, the higher the frequency of adopting that particular coping style. The internal consistency reliability coefficients of Cronbach's α were 0.72 for the confrontation style, 0.65 for avoidance and 0.70 for acceptance/resignation.
Quality control
The investigators were all medical staff who had received the same training. Before the beginning of the survey, the informed consent of each patient was obtained, and the same instructions were given to each patient as to how to fill in the questionnaire. If patients could not fill it in by themselves, the investigators would read to them and fill it in on their behalf. When collecting the questionnaire, the investigator checked carefully whether it was complete and, if any items were missing, it was returned to the patient to fill in. The returned questionnaires were sorted out so that the invalid ones could be eliminated. A total of 60 questionnaires were distributed, 56 valid questionnaires and four invalid questionnaires were collected, and the effective recovery rate was 93.3%. The reason for the invalid questionnaire was that the patients did not cooperate, thought that the questionnaire questions are too many, difficult to answer and quit halfway.
Statistic methods
SPSS20.0 software was used for the data analysis. The skewness coefficient, kurtosis coefficient and Kolmogrov−Smirnov normal test of single sample were used to judge whether the distribution was normal. The data that were in accordance with the normal distribution were described by means and standard deviations and an independent sample t-test and a one-way ANOVA were conducted. The data that did not conform to the normal distribution were analysed by the Mann−Whitney U non-parametric rank-sum test and the Kruskal−Wallis test and Pearson's correlation analysis was used to investigate the correlation. The level of significant difference was set as 0.05.
Results
The total score of disease uncertainty, the score of face, avoidance and coping of severe new crown patients with different characteristics were normal distribution.
Patients' uncertainty in illness
The total score of uncertainty in illness and the scores of each dimension are shown in Table 1. The total score of uncertainty in illness was 66.29 ± 17.25, which was a low level. The percentage of patients with uncertainty in illness of a low level was 64.29% (36/56), and those of a moderate and high level were 33.93% (19/56) and 1.78% (1/56), respectively. The average scores of the four aspects of single items from high to low were as follows: uncertainty, lack of information, complexity and unpredictability. There was no significant difference in the uncertainty in illness among patients of different age, gender, marital status, educational background or occupation, and neither did family residence, family economic status nor the existence of family infection have a differential effect (P > 0.05).
Table 1. Uncertainty in illness in patients with severe type of COVID-19 with different characteristics (n = 56)
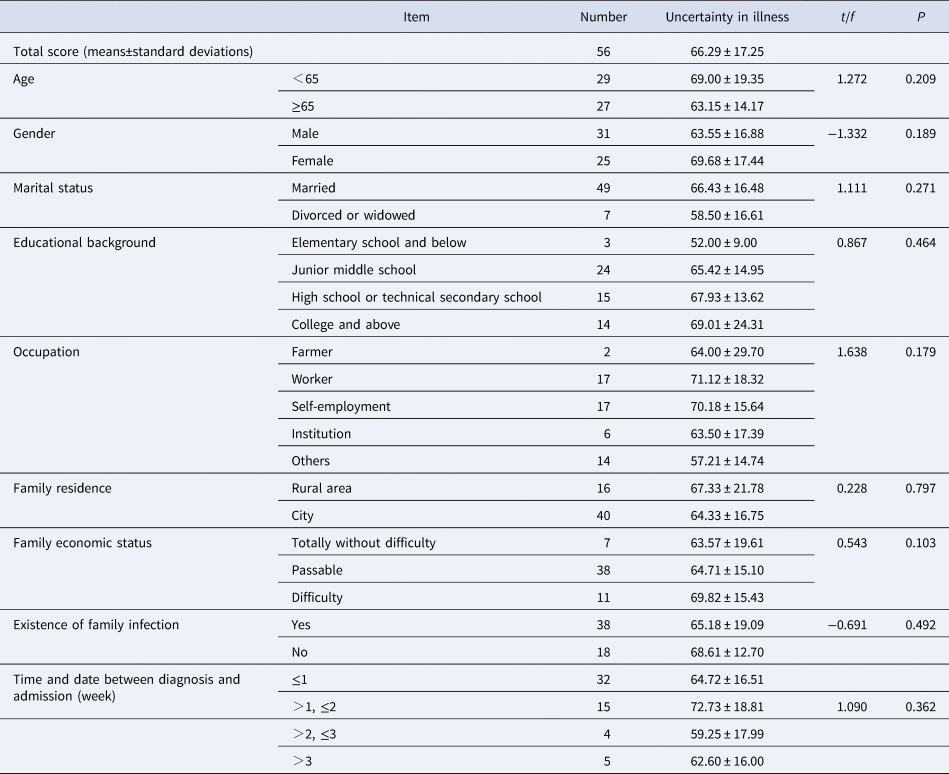
Note: *indicated the difference was statistically significant.
The coping style of patients
The total score of the coping style was 54.16 ± 6.39. Each type of coping style in this study was compared with the Chinese norm and the results showed that the scores of coping styles in this study were higher than those of the Chinese norm, and the scores of facing and avoidance were significantly higher than those of the Chinese norm. The differences were statistically significant, as shown in Table 2. There was no significant difference in the coping style of patients of different age, gender, marital status, educational background or occupation, and family residence and the existence of family disease also showed no significance (P > 0.05). However, a statistical significance did exist for the coping strategy of acceptance/resignation among patients with a different family economic status (P < 0.05), as demonstrated in Table 3.
Table 2. Comparison of coping style dimensions of patients with COVID-19 with the Chinese norm (n = 56)

Note: *indicated the difference was statistically significant.
Table 3. Coping style of patients with severe type of COVID-19 with different characteristics (n = 56)

Note: *indicated the difference was statistically significant.
Relationship between uncertainty of illness and coping style
The total score of uncertainty in illness correlated negatively with the coping style of facing and avoiding (r = −0.361, −0.343, P < 0.05), and correlated positively with the coping style of yielding (r = 0.315, P < 0.05).
Discussion
1. The results of this study showed that the total score of the MUIS of patients with COVID-19 was (66.29 ± 17.25), and the uncertainty in illness was at a moderate level, which was similar to the results of uncertainty of chronic diseases reported in both Chinese and foreign research [Reference Yang11–Reference Zhang13]. The average scores of the four aspects ranked from high to low are as follows: uncertainty, lack of information, complexity and unpredictability. The results suggested that the patients were not clear about the occurrence, development and prognosis of COVID-19 during hospitalisation, and they were prone to developing uncertainty in illness. The possible reasons for this might be that as COVID-19 is a new disease, there is no specific drug targeting it, and the long-term effect of treatment is unclear. This is likely to result in patients lacking confidence in the treatment and its outcomes, and becoming more afraid and sensitive. Secondly, COVID-19 is highly infectious and so patients need to be isolated while they are receiving treatment, which can stir up serious negative emotions. Moreover, COVID-19 has a long incubation period, and patients may worry about whether they have infected other members of their family. In addition, it is necessary to undertake continuous detection of indicators during isolation and before discharge. During this period of time, patients will also show uncertainty in illness [14]. Studies have shown that patients' uncertainty in illness aggravates anxiety and depression [Reference Wang15], increases the burden of self-perception, affects the recovery of physical function and quality of life [Reference Ahadzadeh16], and has adverse effects on prognosis. One study has pointed out that long-term uncertainty in illness may develop into long-term psychological stress and post-traumatic stress disorder [Reference Moreland17]. Therefore, medical staff should explain the science in an understandable way to patients with COVID-19 and help improve their understanding of the occurrence and development of the disease, drug treatment, prognosis, self-care and the current epidemic situation. If patients were given enough disease-related information support, this might reduce the uncertainty in illness. Peer support should also be encouraged, so patients with a good prognosis should be invited to talk to other patients about coping with the disease, and so increase their understanding of the disease process, treatment process and prognosis. For patients with a higher score of uncertainty in illness, follow-up should be carried out after discharge. Follow-up files should be established to track the level of uncertainty in illness in these patients. The psychological pressure on patients might be reduced through network support intervention.
2. The coping style of patients with COVID-19 was significantly better than that of the norm. The results indicated that some patients could actively confront the disease after learning about it. Combined with the current national attention and support for patients with COVID-19, the overall confidence of patients could increase. After the outbreak of the pandemic, all regions sent medical teams to assist Wuhan, and the government provided free treatment for patients with COVID-19. Moreover, the government provided financial support and arranged sites for isolation after discharge. All of these actions gave patients practical social support. However, some patients still adopted an attitude of avoidance towards treatment and the development of the disease. This is because although avoidance is not an escape and is merely a way of diverting attention or only temporarily alleviating a problem, it can reduce the occurrence of negative emotions to a certain extent [Reference Duan18]. In this study, patients with COVID-19 said they were unwilling to talk about their illness with friends or colleagues during their illness and isolation. They were afraid that they would be discriminated against and be isolated. Therefore, the avoidance style might be a protective coping style for patients with COVID-19, which might reduce the psychological pressure they are feeling. However, another study has pointed out that in the case of long-term avoidance, the treatment and prognosis of the patients would be affected [Reference Zhu19]. In addition, patients with family financial difficulties were more likely to accept/resign themselves to the situation as a way of coping. Although the government provided free treatment for patients with COVID-19 and the state reduced the financial burden on them, for patients on a low income, isolation would lead to their being unable to work, which would still affect their finances and psychological well-being.
3. The coping style of patients is one of the influencing factors of uncertainty in illness. In this study, the total score of uncertainty in illness correlated negatively with the coping styles of confrontation and avoidance (P < 0.05), and positively with the coping style of acceptance/resignation (P < 0.05). This suggests that the former are positive coping styles for patients with COVID-19, which can reduce the uncertainty in illness, while the latter is a negative coping style, which may aggravate the uncertainty. This was inconsistent with most other current research results. Many studies of patients with acquired immunodeficiency syndrome and cancer concluded that patients could reduce the uncertainty in illness by adopting an active coping style, while the level of uncertainty was higher when they adopted negative coping styles such as avoidance and acceptance/resignation. The possible reasons might, firstly, be, that since COVID-19 is an infectious disease, COVID-19 patients may feel stigmatised. Therefore, the coping style of avoidance might be beneficial to some patients and might work as a protective mechanism in the short term. Secondly, it might be correlated with the different personality characteristics of patients [Reference Schouws20]. Introverted patients might tend to adopt the coping style of avoidance, and this possibility needs to be further investigated.
4. During the isolation treatment, the more willing the patients are to actively face the disease, actively seek available social resources and communicate their feelings to other patients as well as the medical staff, the lower the uncertainty in illness is. On the contrary, acceptance/resignation was seen as a pessimistic way to deal with the events they are facing. When the patients adopted such an attitude and faced life with a negative attitude, the uncertainty in illness was relatively high. Thus, patients should be made aware of the efforts of the government and the determination of millions of people united in their effort to cope with the disease so that they feel encouraged to face the disease positively. When nursing patients, medical staff should inform the patients of the severity of the disease, together with its current treatability, best outcome and prognosis, so as to reduce the patient's anxiety. Finally, nursing staff should also pay close attention to the psychological state of patients, understand their coping styles and actively correct the less productive coping styles, so as to reduce uncertainty in illness and promote their physical and mental recovery.
This study was a cross-sectional study. The time of investigation was that China was in the period of outbreak. The Chinese government responded quickly and gradually controlled the malignant development of the epidemic. So the investigation was not repeatable. The investigated population came from the centre of the epidemic area, which was representative. To a certain extent, it can reflect the uncertainty of illness and coping style of patients with severe new coronavirus pneumonia. But the sample size is small, the conclusion of the evidence is insufficient; the survey results are the uncertainty of disease and coping style of severe patients in hospital, lack of evaluation results of other types such as mild, common and critical patients, so the research has some limitations.
In conclusion, the uncertainty of illness in patients with severe new coronavirus pneumonia was at a low level. The coping style of patients was one of the influencing factors of uncertainty in illness. Facing and evading is a positive coping style, which can reduce the uncertainty of new crown patients, while giving up is a negative coping style, which will aggravate the uncertainty of illness and pay close attention to patients in nursing. In order to reduce the uncertainty of the disease and promote the physical and mental recovery, we should actively correct the incorrect coping styles.
Financial support
Fujian Province Joint Fund For Science and Technology Innovation (Number:2017Y9052).
Data availability statement
All data generated or analysed during this study are included in this published article.




 Open access
Open access