



No CrossRef data available.
Published online by Cambridge University Press: 15 November 2022
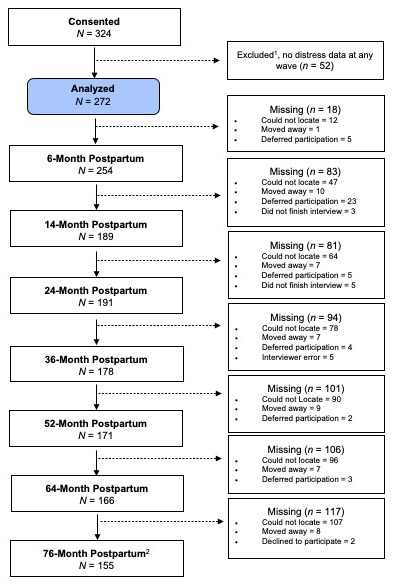
A substantial body of work has established that mothers’ internalizing distress can negatively affect children’s socioemotional development. Yet few studies have examined how distinct patterns of mothers’ distress over time differentially impact child behaviors across early childhood. To address this gap, the current study explored developmental trajectories of mothers’ internalizing distress and examined the associations of these patterns with child adjustment outcomes. Mexican immigrant, Dominican immigrant, and African American mothers (N = 272) were annually assessed for internalizing distress over the first 6 years following childbirth. Children’s psychological adjustment (internalizing, externalizing, and hyperactivity behaviors) was measured at the last yearly assessment in first grade. A growth mixture model revealed two distinct classes of distress where mothers were classified as having low stable distress (82.4%) or moderate distress that began as stable then declined when their children were 64 months old (17.6%). Children of mothers in the moderate, late decline class showed greater internalizing, externalizing, and hyperactivity behaviors in the first grade compared to children of mothers in the low stable class. Findings highlight the necessity of supporting the mental health of ethnic minoritized mothers following childbirth and further expand our knowledge of family psychopathology to promote healthy psychological adjustment in children.

Osornio et al. supplementary material 1

Osornio et al. supplementary material 2
