


INTRODUCTION
Enterohaemorrhagic Escherichia coli (EHEC) is transmitted to humans by food, drinking and swimming water, animal and environmental contact, or directly from person to person. Foodborne transmission is mostly associated with ground beef but outbreaks have also been associated with other forms of beef, fermented sausage, contaminated vegetables and fruits as well as unpasteurized dairy products [Reference Karch, Tarr and Bielaszewska1]. Transmission may also occur through contamination of soil and exposure in a rural environment [Reference O'Brien, Adak and Gilham2] or through direct contact with animals [Reference Crump3].
Large EHEC outbreaks have been reported from Japan [Reference Michino4], Australia [Reference Paton5], Argentina [Reference Gomez6], the United States [Reference Bell7], Canada [Reference Orr8] and Europe. In continental Europe sporadic cases and larger outbreaks are less frequent than in the United States and the United Kingdom [Reference Caprioli, Tozzi, Kaper and O'Brien9]. In Scandinavian countries EHEC infections were rare and mostly travel-associated or imported, until a Swedish outbreak in 1995–1996 with 110 cases of E. coli O157 infections in which the source was never traced [Reference Ziese10]. Four large outbreaks with 11–37 cases in which the source of infection was not identified and limited outbreaks associated with unpasteurized dairy products and animal contact have also been described [11]. In 1999 an outbreak with 37 cases among hospital staff was registered. The source of infection was probably lettuce [Reference Welinder-Olsson12]. Recently, an outbreak involving 120 cases was registered in southwestern Sweden in which contaminated lettuce was implicated as the source of infection [13]. Infections with E. coli O157 became notifiable by law in Sweden in 1996, and all other EHEC serotypes became notifiable in 2004.
Human EHEC infection [Reference Su and Brandt14] may lead to gastroenteritis with watery or bloody diarrhoea and, in severe cases, haemolytic uraemic syndrome (HUS) and mortality although infection may also be asymptomatic. Most clinical isolates of EHEC infections are E. coli O157:H7 which is more easily detected than other EHEC strains. This strain may be more pathogenic [Reference Gerber15] although this issue has been questioned [Reference Tarr, Gordon and Chandler16]. Production of Shiga toxin (Stx) by EHEC strains is associated with the development of haemorrhagic colitis [Reference O'Brien17] and HUS [Reference Karmali18] and bacterial production of Stx2 is associated with a worse clinical outcome than Stx1 [Reference Tarr, Gordon and Chandler16].
The aim of this study was to describe a large outbreak of E. coli O157 in southern Sweden traced to consumption of fermented sausage and to describe the microbiological and epidemiological investigation that led to identification of a specific outbreak-related E. coli O157:H7 strain as the cause of infection and thus prevented the occurrence of further infections. The sausage production processes leading to an increased risk of contamination are described.
METHODS
Case definition
A probable case of EHEC infection was defined as a person residing in or visiting the province of Skania in southern Sweden during the period of 15 September to 5 November 2002 with symptoms consistent with EHEC infection such as abdominal pains, and/or diarrhoea (watery or bloody) and/or HUS defined by the presence of thrombocytopaenia, haemolytic anaemia with fragmented red blood cells and acute renal failure. Individuals who had been abroad within the past 2 weeks were excluded. The first symptomatic member of a family found to be infected was considered the index case and additional household members who were infected were considered secondary cases. Close contacts were defined as household members and children at the same day-care centres as infected symptomatic children. An asymptomatic case was defined as a close contact of an index case with microbiological and epidemiological findings related to the EHEC outbreak. These individuals were included in the study because even asymptomatic close contacts of index cases, who are EHEC carriers, may promote the spread of infection. Outbreak-related cases were verified by microbiological and/or epidemiological findings as described below. A confirmed case was defined as an individual associated with a specific strain of E. coli O157:H7.
Outbreak description
During the period of 15 September to 5 November 2002, 39 cases of EHEC infections (38 symptomatic and one asymptomatic carrier/family member) occurred in Skania, in comparison to 5–10 cases per year in previous years. Cases had a median age of 14 years (range 2–75 years). Sixteen cases were male and 23 were female. Twelve cases developed HUS with a median age of 8·5 years (range 2–45 years), four were male and eight were female.
Of the 39 cases, seven cases of EHEC infection occurred during September in six different counties spread over Skania. During October, 26 cases were registered in a small geographic area covering three counties in northeastern Skania and during the same month another four cases were registered in the remainder of Skania. An additional two cases were registered in two counties in northeastern Skania at the beginning of November.
Microbiological investigation
The purpose of the investigation was to define if all cases were related to infection with one specific EHEC strain. All suspected primary cases and close contacts and a majority of secondary cases were subjected to faecal sampling. Faecal samples obtained within 2 weeks of development of symptoms in index cases were analysed by PCR for detection of stx1, stx2, eae (intimin), uidA (O157 specific) as described [Reference Svenungsson19], and/or cultured on sorbitol McConkey plates (SMAC) and further characterized by latex agglutination assays for E. coli O157 (Oxoid, Basingstoke, UK). When a strain of EHEC was identified in a faecal sample by one of these methods the strain was subtyped by pulsed-field gel electrophoresis (PFGE) [Reference Swaminathan20] in order to determine whether a specific strain of EHEC was the cause of the increased occurrence of infections. PFGE was performed, using restriction enzyme XbaI and a CHEF mapper XA system (Bio-Rad Laboratories, Hercules, CA, USA) on 1% agarose (run time 26 h, voltage 6 V/cm and linearly ramped pulse time 12·5–40 s).
Serum samples were examined by ELISA for detection of antibodies to EHEC lipopolysaccharides of serogroups O157 and O111 and E. coli-secreted protein B (EspB) as previously described [Reference Bitzan and Karch21, Reference Sjogren22].
Epidemiological investigation
An epidemiological investigation by interview was launched on 28 September 2002. At this point six individuals had developed clinical symptoms of EHEC infection and two of the six were children with HUS. The purpose of the investigation was to define if all cases were related to one source of infection or not, and if the source of infection could be traced and thus prevent further spread of infection. Since no increase of EHEC infections was documented in other parts of the country a local common source of infection was suspected.
Index cases were interviewed by health-care personnel from the Regional Centre for Communicable Disease and Prevention. Enrolment criteria for participation in the interview were geographical (first appearance of symptoms while residing in or visiting the province of Skania), clinical signs of EHEC infection as defined above during the time-period of 15 September to 25 October. Cases were interviewed with a questionnaire concerning gastrointestinal symptoms, contact with individuals with these symptoms, domestic and foreign travel, consumption of specific foods including brand names, acquisition of groceries, cooking practices, animal contacts, outdoor bathing, pets, contact with farms and birds, gardening, contact with sandboxes, visits to fairs and restaurants within 2 weeks of first appearance of symptoms. Interviews were held in the hospital for in-patients or by telephone for outpatients (one interview per family, 20 families). When a cluster of cases occurred in the middle of October an outbreak control team was established including representatives from the Swedish Institute for Infectious Disease Control in Stockholm.
A matched case-control study was performed. Three controls per case were selected from the Swedish population registry and matched by age, sex and geographic area. Controls were excluded if they had travelled abroad within the last 14 days or had gastrointestinal symptoms during the past month. Controls were interviewed by telephone with a shorter version of the questionnaire, in which all questions to which at least 80% of cases had responded negatively were excluded and, in addition to the general questions, more specific questions regarding consumption of specific food products and brands were posed.
Environmental investigation
The environmental investigation involved the Regional Centre for Communicable Disease Control, the local Department for Environment and Health Protection and the Bacteriology Department at the regional hospital. Food leftovers from the households of index cases were cultured. Samples were also obtained from a suspected local butcher including minced meat, sausage products, samples from walls and equipment. Fermented sausages, from the same butcher, for sale in stores, were analysed. All samples were analysed by culture (SMAC) and by immunomagnetic separation for E. coli O157 (Dynabeads anti-E. coli O157, Dynal, Oslo, Norway) as previously described [Reference Chapman, Wright and Siddons23]. Isolated E. coli O157 were further subject to PCR for detection of stx1, stx2, eae and fliC H7 and molecular subtyping by PFGE.
Cattle faecal samples were collected from 15 herds. Altogether 298 individual faecal samples and 15 composite manure samples were collected and analysed for E. coli O157 as pooled faecal samples. Faecal and manure samples were pre-enriched in buffered peptone water for 6–8 h at 37°C and analysed with Dynabeads anti-E. coli O157. Beads were spread on SMAC (Oxoid) supplemented with 0·05 mg/l of cefixime and 2·5 mg/l of potassium tellurite and suspected colonies confirmed by latex agglutination (Oxoid DR 622), biochemical typing with API 20E (bioMérieux, Marcy l'Etoile, France) and PCR for stx1, stx2, eae, enterohaemolysin (hlyA) and fliC H7 [Reference Paton and Paton24, Reference Gannon25]. Stx-producing strains were subtyped by PFGE.
Statistics
Results of interviews were entered into a database with Epi-Info version 6.04 (CDC, Atlanta, GA, USA). A matched analysis of results from interviews of cases and controls was performed as conditional logistic regression using SAS version 8.2 (SAS Institute Inc., Cary, NC, USA). Comparison of cases and controls with regard to sausage consumption was assayed by Fisher's exact test (GraphPad InStat version 3; San Diego, CA, USA). P⩽0·05 was considered significant.
RESULTS
Diagnosis of EHEC infection
Thirty-nine domestic cases of EHEC infection were identified in residents of (or visitors of) a defined geographic area, the province of Skania, during the investigated time period: 15 September to 5 November 2002. Faecal samples were available from 33 of these cases and were analysed by culture on SMAC and PCR. Twenty-four of these samples were positive for stx2 and eae and one of the strains was positive for both stx1 and stx2. Serum was available from an additional four patients. Table 1 summarizes the EHEC serogroups and shows that E. coli O157 was the predominant serogroup in 25 cases suggesting that this serogroup was involved in the outbreak. Eleven cases could not be microbiologically confirmed. These cases were close contacts with an individual in whom E. coli O157 was microbiologically confirmed in a faecal sample (n=6) or associated with the outbreak by epidemiological findings (n=5), as described below.
Table 1. Microbiological evidence and epidemiological association with EHEC infection in the 39 patients
EHEC, Enterohaemorrhagic Escherichia coli; HUS, haemolytic uraemic syndrome.
a In these cases the microbiological investigation was negative [faecal sample negative (n=6) or lacking (n=5)] but the person resided in or visited Skania during the defined time period and developed symptoms consistent with EHEC infection such as diarrhoea and/or HUS. The epidemiological investigation described in the text associated these individuals with the outbreak or with other individuals with microbiologically confirmed EHEC infection.
b Faecal samples were not available (n=1) or faecal PCR was negative (n=3), the serogroup of E. coli was determined by ELISA using serum for detection of anti-lipopolysaccharides.
c Faecal PCR result was positive for stx and eae but a bacterial strain was not isolated.
d Serum samples positive for E. coli O157 or E. coli O111 were also positive for EspB.
e One of these patients had a faecal sample positive for both stx1 and stx2.
f The son of this patient had a faecal sample positive for E. coli O157:H7.
g Household member.
PFGE analyses of faecal samples
Twenty-three faecal samples were positive for the E. coli O157 serogroup, all of these were analysed by PFGE. Fourteen cases showed a novel PFGE pattern that was termed smi-H21. Three cases showed a PFGE pattern termed smi-H22. The PFGE patterns for these strains and the other five patterns of faecal E. coli O157 strains are shown in Figure 1a. The 14 cases showing a novel PFGE pattern suggested that this specific bacterial clone was associated with the outbreak.

Fig. 1. PFGE patterns of E. coli O157 strains associated with sausage outbreak and sporadic cases. (a) The PFGE patterns of the sausage-related strain E. coli O157:H7 smi-H21 (n=14) and smi-H22 (n=3) and the other E. coli O157:H7 strains isolated during the investigated time period between 15 September and 5 November 2002. The arrow points to a specific band unique for the smi-H21 strain. (b) The PFGE pattern from the E. coli O157:H7 smi-H21 strain isolated from a sausage sample compared to a E. coli O157:H7 smi-H21 strain from a patient.
Epidemiological investigation, a case-control study
In the case-control study 20 cases and 60 controls were interviewed. The results of the case-control study (Table 2) indicated that consumption of boiled sausage, cold-smoked sausage, or meat balls might be involved with the outbreak. Several cases mentioned a specific brand of locally produced cold-smoked fermented sausage and interviews provided evidence that 10/20 of the cases reported consumption of this brand compared to 1/60 controls (P<0·0001).
Table 2. Association of consumption of specific foodstuffs with the outbreak calculated by odds ratio
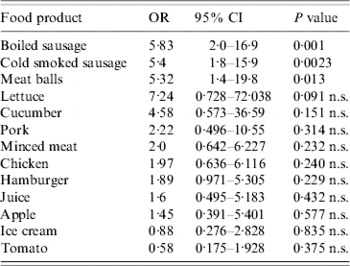
OR, Odds ratio; CI, confidence interval; n.s., non-significant.
PFGE analyses of the sausage strains
Investigation of sausage samples from households of infected individuals (n=6) showed that two of the samples were contaminated with E. coli O157:H7 which had an identical PFGE pattern to the smi-H21 strain isolated from patients as shown in Figure 1b. This strain produced Stx2.
Identification of sausage outbreak-related cases
The results of PFGE analyses of sausage strains implicated the smi-H21 strain with the outbreak. Of the 39 cases diagnosed with EHEC infection during the time period of this study 30 cases could be associated with the locally produced sausage. The description of all outbreak-related cases and how they were microbiologically and epidemiologically associated with sausage consumption is presented in Table 3. Fourteen of the cases had the sausage strain smi-H21 in faecal samples and an additional three of their household contacts were symptomatic. Two symptomatic cases with negative faecal samples were associated with the outbreak due to the presence of E. coli O157 smi-H21 contaminated sausage in their households. Three cases (two symptomatic, one asymptomatic, all in one household) had faecal samples positive for E. coli O157 smi-H22 and they had an additional two symptomatic household members with negative faecal samples. Four of these five household members had consumed the sausage. In addition three cases of HUS (of which two had positive E. coli O157 serology) and three of their symptomatic household contacts were presumed to be associated with the sausage outbreak based on self-reported sausage consumption.
Table 3. Characteristics of sausage outbreak-related cases

a The 30 cases lived in 17 households. Association to the sausage-related outbreak was obtained by presence of the implicated E. coli O157:H7 smi-H21 bacterial strain in a faecal sample or ingestion of the sausage and household proximity or more than one of these parameters. Of the total 30 cases 14 had a microbiological connection (faecal smi-H21 isolation) to the sausage outbreak.
b The smi-H22 strain was not isolated from the sausage but was found in faecal isolates (n=3) from one household (with four out of five symptomatic family members) in which the sausage was consumed.
c Analyses by ELISA for O157 lipopolysaccharide and EspB antibodies.
d Sausage was consumed in 15 out of 17 households with infected individuals and the smi-H21 strain isolated from sausage obtained from two of these households.
e Faecal samples were PCR positive in 17 cases. PCR was negative (n=9) or lacking (n=4) in 13 cases but three of these cases had a positive serology.
f All of these cases had HUS and had consumed the sausage.
g These four individuals did not consume the sausage but were associated with the outbreak by faecal samples positive for the smi-H21 strain (n=3) or smi-H22 (n=1).
Of the original 20 cases that participated in the case-control study presented in Table 2, 12 cases were associated with the sausage outbreak (seven of these had smi-H21 in faecal samples). The remaining eight cases, who had participated in the case-control study, and one of their symptomatic household members, who presented with EHEC infection during the same time period, account for the nine sporadic cases who were not associated with the outbreak.
Implications of the epidemiological and environmental investigation and the course of events
The course of the outbreak is described in Figure 2. The first three cases of E. coli O157:H7 with a faecal isolate identical to that found in the sausage developed symptoms on 29 September as well as 3 and 10 October 2002 but due to patient delay (the first patient sought medical care on 18 October) and initial negative faecal cultures, positive culture results from these patients were first obtained between 15 October and 4 November.
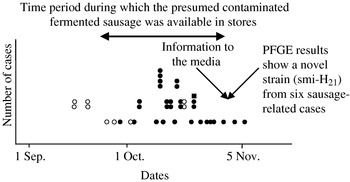
Fig. 2. Time distribution of EHEC cases in Skania in autumn 2002 in relation to sausage production and information to the local media. This figure shows the time period when the sausage outbreak-related cases were registered in relation to the period when the locally produced fermented sausage was available in the stores. The first sausage-related case developed symptoms on 29 September but did not seek medical care until 18 of October, which delayed the start of the investigation. The following two cases developed symptoms on 3 and 10 of October respectively. The first positive results from faecal cultures were obtained on 15 October and PFGE results were available on 26 October. The last sausage-related case occurred on 5 November, 6 days after the sausage had been removed from stores (30 October) and information was publicized by the local media (31 October). •, Sausage-related cases; ○, sporadic cases; ■, asymptomatic cases.
The first PFGE results demonstrating the E. coli O157 smi-H21 strain isolated from two affected individuals were available on 26 October. The results of the case-control study, available on 29 October 2002, implicated a specific locally produced, fermented cold-smoked sausage in the outbreak. On 30 October 2002 the environmental and health protection authorities performed an inspection of the suspected local butcher's premises. Manufacturing was closed down for production during a 2-week period while the investigation proceeded. All retailers (n=40) were contacted and the remaining sausage products were removed from the stores. The information implicating the sausage with the outbreak was reported in the local media on 31 October 2002.
On 1 November it became apparent that the smi-H21 strain was involved with the outbreak as PFGE results from six individuals showed an identical pattern and these cases had reported sausage consumption, the PFGE results for the remaining sausage outbreak-related cases were available between 6 November and 4 December 2002. No new cases of EHEC infection occurred after 5 November. The results of PFGE analysis of sausage samples from infected individuals were available on 7 and 14 November.
Investigation of samples from walls (n=2), equipment (n=8), minced meat (n=1) and packaged sausage (n=3) from the butcher's premises were negative for E. coli O157:H7. Samples of the sausage from stores (n=7) were found to be negative for E. coli O157:H7 by 11 November. Early in the investigation samples from minced meat (n=1) and beef (n=1) were also taken from households of infected individuals and found to be negative for E. coli O157:H7.
The smi-H22 strain was not isolated from the sausage but found in faecal samples (n=3) from one family in which four out of five household members consumed the sausage. These PFGE results were available on 26 October, 1 and 9 November 2002. The smi-H21 strain was not isolated in these faecal samples. This suggests that the sausage may also have been contaminated with the smi-H22 strain.
The known EHEC incubation time of about 10 days (plus an additional 10 days to cover for the possibility of unknown cases) suggested that sausage batches delivered to stores between 9 September and 1 October had the greatest likelihood of being contaminated. An effort was made to trace the beef that had been used for production of these batches. As the sausage production process lasted 2 weeks the beef that was delivered to the butcher's between 28 August and 18 September was able to be traced. Fifteen out of 17 herds, that had animals to sample, and from which the beef in the contaminated sausages could have originated, were investigated by collection of faecal and manure samples for analysis of E. coli O157. Five of the herds were positive for E. coli O157. From three out of five herds a total of nine Stx2-producing strains with PFGE patterns differing from the outbreak-related strains smi-H21 and smi-H22 (data not shown) were identified. The remaining strains identified from the two other herds were stx1 or both stx1 and stx2 producing.
In addition to beef, the cold fermented smoked sausage contained pork, potatoes, spices and a starter culture. These ingredients were not investigated.
Aspects of sausage production which may contribute to contamination with E. coli O157:H7
The sausage contained raw meat from beef including bovine diaphragm. The meat was pretreated with a 2·5–3% nitrite/salt mixture for 2 days at 2–4°C and then spices and starter culture were added. The starter culture contains lactic acid-producing bacteria, added to lower the pH in the batter, and was added freeze-dried in a dormant state. The sausage was fermented and dried first without smoke for 1 day at 28°C and then fermented and smoked by addition of smoke aroma substances, which have a minimal drying effect, every third hour for ~1 h for 5–7 days at 26°C. After this period the pH was ~4·5. This step was followed by curing at 2–4°C for ~1 week before the sausage was vacuum-packaged and distributed to stores to be kept refrigerated.
Specific aspects of preparation that may contribute to EHEC contamination were:
(1) Lack of heat-treatment.
(2) Addition of starter culture in a dormant state, which delayed the start of fermentation allowing an initial EHEC proliferation in the batter.
(3) A short curing period; E. coli O157:H7 is known to be acid-resistant and to survive a short curing process [Reference Duffy, Grau and Vanderlinde26].
Revised recommendations for sausage preparation as the result of this outbreak
Following this outbreak the Swedish National Food Administration developed a risk profile on cold-smoked, non-heat-treated fermented meat products as a source of EHEC infections. The recommendations are shown in Table 4 [27].
Table 4. Revised recommendations for sausage preparation
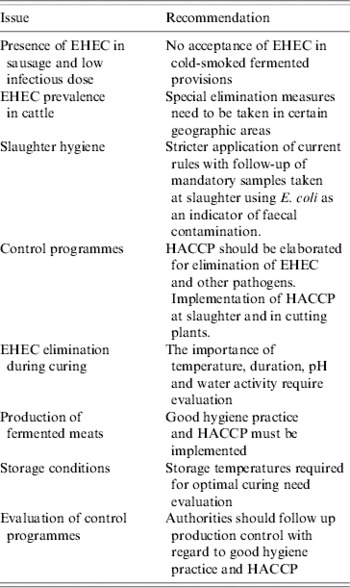
EHEC, Enterohaemorrhagic Escherichia coli; HACCP, hazard analysis critical control programmes.
Clinical characteristics of sausage related cases
Sausage-related cases (n=30) exhibited first appearance of symptoms between 29 September and 5 November 2002 and were concentrated to three counties in northeastern Skania (Fig. 3). The median age for sausage-related cases was 19 years (range 2–75 years) and 14 cases were aged <10 years. Sixteen (53%) were female. One case was asymptomatic, 29 cases had diarrhoea of which 16 cases had bloody diarrhoea. Thirteen patients (43%) were hospitalized. HUS developed in nine cases (30%) of which four required dialysis. There were no fatalities but two patients developed severe neurological complications.
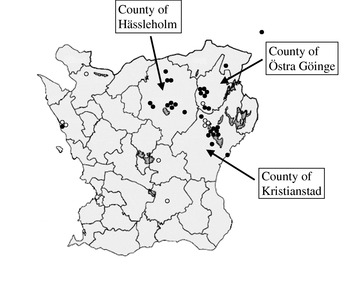
Fig. 3. Geographical distribution of sausage-related and sporadic EHEC cases in Skania in autumn 2002. The sausage-related cases were geographically concentrated in three counties in northeastern Skania. •, Sausage-related cases; ○, sporadic cases.
DISCUSSION
In this study we describe an outbreak of EHEC infection in southern Sweden and the epidemiological investigation and bacteriological results that identified the source of infection as a locally produced, cold-smoked non-heat-treated fermented sausage. The outbreak was rapidly contained as a result of an investigation involving numerous authorities (The Regional Centre for Communicable Disease Control and Prevention, The Swedish Institute for Infectious Disease Control, The Swedish Board of Agriculture, The National Veterinary Institute) and the case-control study conclusively indicated the implication of the sausage. PFGE analysis showed a novel strain termed smi-H21 in 14 faecal samples from sausage- related cases and in two out of six samples of locally produced sausage obtained from households of infected individuals. Six days after removal of the sausage from retailers and information to the public via the local media no further cases occurred suggesting that this was the sole source of infection during this outbreak. This is the first time that the source of infection in a larger foodborne EHEC outbreak has been identified in Sweden. Specific sausage curing procedures, which contribute to food contamination, are discussed below.
Cattle are the main EHEC reservoir [Reference Wells28] but although EHEC is considered a zoonotic disease most carriers do not develop symptoms [Reference Wells28]. Prevalence studies among cattle herds in Europe have shown the presence of E. coli O157 in up to 13% of herds and in Sweden up to 9%. In southern Sweden the prevalence is up to 23% of herds [Reference Eriksson29]. Measures aimed at identification and destruction of E. coli O157-infected farm animals have not proved logistically feasible. Furthermore, other, not so easily detectable, EHEC strains would persist. Certain precautions can be taken to reduce E. coli O157 on farms, but more importantly, strict methods concerning slaughter hygiene and sausage production need to be applied. E. coli O157 is not always completely eradicated during curing of cold-smoked dry-fermented sausage [Reference Tilden30]. The risk of human infection after consumption of non-heat-treated fermented meat products should therefore not be ignored.
In the current outbreak several steps in sausage production were suboptimal with regard to EHEC eradication. The most likely specific production aspects which enabled survival of EHEC, thereby causing the outbreak, were lack of heat treatment, a slow start of fermentation due to the addition of a dormant starter culture allowing E. coli O157 to proliferate in the batter during the initial phase of fermentation, followed by a too short curing process at 2–4°C instead of at room temperature. In the epidemiological investigation a bovine source of E. coli O157 was considered the most probable although this was never confirmed. Irrespective of the original source of contamination the suboptimal production procedure described above allowed possible contamination of the batter to persist in the final product. The fact that the infectious dose of E. coli O157:H7 is extremely low (<50 c.f.u.) [Reference Tilden30] suggests that bacterial survival in the batter is sufficient to cause human infection, even without proliferation.
The importance of the presence of bovine diaphragm in the batter is unclear [Reference Nyeleti31]. The Swedish Meat Industry Association has recommended that diaphragm not be used in non-heat-treated meat products due to possible risk of cross-contamination during slaughter, although this issue is unresolved.
Since most cases of EHEC infections are sporadic or occur in small clusters [Reference Karmali18] and detection and prevalence studies of EHEC in shortly ripened raw sausages in Dessau, Germany [Reference Timm32] have shown that 8·8% of investigated sausages (n=158) were contaminated with Stx-producing E. coli (some identical to clinical isolates), there may be a large number of EHEC/HUS cases associated with dry-fermented sausages in which the source is not traced. This is supported by results from the epidemiological investigation of the salami-linked Canadian E. coli O157:H7 outbreak in 1999 [Reference MacDonald33] in which only nine out of 43 leftover household samples of infected individuals were E. coli O157:H7 positive. In the same investigation salami samples were subsampled by the company before sale and no E. coli O157:H7 was detected, however, after the product was exported to the United States and re-tested due to the Canadian outbreak it was found to be positive for E. coli O157:H7.
Human EHEC infections associated with consumption of fermented meat products are not uncommon. This is the seventh outbreak reported during the period 1996–2006 as presented in Table 5 [Reference Paton5, 30, 33–36]. Previous studies have partially addressed production processes in trying to understand the cause of sausage contamination and found association with raw meat contamination, shortened drying periods and inadequate pH calibration. To assure food safety, several countries (United States, Australia, Canada) have enforced control programmes with predictive modelling techniques to predict the survival and growth of different pathogens in food products [Reference Reed37–39]. Since 1996 the US Department of Agriculture requires salami producers to follow one of five safety options aimed at achieving up to a 5-log kill (decrease the amount of bacteria with 105 c.f.u./g) [Reference Reed37].
Table 5. Reported outbreaks of EHEC infections associated with fermented sausage
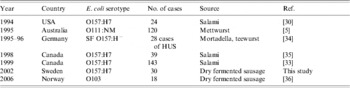
EHEC, Enterohaemorrhagic Escherichia coli; HUS, haemolytic uraemic syndrome; SF, sorbitol fermenting; NM, non-motile.
In conclusion, we describe an outbreak of E. coli O157:H7 associated with consumption of cold-smoked, non-heat-treated, fermented sausage and the microbiological and epidemiological investigation that identified the source of infection. We propose that in Sweden and Europe non-heat-treated fermented products containing beef may cause a background level of EHEC infections which are seldom traced due to the low infectious dose needed for human infection, as previously proposed in a Canadian outbreak [Reference MacDonald33]. We suggest that sausage preparation by fermentation and curing needs to be combined with an efficient control programme to ascertain that possible contamination of the raw batter with EHEC bacteria is eliminated during the processing method. If this cannot be achieved this kind of meat product is unsuitable for consumption, especially for young children susceptible to developing HUS. Public awareness is low in this matter, which in terms of food safety needs to be discussed in a forum where experts in food microbiology and clinicians and epidemiologists can meet. There is no specific treatment available for HUS. For this reason preventive work and food production regulations are essential for decreasing morbidity and mortality in EHEC infections.
ACKNOWLEDGEMENTS
The authors thank Anna Törner for statistical assistance, Yvonne Andersson for epidemiological evaluation and Margareta Ramberg and Ingela Hedenström for PFGE analyses, all from the Swedish Institute for Infectious Disease Control, Stockholm. This study was supported by grants from the Swedish Research Council (06X-14008), Swedish Renal Foundation, Anna-Lisa and Sven-Eric Lundgren Foundation for Medical Research, Maggie Stephens Foundation, Greta and Johan Kock Foundation, Crafoord Foundation, Inga and John Hains Foundation, Alfred Österlund Foundation, Crown Princess Lovisa's Sociey for Child Care, Thelma Zoegas Foundation, Sven Jerring Foundation, the Swedish Society of Nephrology, Åke Wiberg Foundation, Magnus Bergvalls Foundation and the Blood and Defence Network at Lund University (all to D.K.).
DECLARATION OF INTEREST
None.








