


INTRODUCTION
A novel H1N1 influenza A virus emerged in the United States in spring 2009, and rapidly became a global pandemic. While seasonal influenza typically affects the elderly and infants, the 2009 pandemic strain affected a broader population, with 45% of hospitalized cases aged ⩽18 years [Reference Jain1]. Children who are hospitalized as a result of seasonal influenza infection are likely to have an underlying medical condition, receive mechanical ventilation, and have neurological complications, resulting in extended hospital stays and increased hospital costs [Reference Jain1–Reference Placzek and Madoff5]. Despite the extensive geographical distribution of the 2009 pandemic strain, our knowledge is limited on how the H1N1 influenza A strain affected children who required hospitalization. Understanding the risks associated with disease severity in children will allow for better identification of patients at risk for adverse outcomes from influenza infection. We abstracted electronic medical records to identify clinical characteristics associated with adverse outcomes in documented paediatric H1N1 cases presenting to the emergency department (ED) at Texas Children's Hospital (TCH) in Houston during the 2009 influenza pandemic. The objective of our study was to identify clinical predictors of severity to aid clinicians in triaging paediatric patients during influenza epidemics.
METHODS
This retrospective medical record review study was approved by the Baylor College of Medicine Institutional Review Board and Ethics Committee and received a waiver of consent.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Study population
TCH is the largest free-standing paediatric hospital in Texas, with a 639-bed capacity, and 92 627 ED visits annually. Cases were identified by reviewing the Clinical Diagnostic Laboratory sample submission log for positive influenza A(HIN1) strain test results. Cases of influenza A(H1N1) pandemic virus [A(H1N1)pdm] were defined as patients aged 0–18 years who presented to TCH between 1 April 2009 and 30 June 2010, and who were diagnosed with laboratory-confirmed A(HIN1)pdm influenza infection. In order to evaluate the factors associated with severity of influenza illness, cases were classified as: non-hospitalized, hospitalized without intensive care unit (ICU) admission, and hospitalized with admission to the ICU. Non-hospitalized cases were patients who were discharged home directly from the ED in <24 h. Hospitalized cases were defined as those who were admitted for ⩾24 h but were not admitted to the ICU. ICU cases were defined as patients admitted to the ICU directly from the ED or during the course of hospitalization. Cases transferred from other healthcare organizations were excluded from this analysis due to incomplete records available for abstraction at the time of their acute clinical presentation.
Laboratory confirmation of cases
The decision to test a patient for influenza infection was made by the clinicians providing routine patient care. Respiratory secretions were collected by nasal wash for testing at the Clinical Diagnostic Laboratory. All samples were first extracted using the Qiasymphony platform (Qiagen, USA). For detection of the influenza A matrix gene, one of two different assays were used: from April 2009 to December of 2009 a real-time PCR (rtPCR) assay that was developed and validated at TCH utilizing the CDC rtPCR as the reference standard to detect the matrix gene of influenza A on the Roche Light Cycler 480 platform (Roche Diagnostics, USA); from December 2009 to June 2010 the Prodesse (now Hologic Gen-Probe, USA) rtPCR assay, ProFlu+, was used to detect the influenza A matrix gene. In order to accommodate the high volume of specimens, the ProFlu+ assay was validated using the ABI 7500 Real Time PCR System (Applied Biosciences, USA) and the QIAsymphony extraction platform (Qiagen, USA). While specificity and sensitivity were not known at the time of testing due to the rapid development of this new diagnostic, we feel confident that pandemic A(HIN1) strain was accurately detected compared to H3N2 provided that pandemic A(HIN1) was the predominantly circulating strain in both Texas and the United States [6, 7].
Data collection
Demographic and clinical information were abstracted from the patients' medical records using a standardized data collection form (see Supplementary material). Demographics, presenting symptoms, existing health conditions/comorbidities, disease complications/secondary infections, medications, and health outcomes were recorded. The charts of non-hospitalized patients were reviewed for additional ED visits within 1 week post-initial ED visit, to capture any possible further disease complications not noted in the initial ED chart. Three medical chart electronic systems (EPIC, On Base, Logician) were used due to the transition during that time from paper to electronic medical records at TCH. Using all three systems allowed us to capture paper and electronic medical records as well as any potentially misclassified records.
Definitions of specific clinical events are as follows: Dyspnoea was defined as increased respiratory rate based on the standard respiratory rate for age, and reported laboured breathing, with or without related cyanosis, or hypoxaemia (arterial oxygen saturation below 90%). Cardiovascular diseases included electrical abnormalities, physical/structural abnormalities and congenital heart disease. Immunosuppression was defined by receipt of immunosuppressive medications or chemotherapy. Lung disease was defined by a collective grouping of chronic lung diseases, including rare lung disorders. Seizures were defined as clinical seizures with or without evidence of encephalitis or meningitis, febrile seizures, and a pre-existing seizure disorder with increased frequency of seizures.
Statistical methods
The primary outcome of the study was to identify clinical predictors of severity on a three-level ordinal scale. Descriptive statistics were used to describe the three outcome groups (non-hospitalized, hospitalized, admitted to the ICU) and associated variables. Map Info software (Pitney Bowes, USA) was used to spatially analyse case distribution radiating outward from the hospital. An epidemic curve based on date of disease onset was created to temporally describe the timing of pandemic A(HIN1) cases seen at TCH. Proportional-odds ordinal logistic regression models were used to identify risk factors associated with adverse outcomes. Univariate models were calculated to identify factors associated with ICU hospitalization. Separate predictive multivariate models were constructed for symptoms and comorbidities. All risk factors on univariate analysis with P ⩽ 0·25 were included in multivariate analysis. A backwards step-wise elimination of the highest non-significant value method was used. Only those factors with P ⩽ 0·10 were considered significant in final multivariate models.
Multivariate models included race and insurance status to control for confounding. The Brant test was used to verify that the model met the assumption of proportional-odds regression and that the odds of disease severity increased consistently across risk groups. Goodness of fit was verified using Hosmer–Lemeshow test statistics on constrained binary logistic models. In order to evaluate the predictive value of identified covariates, receiver operating characteristic (ROC) plots were constructed on constrained binary logistic models. The ordinal regression model was assessed for its validity by comparing the three outcome groups in terms of length of hospital stay, time between symptom onset and presentation to the ED, use of medications, and presence of disease complications. All calculations were performed using Stata v. 13.1 software (StataCorp., USA).
RESULTS
From April 2009 to June 2010, 150 616 children presented to the TCH ED. Less than 1% (695/150 616) had confirmed A(HIN1)pdm influenza infection. The overall epidemic curve of disease peaked around week 38 (14–20 September 2009) (Fig. 1). Non-hospitalized cases peaked slightly before hospitalized and ICU cases. Distance from residence to the hospital increased significantly with disease severity (P < 0·001) (Fig. 2). Children lived an average of 18 miles, 28 miles, and 42 miles for non-hospitalized, hospitalized non-ICU, and ICU cases, respectively.

Fig. 1. Epidemic curve of 2009 A(HIN1)pdm influenza cases' date of onset, stratified by hospital admission status, April 2009–June 2010.

Fig. 2. Count of H1N1 paediatric cases per zip code attending Texas Children's Hospital from April 2009 to June 2010. The bold red cross represents the location of Texas Children's Hospital.
Figure 3 shows the demographic characteristics of the study population. Overall, 263 (38%) patients were hospitalized without being admitted to the ICU, and 116 (17%) were admitted to the ICU. Males were significantly more likely to be admitted to the hospital or ICU than females [P = 0·016, OR 1·42, 95% confidence interval (CI) 1·07–1·89]. Compared to non-Hispanic whites, children identified as minorities were less likely to be admitted to the hospital or ICU. Black race was associated with 0·54 times lower odds (P = 0·010, 95% CI 0·34–0·87) and Hispanic with 0·43 times lower odds (P < 0·001, 95% CI 0·28–0·64). Compared to children with private insurance, children with Texas Children's Health Plan (TCHP)/Medicaid [P = 0·004, odds ratio (OR) 0·63, 95% CI 0·46–0·86] or no insurance (P < 0·001, OR 0·21, 95% CI 0·11–0·35) were less likely to be admitted to the hospital or ICU. Because of the strength and interaction of these associations, we adjusted for race and insurance status in all multivariate models.

Fig. 3. Descriptive characteristics of the 2009 A(HIN1)pdm influenza paediatric cases at Texas Children's Hospital by hospital admission status. Texas Children's Health Plan (TCHP) is a type of insurance for children living in Harris County that qualify for Medicaid or Medicare, which allows for Harris County to directly pay providers within the Texas Children's healthcare network (http://www.texaschildrenshealthplan.org).
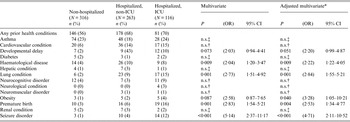
Presenting signs and symptoms were evaluated to develop predictive models for severity of disease, as shown in Table 1. Of the 11 signs and symptoms included in the multivariate model, three were statistically predictive of hospitalization. Patients who required hospitalization were more likely to present with dyspnoea (OR 5·82), tachycardia (OR 2·61), and fatigue (OR 1·96). Conversely, patients who exhibited chills (OR 0·44), congestion (OR 0·68), fever (OR 0·41), headache (OR 0·51), myalgia (0·44), or sore throat (0·72) were statistically less likely to be hospitalized or admitted to the ICU. Children who had a known influenza diagnosis at the initial emergency room evaluation (P < 0·001, OR 0·2, 95% CI 0·17–0·32) or had a reported sick contact (P = 0·003, OR 0·65, 95% CI 0·49–0·86) were less likely to be admitted to the hospital or ICU.
Table 1. Documented signs and symptoms at the time of presentation of patients with A(HIN1)pdm influenza by hospitalized status, multivariate and adjusted multivariate analysis

OR, Odds ratio; CI, confidence interval.
* Adjusted for insurance status and race.
† n.s., Not significant in multivariate analysis (P > 0·1).
‡ n.s., Not significant in univariate analysis (P > 0·25).
Children with one or more pre-existing health condition had 2·51 times greater odds (P < 0·001, 95% CI 1·81–3·42) of developing severe disease from influenza A(HIN1)pdm infection compared to those who had no comorbidities (Table 2). Following model fitting, six comorbidities were identified as significant predictors of disease severity (Table 2). Seizure disorders (OR 4·71), obesity (OR 3·28), chronic lung disease (OR 2·84), premature birth (OR 2·53), developmental delay (OR 2·20), and haematological diseases (OR 2·22) were all significantly associated with hospitalization. Of the 38 hospitalized and ICU-admitted children who had a history of premature birth, the average gestation was 30 weeks (range 22–36 weeks).
Table 2. Prior health conditions by hospitalized status, multivariate and adjusted multivariate analysis
OR, Odds ratio; CI, confidence interval.
* Adjusted for insurance status and race.
† n.s. Not significant in multivariate analysis (P > 0·1).
‡ n.s., Not significant in univariate analysis (P > 0·25).
We evaluated the model and found it to be appropriate based on the following fitness tests as described in the Methods section. Hosmer–Lemeshow test statistics on constrained binary logistic models corresponding to each level of outcome were non-significant for both symptom and comorbidity models (P > 0·35). The proportional-odds assumption was verified for these multivariate models using non-significant Brant tests (P > 0·35) and approximate likelihood ratio tests (P > 0·30). We evaluated the predictive ability of each of the multivariate models by generating ROC curves for constrained binary logistic models, and the area under curve (AUC) was calculated. For presenting systems, the AUC for the binary model corresponding to ICU vs. hospitalized and non-hospitalized cases was 80% while the model corresponding to ICU and hospitalized vs. non-hospitalized cases had an AUC of 74%. For pre-existing conditions, the AUC for the binary model corresponding to ICU vs. hospitalized and non-hospitalized cases was 65% while the model corresponding to ICU and hospitalized vs. non-hospitalized cases had an AUC of 61%.
In order to assess whether the ordinal outcome was an appropriate measure of adverse outcomes, we analysed hospital length of stay, prescription medications, and disease complications as proxies for disease severity. Patients admitted to the ICU had a median length of stay of 7 days [interquartile range (IQR) 3–16 days], which was significantly longer (Mann–Whitney P < 0·001) than those admitted to the hospital who had a median length of stay of 2 days (IQR 1–4 days). Likewise, ICU-admitted cases had a longer duration of symptom onset to ED presentation than children who were discharged the same day or were hospitalized without ICU admission (Mann–Whitney P < 0·001).
Oseltamivir prescription rates were prevalent in the entire population (78%). However, severe cases had increased odds of antiviral prescription (P = 0·004, OR 1·68, 95% CI 1·19–2·36). Antibiotic prescriptions were highly associated with disease severity (P < 0·001, OR 15·98, 95% CI 11·14–22·91) with prescription rates of 17% in non-hospitalized cases compared to 67% in hospitalized cases and 94% in cases admitted to the ICU. Corticosteroid use was also associated with a more adverse outcome (P < 0·001, OR 3·89, 95% CI 2·59–5·84), with rates of 8% in non-hospitalized cases compared to 15% and 35% in cases admitted to the hospital or ICU, respectively.
Disease complications and secondary infections were evaluated between the groups to understand health outcomes for future case management. As seen in Table 3, disease complications were highly associated with severity (P < 0·001), with the presence of complications corresponding to a >8 times odds of an adverse outcome. Of patients admitted to the ICU, 94% experienced complications, compared to 58% who were hospitalized but not admitted to the ICU, and 24% in those directly discharged home. Secondary S. aureus infection, central nervous system manifestations, pneumonia, acute respiratory distress, pneumothorax, sepsis, heart failure, pharyngitis, renal failure, otitis media, pleural effusion, and death were all statistically more (P < 0·05) likely to occur in cases admitted to the ICU or hospital. Pneumonia cases had the greatest association with hospitalization or admission to the ICU, with an odds ratio of 13·0 (95% CI 8·73–19·41). Central nervous system manifestations included seizures, encephalitis, meningitis, and parenchymal brain infarction. Seizures were the most prevalent manifestation, and experiencing seizures was statistically associated (P < 0·05) with having a prior diagnosis of a seizure disorder. Sepsis was only reported in hospitalized and ICU cases: viral sepsis (58%, 18/31), bacterial sepsis (39%, 12/31), and fungal sepsis (3%, 1/31).
Table 3. Disease complications of paediatric A(HIN1)pdm influenza cases by hospitalized status, univariate analysis

OR, Odds ratio; CI, confidence interval.
* Unable to calculate or unreliable OR or 95% CI due to zero count cells.
DISCUSSION
From April 2009 to June 2010, 696 children were treated at TCH for laboratory-confirmed influenza A(HIN1)pdm infection. Over half of these children were hospitalized or admitted to the ICU. Although the 2009 influenza pandemic has been perceived as a ‘mild’ pandemic, we have documented a substantial impact and morbidity of A(HIN1)pdm infection in children, including children with no previous underlying medical conditions. During large outbreaks, it is imperative that children are appropriately triaged to ensure resources are available to treat and manage the most severe cases. This study aimed to determine clinical factors predictive of disease severity in children with influenza in order to develop targeted interventions during future influenza epidemics.
Overall, our models were predictive of severity as indicated by statistical measures and their correlations with proxy clinical measures. The ordinal scale used in this study was associated with increasing probability of disease severity and complications. ROC curve analysis showed that presenting symptoms were better predictors of disease outcomes than comorbidities. This could be due to the relatively small number of patients in our sample presenting with each individual comorbidity; however, during a pandemic, patients without underlying comorbidities are likely to be affected, and our findings confirm that symptoms of lower respiratory tract disease are more indicative of severe influenza disease. Importantly, evidence of systemic disease and a diagnosis of ‘sepsis’ was common in children admitted to the ICU, which is indicative of the severity of A(HIN1)pdm infection, as most of the patients had viral sepsis, with some having complications due to secondary bacterial infection. In our patient population, an increased risk for severe influenza disease was documented in otherwise healthy children aged <5 years, in children with neurodevelopmental conditions, obesity, chronic lung disease and prematurity. Several of these risk factors, particularly prematurity, are being recognized after the pandemic.
A predictive model for improved triaging in the event of a future influenza pandemic is particularly important due to the potential unique characteristics of pandemics in children. One third of our population admitted to the ICU was healthy children with no prior health conditions. Healthy children admitted to the ICU had no statistical difference in disease severity and progression compared to their ICU-admitted counterparts with pre-existing conditions, including duration of ICU stay, oxygen requirement, use of mechanical ventilation, and use of extracorporeal membrane oxygenation. The only difference was that healthy ICU-admitted children were significantly younger (median age 4 years) than their counterparts with pre-existing comorbidities (median age 6 years). Considering that healthy children are likely to be affected by emerging influenza strains, it is important to consider their presenting symptoms and other risk factors such as young age and presence of underlying medical conditions.
Some historical and clinical characteristics might be helpful to better ascertain which patients should be monitored more closely due to high risk of complications. We found that cases not admitted to the hospital or ICU were statistically more likely to have a sick contact with known influenza diagnosis at the time of their initial evaluation. Therefore, it is possible that knowledge of A(HIN1)pdm influenza exposure likely influenced the caregiver's decision to seek early emergency care for their child of concern, even though the child's illness was not severe enough to warrant hospitalization. In addition, these patients were more likely to have traditional influenza-like illness symptoms, such as fever, myalgia, headache, and congestion with no evidence of lower respiratory tract involvement or prior health conditions, which made them good candidates for at-home care and disease management with antiviral treatment. Interestingly, non-hospitalized children were more likely to have fever and chills which could be indicators of early disease progression. Conversely, patients presenting with dyspnoea, debilitating fatigue, and tachycardia, all suggestive of lower respiratory tract or systemic disease, were more likely to have severe disease outcomes. Children with developmental delay, seizure disorders, notable obesity, haematological disorders, history of premature birth, and/or chronic lung diseases should be treated promptly and monitored closely due to risk of disease severity and complications.
Our findings of prior health conditions associated with hospital admission were consistent with the literature. A study in Great Britain reported that persons with chronic lung disease and obesity were at an increased risk for severe disease [Reference Singanayagam8]. While we found that children with an underlying lung disease had a twofold increase in risk for hospitalization, we also found obesity to be statistically associated after multivariate analysis. The importance of obesity was not widely recognized as a risk factor for influenza complications prior to the pandemic. However it is an important one in children, considering that obesity was likely underreported in the emergency room medical records, and that one third of children are reported to be obese in the United States [Reference Ogden9]. Future studies should aim at testing this correlation in children, with more precise body mass index measurements. Similar to our severity disease association in children with developmental delay, a New Zealand study found children with developmental delays had a tenfold increase in odds for having severe infection [Reference Dalziel10]. Interestingly, neurological manifestations were prominent in children infected with A(HIN1)pdm influenza, and seizures were more likely to occur in patients with a previous history of seizures [Reference Wilking11]. In our univariate analysis, we identified immunosuppressing conditions as associated with admission to the hospital but not to the ICU. We hypothesize this is because these children were admitted as a precautionary measure rather than due to an adverse outcome. This was corroborated with the fact that these children's length of stay and rate of complications was not higher, and therefore pre-existing immunosuppression was excluded from the multivariate analysis.
Limitations of this study are related to inherent limitations of retrospective data collection methods [Reference Gilbert12]. By using three electronic medical record systems at TCH and using trained health personnel, we feel confident in our interpretation of the records and results in our study. It is possible that those children presenting with more severe disease could have been more thoroughly assessed with regard to their prior medical history. We found that children with TCHP/Medicaid or no insurance were less likely to be admitted to the hospital or ICU. It is possible that these children are more likely to utilize emergency centre services as their source for primary care, compared to those with private insurance who would only use the hospital emergency centre for more severe disease. We were not able to collect enough information to analyse the influence of recent seasonal influenza and H1N1 influenza immunization histories on disease severity and outcome. National seasonal influenza vaccine coverage was 31·1% in children during the normal 2007–2008 season, but peaked at 43·7% during the 2009–2010 season [Reference Lu13, 14]. The influenza A(H1N1) 2009 monovalent vaccine became available in Houston starting in October 2009, and nationally 40·2% of children were vaccinated during the pandemic [14]. It is unknown if H1N1 influenza immunization rates were truly low (<1%) in our population as evidenced by the chart abstraction, or if they were not accurately documented in the medical chart. Finally, long-term follow up for the assessment of sequelae or resolution of complications was not possible in this study.
This study analysed risk factors associated with hospitalization and ICU admission of children with influenza A(HIN1)pdm infection. Younger children, those with clinical symptoms of lower respiratory tract disease involvement or systemic disease, and those with certain underlying medical conditions, had increased risk for ICU admission and complications of influenza. Children travelling from outlying areas of the metropolitan area were more likely to have severe cases than those closest to the ED. Healthy children without prior comorbidities accounted for one-third of our ICU-admitted patients, a unique characteristic of this pandemic influenza strain. We identified several clinical characteristics, particularly those related to systemic and pulmonary disease involvement, associated with severe disease that can be used for triaging case management in future influenza outbreaks in children.
SUPPLEMENTARY MATERIAL
For supplementary material accompanying this paper visit http://dx.doi.org/10.1017/S0950268815000114.
ACKNOWLEDGEMENTS
We thank Gloria Jackson for her help retrieving all the records for review. We also thank Ana Maria Gomez-Rubio and Ashley Wilking for their help with chart abstractions.
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
DECLARATION OF INTEREST
None.








