


INTRODUCTION
The mortality rate associated with diarrhoea in children living in developing countries has shown a tendency to decline; however, it still represents a significant health-related issue that results in approximately 1·3 million deaths in children aged <5 years annually [Reference Black1]. In addition, estimated figures for morbidity remain unchanged at around 3·2 episodes/child annually [Reference Kosek, Bern and Guerrant2].
An episode of diarrhoea is an event that varies in duration and may be classified as acute (⩽14 days) or persistent (>14 days) diarrhoea [3]. This definition has allowed the identification of potential risk factors involved in episodes of persistent diarrhoea, such as inadequate diet, short duration of breastfeeding, poor nutritional status, micronutrient deficiency, inadequate hygiene behaviour and precarious socio-environmental and sanitary conditions, among others [Reference Mahalanabis4–Reference Bitarakwate, Mworozi and Kekitiinwa9]. Despite these findings, knowledge regarding diarrhoeal episodes of longer duration remains incomplete. For this reason, other methods of investigation have been developed, in which the duration of episodes is treated as a continuous response variable [Reference Mirza10–Reference Strina12]. We present the results of a longitudinal study conducted in Brazil with the aim of investigating the individual and contextual determinants of the duration, treated as a continuous variable, of episodes of diarrhoea in preschool-age children, using a hierarchical conceptual model that allowed us to measure the overall effects and their non-mediated (or direct) hierarchical components.
MATERIAL AND METHODS
Study design
The study was conducted between October 2000 and January 2002, and involved a sample of preschool-age children living in sentinel areas of the city of Salvador, a large urban centre of around 2·4 million inhabitants in northeastern Brazil. Details of the sampling procedure have been described elsewhere [Reference Teixeira13]. Briefly, ‘sentinel areas’ were delimited by aggregating adjacent census districts with similar socioeconomic and sanitary characteristics, and an original sample of 30 sentinel areas was randomly selected to represent the different income levels and sanitary conditions present in the city at that time. In each area, a random list of children aged <3 years was established at the beginning of the study, and the children were sequentially enrolled in this study as an open cohort. Data on the occurrence of diarrhoea were collected during twice-weekly visits with the use of questionnaires that were completed during interviews with the children's mothers or caregivers. The data obtained referred to the 3–4 days preceding the interview.
The 23 sentinel areas included in the present study, with a total of about 11 000 dwellings, refer to those in which there was no public sewage system. A total of 1233 children were enrolled over the first 10 months of the study. Of these, 693 children having at least one episode of diarrhoea and followed-up for at least 90 days were considered for analysis. A day of diarrhoea was defined as the occurrence of ⩾3 more watery or soft stools within a 24-h period [Reference Barreto14, Reference Morris, Cousens, Lanata and Kirkwood15], and a diarrhoea episode was identified by a minimum 3-day diarrhoea-free gap (following our definition of day of diarrhoea) to mark the beginning of a new episode [Reference Baqui16]. The study endpoint was the duration of episodes, defined as a continuous variable.
Conceptual model and study variables
A hierarchical conceptual model, reflecting our proposed causal frame of diarrhoea, was established to map the determinants of the duration of diarrhoeal episodes. It included contextual factors (those referring to the sentinel areas in which the children resided) [Reference Diez Roux17, Reference O'Campo18] and individual factors, that were organized hierarchically into four blocks in two levels, in accordance with their proximal-distal relationships to outcome [Reference Genser19–Reference Ferrer21] (Fig. 1). This strategy allowed us to estimate the overall effects and their non-mediated (direct) components.
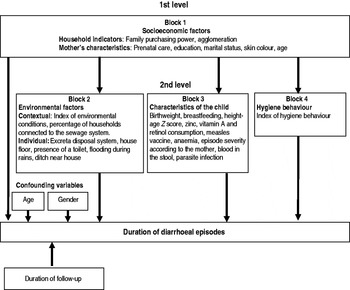
Fig. 1. Hierarchical conceptual model.
Socioeconomic factors occupied the most distal level, and the second level included more proximal routes: environmental determinants (block 2), characteristics of the child (block 3) and hygienic behaviours (block 4). Most of the variables in blocks 1–3 were collected only once, at the beginning of follow-up, using a previously codified and standardized questionnaire. Data regarding mother's marital status and education level, presence of streams or ditches close to the home, quality of floor, sewage disposal system and presence of an indoor toilet were collected at least twice during the study, using supplementary questionnaires. Anthropometric measurements were obtained at three different time points (at the beginning of the study, at 6 months, and at 12 months follow-up).
In block 1, family purchasing power was defined by the possession of selected goods (washing machine, microwave oven, telephone and computer, etc.), and was subsequently dichotomized into low (<0·17) or fair/good (⩾0·17) in accordance with the median value calculated.
The contextual variables in block 2 (index of environmental conditions and percentage of homes connected to the sewage system) were based on data obtained during previous field surveys on technical and operational aspects concerning water supply system, sewage system, drainage system and garbage collection system, details of which have been published previously [Reference Milroy, Borja and Barros22, Reference Barreto23]. The percentage of households connected to the sewage system was classified into quartiles as very low (<34·1%), low (⩾34·1% to <47·2%), normal (⩾47·2% to <55·1%) or good (⩾55·1%).
From a single-occasion dietary survey by 24-h recall [Reference Magalhães, Oliveira and Santos24], conducted by nutritionists and applied to the children's mothers or caregivers, the daily consumption of zinc, vitamin A and retinol was estimated [Reference Philippi, Szarfarc and Latterza25]. Their median levels (3·49 mg, 1705 μg, 448 μg, respectively) were used as cut-off values for classifying the children (block 3). The severity of the diarrhoea episode, according to the perception of the mothers/caregivers, was considered to represent the child's state of health on the first day of the episode. The anthropometric indicator height/age (H/A) and weight/age (W/A), expressed as H/A and W/A Z scores, were calculated using the ANTHRO software program (CDC/WHO, 1990). Stool samples, collected on a single occasion, were examined using the Kato-Katz method [Reference Katz, Chaves and Pellegrino26] to identify and quantify Trichuris trichiura, Ascaris lumbricoides and Ancylostomatidae eggs. Giardia lamblia cysts were identified by sedimentation technique. Haemoglobin levels were measured with a portable haemoglobinometer (HemoCue AB, Sweden), and a cut-off value of 11 g/dl was employed to classify a child as anaemic [Reference Hunter and Smith27] (block 3). The individual hygiene behaviour score (block 4) was constructed from 33 forms of hygienic [Reference Morris, Cousens, Lanata and Kirkwood15] or unhygienic [Reference O'Campo18] behaviour by the child or his/her caretaker, observed during the home visits [Reference Strina28].
This study was approved by the Research Ethics Committee of the Federal University of Bahia. The children were only included in the study after the parents or guardians had read and signed a statement of free and informed consent. Whenever necessary, the field workers counselled the mothers regarding seeking healthcare services.
Statistical analysis
In the bivariate and multivariate analyses, the duration of diarrhoeal episodes was modelled through gamma generalized linear model (GLM) equations for population mean response with identity link function. This method can efficiently deal with asymmetric and correlated continuous data [Reference Cordeiro29–Reference Twisk31]. The Huber sandwich estimator was used to correct possible violations of non-independence and mis-specification of the probability distribution [Reference Harrell30]. In the bivariate analyses, missing data of explanatory variables were treated as a separate category [Reference Mirza10, Reference Genser19], except for H/A and W/A Z scores, whose missing values were imputed with the modal value [Reference Twisk32]. In all multivariate models, missing values for explanatory variables were all imputed with their modal values.
An effect-decomposition strategy was applied for multivariate analysis [Reference Victora20]. For each block of potential determinants, we used a backward elimination procedure to select the significant determinants (P⩽0·10), and only these were admitted to the following multivariate stage, where several GLM equations for the population mean response were sequentially fitted by including the blocks step-by-step according to the predefined hierarchy. This methodology allowed us to estimate the mean increase (or decrease) of duration of diarrhoeal episodes (β) compared to the reference category of a given variable. Following our conceptual framework (Fig. 1), we fitted five gamma GLMs. Model A estimated the overall effect of the socioeconomic determinants. Models B, C and D, which included the determinants of blocks 2–4, respectively, estimated the effect of the socioeconomic determinants not mediated by the corresponding blocks above, taken individually. Model E estimated the effect of the socioeconomic determinants not mediated simultaneously by the determinants of blocks 2–4, as well as the overall effects of blocks 2–4. All models were adjusted for possible confounding factors (child's gender and age at onset of the episode, and follow-up duration in months). Additional analyses were performed of possible modifying effects of contextual determinants on the association of individual determinants and duration of diarrhoea in models A and E. The Anscombe residual was used to diagnose the adjustment of the gamma GLM for population mean response [Reference Cordeiro29]. All statistical analyses were performed using Stata version 9.0 (StataCorp., USA).
RESULTS
The study population consisted of 693 children (53·8% boys), aged 6–36 months at the start of the study. They were followed up for a total of 216 392 child-days [median follow-up 355 days, interquartile range (IQR) 291–383) days]. A total of 2397 episodes of diarrhoea were recorded, 46·0% of which lasted for 1 day, 77·8% for up to 3 days with 1·1% persisting for ⩾14 days. The incidence rate was 3·13 episodes/child per year (95% confidence interval 2·91–3·38), and the median duration of the episodes was 2 days (IQR 1–3 days) overall. Both the incidence rate and duration tended to decrease with age (Table 1).
Table 1. Incidence and duration of diarrhoeal episodes, by age
CI, confidence interval; IQR, Interquartile range.
A table listing the results of the bivariate analyses of all investigated variables in each block of the conceptual model is available online (Supplementary Table 1). We identified potential risk factors in all blocks. Very poor environmental conditions, poor quality of floor, absence of a toilet in the house, presence of a ditch close to the household and a very low percentage of households connected to the sewage system, all in the environmental block, were among the variables most strongly associated with longer duration of diarrhoea (with 1·12, 0·96, 0·91, 0·89 and 0·88 days of mean increase of duration, respectively), followed, in block 1, by maternal age <19 years (which, with β=1·16, showed the highest risk), household crowding (β=0·75) and family low purchasing power (β=0·47). Other factors associated with longer duration of diarrhoea were no dose of measles vaccine (β=0·85), H/A Z score <−2 (β=0·82), haemoglobin level <11 g/dl (β=0·67), episode severity (β=0·55), breastfeeding for <6 months (β=0·87), intestinal infection by T. trichiura or hookworm (β=0·87, β=0·80, respectively) and a predominantly negative pattern of hygiene behaviour (β=0·78).
Table 2 summarizes the results of the effect-decomposition strategy of analysis, obtained by adjusting five gamma GLMs (see Methods section). Low family purchasing power, crowding, mother's young age, low percentage of households connected to the sewage system, low consumption of zinc, and severity of the episode according to the perception of mother/caregiver were all significantly associated with increasing duration of diarrhoeal episodes (models A and E). Interestingly, the effects of the socioeconomic determinants on duration of diarrhoea decreased after adjusting for variables in blocks 2–4. The effect of family purchasing power (β=0·31) decreased after adjusting for variables in block 2 (β=0·22) or, less so, in block 3 (β=0·28), crowding effect (β=0·62) decreased after adjusting for hygiene behaviour (β=0·49), and mother's young age effect (β=0·68) decreased after adjusting for variables in block 3 (β=0·56) and block 4 (β=0·59).
Table 2. Effect of the determinants of duration of diarrhoea in different models

Shaded cells indicate best models for levels 1 and 2.
* See Methods section – Conceptual model and study variables.
† Reference category.
‡ P⩽0·05.
§ P⩽0·10.
|| Strina et al. [Reference Strina28].
In the multivariate analyses including interaction terms (extensions of models A and E; data not shown), significant product terms were found between the percentage of households connected to the sewage system (contextual variable), and two individual variables, measles vaccine status and breastfeeding. The overall effects of no dose of vaccine and being breastfed for <6 months were −0·08 and 0·43 days, respectively, when the percentage of households connected to the sewage system was good, and 0·57 and 0·73 days, respectively, when the percentage of households connected was very low.
DISCUSSION
This study aimed to identify factors associated with the duration of diarrhoeal episodes. Unlike most longitudinal studies in which duration is treated dichotomously (acute episodes vs. persistent episodes), this is one of the few studies in which the episode duration was treated as a continuous variable [Reference Mirza10, Reference Strina28]. In fact, the recommended cut-off point of ⩾14 days used to define persistent episodes of diarrhoea [3] is to a certain extent arbitrary, since there is no convincing evidence that this represents a subgroup completely apart from that of the acute episodes [Reference Mahalanabis4, Reference Mirza10]. Moreover, estimates of risk associated with episodes of longer duration may be difficult to assess through a categorical approach, when those episodes represent just a small proportion of the total, as is often the case.
A hierarchical model was used, with the block of socioeconomic determinants occupying the distal level, and the environmental determinants, along with those related to biological characteristics of the children and to hygienic habits, occupying the proximal level. The effect-decomposition analytical strategy allowed us to extract the non-mediated (or direct) components of the overall effects, under the assumption of the absence of confounding at the level of the intermediate variables [Reference Genser19]. However, this potential limitation is mitigated by the fact that our model included a wide range of factors potentially acting on the duration of diarrhoeal episodes and grouped them in meaningful blocks, thus making it unlikely that unobserved factors are associated with both an intermediate block and outcome.
Due to the asymmetrical distribution of episode duration as a continuous variable, the dependence arising from recurrent episodes in the same individual, and our interest in duration in its natural scale and not in ratios, the gamma GLM for population mean response with identity link function was applied in the bivariate and hierarchical analyses.
Bivariate analysis identified significant determinants of duration of diarrhoea in each of the four blocks: reduced purchasing power, crowding, low level of education, and unmarried mother (block 1); low or fair proportion of dwellings connected to the sewage system, presence of a stream or a ditch near the house, and poor quality of floor (block 2); breastfeeding <6 months, episode severity according to mother/caregiver, no measles vaccine, low haemoglobin level and hookworm infection (block 3); and negative hygiene behaviours in block 4 (Supplementary Table 1). Most of these factors remained significant in intra-block analyses (data not shown).
In our analysis, the overall effects of the socioeconomic factors ranked among the strongest determinants of duration of diarrhoea (Table 2, model A). They were partly mediated, however, by proximal variables (Table 2, model E): the low purchasing power effect was in part explained by environmental, child-related or hygiene behaviour-related variables, the crowding effect was in part explained by hygienic negative behaviours, and the effect of young age of mother was reduced by child-related variables or hygienic negative behaviour (Table 2, models B, C, D).
A low or very low proportion of dwellings connected to the sewage system was associated with a longer duration of episode, as was hookworm infection (Table 2, model E). Unlike the findings of Lima et al. [Reference Lima33], no statistically significant association was found between intestinal infections by G. lamblia and the duration of diarrhoeal episodes.
A noticeable, although non-significant, association was found between duration of diarrhoea and breastfeeding for <6 months, in line with results from other studies [Reference Mirza10, Reference Strina28, Reference Mølbak34] (Table 2, model E). A low intake of zinc, despite the limitations of the measure used [Reference Philippi, Szarfarc and Latterza25], was also associated with longer episodes, a finding consistent with zinc supplementation being reported to significantly reduce duration of diarrhoea in children [Reference Bitarakwate, Mworozi and Kekitiinwa9, Reference Dutta35]. Few studies have been conducted to evaluate the association between hygiene behaviour and duration of episodes of diarrhoea. In the present investigation, predominantly negative behaviours contributed to increasing the duration. These findings are consistent with results from other studies that have reported longer episodes of diarrhoea resulting from the use of dirty utensils, the mother or child not washing hands after using the toilet, or food remaining unprotected for long periods of time [Reference Mahalanabis4, Reference U6, Reference Mirza10, Reference Strina28].
Sanitary conditions (percentage of households connected to the sewage system) were found to constitute a potential modifier of the effect of measles vaccine and breastfeeding on duration of diarrhoea. These results are in agreement with the findings of other studies that have reported the protective role of measles vaccine [Reference Mølbak34, Reference Feachem and Koblinsky36, Reference Fine37] and breastfeeding [Reference Mahalanabis4, Reference Mirza10] on duration of diarrhoea in areas where the sanitation infrastructure is poor [Reference VanDerslice, Popkin and Briscoe38].
Although longitudinal prevalence of diarrhoea is considered a better predictor than incidence of mortality associated with childhood diarrhoea [Reference Morris39], it still ignores the dimension represented by duration, and treats, for example, a single long episode the same way as two or more shorter episodes with an equal overall duration, thus overlooking the importance of the cumulative effect of the days with diarrhoea experienced by children suffering from a prolonged episode [Reference Lima33]. Studying the duration of the episodes allows us to enrich with further elements the epidemiology of diarrhoea.
Despite the time elapsed since the study was undertaken, and the changes that occurred in the meantime in the local situation (e.g. improvement of sanitation and introduction of rotavirus vaccine), our investigation is still of relevance, for at least two reasons. First, for future comparison with the present situation in Salvador; and second, because there are numerous places worldwide where the present situation is similar to the situation that prevailed in Salvador some years ago.
In conclusion, the results of this study suggest that when an episode of diarrhoea occurs, its duration is affected by the socioeconomic conditions of the family and by the environmental and sanitary infrastructure, as well as by nutritional and immunological factors, and that the context acts as a potential modifier of the effect of some factors.
NOTE
Supplementary material accompanies this paper on the Journal's website (http://journals.cambridge.org/hyg).
ACKNOWLEDGEMENTS
Financial support for the study was provided by the PRONEX Centres of Excellence Program, CNPq, Brazilian Federal Government (Grant 661086/1998–4) and the Department of Infrastructure, State Government of Bahia. The authors thank the field work team and the families that participated in the study.
DECLARATION OF INTEREST
None.





