



Disaster is defined by the Asian Disaster Reduction Center as “a serious disruption of the functioning of society, causing widespread human, material, or environmental losses that exceed the ability of affected society to cope using only its resources.”1 They are most often characterized by being unexpected, unpredictable, uncertain, and unplanned. The increase in population, resource scarcity, and escalating conflicts has increased both man-made and natural disasters around the world.Reference Mahdi, Jafri and Allana2 As the global effects of climate change are felt more intensively, so too are the human and economic consequences of catastrophic disaster events.Reference Jones, Guha-Sapir and Tubeuf3 Every year, millions of people across the world are being affected by floods, landslides, cyclones, hurricanes, tornados, tsunamis, volcanic eruptions, earthquakes, wildfires, or human-made disasters. In the past 10 years, 83% of all disasters triggered by natural hazards were caused by extreme weather and climate-related events.4 Asia has suffered the highest number of disaster events. In total, there were 3068 disasters occurring in Asia from 2000-2019. China reported the highest number of disaster events (577 events).Reference Munasinghe, O’Reilly and Cameron5
A disaster is not just a single event but has 3 phases: pre-incident, incident, and post-incident. To decrease the impact of the disaster throughout its different phases, numerous nursing activities are required, including prevention or mitigation, preparedness, response, recovery, and reconstruction or rehabilitation.Reference Tzeng, Feng and Cheng6 Based on the International Strategy for Disaster Reduction (UNISDR 2011), preparedness is “the knowledge and capacities developed by governments, professional response and recovery organizations, communities and individuals to effectively anticipate, respond to, and recover from, the impacts of likely, imminent or current hazard events or conditions.”7 Hospitals are the basic infrastructure for disaster response. While they themselves are exposed to disasters, they also play an important role during the disaster response period.Reference Azarmi, Sharififar and Pishgooie8 A lack of preparedness was a major contributor to the struggles experienced by health care facilities around the world. Items such as personal protective equipment (PPE) for health care workers, hospital equipment, sanitizing supplies, toilet paper, and water were in short supply. These deficiencies were exposed by COVID-19 and have prompted health care organizations around the world to invent new essential plans for pandemic preparedness.Reference Kaye, Okeagu and Pham9 There is considerable evidence that preparedness for disasters in front line and non-front line hospitals is sub-optimal.Reference Biswas, Bahouth and Solomonov10‒Reference Goniewicz, Goniewicz and Włoszczak-Szubzda12 Most felt “not really” prepared or “unsure” about their preparedness to respond to a disaster.
Because disaster strikes without warning, all health care providers, especially nurses, must be prepared with appropriate skills and resources for disaster procedures and management during the 3phases of disaster.Reference Hugelius and Adolfsson13 The International Council of Nurses (ICN) emphasizes that disaster preparedness and response should be a part of nurses’ knowledge and skills, making nurses’ training in disaster management a globally agreed upon requirement (ICN, 2006).Reference Koca and Arkan14 Nurses are usually the first health professionals to meet patients during a disaster event. There is a formal global consensus that nurses require some knowledge of disaster management, leading to the development of the disaster nursing concept that stresses the need to improve nurses’ competencies in such situations.Reference Kalanlar15
Rural communities are heavily impacted by natural disasters and have different health care needs than urban communities.Reference Chan, Man and Lam16 In large and high-level cities in China like Shanghai, the disaster preparedness is comprehensive and extensive, which can also be described as broad and refined. With the scientific layout and establishment of emergency medical rescue base, training base, major infectious disease prevention and control base and nuclear treatment base, an emergency medical rescue system based in Shanghai that can serve all parts of the country has basically formed. Nevertheless, in Chinese small cities such as many of those in Henan Province with mountainous areas accounting for 47% of the total area of the province and spanning the 4 major river basins of the Hai River, Yellow River, Yangtze River, and Huai River, are influenced by complex weather systems. Due to the impact of rainfall, underlying surface environment and human activities, flash floods occur frequently in Henan Province, which also leads to frequent gas and roof accidents in this coal producing province. An extremely heavy rainstorm disaster happened on July 20, 2021 in Zhengzhou, Henan Province and caused a total of 14 786 million people in 150 counties (cities and districts) to be affected; 398 people died and disappeared due to the disaster. The cross-country marathon held in Baiyin, Gansu Province resulted in 21 deaths and 8 injuries for encountering extreme weather. Therefore, it’s particularly necessary for these places to improve certain capacities of disaster preparedness in response to natural disasters. Disasters magnify and more fully expose these health care disparities.Reference Cornelius, Char and Doyle17 Regarding the disaster preparedness of nurses, research in China mainly focuses on emergency departments and emergency rescue teams in tertiary hospitals, with very little concern about survey data on disaster preparedness of nurses in county-level hospitals. When serious disasters occur, whether they be natural disasters or large-scale epidemics, they tend to have more serious impacts in small cities with relatively poorer disaster preparedness. The city of Yongcheng in Henan Province, where the author works, is in the easternmost part of Henan Province, with a population of 1.68 million and a total area of 2020 square kilometers. It is rich in mineral resources. This study focuses on 4 hospitals in Yongcheng, Henan Province, 2 of which are tertiary hospitals and serve as Yongcheng’s main medical care and emergency centers. The other 2 are secondary first-class hospitals and are affiliated with a group. There is no medical college in Yongcheng. The aim is to understand the current status of disaster preparedness and influencing factors among nurses in county-level hospitals in China. It is hoped that through data analysis and dissection of the local actual situation, references for the cultivation of qualified nursing talent teams for disaster rescue in county-level hospitals can be provided to explore strategies for improving disaster nursing in small cities in China.
Objectives
The aim of this study was to understand the current status and influencing factors of disaster preparedness among nurses in non-first-tier (inland) cities, explore strategies for improving disaster nursing in small cities in China and provide a reference basis for the development of training programs for the disaster rescue nursing workforce.
Methods
Design and Participants
A cross-sectional research design was used. Nursing personnel from 4 comprehensive hospitals at or above the second level in Yongcheng were selected from 0:00 to 24:00 on April 14, 2023.
Participant Recruitment
Inclusion criteria: 1. Nurses who have obtained a nurse qualification certificate and have worked in the unit for at least 1 year. 2. Nurses who agree to participate in this study.
Instrument Development (Validity and Reliability)
Survery instrument
Demographics
A self-designed questionnaire for general information was used, which included gender, age, current education background, years of work experience, professional title, disaster relief participation experience, disaster training participation, and other survey items.
Disaster Preparedness Evaluation Tool(DPET)
DPETReference Tichy, Bond and Beckstrand18 chosen in this research is the scale for nurses’ disaster preparedness that was first created by Tichy and Bond, introduced into Jordan by AI Khalaileh in 2010,Reference Al Khalaileh, Bond and Beckstrand19 accepted for localization and revision, and was later Sinicized by Li Zhen in 2013. This questionnaire includes with a total of 45 survey entries. The scale ranges from strongly disagree to strongly agree, with scores ranging from 1-6 and a total score of 45-270. Cronbach’s alpha of this scale is 0.91 in China, which has good reliability in statistics.
Data Collection
Questionnaires were distributed by researchers on site to various departments, and the nurses in the department completed them within the specified time of 20-30 minutes. After that, questionnaires were collected on site.
Data Analysis
SPSS 25.0 data analysis method is adopted. The enumeration data is expressed in frequency and percentage. Measurement data is represented by “mean ± standard deviation.” T test is used for comparison between 2 groups, and analysis of variance is used for comparison between multiple groups. The influencing factors are analyzed using multiple linear regression analysis. P < 0.05 indicates that the difference is statistically significant.
Ethical Approval
The Ethics Committee of Shanghai East Hospital approved the study. All participants were provided a description of the study and informed that participation was voluntary and anonymity assured.
Results
Demographic and work-related characteristics are summarized in Table 1.
Table 1. Demographic and work-related characteristics of nurses (n = 784)
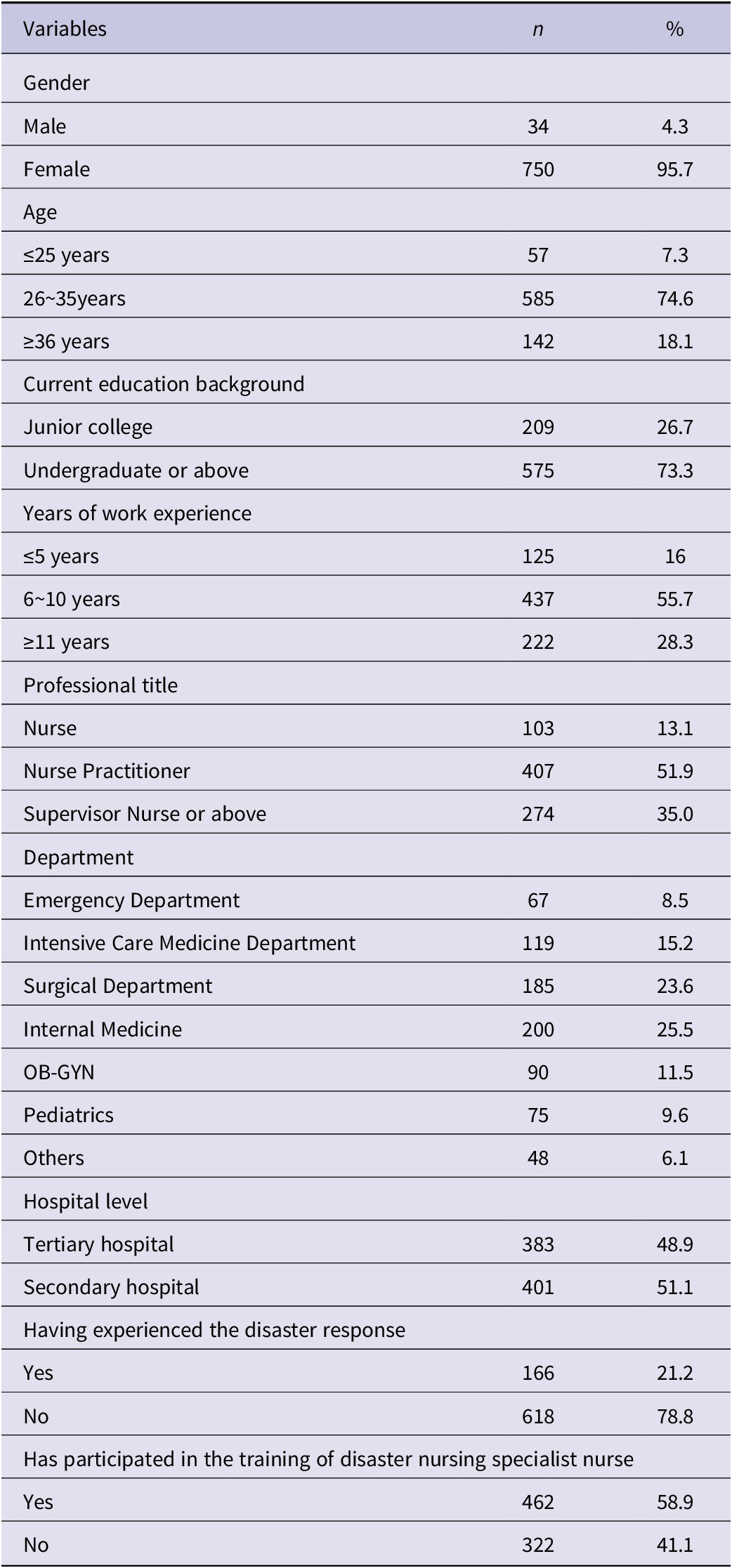
A total of 813 questionnaires were distributed. Having excluded 12 questionnaires with identical answer options and 17 questionnaires with incomplete information, 784 valid questionnaires were finally returned, for an effective questionnaire response rate of 96.43%.
Score of Nurses’ Disaster Preparedness Survey
The total average score of the disaster preparedness questionnaire for 784 nurses is (146.76 ± 34.98) and the average score of all the entries is (3.26 ± 0.45), indicating moderate performance. The scores for each dimension are shown in Table 2A and 2B. Figure 1 is the distribution chart of disaster preparedness score frequencies of nursing personnel.
Table 2A. Scores of nurses’ disaster preparedness in various dimensions.(categorize by content points,
 $ \overline{x} $
± s)
$ \overline{x} $
± s)
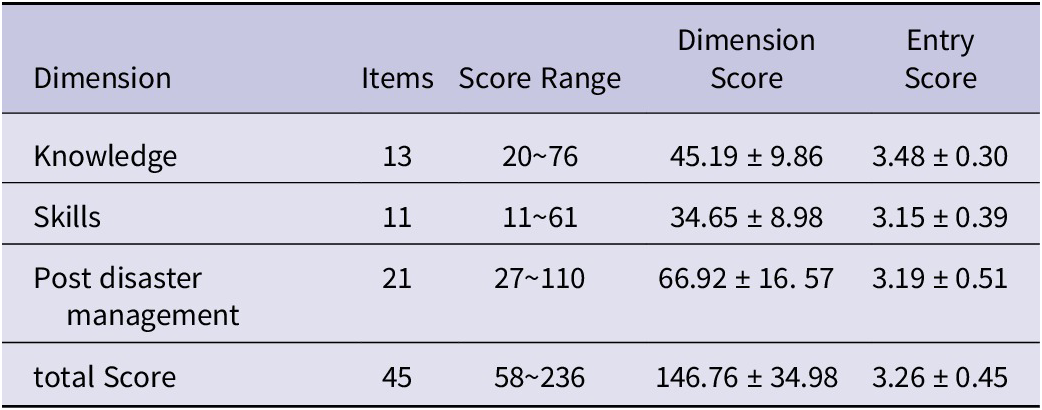
Table 2B. Scores of nurses’ disaster preparedness in various dimensions (classified by stage; points,
$ \overline{x} $
± s)

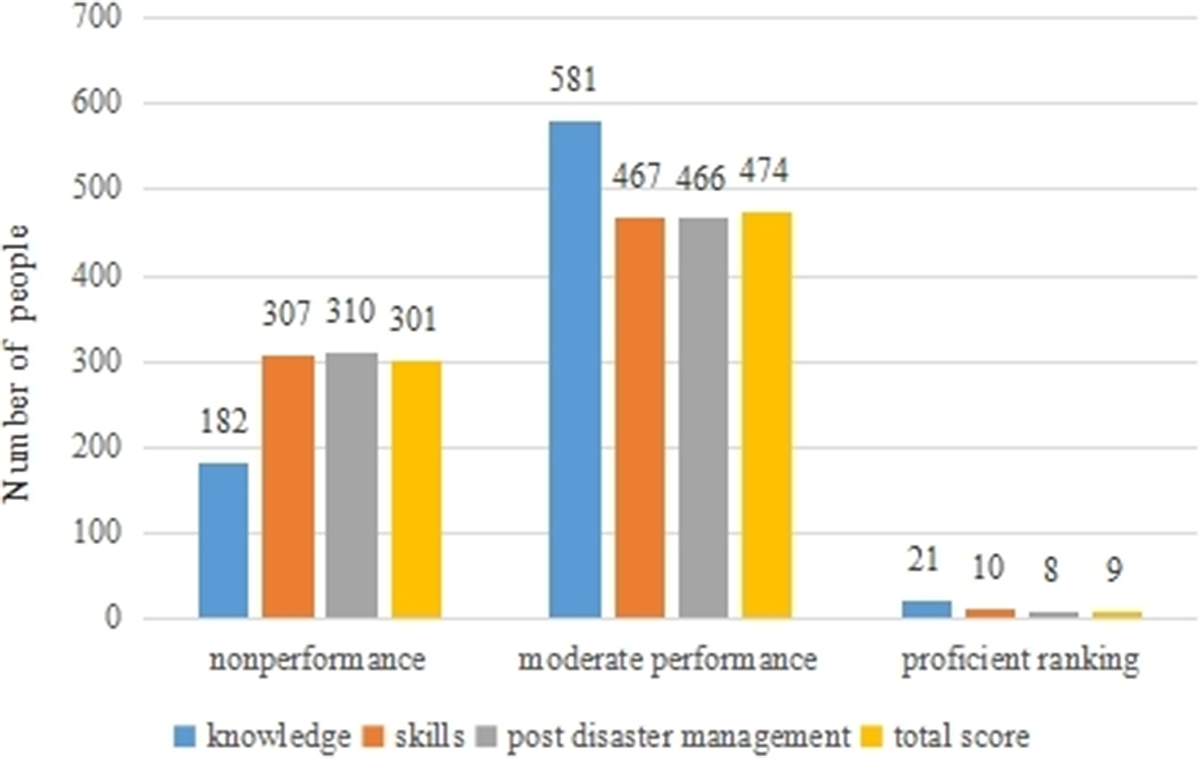
Figure 1. Distribution chart of disaster preparedness score frequencies of nursing personnel.
An average score of 1-2.99 (total score of 45-134) indicates nonperformance, an average score of 3-4.99 (total score of 135-224) equates to moderate performance, and an average score of 5-6 (total score of 225-270) denotes proficient ranking. The overall distribution is shown in Figure 1. The entry with the highest score (4.39±1.03) is “I know the limits of my knowledge, skills, and authority as an RN to act in disaster situations, and I would know when I exceed them,” while the lowest score (2.48±1.14) lies in “I am familiar with the main Groups (A, B, C) of biological weapons (Anthrax, Plague, Botulism, Smallpox, etc.), their signs and symptoms, and effective treatments.” The specific scores for some entries are shown in Table 3 from low to high
Table 3. Scores of nurses’ disaster preparedness in each item (points,
$ \overline{x} $
±s)

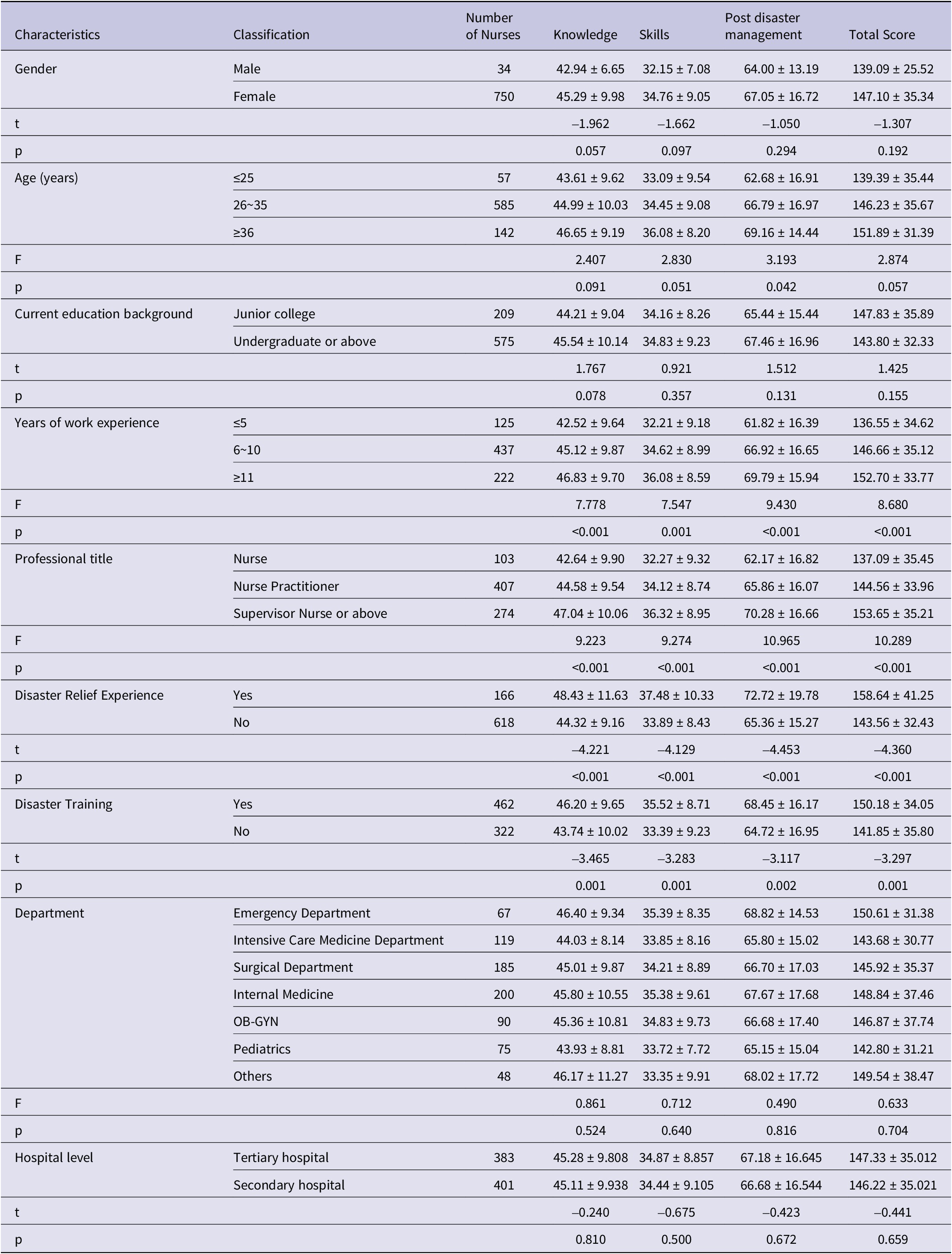
Single Factor Analysis of Nurses’ Disaster Preparedness
We set the general information of the respondents as independent variables and analyzed the differences in disaster preparedness scores across different dimensions and characteristics compared to the nurses’ total scores. The results indicate that age affects disaster management (P < 0.05), meaning that as age increases, the scores also tend to be higher. Work experience, professional titles, disaster relief experience, and disaster training significantly differ in terms of disaster knowledge, skills, management scores, and total scores (P < 0.01). Details are demonstrated in Table 4.
Table 4. Single factor analysis of the total score and scores in various dimensions (points,
$ \overline{x} $
±s)
Multivariate Analysis of Nurses’ Disaster Preparedness
We set the total score of disaster preparedness as the dependent variable and general information of survey subjects as independent variables. Four variables including years of work, title, disaster relief experience, and disaster training were introduced into the regression equation. The result indicates that titles, disaster relief experiences, and disaster training are the main factors affecting the disaster preparedness of nurses in county-level hospitals (P < 0.05). Details are demonstrated in Table 5.
Table 5. Multiple linear regression analysis of factors influencing nurses’ disaster preparedness

Discussion
Nurses play various roles at each stage of a disaster, including as caregivers, rescuers, educators, coordinators, and managers.Reference Labrague, Hammad and Gloe20 There have been reports on relevant studies in China and other countries around the world that nurses play a crucial role in disaster management before, during or after a disaster while also facing some challenges.Reference Al Harthi and Al Thobaity21‒Reference Alharazi and Al Thobaity24
Results show that the overall level is relatively moderate to low, which indicates a significant gap compared to some foreign developed countries such as the United States, Japan, Australia,Reference Brewer, Hutton and Hammad25 Singapore, Germany, Saudi Arabia,Reference Farghaly Abdelaliem, Baghdadi and Al Anizi26 and major domestic cities like Shanghai (199.78±54.51) and Beijing (201.84±38.97) in terms of disaster preparedness.Reference Wang, Liu and Yu27 The scores are also lower than those from cities in Hubei and Sichuan provinces in China, which have scores of 187.60±40.45 (results from Chinese literature). Analyzing by dimension, the score for Knowledge (3.48±0.30) was the highest. When broken down by phase, the score for Recovery stage was extremely low (2.82±0.42), significantly under-performing in comparison to Pre Disaster Preparedness and Response.
Entries with the highest score are “I know the limits of my knowledge, skills, and authority as an RN to act in disaster situations, and I would know when I exceed them” and “I participate in disaster drills or exercises at my workplace (clinic, hospital, etc.) on a regular basis.” This is closely related to the Chinese experience of gradually attaching importance to and establishing a disaster relief system following the 2008 Wenchuan earthquake and the recent COVID-19 pandemic in the years 2019 to 2020. Whereas entries like “I would be considered a key leadership figure in my community in a disaster situation,” “I am familiar with what the scope of my role as a registered nurse in a postdisaster situation would be” and “I am familiar with the main Groups (A, B, C) of biological weapons (Anthrax, Plague, Botulism, Smallpox, etc.), their signs and symptoms, and effective treatments” are of the lowest scores. Among them, except for the last entry which may be related to the currently stable social environment in China and that biochemical threats are rare, the direct causes of the former 2 should be related to nursing staffs’ lack of clarity about their roles at various stages of disasters and a lack of confidence. The indirect reasons leading to this outcome may have a tight bond with the education, training, drills, and management systems for nurses in disaster nursing.
Overall, factors such as nursing seniority (years of service and professional title), experience in disaster relief, and disaster training influence scores, but nurses working in emergency departments and ICUs do not have an advantage in scoring. This is inconsistent with some domestic studies, which show that emergency and ICU nurses in many cities receive broader and more frequent disaster-related training. This indirectly suggests that the 4 hospitals in Yongcheng may not be adequately implementing nurse training programs, nor are they conducting stratified training.
Yongcheng is typical of non-first-tier (inland) cities in China, so the sample surveyed here can represent the nursing level in most small cities in China. Following the analysis of survey data, it is more appropriate to develop and implement strategies for the preparation of disaster nursing in a step-by-step and context-specific manner. We aimed to explore strategies from 4 aspects:
Strategy 1. An education in comprehensive knowledge is necessary for nursing professionals. Disaster rescue knowledge cannot solely rely on accumulated experience and training. Rather, it should commence from the foundational education as part of a systematic learning process.
By 2008, 7 nursing schools, including Columbia University School of Nursing and Johns Hopkins University School of Nursing, had made disaster nursing a major direction for master’s students, with the aim of cultivating professional talents in disaster rescue and scientific research.Reference Tang, Shi and Jiang28‒Reference Du, Shi and Jiang30 These students are required to complete courses such as health management, education, domestic and international humanitarian comfort studies, emergency plan development, and disaster response studies. In the United States, disaster education content is primarily divided into theoretical knowledge related to disaster rescue and practical skills.Reference Loke, Guo and Molassiotis31 The theoretical knowledge in disaster nursing education includes triage, monitoring rare epidemics, emergency plan development, leadership development, group collaboration, mental health care, ethics, and legal aspects. Rescue skills not only cover basic skills training in trauma treatment and first aid but also include training in using personal protective equipment in biological, nuclear events, and terrorist attacks.
In Yongcheng, as well as in most of China’s coastal big cities, most nurses hold a diploma as their first academic qualification, with a 3-year program. Their basic education is relatively weak, professional course teaching progresses quickly, and the disaster rescue knowledge they learn is fragmented and unsystematic. We also found in this survey that scores for the 2 items related to PTSD were low, indicating that nurses’ knowledge reserves and responses in this area are inadequate. During the disaster mitigation phase, it is crucial for nurses to pay attention to both the emotional and physical trauma of survivors and their own psychological states. Psychology courses must also be incorporated into basic education. Furthermore, entries related to bioterrorism and biochemical attacks generally scored lower in the survey. Despite the favorable social environment in China, if the influence of biological hazards or even bioterrorism spread out because of ineffective containment, it could potentially escalate into large-scale terrorist events resulting in significant casualties. Consequently, knowledge acquisition in relevant areas should also be integrated into the curriculum of basic nursing education.
In 2015, the Disaster Professional Committee of Chinese Nursing Association organized the compilation of the textbook Disaster Nursing, marking a gradual advancement in disaster nursing education in China to address the current situation. However, due to a lack of corresponding faculty and supportive educational resources in China, institutions offering disaster nursing as a standalone course remain limited. Nursing institutions at all levels have begun to train disaster rescue specialist nurses and develop training courses to compensate for the deficiencies in basic education. Additionally, Tongji University’s Liu Zhongmin and Wang Tao launched the nationally renowned “Escape and Self-Rescue (Chinese University MOOC)” course in Shanghai, but it was only incorporated into the curriculum for clinical medical students. Nursing education in China is divided into graduate, undergraduate, and diploma programs. It is suggested to tailor education according to different levels of academic qualifications to cultivate professional talents in disaster nursing. For nursing vocational and undergraduate students, students will be enabled to possess basic knowledge and skills in disaster nursing, so that a solid foundation for future participation in rescue practice or advanced training can be laid. For regions prone to various disasters, master’s and doctoral programs in disaster nursing should be established referring to the ICN Nursing Core Competencies standards for curriculum design and regular updates with the target of setting “Disaster Nursing Core Competencies” Level II and III as training objective,emphasizing the integration of theory and practice and encouraging international academic exchanges to learn from the forefront of disaster nursing research to provide a continuous supply of emergency mid-to-high-level talents in disaster nursing for regions that are susceptible to frequent disasters comparatively in China, especially in the western regions.
Strategy 2. Maximize the scope of extensive nursing skills training and emphasize the importance of cultivating nursing leaders, as it’s accepted that training paramedics in disaster response is an essential part of preparedness within the disaster management cycle.Reference Horrocks, Hobbs and Tippett32
Currently, the training of core disaster nursing skills for junior nurses relies solely on traditional materials such as PowerPoint presentations and literature, combined with practical training in skills like CPR. This method of training is far from sufficient for adequately preparing nurses to respond to disaster situations. County-level cities like Yongcheng have limited funds available for disaster preparedness. As a result, laying emphasis on training related to potential disasters in the local context can make nursing training within hospitals or collaborations between hospitals more effective. For instance, in areas prone to earthquakes, mudslides, and collapses, hospitals can prioritize training in skills such as fracture immobilization, hemostasis, and bandaging. In regions near industrial zones like chemical and petroleum facilities, it is essential to concentrate on training for prevention of inhalation, mitigation of radiation exposure, and handling of poisoning and burns. For serious epidemics, natural disasters, biological accidents or attacks, chemical accidents or attacks, explosions/combustion accidents or attacks, and nuclear/radioactive accidents,approaches like online training and remote lectures by inviting experts from major cities can be applied.
Since its inception in 2018, the National Virtual Simulation Experimental Teaching Course Sharing Platform in China has significantly advanced the field of online experimental teaching. This platform now boasts 4790 experimental centers across 12 disciplines, including 658 in medicine, marking a qualitative leap in online experimental education. The platform is focused on enhancing emergency core competencies by fully simulating urgent and complex situations, facilitating scenario simulations, investigative deductions, and immersive experiences. Notable virtual simulations include “Emergency Handling of a Sudden Plague Outbreak” and “Key Technologies for Health Emergency Handling of Biological Terror Attacks in Public Places,” with over 10 000 training sessions completed to date. However, the primary users have been students enrolled in medical universities. There is a growing need to make these resources available to a broader audience, particularly for continuing education among graduates.
Except for this, given the complex nature of disaster rescue operations which often involves multiple casualties, challenging conditions, and heavy treatment tasks, rescue team members are required to have comprehensive capabilities that are specialized and versatile. In the face of disaster, individual capabilities seem insignificant, and skills can become non-standard in emergency states. Therefore, good nursing team cooperation is extremely important. Nurses make up 50% of disaster relief teams, and we recommend selecting excellent professionals with strong emergency skills, such as those in emergency and intensive care, to be trained as nursing leaders who can oversee the reasonable allocation of nursing staff, detail responsibilities, and enhance treatment efficiency. Training programs like the American Heart Association’s ACLS and TEAMSTEPPS are recommended for team training and have already been implemented in many cities across China.
Strategy 3. Explore the implementation of disaster simulation training between urban areas. From the survey analysis in this research, it is evident that nursing personnel with disaster relief experience generally exhibit a higher level of disaster preparedness compared to their counterparts without such experience. We believe that inter-city disaster simulation training is a way to improve the disaster preparedness level of nursing staff.
In May 2018, Chinese disaster prevention and emergency alliance was established by the efforts of 10 first level-rated medical health associations and societies. The experts agree that the Chinese disaster medical rescue system should start before the disaster, emphasize action during the disaster, and extend care after the disaster. The current situation in Yongcheng’s hospitals is that disaster training exercises are isolated, fragmented, and conducted on a small scale. There is an urgent need to develop integrated and comprehensive inter-city joint simulation training programs. Such collaborative initiatives would enable the pooling of resources and expertise, fostering a more unified and effective approach to disaster preparedness.
In 2001, China established the National Earthquake Disaster Emergency Rescue Team, and since 2003, it began to plan for the establishment of a national-level health emergency team. By 2010, national administrative departments had formed 37 national health emergency rescue teams in 23 provinces across the country, for emergency response to disasters and sudden incidents, counterpart support, and health poverty alleviation. They have accumulated rich experience in emergency drill equipment, participating in practical drills for rapid response, on-site rescue, and talent and discipline construction. However, Henan Province only has 1 such team. Referring to the national-level emergency rescue team’s training program and localizing it to explore and form a municipal-level regional simulation training program might be something for health department managers in cities like Yongcheng to consider. In the summer of 2023, Yongcheng City Central Hospital Medical Health Group issued an implementation plan for the establishment of a health emergency team, with 4 emergency teams under it, marking a leap in exploring regional cooperative disaster rescue models. The organizational structure is shown in the Figure 2.
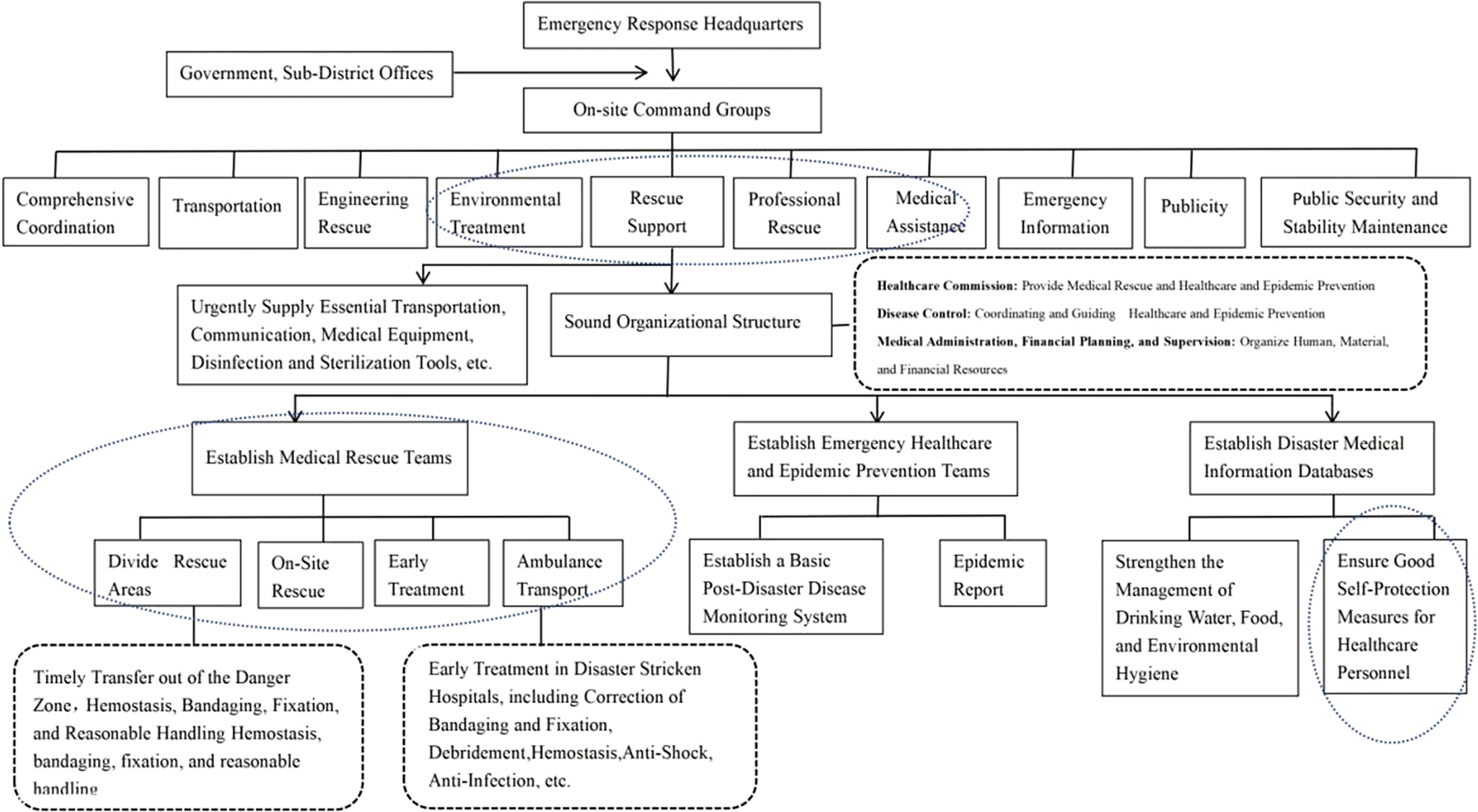
Figure 2. Emergency organization command system structure chart.
Strategy 4. The government and health administrative departments need to further highlight their supporting roles. In addition to enhancing the disaster rescue capabilities of medical personnel through knowledge and skills training and drills, the role of the government and health administrative departments is crucial. As public hospitals, the government needs to allocate funds for material reserves, talent training, and project construction.
Regarding disaster rescue triage, while it may not be feasible to establish large-scale, fully functional medical rescue bases like those in major cities, county-level cities should also establish a disaster management and diversion system with tertiary hospitals (higher-level hospitals) as the central force for emergency rescue, secondary hospitals providing auxiliary support in treatment, and community hospitals serving as the main force for post-disaster rehabilitation. When higher-level hospitals are unable to immediately accommodate a large number of casualties during the disaster, experienced nursing specialists or doctors from those hospitals can coordinate with and assist lower-level hospitals to divert and manage the injured individuals. It is undeniable that in the face of disaster, managers and coordinators can be government personnel with some medical knowledge. This necessitates the identification and development of such disaster preparedness capabilities through joint participation in regular training and exercises. During the planning phase, it is essential to clarify the division of tasks among hospitals at various levels and various organizations. Coordinating task assignments and establishing an executable system require the support of the local government. To integrate emergency management and public health response more seamlessly, exercises inclusive of partner agencies as well as relevant and senior-level leaders from respective organizations may be considered.Reference Li, Hsu and Pham33
In addition, the allocation of nursing resources for disaster preparedness, including human resources; material resources, such as a sufficient blood supply containing as many blood types as possible; respiratory masks; gas masks; and other special requirement supplies, as well as the turnover and timely supply of other basic medical materials, should be taken into consideration. If it’s possible, coordinating and connecting with emergency teams from other provinces to supplement and respond to particularly severe disasters can also be a method.
During the early stages of the COVID-19 pandemic in 2019, many parts of inland China experienced a shortage of medical supplies and a rapid conversion of numerous hospital resources to pandemic response, causing a halt in routine medical services and significant distress to the general public’s health. Effectively allocating medical resources and making reasonable arrangements for nursing staff is a prerequisite for improving the success rate of disaster relief and serves as strong support for frontline medical personnel.
Limitations
This study surveyed nurses from 4 comprehensive hospitals at or above the second level in Yongcheng, thereby limiting the generalizability of its results to other countries or even other parts of China. This survey was cross-sectional in nature, so represents the views of the participants at the time of the survey. Further, this survey was voluntary and those who did not complete it might represent groups with different responses than those reported in this paper. Participants might represent the core competence of local nurses in Yongcheng but is not representative of the global nursing workforce. This led to a potential for selection bias, as well as the limited generalizability of the research design. We look forward to further research that addresses these deficiencies.
Conclusion
This paper presents a survey conducted on nurses from secondary or higher-level hospitals in Yongcheng City, Henan Province, China, and discusses strategies for improving disaster preparedness. It holds certain reference significance for some key small cities in inland China, such as those with coal, petroleum, nuclear, chemical industrial zones, or tourist destinations, as well as various transportation hubs. We are also conducting interviews with nurses who have participated in disaster relief and had expected further guidance, focusing on their experiences at the disaster sites and self-evaluation with the objective of establishing appropriate and feasible nursing training programs. Additionally, regardless of natural disasters, man-made disasters, or sudden outbreaks of epidemics, how to refine responses, management, and disposal at various stages of disasters could be topics for further exploration in the future.
Author contribution
Li Xu: Conceptualization, Methodology. Min Wu: Visualization, Investigation, Data curation, Writing- Original draft preparation. Xueyan Li:Supervision, Writing- Reviewing and Editing. Yanshen Wang: Data curation, Writing- Original draft preparation, Visualization, Investigation.
Funding statement
This study was supported by grants from the National Natural Science Foundation of China (No. 82070541, 81600625, 82271406, 81771332, 81571184); the Natural Science Foundation of Shanghai (22ZR1451200), the Health Industry Clinical Research Project of Shanghai Municipal Health Commission (20204125, 201840110); the Key Disciplines Group Construction Project of Shanghai Pudong New Area Health Commission (PWZxq2022-10); the Medical Discipline Construction Project of Pudong Health Committee of Shanghai (PWYgy2021-07); the Li Jieshou Intestinal Barrier Research Foundation (LJS-201901A); the Japan-China Sasagawa Medical Fellowship; Important Weak Subject Construction Project of Shanghai Pudong New Area Health Commission (Grant No. PWZbr2022-04); the Three-Year Action Plan for Discipline Construction of School of Nursing, Tongji University (JS2210320).
Competing interest
The author(s) declare no competing interests.










 Open access
Open access