


Communication Deviance (CD)
The concept of CD, first proposed by Lyman Wynne and Margaret Singer (e.g., Wynne & Singer, Reference Wynne and Singer1963a, Reference Wynne and Singer1963b) in an attempt to understand familial predictors of psychosis, refers to qualities of communication, usually coded from parental speech, that leave a listener uncertain, puzzled, and unable to share a focus of attention with the speaker. It is defined in terms of a range of verbal-linguistic atypicalities that are believed to disrupt the establishment and maintenance of focus of attention during communication. These atypicalities are argued to impair the development of conversational alignment between interlocutors, compromising shared meaning and grounding (i.e., mutual knowledge, beliefs, and assumptions; Miklowitz & Stackman, Reference Miklowitz and Stackman1992; Nuechterlein, Goldstein, Ventura, Dawson, & Doane, Reference Nuechterlein, Goldstein, Ventura, Dawson and Doane1989; Singer & Wynne, Reference Singer and Wynne1965a, Reference Singer and Wynne1965b; Wynne & Singer, Reference Wynne and Singer1963a, Reference Wynne and Singer1963b; Wynne, Singer, Bartko, & Toohey, Reference Wynne, Singer, Bartko, Toohey and Tanner1977). They are subtle and can range from ambiguous linguistic references (e.g., “Kid stuff that's one thing but something else is different too”; Velligan, Goldstein, Nuechterlein, Miklowitz, & Ranlett, Reference Velligan, Goldstein, Nuechterlein, Miklowitz and Ranlett1990, p. 18) or contradictions (e.g., “I didn't get much sleep last night. [Interviewer: Are you tired?] Yeah, I ain't tired”; Docherty, Reference Docherty1993, p. 753) to more overarching nonverbal characteristics at the level of the pragmatics of communication (e.g., mistimed turn taking; Wynne et al., Reference Wynne, Singer, Bartko, Toohey and Tanner1977).
The concept of CD possibly overlaps with other constructs measured in developmental longitudinal studies, but has some specific elements. For example, there is a substantial literature on the relationship between parents’ mental representations of attachment, coded from their accounts of their own childhood attachment-related experiences and their sensitivity to their infants’ attachment signals (van Ijzendoorn, Juffer, & Duyvesteyn, Reference van Ijzendoorn, Juffer and Duyvesteyn1995; Verhage et al., Reference Verhage, Schuengel, Madigan, Pasco Fearon, Oosterman, Cassibba and van Ijzendoorn2016). The concept of narrative coherence, which is rated from the Adult Attachment Interview in terms of representations of attachment that are well integrated, clear, relevant, and reasonably succinct, appears similar to the concept of CD. However, CD differs from narrative incoherence because it is defined entirely in terms of the quality and formal aspects of the speech and communication of the parent (e.g., unintelligible remarks, odd word usage, etc.). Similarly, some developmental studies have measured maternal expressed emotion (EE) with one study showing a significant association between parental EE, measured during pregnancy, and lower levels of sensitive parenting when the child was aged 4 (Lucassen et al., Reference Lucassen, Tiemeier, Luijk, Linting, Bakermans-Kranenburg, van Ijzendoorn and Lambregtse-Van den Berg2015). However, EE is defined in terms of parental overinvolvement, criticism, or hostility, and not the parents’ quality of communication or speech, and the two constructs appear to be readily distinguishable from each other (Velligan, Goldstein, Nuechterlein, Miklowitz, & Ranlett, Reference Velligan, Goldstein, Nuechterlein, Miklowitz and Ranlett1990).
Wynne (Reference Wynne1981) proposed that CD in the caregiver, in interaction with genetic vulnerability in the offspring, would lead to the escalation of the cognitive and affective abnormalities, especially thought disorder (TD), later observed in schizophrenia. Consistent with this hypothesis, a recent meta-analysis of 20 studies (N = 1,753) found a large magnitude (g = .97) association between maternal (but not paternal) CD and offspring diagnosis of psychotic disorder (de Sousa, Varese, Sellwood, & Bentall, Reference de Sousa, Varese, Sellwood and Bentall2014). Moreover, in a longitudinal study of children attending a child guidance service, Goldstein (Reference Goldstein1987) found that both CD and EE were independently strong predictor of later psychosis.
The relationship between CD and genetic risk for schizophrenia was explored by Wahlberg et al. (Reference Wahlberg, Wynne, Oja, Keskitalo, Pykalainen, Lahti and Tienari1997, Reference Wahlberg, Wynne, Oja, Keskitalo, Anais-Tanner, Koistinen and Tienari2000), who used an adoption study design to show that the interaction between having a biological mother diagnosed with schizophrenia and adoptive parents’ CD was a significant predictor of TD in the adoptee. In this study, high genetic risk alone did not predict TD (high genetic-risk adoptees, when exposed to low CD parents, displayed less TD than low-risk adoptees).
Despite these important findings, it is important to acknowledge that it remains unclear whether parental CD is a risk factor specific to TD, schizophrenia, or a wider range of psychiatric conditions (Roisko, Wahlberg, Miettunen, & Tienari, Reference Roisko, Wahlberg, Miettunen and Tienari2014). Furthermore, it is possible that CD may reflect an important environmental risk for a range of mental health disorders (Wahlberg et al., Reference Wahlberg, Wynne, Hakko, Läksy, Moring, Miettunen and Tienari2004).
The Influence of CD on Cognitive and Social Development
Given that parental, especially maternal CD is associated with later psychiatric symptoms in offspring, it is important to investigate mechanisms that could account for this relationship. Wynne and Singer argued that parental CD has this effect through its pervasive impact on the offspring's social and cognitive development during formative years (Wynne et al., Reference Wynne, Singer, Bartko, Toohey and Tanner1977). According to them, this development is embedded in different facets of family relatedness such as caregiving, problem solving, mutuality, and intimacy, and these facets represent evolving and increasingly complex levels of interconnected dyadic and familial interaction (Wynne, Reference Wynne1984, Reference Wynne and Falicov1988). Within this framework, children learn to share and sustain foci of attention, and thereby derive meaning from the world around them, through communication with their caregivers (Wynne, Reference Wynne1981, Reference Wynne1984). Atypicalities at the level of communication in the caregiver can therefore disrupt very early development through their expression at the more basic level of relatedness with the infant during early preverbal dialogues (Wynne, Reference Wynne1968). In this context, CD is conceptualized as a risk marker for parental mental processes that might give rise to disruptions to the caregiving system (Singer & Wynne, Reference Singer and Wynne1966a, Reference Singer and Wynne1966b).
However, empirical evidence on mechanisms linking CD to specific developmental processes in early childhood has so far been limited. Cross-sectional studies have found that CD in the caregiver is associated with poorer social, cognitive, and emotional development in the 7- and 10-year-old children of parents diagnosed with severe mental health disorders (Doane et al., Reference Doane, Jones, Fisher, Ritzler, Singer and Wynne1982), and with social withdrawal and behavioral problems in 9-year-olds (Velligan, Christensen, Goldstein, & Margolin, Reference Velligan, Christensen, Goldstein and Margolin1988). Drawing from data collected in a high-risk longitudinal study (the University of Rochester Child and Family Study; Wynne, Cole, & Perkins, Reference Wynne, Cole and Perkins1987), Wynne and his colleagues reported associations between parental communication that is vague, contradictory, and unresponsive and both anxiety (Wichstrøm, Holte, & Wynne, Reference Wichstrøm, Holte and Wynne1993) and poorer social competence in 7- and 10-year-old children (Wichstrøm, Holte, Husby, & Wynne, Reference Wichstrøm, Holte, Husby and Wynne1993, Reference Wichstrøm, Holte, Husby and Wynne1994). In the same high-risk cohort, but at longer follow-up (≥18 years of age), unresponsive communication in parents significantly predicted psychological distress, poorer well-being, and global mental health in the offspring (Wichstrøm, Anderson, Holte, Husby, & Wynne, Reference Wichstrøm, Anderson, Holte, Husby and Wynne1996), and disconfirmatory communication, which ignores or rejects what the child says, was a significant predictor of poor interpersonal functioning and mental health hospitalization (Wichstrøm, Anderson, Holte, Husby, et al., Reference Wichstrøm, Anderson, Holte, Husby and Wynne1996).
The study of parental representations may provide further clues about the likely developmental impact of CD. An important body of literature on the Working Model of the Child Interview (WMCI; Vreeswijk, Maas, & van Bakel, Reference Vreeswijk, Maas and van Bakel2012) emerging during the last decade has shown that distorted maternal representations of offspring are a predictor of atypical and noncontingent maternal behaviors (Schechter et al., Reference Schechter, Coates, Kaminer, Coots, Zeanah, Davies and Myers2008) and poorer quality of dyadic interactions between the caregiver and the child (Korja et al., Reference Korja, Ahlqvist-Björkroth, Savonlahti, Stolt, Haataja, Lapinleimu and Lehtonen2010). In this literature, distorted representations are characterized by descriptions of the child that are incoherent, confused, contradictory, or even bizarre (Vreeswijk et al., Reference Vreeswijk, Maas and van Bakel2012). Of particular significance for the present purposes, some studies have explored mothers’ representations of their future children using a prenatal version of the WMCI, observing that distorted maternal representations during pregnancy are associated with higher levels of hostility and anger in caregiver's interaction with the infant at 12 months postpartum (Dayton, Levendosky, Davidson, & Bogat, Reference Dayton, Levendosky, Davidson and Bogat2010) and more disengagement and less sensitive and warm parenting (Theran, Levendosky, Bogat, & Huth-Bocks, Reference Theran, Levendosky, Bogat and Huth-Bocks2005).
Maternal Sensitivity
Maternal sensitivity is defined in terms of the extent to which the caregiver's responses to infant cues are contingent, appropriate, interested, and warm (Bornstein & Tamis-Lemonda, Reference Bornstein and Tamis-Lemonda1997). Its importance during infancy is supported by diverse findings. For example, low maternal sensitivity during infancy predicts harsh parental discipline during toddlerhood (Joosen, Mesman, Bakermans-Kranenburg, & van Ijzendoorn, Reference Joosen, Mesman, Bakermans-Kranenburg and van Ijzendoorn2012), and interacts with monamine oxidase A (MAOA) polymorphisms in offspring to predict temperamental anger proneness (Pickles et al., Reference Pickles, Hill, Breen, Quinn, Abbott, Jones and Sharp2013), and with dopamine D4 receptor (DRD4) polymorphisms in offspring to predict child externalizing behaviors (Bakermans-Kranenburg & van Ijzendoorn, Reference Bakermans-Kranenburg and van Ijzendoorn2006).
Fraley, Roisman, Booth-LaForce, Owen, and Holland (Reference Fraley, Roisman, Booth-LaForce, Owen and Holland2013) took advantage of repeated measurements of maternal sensitivity and of social and academic competence over childhood, together with measures of potential confounders, and reported that the strength of association between maternal sensitivity and later social and cognitive functioning did not attenuate over time, and that it could not be accounted for by potential confounding variables nor by transactional processes. The same group showed similar effects up to age 32 for academic functioning although, in the case of social functioning, associations with maternal sensitivity were accounted for by confounders such as early socioeconomic factors and child's sex (Raby, Roisman, Fraley, & Simpson, Reference Raby, Roisman, Fraley and Simpson2014). Van der Voort et al. (Reference van der Voort, Linting, Juffer, Bakermans-Kranenburg, Schoenmaker and van Ijzendoorn2014) addressed the possibility of genetic confounding in a longitudinal study of children adopted in infancy and found that maternal sensitivity during infancy predicted internalizing symptomatology during adolescence. A causal role for maternal sensitivity is further supported by clinical trials of attachment-based interventions that show that rates of insecure or disorganized attachment can be reduced by increasing maternal sensitivity (Juffer, Bakermans-Kranenburg, & van Ijzendoorn, Reference Juffer, Bakermans-Kranenburg and van IJzendoorn2005; van Ijzendoorn et al., Reference van Ijzendoorn, Juffer and Duyvesteyn1995).
Methods of assessing maternal sensitivity vary considerably in the extent to which they use home or lab-based observations, whether the conditions are standardized, their coding, or the duration of the observations. It may be that these broad characterizations ignore possible issues of domain specificity whereby aspects of sensitivity that entail different processes may have different developmental consequences (Grusec & Davidov, Reference Grusec and Davidov2010). In particular, maternal sensitivity to infant bids for reciprocity in playful interactions are likely to promote joint exploration and joint attention (Hobson, Patrick, Crandell, Perez, & Lee, Reference Hobson, Patrick, Crandell, Perez and Lee2004) and hence cognitive development (Bornstein & Tamis-Lemonda, Reference Bornstein and Tamis-Lemonda1997) but does not appear to contribute to attachment security (Murray et al., Reference Murray, Hentges, Hill, Karpf, Mistry, Kreutz and Green2008). In contrast, sensitive and comforting responses to infant distress are associated with attachment security (Leerkes, Reference Leerkes2011) but not cognitive development (McElwain & Booth-Laforce, Reference McElwain and Booth-Laforce2006). Moreover, it has been suggested that sensitivity to distress and nondistress may have different antecedents, with the later being significantly associated with sociodemographic factors (e.g., age, education, income, or uninvolved partner) and the former with the caregiver's emotional and cognitive competencies and responses to the infant's negative emotions (Leerkes, Reference Leerkes2010; Leerkes, Crockenberg, & Burrous, Reference Leerkes, Crockenberg and Burrous2004; Leerkes, Weaver, & O'Brien, Reference Leerkes, Weaver and O'Brien2012).
Current Study
Previous studies have typically measured parental CD during the child's early years and have therefore failed to consider the possibility that the association between CD and offspring's development might have been confounded by the evocative effect of child's behavior on the parents’ communication (Miklowitz & Stackman, Reference Miklowitz and Stackman1992). Just as important for the present purposes, Wynne (Reference Wynne1968) originally conceived CD to be a risk marker for parental mental processes that disrupt early caregiving (Singer & Wynne, Reference Singer and Wynne1966b), but this possibility is difficult to test in studies that focus exclusively on verbal communication between parents and verbally competent children.
In this study, we addressed both of these issues by investigating whether CD measured during pregnancy (in primiparous mothers) was a significant predictor of caregiver–infant interaction at 29 weeks. Given the more recent research that has shown that maternal representations during pregnancy that are incoherent, confused, contradictory, or bizarre, measured with the WMCI, are associated with later parenting characterized by disengagement and less sensitivity and warmth (Theran et al., Reference Theran, Levendosky, Bogat and Huth-Bocks2005), we predicted that increased CD at 32 weeks gestation would be associated with decreased maternal sensitivity during early caregiver–infant dyadic communication and that these effects would not be accounted for by plausible confounders. Moreover, as maternal sensitivity in the context of infant distress and nondistress may each have distinct antecedents, and different consequences to the infant's social and cognitive development, we examined the contribution of CD to each.
Method
Design
The current study draws on data from the Wirral Child Health and Development Study (WCHADS; Sharp et al., Reference Sharp, Pickles, Meaney, Marshall, Tibu and Hill2012), a prospective longitudinal study that aims to identify early social, emotional, and biological risks involved in the development of childhood conduct problems.
In the WCHADS, first-time mothers were recruited to establish a general population (extensive sample) from which an intensive subsample was drawn. The extensive sample comprised primiparous mothers (≥18 years of age and English speaking) who sought antenatal care at 12 weeks gestation between February 2007 and October 2008 at the Wirral University Teaching Hospital. The intensive subsample was stratified by psychosocial risk (partner psychological abuse), and both samples were then followed in tandem. A detailed flowchart of the sampling and recruitment procedure can be found elsewhere (Sharp et al., Reference Sharp, Pickles, Meaney, Marshall, Tibu and Hill2012). This two-stage stratified design enables intensive measurement in the subsample (including the assessment of CD and maternal sensitivity), while collection of other measures across the extensive sample allows weighting back of the findings from the intensive subsample to give general population estimates.
At 32 weeks, mothers in the intensive sample provided 5-min speech samples in which they spoke without interruption about their anticipated relationship with their as yet unborn child (Leeb et al., Reference Leeb, Hahlweg, Goldstein, Feinstein, Mueller, Dose and Magana-Amato1991), as described in more detail below. This methodology, adapted from a method used to measure EE in patients, has been previously used to measure EE during pregnancy (e.g., Lambregtse-van den Berg et al., Reference Lambregtse-van den Berg, Lucassen, Kuipers-Nap, Dingemans, Jaddoe, Hofman and Tiemeier2013; Lucassen et al., Reference Lucassen, Tiemeier, Luijk, Linting, Bakermans-Kranenburg, van Ijzendoorn and Lambregtse-Van den Berg2015). The speech samples were audio-recorded, transcribed by members of the WCHADS team, and later coded for CD.
At 29 weeks into the postnatal period, mothers completed a 15-min play protocol with their babies in the research base (NICHD Early Child Care Research Network, 1999). Maternal sensitivity was coded from these interactions. Approval for the procedures was obtained from the local Research Ethics Committee.
Recruitment and sample
As described in detail in Sharp et al. (Reference Sharp, Pickles, Meaney, Marshall, Tibu and Hill2012), the full cohort of 1,233 WCHADS mothers (with live singleton births) participated in several waves of assessment, and a stratified random subsample of 316 was drawn for additional more intensive assessments. Of the 316 participants, 29 either indicated that they did not wish to do the task or found they were unable to speak for the 5 min. Of the 287 who provided the 5-min speech sample in pregnancy, 237 attended for the 29 weeks assessment that included the observations of mothers and infants in play. Reasons for nonattendance included that the family no longer wished to participate, illness in the family, and other family events. Adjustments for attrition made in the analyses are described in the Statistical Analysis section. Sensitivity to distress could be rated on the 180 assessments where the child showed distress at some point over the 15 min of observations. The design allows estimates of means and coefficients for the whole general population cohort to be derived for all measures including those available only in the intensive sample using methods described in the Statistical Analysis section.
Measures and procedure
CD at 32 weeks of pregnancy
The CD coding system was originally developed for family interactions (Velligan, Reference Velligan1985) and captures eight different types of communicational atypicalities that were identified in previous work on CD (Doane & Singer, Reference Doane and Singer1977; Singer & Wynne, Reference Singer and Wynne1965a, Reference Singer and Wynne1965b, Reference Singer and Wynne1966b; Wynne et al., Reference Wynne, Singer, Bartko, Toohey and Tanner1977; Wynne & Singer, Reference Wynne and Singer1963a, Reference Wynne and Singer1963b); namely:
1. Abandoned, abruptly ceased, uncorrected remarks;
2. Unintelligible remarks;
3. Contradictions, denials, and retractions;
4. Ambiguous referents;
5. Extraneous questions and remarks;
6. Tangential, inappropriate responses to questions or remarks;
7. Odd word usage or odd sentence construction; and
8. Reiterations.
Table 1 shows definitions and examples for the different codes. CD scores were calculated as the number of instances of CD divided by the number of words spoken to account for verbosity (as recommended by previous researchers; Hirsch & Leff, Reference Hirsch and Leff1971; Miklowitz & Stackman, Reference Miklowitz and Stackman1992). This coding protocol has been shown to have good reliability and construct validity (Velligan et al., Reference Velligan, Goldstein, Nuechterlein, Miklowitz and Ranlett1990), and has been previously used with clinical (Velligan, Funderburg, Giesecke, & Alexander, Reference Velligan, Funderburg, Giesecke and Alexander1995; Velligan et al., Reference Velligan, Miller, Eckert, Funderburg, True, Mahurin and Hazelton1996) and high-risk populations (Velligan et al., Reference Velligan, Christensen, Goldstein and Margolin1988). The system has also been previously applied to 5-min speech samples (Kymalainen, Reference Kymalainen2005; Kymalainen, Weisman, Rosales, & Armesto, Reference Kymalainen, Weisman, Rosales and Armesto2006), and to natural speech samples (Docherty, Reference Docherty1993).
Table 1. Definitions and examples of the communication deviance codes (Velligan, Reference Velligan1985).
The 5-min speech sample used in this study is an adaptation of the procedure developed for use with parents in which they are asked to talk about how they get along with their child (Magaña et al., Reference Magaña, Goldstein, Karno, Miklowitz, Jenkins and Falloon1986). The instructions for the original measure are “I'd like to hear your thoughts about [patient's name] in your own words and without my interrupting you with any questions or comments. When I ask you to begin, I'd like you to speak for 5 minutes, telling me what kind of a person [patient's name] is and how the two of you get along together. After you have begun to speak, I prefer not to answer any questions. Are there any questions you would like to ask me before we begin?” In adapting this for use in pregnancy, Lucassen et al. (Reference Lucassen, Tiemeier, Luijk, Linting, Bakermans-Kranenburg, van Ijzendoorn and Lambregtse-Van den Berg2015) changed the initial wording to “I would like you to tell me about your unborn child. What I would like to hear from you is what you expect or hope your child will be like and how you would like to relate to your child.” In view of the emphasis in the original version, the speakers’ view of the present rather than the future, we wrote a version that focused on the present and also was appropriate in pregnancy: “I would like to hear your thoughts and feelings about your baby at the moment, in your own words without me interrupting. When I ask you to begin, I would like you to speak for 5 minutes, tell me what your impressions have been of your baby whilst you've been pregnant.”
For purposes of training, the first (P.S.) and third authors (K.F.) both coded 31% (90) of the speech samples. This training period was preceded by the careful reading of relevant papers in the field of CD (Singer & Wynne, Reference Singer and Wynne1966b) and the coding manual that was kindly provided by its author (Velligan, Reference Velligan1985). Both coders were only provided with anonymized transcripts and audio-recordings (the only other information available was the participants id number), hence remaining blind to any background information about the mothers and study hypotheses. Following training, both coders independently scored a subset of 30 speech samples (~10%). Some of the CD codes were very infrequent (e.g., reiteration) but the estimated reliability was good (intraclass correlations for the different items ranged from .77 to .97). After reliability was established, the first author (P.S.) coded the remainder of the speech samples, including those used in the training. All coding of CD was conducted independently of the coding of maternal sensitivity and blind to all other measures.
Maternal sensitivity at 29 weeks
Maternal sensitivity was assessed with a 15-min standardized laboratory-based protocol (NICHD Early Child Care Research Network, 1999). Mothers were asked to play with their infants seated in a reclining chair or on the floor mat, as they would at home. The protocol started with the following prompt: “Play as you might usually do with your baby.”
During the initial 7 min, mothers were instructed to play with their babies using a toy of their choice. After this period, a researcher knocked on the door and instructed the mother to play for an extra 8 min with a set of standardized toys provided by the WCHADS team, resulting in a total of 15 min of video-recorded play. The camera was placed so that full-face view of the infant and the mother could be captured (to enable the team to code eye-to-eye contact between mother and infant).
Maternal sensitivity to distress and maternal sensitivity to nondistress were rated using a 5-point scale, ranging from 1 (not at all characteristic) to 5 (highly characteristic) reflecting mothers’ appropriate, supportive, warm responding to infant communications, playful bids, or distress.
An investigator from the NICHD Early Child Care Research Network trained the raters, who then coded sensitivity from the video recordings blind to all other study measures of this report. Each rater (K.A. and L.F.) achieved good interrater reliability for maternal sensitivity on a subset of 30 assessments (intraclass correlations ranged from .85 to .91). All ratings of maternal sensitivity were made by different coders than those who rated CD, and blind to all other measures.
The video recordings in which distress was observed were also rated for duration of distress (207 in total). The interrater reliability for distress duration on a subset of 20 recordings was .92 (intraclass correlations). The duration of distress varied across the sample (129.86 s; SD = 115.90), with the child spending an average of 14.7% (SD = 13.6%) of the 15 min of the assessment period distressed. The validity of the maternal sensitivity construct was explored by testing the association between sensitivity to distress and nondistress in each quartile of the distribution of the duration of distress (as a percentage of the assessment period). Correlations were all sizable and significant across the four quartiles (Spearman's correlations varied between .64 and .75) supporting the validity of the sensitivity to distress measure. A more detailed analysis can be found elsewhere (Wright, Hill, Sharp, & Pickles, Reference Wright, Hill, Sharp and Pickles2018).
Confounders
Maternal age, depression, and socioeconomic deprivation have been found to be associated with maternal sensitivity (Campbell, Matestic, von Stauffenberg, Mohan, & Kirchner, Reference Campbell, Matestic, von Stauffenberg, Mohan and Kirchner2007; Leerkes et al., Reference Leerkes, Weaver and O'Brien2012; Murray, Fiori-Cowley, Hooper, & Cooper, Reference Murray, Fiori-Cowley, Hooper and Cooper1996) and therefore were included as potential confounders. Although CD has been found to be unrelated to IQ and depression in previous studies (e.g., Doane, West, Goldstein, Rodnick, & Jones, Reference Doane, West, Goldstein, Rodnick and Jones1981; Velligan et al., Reference Velligan, Christensen, Goldstein and Margolin1988), this has not been tested in studies with samples similar to the WCHADS, and so maternal verbal IQ and depressive symptoms were accounted for in analyses with confounds.
Index of Multiple Deprivation (IMD)
Socioeconomic status was determined using the revised IMD (Noble et al., Reference Noble, Wright, Dibben, Smith, McLennan, Anttila and Lloyd2004). According to this system, postcode areas in England are ranked from the most deprived (IMD of 1) to the least deprived (IMD of 32,482) based on seven domains of inequality: income deprivation; employment deprivation; health deprivation and disability; education, skill, and training deprivation; barriers to housing and services; living environment deprivation; and crime. All mothers were ranked according to their area postal code and assigned to a quintile based on the UK distribution of deprivation.
Verbal IQ
Verbal IQ in mothers was measured with the Wechsler Test of Adult Reading (WTAR). The WTAR is a neuropsychological test that takes approximately 10 min to complete and that assesses premorbid intelligence through the use of 50 irregularly spelled words. During the test, the examiner presents a series of cards with the words prompting the participant for a single pronunciation of the word. The test is stopped when the participant gives 12 consecutive incorrect pronunciations. Each correct pronunciation is given a score of 1 with the maximum raw score of 50. The raw score is then standardized by age and education using published guidelines (Holdnack, Reference Holdnack2001). WTAR scores are strongly correlated with measures of verbal IQ, verbal comprehension, and full-scale IQ (Strauss, Sherman, & Spreen, Reference Strauss, Sherman and Spreen2006).
Maternal depression in pregnancy and at follow-up
Symptoms of depression were assessed with the Edinburgh Postnatal Depression Scale (EPDS; Cox, Reference Cox1996). The EPDS includes 10 items that cover different symptoms of depression (e.g., anhedonia, low mood, or thoughts of self-harm) in the last 7 days. Questions are answered on a 3-point severity scale, and total scores can range from 0 to 30. Scores above a threshold of 12 are likely to indicate clinical depression in the mother (Cox, Holden, & Sagovsky, Reference Cox, Holden and Sagovsky1987).
Statistical analysis
In order to make inference about the general population from our sample, we applied inverse probability weights that accounted for both the stratified sample and sample attrition associated with maternal age, education, depression score at booking and in pregnancy, smoking, and marital status (Dunn, Pickles, Tansella, & Vázquez-Barquero, Reference Dunn, Pickles, Tansella and Vázquez-Barquero1999). We then ran three separate linear regressions with the CD as the predictor variable for the three different maternal sensitivity scores (overall sensitivity and sensitivity in and out of the context of infant distress, with different weights to account for the fact that a substantial proportion of the infants did not become distressed during the observation). These analyses were carried out in a stepwise fashion with estimation of an initial unadjusted model and then with adjustment for confounders (i.e., maternal age, verbal IQ, and IMD quintile). As the sample size was somewhat reduced for analyses including prenatal and postnatal depression (see Table 2), they were included as additional confounds in separate analyses. Finally, we checked for nonlinearity in the association of CD and overall maternal sensitivity using a LOWESS regression smooth (Cleveland, Reference Cleveland1979) and a “bent-stick” regression that hypothesized that the association was limited to only part of the range of CD scores (Bacon & Watts, Reference Bacon and Watts1971). All analyses were carried out in Stata 13 by the fifth author (A.P.).
Table 2. Means and standard deviation for the key variables (unweighted)
Note: IMD, Index of Multiple Deprivation. EPDS, Edinburgh Postnatal Depression Scale. aNot all infants became distressed so sensitivity to distress is available for only a subset of mothers.
Results
Characteristics of the sample
Table 2 shows the mean and standard deviation for the key variables of the study. The mean age of the mothers was 26.96 years (SD = 5.96) and the mean IQ score was 105.68 (SD = 6.43). Regarding the IMD, mothers in the sample ranked on average in the second lowest quintile (2.29, SD = 1.3) consistent with the high levels of deprivation in the study catchment area. In Table 2, we also present the means and standard deviations for the depression and maternal sensitivity scores, the different CD codes, duration of speech samples, and word count.
The means and standard deviations for CD in our study are considerably lower than CD scores previously published by Kymalainen et al. (Reference Kymalainen, Weisman, Rosales and Armesto2006). However, in their study, the authors tested relatives of patients diagnosed with schizophrenia from different ethnic groups (White Americans: mean = 2.89, SD = 2.12; Afro-Americans: mean = 3.22, SD = 2.18; and Latinos: mean = 1.27, SD = 1.35).
CD and maternal sensitivity scores
Bivariate correlations between the study variables are provided in the online-only Supplementary Materials. Table 3 shows the summary of the regression analysis testing the associations between CD at 32 weeks gestation and the different maternal sensitivity scores at 29 weeks, before and after adjustment for confounders.
Table 3. Linear regression with communication deviance (CD) as a predictor of overall maternal sensitivity, sensitivity to nondistress, and distress before and after controlling for confounders (weighted for sample stratification and attrition)
Note: IMD, Index of Multiple Deprivation.
An initial regression with CD predicting overall maternal sensitivity score showed a highly significant association (p < .001), suggesting that a 1 SD increase in CD was associated with a 0.385 SD decrease in maternal sensitivity, 95% confidence interval (CI) [–0.567, –0.203]; F (1, 236) = 17.38; p < .001; R 2 = .078. The effect of CD on overall maternal sensitivity score remained significant (p < .005) after adjustment for confounders (maternal age, verbal IQ, and IMD quintile) despite the smaller estimated coefficient of –0.216, 95% CI [–0.365, –.067]. Of note is the significant association between the confounders and overall sensitivity scores (p values ranging from p < .001 to p = .015), especially maternal age. The inclusion of these confounders led to an overall improvement of the model, F (4, 233) = 19.30, p < .001; R 2 = .266.
In our second set of analyses, we repeated the same procedure but this time with the maternal sensitivity to nondistress as the outcome variable. The initial model, without confounders, revealed that CD was significant predictor of maternal sensitivity to nondistress: –0.311, 95% CI [–0.547, –0.076], p = .01. After adjustment for confounders, CD remained a significant predictor of sensitivity to nondistress: –0.185, 95% CI [–0.346, –0.024], p = .024. Again, the confounders were significantly associated with the outcome variable (p values ranging from p < .001 to p = .036) especially maternal age and verbal IQ. The overall model with all the variables proved to be highly significant explaining 24.7% of the observed variance, F (4, 233) = 17.65, p < .001, R 2 = .247.
In order to draw the comparison with sensitivity to nondistress, we then tested the association between CD and maternal sensitivity in the context of infant distress. In this analysis, the effect estimate, without adjustment for confounders, was not only significant but also substantially larger, –0.514, 95% CI [–0.767, –0.262], p < .01, than the one reported for the association between CD and maternal sensitivity to nondistress. After adjustment for confounders, CD remained a highly significant predictor (p < .001) despite the smaller estimate coefficient, –0.293, 95% CI [–0.421, –0.164]. However, in this model maternal age and verbal IQ were not significantly associated with maternal sensitivity in the context of infant distress (p = .257 and p = .243, respectively); only IMD quintile was (p = .006). Again, the overall model was highly significant, F (4, 176) = 11.36, p < .001; R 2 = .216.
CD and maternal sensitivity with maternal depression as a confounder
In order to explore the potential confounding effect of maternal depression on the association between CD and the maternal sensitivity scores, we ran another set of analyses additionally adjusting for mothers’ scores on the EPDS at 32 weeks of pregnancy and at 29 weeks postnatal.
For overall sensitivity, the N fell to 229, but the effect of CD remained significant, p = .023. For maternal sensitivity to nondistress, the N fell to 229, and the coefficient for CD was no longer significant, p = .094. Finally, for maternal sensitivity in the context of infant distress, the N fell to 173, but CD remained a highly significant predictor, p < .001. In none of the three cases did either depression score significantly predict sensitivity.
Testing nonlinearity in the association between CD and maternal sensitivity
Figure 1 shows the fitted regression model together with a nonlinear regression (locally weighted scatterplot smoothing; LOWESS). The LOWESS suggested that the association might be restricted to the upper end of the distribution of CD scores. A “bent-stick” regression was estimated, which allowed for the lower end of the distribution of CD scores to have no effect. The distribution is shown in Figure 1. This suggests that the point of inflection in the regression, though appearing quite close to the lower end of the range of raw scores, fell at the 48th percentile (close to the middle of the distribution) because of the skew of the distribution. The 95% confidence interval for this break point or threshold spanned from the 37th to the 60th percentile. A formal test of the superiority of this model in our stratified sample was not straightforward.
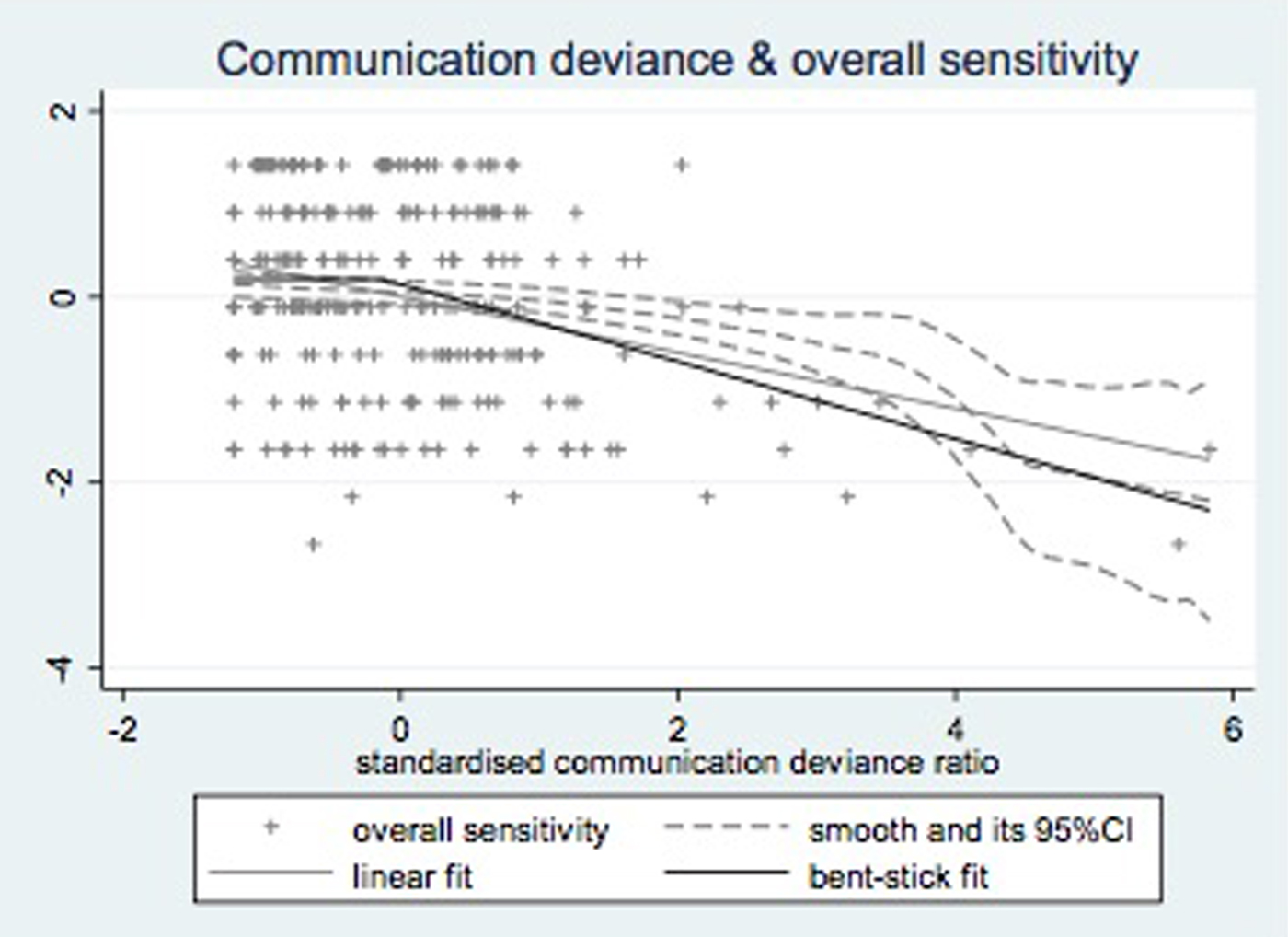
Figure 1. Regression model with LOWESS smooth, linear, and “bent-stick” fit.
Discussion
CD in first-time pregnant women, assessed as the use of confusing verbal constructions when describing their anticipated infants, predicted lower sensitivity to infant cues approximately 9 months later. This association was stronger in the context of their infant's distress rather than in a nondistress context, and it was greater over the upper range of the CD distribution. These associations were not accounted for by maternal depressive symptoms either during pregnancy or at the time of the sensitivity assessment. The findings could have implications for our understanding intergenerational transmission of developmental vulnerabilities, and for the study of processes that may influence both verbal and nonverbal parenting behaviors.
Previous research has suggested that maternal sensitivity in the context of infant's nondistress cues is significantly predicted by sociodemographic risk factors (Leerkes et al., Reference Leerkes, Weaver and O'Brien2012). Our analyses supported this assertion by revealing significant associations between maternal sensitivity to nondistress cues and maternal age, verbal IQ, and deprived living conditions. In contrast, maternal sensitivity in the context of infant distress may be more related to the emotional and cognitive competencies of the mother (e.g., negative emotions in response to infant crying or better skills at detecting infant distress; Leerkes, Reference Leerkes2010). The results of the present study suggest that CD and, generally speaking, communicational difficulties are associated with more basic early relational difficulties between mothers and their infants, particularly in emotionally stressful contexts, such as when there is a need to respond to the infant's distress.
The findings should be interpreted in the larger context of previous studies that have reported associations between disrupted communication during face-to-face interactions between caregivers and their infants, and caregivers’ difficulties in sensitively attuning to their 4-month-old's distress cues (Crockett, Holmes, Granger, & Lyons-Ruth, Reference Crockett, Holmes, Granger and Lyons-Ruth2013) and initiating and sustaining joint attention bids from the infant (Annie Yoon, Kelso, Lock, & Lyons-Ruth, Reference Annie Yoon, Kelso, Lock and Lyons-Ruth2014; Schechter et al., Reference Schechter, Willheim, Hinojosa, Scholfield-Kleinman, Turner, McCaw and Myers2010). Relevant in this context as well is the robust association observed in previous studies between a caregiver's disrupted communication (12 to 18 months) and disorganized attachment styles in children (Madigan et al., Reference Madigan, Bakermans-Kranenburg, van Ijzendoorn, Moran, Pederson and Benoit2006). In these studies, disrupted communication was conceptualized as the caregiver's failure to grasp and respond to the intentions conveyed in the infant's communication. It therefore seems likely that disrupted communication and CD reflect broader impairments in the cognitive and emotional processes that are important in attuning to and responding to infant distress (Leerkes & Crockenberg, Reference Leerkes and Crockenberg2006).
A possible interpretation of our results is that both maternal CD and low maternal sensitivity reflect limitations in “mentalizing” (the ability to think about the mental states of others). For example, it has been argued that mentalizing is important for repairing misunderstandings during conversation (e.g., clarifying deictic references that the listener finds ambiguous or vague) and that both mentalizing and alignment, although dissociable processes, contribute to successful communication (Brennan, Galati, & Kuhlen, Reference Brennan, Galati and Kuhlen2010). Consistent with this hypothesis, “maternal mind-mindedness,” defined in terms of the caregivers’ ability to “read” their infants’ thoughts and feelings accurately during play and to comment on their internal states in an attuned way, has been found to be an important predictor of children's sociocognitive development (Meins et al., Reference Meins, Fernyhough, Wainwright, Das Gupta, Fradley and Tuckey2002, Reference Meins, Fernyhough, Wainwright, Clark-Carter, Das Gupta, Fradley and Tuckey2003).
Our findings therefore broaden the possible range of interpretations of the associations between parental CD and poor social and emotional outcomes in children (e.g., Wichstrøm, Anderson, Holte, Husby, et al., Reference Wichstrøm, Anderson, Holte, Husby and Wynne1996; Wichstrøm, Anderson, Holte, & Wynne, Reference Wichstrøm, Anderson, Holte and Wynne1996) and psychopathology in adults (de Sousa et al., Reference de Sousa, Varese, Sellwood and Bentall2014), outlined earlier. If parental CD is a stable trait, it is possible that the associations we have observed reflect an intergenerational process in which prenatal CD is linked to low maternal sensitivity in infancy, which is a key developmental influence on later adjustment. If this is the case, there are implications not only for the timing of the effects of CD but also for the mechanisms. Associations between CD and child mental health outcomes are typically interpreted as effects of verbal communication on the verbal child. However, our findings offer the alternative possibility that CD is a marker for nonverbal communication patterns during infancy, and also possibly during childhood, which also influence development. Further research is required to address questions raised by this possibility. For example, to what extent is CD regarding an anticipated infant in pregnancy a “traitlike” reflection of a tendency to speak in this way about people in general, or does CD vary depending on the person the speaker is referring to?
Important strengths of this study included that both the predictor and the outcome measures were based on observation, and coded by independent raters, blind to all other measurement, and that potential confounding effects of maternal depression were accounted for. Assessment of CD during pregnancy eliminated the possibility of evocative effects of infant behavior on the parent, a weakness previously identified in the CD literature (Miklowitz & Stackman, Reference Miklowitz and Stackman1992). A limitation of the study is that we were not able to rule out some plausible confounds such as previous trauma or current stressors experienced by the mothers. While the case was made earlier that elevated expressed emotion, and coherence of attachment representations, are different constructs, the extent of their overlap with CD is unknown, and controlling for them may have altered the association between CD and maternal sensitivity. Five-minute speech samples are not an everyday conversation; they reflect soliloquies rather than dialogues, and it could be argued that CD scores were confounded by the constraints of the experimental condition (e.g., anxiety and self-consciousness). Furthermore, the version of the 5-min speech sample used in this study is an adaptation from the original, which refers to the relationship between a parent and a living child, which may limit the generalizability of the findings.
Thus far, research on CD has been largely carried out by researchers interested in environmental and developmental influences on later psychopathology, especially schizophrenia (Bentall, Reference Bentall2003; Bentall et al., Reference Bentall, de Sousa, Varese, Wickham, Sitko, Haarmans and Read2014; Bentall & Fernyhough, Reference Bentall and Fernyhough2008; de Sousa et al., Reference de Sousa, Varese, Sellwood and Bentall2014). The present findings suggest that CD may be a useful concept in understanding the impact of maternal characteristics on early child development. Future studies should examine maternal characteristics associated with CD and its associations with a wider range of developmental processes in children.
Acknowledgments
This study was funded by UK Medical Research Council Grant G0400577 (to J.H. and H.S.) and Fundação para a Ciência e a Tecnologia Grant SFRH/BD/ 77379/2011 (to P.S.). This work was also supported by Wirral University Teaching Hospital NHS Foundation Trust, Cheshire and Wirral Partnership NHS Foundation Trust and Wirral Community NHS Foundation Trust, the NIHR Biomedical Research Centre for Mental Health at the South London and Maudsley NHS Foundation Trust, and King's College London. The views expressed are those of the authors and not necessarily those of the funders, the NHS, theNIHR or the UK Department of Health. The authors would like to thank Professor Dawn Velligan for advice on the assessment of communication deviance. We are very grateful to all participating families and to the research staff who contributed to this work.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579418001189







 Open access
Open access