The SARS-COV-2 virus remains a major threat all over the world including Iraqi Kurdistan. As at February 25, 2022, there were 2298164 confirmed COVID-19 cases and 24931 death cases recorded in Iraq. 1
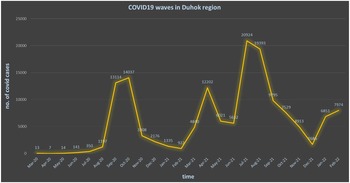
The increasing trends of COVID-19 in the 2 neighboring countries, Iran and Turkey, have had alarming effects on Iraqi Kurdistan. The first cases were reported in Iraq and Iraqi Kurdistan on February 24, 2020 and March 1, 2020 respectively. Reference Merza, Haleem Al Mezori and Mohammed2,Reference Merza, Aswad and Sulaiman3 This letter is a brief retrospective review of COVID-19 waves in Duhok from March 1, 2020 until February 24, 2022 (24 months). Iraqi Kurdistan was exposed to 3 COVID-19 waves: The first wave from March to December 2020, the second wave from January to June 2021, and the third 1 from July to December 2021 (Figure 1). 4 The predominant variants of concern (VOC) in the first 2 waves were Alpha and Beta variants; Reference Al-Rashedi, Alburkat and Hadi5 whereas the dominant variant in the third was the Delta strain. 6 Overall, in Iraq, the death rates in the first, second, and third waves were 2.15%, 0.58% and 0.92% respectively. 1 The Delta variant was much more severe, however, death rates in the third wave were lower than those of the first wave. Reference Ong, Chiew and Ang7 This was due to the lack of experience in the management of COVID-19 cases and inadequate prepared health services for coping with the pandemic in the first wave.

Figure 1. COVID-19 waves in Duhok region.
Currently, there is a marked decline in the rates of COVID-19 cases in Kurdistan hospitals, however there is an increase in number, regarding mild and moderate cases that do not need hospitalization, and a death rate of 0.55%. 1 This coincides with the start of the fourth wave in Iraqi Kurdistan along with the Omicron variant that we are facing now. At the beginning of January 2022, the first 5 cases of the Omicron variant were reported from a family in Duhok after 1 of its members returned from abroad. 6 Moreover, the new strain mainly emerged throughout the arrival of many Kurdish citizens that spent time in Turkey for vacation. Such risky groups circulate the virus in the community particularly to vulnerable people who have not been vaccinated or ones that do not follow preventive measures e.g., wearing masks and practicing social distancing.
This variant is highly transmissible with a greater possibility to infect vaccinated and previously infected people than other variants. Reference Lippi, Mattiuzzi and Henry8 Therefore, it was thought that the magnitude of this new wave would be different from previous ones. As a result, this variant would spread swiftly to peak and decline rapidly. In agreement with our expectations, for the past few months, we found a high number of Omicron patients among non-infected, previously infected, and vaccinated people, majority with a mild disease, making a quick and full recovery, and not demanding hospitalization. The rate of Omicron infected cases relatively did not depend on whether the individual was infected, not infected, or vaccinated before. However, it is more severe among those who have not been infected previously, particularly elderly individuals with comorbidities. Contrary to the reported numbers of previous waves in Duhok by the health authorities, the numbers of Omicron infections are much higher than the actual reported data. This is explained by its milder presentation which led to a lot of people not seeking medical care. Furthermore, recently, the wide availability of COVID-19 rapid antigen tests in drug stores and its cheap cost have a negative impact on the actual reported numbers by official authorities in Kurdistan. 9
A main factor that causes the spread of this contagious virus is school attendance. Reference Project10 Students below the age of 16 are excluded from the vaccination program in Kurdistan region; such vulnerable groups do not strictly follow Covid-19 preventive measures, which plays a major vehicle in the transmission of the virus in the community. To contain this challenge, preventive measures should be revised; reducing the vaccination age requirement to children aged 5 and above, and encouraging a booster vaccination dose for everyone aged 16 and older, 11 not as the current regulations of Iraq. 12 It is important to implement and ensure wearing of masks in indoor public areas, and to practice effective social distancing.
In conclusion, the COVID-19 universal vaccination program is highly indicated with encouraging booster doses. Strict implementation of preventive measures is an essential priority.