



Background
Risky sexual behaviour (RSB) is defined as any sexual activity that increases the risk of acquiring sexually transmitted infections (STI) and unwanted pregnancies [Reference Eaton1]. RSB is a major public health problem around the globe [Reference Brener2]. RSB includes having sex with multiple sexual partners, not using or inconsistent condom use, sexual intercourse under the influence of substance use [Reference Tilahun and Mamo3]. If not appropriate interventions exist, unsafe behaviours can expose them to a higher risk of acquiring HIV, other STIs and unwanted pregnancy [Reference Mamo, Admasu and Berta4].
Globally, young people (15–35 years of age) are the most susceptible groups for RSB and account for an estimated 45% of new HIV infections [Reference Dadi and Teklu5]. RSB can be aggravated by low income, job insecurity, lack of awareness about sexual and reproductive health issues and harmful traditional practices [Reference Muche6]. University students are viewed as being at higher risks to acquire HIV infection or STI and they are categorized under the most at-risk population due to their engagement in RSB and their sense of non-vulnerability [Reference Jibril and Kibru7].
It is considered that University and College students are aware of HIV risks and preventive mechanisms; however, evidence showed that they are usually engaged in higher in RSB [Reference Gebresllasie, Tsadik and Berhane8]. Promoting safe sexual activity would contribute to the reduction of sex-related morbidity and mortality caused by unsafe abortion and HIV. Unprotected sexual practice and the associated exposure to infection is one of the major causes of preventable mortality in low and middle-income countries. It is the major mode of transmission for HIV and human papillomavirus, about the mortality of more than one million people worldwide [Reference Ross9].
According to the result of different studies, the extent of RSB among university students in Africa is high. The prevalence of RSB was 26% in Uganda [Reference Musiime and Mugisha10], 63.9% in Botswana [Reference Hoque11] and 63% in Nigeria [Reference Omoteso12].
In Ethiopia, youth people represented one of the country's largest groups, comprising about 35% of the population, and University students are exposed to RSB such as unsafe sex leading to HIV infection and other STIs as well as unwanted pregnancies [Reference Shore and Shunu13]. Identifying the determinant factors of RSB among University students is also an important indicator for the rest young population to take appropriate preventive measures [Reference Kovács14]. They are more susceptible to wider sexual and reproductive health problems due to the new environment in the universities with poor protection [Reference Derese, Seme and Misganaw15]. Age and the need to explore life, financial benefit, substance use, peer pressure and absence of preventive strategies and living independently away from home were considered important factors for RSB [Reference Shore and Shunu13].
There are studies about University students' in African countries indicating a higher prevalence of RSB [Reference Mekuanint16]. However, the determinant factors of RSB among University students are not well known in the study area. RSB such as having multiple sexual partners and sexual intercourse without a condom with a non-regular partner is a common practice [Reference Tura, Alemseged and Dejene17]. Therefore the purpose of this study was to assess the prevalence and determinant factors of RSB among University of Gondar undergraduate students, Northwest Ethiopia.
Method and materials
Study design and period
An institution-based cross-sectional study was conducted from June to 30 July 2019.
Study area
The study area was at the University of Gondar which is located 750 km far from Addis Ababa, the capital city of Ethiopia. It is one of the first generation universities in Ethiopia and was established as a public health college in 1954.
Study participants
Those students who were available during the data collection period were included in the study. While those students who were not present during the data collection period were excluded from the study.
Sample size determination and sampling technique
The sample size was calculated using the single population proportion formula by taking the estimated proportion of RSB 46.6% from a study conducted in southwest Ethiopia [Reference Tilahun and Mamo3], 95% confidence interval (CI) and a 5% margin of error. The final sample size was 420 after adding a 10% non-response rate. The proportional allocation formula was used to allocate the number of students to the five campuses. Then the sampling frame was prepared for each campus by having lists of students from the main registrar's office. Finally, the study participants were selected using a simple random sampling technique.
Operational definitions
Risky sexual behaviours
Having more than one sexual partner or inconsistent condom use/not using a condom during sex in a lifetime.
Data collection tools and procedure
A structured pre-tested self-administered questionnaire was used to collect the data. The tool was arranged into four categories; the first part of the questionnaire contains the socio-demographic characteristics of the participants, the second part describes sexual experience-related variables, the third section states the sexual behaviour in the past 12 months, and the last section contains RSB related questions. There were three trained BSc nurse data collectors and two MSc nurse supervisors during data collection.
Data quality control
Before the actual data collection period, the tool was pretested with 5% of the total sample size. Amendments on the instrument, such as unclear questions and ambiguous words made accordingly. The pretest was also be used to estimate how much time it takes to administer the entire questionnaire. The tool was first developed in the English language and translated to the Amharic language with back translation to English for consistency. The one-day training was given to data collectors and supervisors on the objective of the study, instrument and data collection procedures by the principal investigators. Supervision was conducted by the principal investigators and supervisors. To ensure data quality, each data collector checked the questionnaire from each study participant for completeness. The supervisors and principal investigators review each questionnaire daily and check for completeness.
Data processing and analysis
Before the analysis data clean-up and cross-checking were done. Then the data were entered into Epi-info version 7.0 and exported to Statistical Package for Social Sciences (SPSS) version 25 for analysis [18]. Descriptive statistics like frequencies, percentages and tables were used to present data. To assess the association between the different independent variables (Age, marital status, residence, mother's education, living arrangement, daily religious attendance, chew chat, drink alcohol, ever see pornography and having information about reproductive health and sexually transmitted diseases) with the dependent variable (RSB), first, bivariable relationships between each independent variable and outcome variable were investigated using a binary logistic regression model. Those independent variables with a P-value <0.2 at the bivariable level were eligible for multivariable analysis to control potential confounding factors. After adjusting their effect on the outcome variable, those variables with a P-value < 0.05 with a 95% CI were considered as significantly associated with RSB.
Ethical consideration
Ethical clearance was sought from the University of Gondar, School of Nursing. From the campus dean's office, a written letter was taken. The participants were informed and written consent was obtained from each study participant. Omitting direct personal identifiers on the questionnaire, by using code numbers, storing data locked with a password and not misusing or wrongfully disclosing their information were considered to maintain confidentiality. Study participants were also informed that involvement was a volunteer and they can take out from the study involvement at any step if they are not happy with the study.
Results
Socio-demographic characteristics of respondents
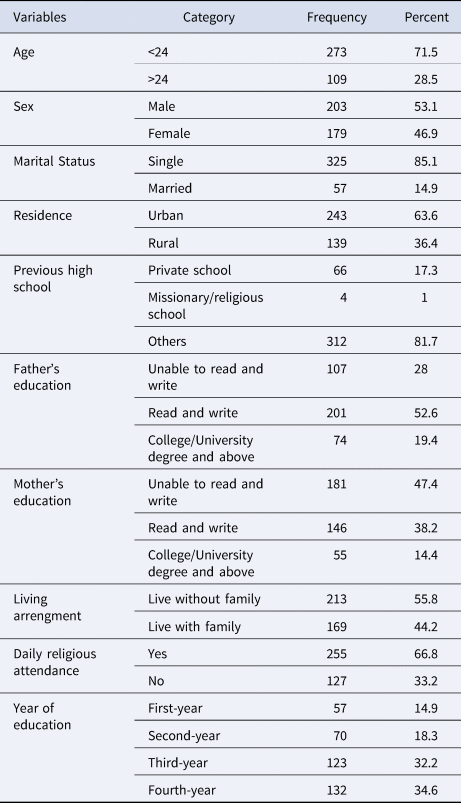
A total of 382 undergraduate students participated in this study, with a response rate of 91%. More than half (53.1%) of the respondents were male. Nearly three fourth (71.5%) of the respondents were under the age category of less than 24 years with the age range of between 18 and 34 years. Concerning their residence more than half (63.6%) of the respondents live in an urban area. Regarding their living arrangement, more than half (55.8%) of the respondents did not live with their families (Table 1).
Table 1. Socio-demographic characteristics of undergraduate students at the University of Gondar, Northwest Ethiopia, 2019 (n = 382)
Sexual experience of the respondents
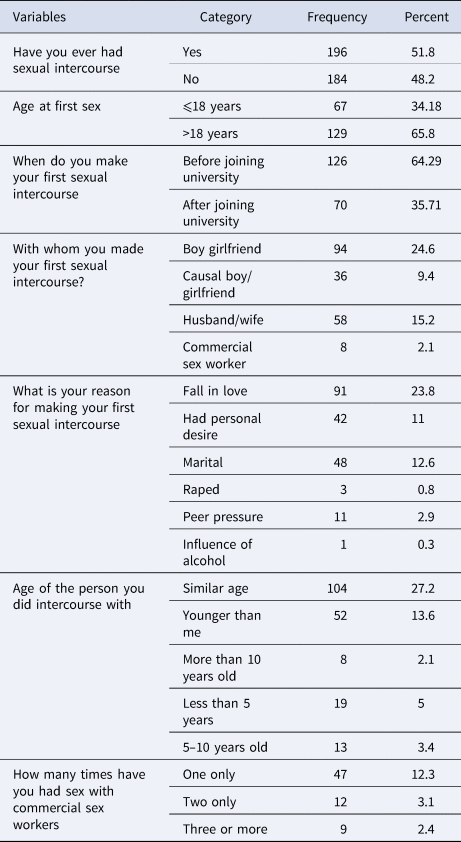
Of the total study participants majority, 196 (51.8%) reported having a history of previous sexual intercourse, among those 34.2% of them made their first sexual intercourse before 18 years old. The majority 126 (64.29%) of the study participants made their first sexual intercourse before joining the university, and 94 (24.6%) of them made their first sexual intercourse with their boy/girlfriends. About 68 (17.8%) of them had sex with a commercial sex worker (Table 2).
Table 2. Sexual experience of undergraduate students at the University of Gondar, Northwest Ethiopia, 2019 (n = 382)
Substance use and health risk behaviours of the students
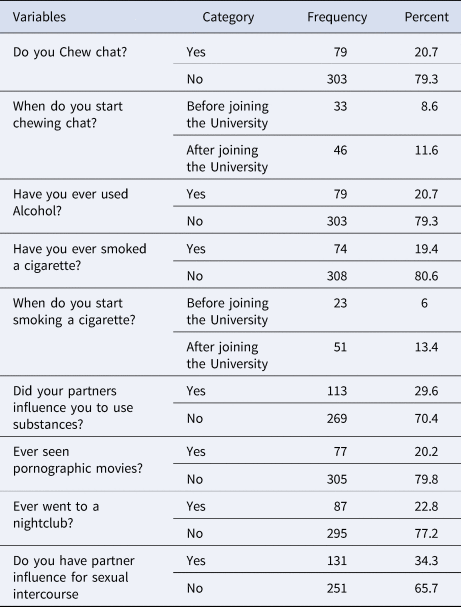
Among the total respondents, seventy-nine (20.7%) of them were alcohol users and seventy-nine (20.7%) of the students were chat chewers. Seventy-four (19.4%) of the students were cigarette smokers. One-fifth (20.6%) of the respondents had seen pornographic movies in their life. Eighty-seven (22.8%) of the students were going to the nightclub. One hundred thirty-one (34.3%) of the students had a partner who influence sexual intercourse (Table 3).
Table 3. Substance use and health risk behaviours of undergraduate students at University of Gondar, Northwest Ethiopia, 2019 (n = 382)
Prevalence of risky sexual behaviour
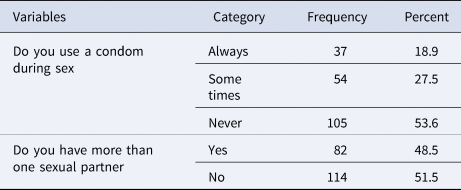
Among the total participants who had a history of sexual intercourse, more than half (53.6%) of the respondents were never used a condom during sex. Regarding their sexual partner, nearly half (48.5%) of the respondents had more than one sexual partner. The overall prevalence of RSB of undergraduate students of the University of Gondar was 44.0% with 95% CI (38.7–49.2%) (Table 4).
Table 4. Prevalence of RSB of undergraduate students at the University of Gondar, Northwest Ethiopia, 2019 (n = 196)
Factors associated with risky sexual behaviour
In bivariable logistic regression analysis, age, marital status, residence, mother's education, living arrangement, daily religious attendance, chew chat, drink alcohol, ever see pornography and having information were found to be significantly associated with RSB. Using multivariable logistic regression analysis, age, residence, living arrangement, daily religious attendance, drinking alcohol and having information were significantly associated with RSB. Those students in age group greater than 24 years were 2.12 times more likely to be engaged in RSB as compared to the younger age group of the students [adjusted odds ratio (AOR): 2.12; 95% CI (1.19–3.79)]. Those students who lived in urban areas were almost 2.14 times more likely to be engaged in RSB as compared to those students who lived in rural areas [AOR: 2.14; 95% CI (1.22–3.75)]. Students who lived without family or were not controlled by family members were more than 9.79 times more likely to be engaged in RSBs as compared to those students who lived with family members or controlled by family members [AOR: 9.79; 95% CI (5.34–17.9)]. Those study participants who reported to have alcohol are about nine times more likely to have RSB as compared with those study participants who reported not to have alcohol[AOR: 9.19; 95% CI (3.74–22.59)].
The odds of having RSB is about 43% less likely In study participants who have a daily religious attendance than study participants who have no daily religious attendance [AOR: 0.57; 95% CI (0.33–0.99)]. Moreover, those study participants who have information regarding reproductive health and sexually transmitted disease are about thre times more likely to have RSB as compared with respondents who have no information regarding RSB [AOR:3.05; 95% CI (1.00–9.27)] (Table 5).
Table 5. Bivariable and multivariable logistic regression analysis of factors associated with RSB among undergraduate students at the University of Gondar, Northwest Ethiopia, 2019 (n = 382)
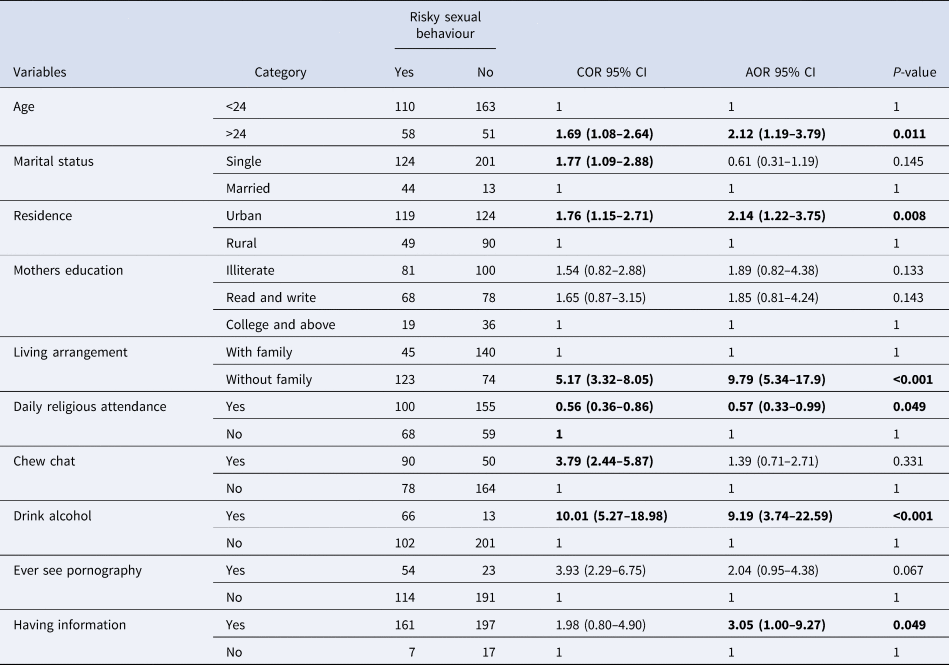
Note: Significant variables are provided in bold.
Discussion
The result of the current study revealed that the prevalence of RSB is 44.0%. It implies that RSB is a common health concern among undergraduate university students which needs special consideration from youth-friendly service givers, policymakers, university administrators and families. The finding of this study is in line with studies conducted in Jimma Ethiopia 43.5% [Reference Fentahun and Mamo19] Addis Ababa Ethiopia 43.1% [Reference Fetene and Mekonnen20], Wolyita Ethiopia 46.0% [Reference Yohannes, Gelibo and Tarekegn21], Lalibela Ethiopia 46.5% [Reference Desale, Argaw and Yalew22]. The prevalence of RSB in this study is higher than studies conducted in Arba Minch 22.4% [Reference Mersha23], Siri Lanka 12.4% [Reference Perera and Abeysena24]. The possible reason for this difference might be due to the difference in year of study, sample size and definition of RSB used in each study. However, it is lower than studies conducted in Portugal 64.0% [Reference Dias25], China 49.4% [Reference Li26]. The possible justification for this difference might be that due to the variation in socio-cultural difference. On the other hand, it might be due to the fear of becoming infected with sexually transmitted diseases like HIV. Meaning in developing countries the risk of exposing to STD is high compared with developed countries.
Among the determinant factors, the age of the participants was one of the factors significantly associated with RSB. Those students with ages greater than 24 years were about two times more likely to be engaged in RSB as compared to the younger age group of the students. This finding was supported by the study conducted in Addis Ababa, Ethiopia [Reference Fetene and Mekonnen20]. This might be due to the age group of students greater than 24 years who were commonly called sexually active and in the fire age group because their sexual desire increased as they became physically and physiologically matured.
This study also showed that place of residence was another determinant factor associated with sexual behaviour. Those students who lived in urban areas were almost two times more likely to be engaged in RSB as compared to those students who lived in rural areas. This finding was supported by other studies, which revealed that those study participants who had urban residency are more likely to engage in RSB [Reference González, Kadengye and Mayega27–Reference Zou30]. This might be due to that students from the urban area had access to mobile communication, online chatting, seeing pornography and sex film in the cinema or on the internet which easily initiated their sexual desire and engaged in RSB, but students from the rural area might be less exposed to sex initiating situations. This might also be due to there is a culture in rural Ethiopia, sex before marriage is morally not acceptable.
Another factor associated with RSB was living arrangements. Students who did not live with family were more than nine times more likely to be engaged in RSBs as compared to those students who lived with the family. This finding was in agreement with other studies conducted in different countries [Reference Tarkang29, Reference Negeri31, Reference Srahbzu and Tirfeneh32]. This might be due to students, who lived without family feeling free to have sexual contact with an opposite-sex partner, but those students who lived with family were under the control of their family and they did not get free time for sexual contact.
The result of this study revealed that alcohol consumption and RSB are significantly associated. The odd of engaging in RSB is nine times higher in respondents who consume alcohol than respondents who didn't consume alcohol. This finding is supported by studies conducted in different countries [Reference Mamo, Admasu and Berta4, Reference Fentahun and Mamo19, Reference Perera and Abeysena24, Reference Sun33, Reference Soboka and Kejela34]. The possible justification could be because having alcohol will cause intoxication which leads university students to have more sexual arousal to commit RSB.
The finding of this study also revealed daily religious attendance and engaging in RSB are inversely associated. Those students who reported to have daily religious attendance are about 43% less likely to engage in RSB as compared with university students who reported not to have daily religious attendance. This finding is in agreement with other studies [Reference Moore, Berkley-Patton and Hawes35, Reference Lafarga36]. The possible justification could be because those study participants who reported to have daily religious attendance might be more prone to follow religious commandments so that they might not have alcohol and other substances. Therefore, they might be less likely to engage in RSB.
Moreover, the study revealed that having information regarding reproductive health and sexually transmitted diseases is significantly associated with RSB. Study participants who have information regarding reproductive health and sexually transmitted disease are about three times more likely to have RSB as compared with respondents who have no information regarding reproductive health and sexually transmitted disease. Logically, it is expected to be less RSB with participants having information about reproductive health and RSB. But in our finding, participants having information were more likely to have RSB. It might be due to ignorance and limitation of the study design. Whether the act of RSB or information regarding RSB comes first is not identified. Furthermore, participants with RSB may seek more information after they engaged in RSB due to fear of its negative outcomes.
Conclusion
Nearly half of the respondents engaged in risky sexual activity. This prevalence is high and the students are at high risk for exposure to sexually transmitted diseases that need reproductive health intervention like counselling and discussion. Creating awareness for the students regarding reproductive health and the risk of sexually transmitted diseases is needed. In addition, giving special attention is required for students who use alcohol, who did not live with family, and who have urban residence.
Acknowledgements
The authors acknowledge the University of Gondar, data collectors, supervisors and study participants.
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Financial support
No funding was received for the conduction of the study or manuscript preparation.
Data availability statement
All data are available upon reasonable request.






 Open access
Open access