



Introduction
For some children, displaying disruptive behavior in childhood can lead to persistent and increasingly negative outcomes in adulthood (Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008). Early disruptive behavior is related not only to future criminal behavior, but also to other negative outcomes such as substance abuse and psychiatric illness (Fombonne et al., Reference Fombonne, Wostear, Cooper, Harrington, Rutter and Alcaraz2001). However, not all children who exhibit disruptive behavior mature into adult offenders (Odgers et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007) and there might be individual or environmental factors that influence remission of disruptive behavior symptoms. One individual factor is difficulty in emotion recognition (Marsh & Blair, Reference Marsh and Blair2008). Interventions that target emotion recognition may help to deflect an individual from an antisocial developmental trajectory. The current paper reports on the efficacy of a computerized intervention that aims to improve emotion recognition.
The Research Domain Criteria (RDoC; National Institute of Mental Health; Insel et al., Reference Insel, Cuthbert, Garvey, Heinssen, Pine, Quinn and Wang2010) approach advocates the need to study transdiagnostic processes underlying mental health problems, and promotes the development of interventions based on core mechanisms. Emotion recognition problems are a common precursor of adult psychopathology (Copeland, Shanahan, Costello, & Angold, Reference Copeland, Shanahan, Costello and Angold2009). Being able to detect, process, and respond appropriately to the emotions of others is crucial for normal social interaction and helps to initiate and maintain healthy social relationships (Izard et al., Reference Izard, Fine, Schultz, Mostow, Ackerman and Youngstrom2001). Aptitude in emotion recognition helps to initiate and maintain healthy social relationships; individuals who are proficient in emotion recognition are more socially competent and function more effectively in social situations (Izard et al., Reference Izard, Fine, Schultz, Mostow, Ackerman and Youngstrom2001); they are also more popular and rated by others as more socially skilled (Edwards, Manstead, & MacDonald, Reference Edwards, Manstead and MacDonald1984). Distress cues, such as facial expressions of fear or sadness, are social reinforcers that condition individuals to avoid engaging in distress-causing behavior (Marsh & Blair, Reference Marsh and Blair2008); a failure to understand or interpret distress cues will almost certainly compromise the development of socially appropriate behavior (Fairchild, van Goozen, Calder, Stollery, & Goodyer, Reference Fairchild, van Goozen, Calder, Stollery and Goodyer2009).
Emotion recognition problems are prominent in antisocial populations, including in both adults and children (Marsh & Blair, Reference Marsh and Blair2008). On average, such individuals have difficulty in recognizing negative emotions, particularly fear and sadness, from others’ facial expressions, while the recognition of happiness is relatively unimpaired (Bowen, Morgan, Moore, & van Goozen, Reference Bowen, Morgan, Moore and van Goozen2014; Dawel, O'Kearney, McKone, Palermo, & O'Kearney, Reference Dawel, O'Kearney, McKone, Palermo and O'Kearney2012; Fairchild et al., Reference Fairchild, van Goozen, Calder, Stollery and Goodyer2009). However, there is considerable individual variability in emotion recognition ability (Eugène et al., Reference Eugène, Lévesque, Mensour, Leroux, Beaudoin, Bourgouin and Beauregard2003), in part due to the wide range of responses that emotional stimuli evoke (Hamann & Canli, Reference Hamann and Canli2004).
A potential explanation for emotion recognition impairments is that these are caused by reduced gaze towards the eye region, another transdiagnostic process (Dadds et al., Reference Dadds, Perry, Hawes, Merz, Riddell, Haines and Abeygunawardane2006). However, recent evidence has cast doubt on this (Airdrie, Langley, Thapar, & van Goozen, Reference Airdrie, Langley, Thapar and van Goozen2018; Martin-Key, Graf, Adams, & Fairchild, Reference Martin-Key, Graf, Adams and Fairchild2017; van Zonneveld, Platje, de Sonneville, van Goozen, & Swaab, Reference van Zonneveld, Platje, de Sonneville, van Goozen and Swaab2017), finding no evidence of an impairment in attention to the eyes in children or adolescents with externalizing behavioral problems. This evidence prompts the need for further investigation into the role of eye gaze in emotion recognition impairments.
Given the importance in psychopathology of the ability to recognize the emotions of others, interventions to address emotion recognition impairments can play an important role. Penton-Voak and colleagues (Penton-Voak et al., Reference Penton-Voak, Thomas, Gage, McMurran, McDonald and Munafò2013) completed a computerized program with juveniles with histories of frequent aggressive behavior and/or criminal records. They aimed to modify the hostility bias, which is a tendency to interpret benign or neutral information as hostile. The program modified automatic tendencies to interpret ambiguous expressions as anger by adjusting the balancing point of when an ambiguous face is classified as angry versus happy. They were successful in reducing a hostility bias in aggressive youths and recorded a decrease in independently rated aggressive behavior two weeks later. However, their study focused only on anger, whereas the emotions that are most commonly impaired are fear and sadness (Marsh & Blair, Reference Marsh and Blair2008). Dadds, Cauchi, Wimalaweera, Hawes, and Brennan (Reference Dadds, Cauchi, Wimalaweera, Hawes and Brennan2012) completed the MindReading intervention with clinic-referred children and adolescents. This involved daily parent–child interactional exercises and therapist sessions with the computerized MindReading program. They found that children with callous–unemotional (CU) traits showed improvements in conduct problems, as rated by their mothers, following the program. However, there was no improvement in emotion recognition, so it remains unclear what led to the improvements in conduct problems. Hubble, Bowen, Moore, and van Goozen (Reference Hubble, Bowen, Moore and van Goozen2015) examined the influence of emotion recognition training on objective crime data. They used a computerized program to direct attention to relevant facial features in three sessions. They found that juvenile offenders’ ability to recognize negative emotions significantly improved following a short but intensive training. In addition, the severity of their criminal behavior significantly decreased in the six months following the training. However, this study was conducted with juveniles and we currently do not know the effect of emotion recognition training in children displaying disruptive behavior.
Although these studies suggest that emotion recognition training has beneficial effects, some issues still need to be addressed (Hunnikin & van Goozen, Reference Hunnikin and van Goozen2018). First, emotion recognition is a process that is likely to vary across individuals within diagnostic categories (Insel et al., Reference Insel, Cuthbert, Garvey, Heinssen, Pine, Quinn and Wang2010). Allocation to training should therefore be determined by evidence of impairment in this ability, as assessed in an emotion recognition task. If an individual does not present with impairments, then an intervention is likely to be unnecessary. A targeted intervention approach is likely to be more effective and represents a better use of time and financial resources (van Goozen & Fairchild, Reference van Goozen and Fairchild2008; Wilkinson, Waller, & Viding, Reference Wilkinson, Waller and Viding2015). Second, no study to date has examined the role of eye gaze in emotion recognition training. Although eye gaze is thought to be a key process in emotion recognition because of the role that the eyes play in providing emotionally significant information (Jack, Blais, Caldara, Scheepers, & Caldara, Reference Jack, Blais, Caldara, Scheepers and Caldara2010), questions remain about the role of attention to the eye region, given recent evidence (Airdrie et al., Reference Airdrie, Langley, Thapar and van Goozen2018).
The current study aimed to address these outstanding issues. Children with disruptive behavior who were enrolled in an early intervention program to prevent antisocial and criminal outcomes completed an emotion recognition task with concurrent eye tracking. Only those who showed an impairment in emotion recognition completed the Cardiff Emotion Recognition Training (CERT; https://emotionrecognition.cardiff.ac.uk/info/videos/); those who did not have an emotion recognition impairment continued to receive their usual support. Emotion recognition and eye tracking assessments were repeated again with all children. The outcome measures were therefore emotion recognition scores for five emotions (happy, sad, fear, anger, and neutral) and proportion of time spent looking at the eyes during emotion recognition tasks.
It is important to explain the rationale underlying the design of this study. Targeted interventions are likely to be more effective (van Goozen & Fairchild, Reference van Goozen and Fairchild2008; Wilkinson et al., Reference Wilkinson, Waller and Viding2015) and not all individuals within a diagnostic category will show the same impairments (Insel et al., Reference Insel, Cuthbert, Garvey, Heinssen, Pine, Quinn and Wang2010). Therefore, we allocated children to receive the training based on evidence of emotion recognition impairments; if a child showed emotion recognition impairments, they received the intervention, and if they did not show an impairment, they were judged not to need the training. When analyzing the emotion recognition scores of the children who did not show an impairment, they were statistically comparable to a group of typically developing children (Hunnikin, Reference Hunnikin2018; Hunnikin, Wells, Ash, & van Goozen, Reference Hunnikin, Wells, Ash and van Goozen2019), with high mean accuracy scores ranging between 86% and 94%, thus not needing the intervention. An additional important aspect of this study is that all children who showed emotion recognition impairments received the CERT, instead of being randomly allocated to receive or not receive the CERT. Given that this was the first time the CERT was being used, it was important to assess the effectiveness of it in improving emotion recognition in a relatively large sample of children. If proven to be effective, a next step would be to randomly assign children with disruptive behavior and impairments in emotion recognition to receive or not receive the CERT. For now, the purpose of this study was to show that the CERT can improve emotion recognition and to examine the relationship between emotion recognition and eye gaze.
To show the importance of targeting the intervention to a child's needs, we hypothesized that emotion recognition would vary in children with disruptive behavior and would be related to the severity of disruptive behavioral problems. We also predicted that participation in the CERT would result in an improved emotion recognition, especially for negative and neutral facial expressions. Given the mixed evidence regarding the role of eye gaze in emotion recognition, we had no prediction concerning the relation between these variables, or how our measure of attention would be affected by the emotion training.
Method
Ethics statement
The study was approved by the Cardiff University School of Psychology Research Ethics Committee. Written informed consent was obtained from parents/guardians and teachers, and written informed assent was obtained from children.
Participants
Ninety-two children (74 male) between 7 and 11 years old (M = 8.8 years, SD = 1.12 years) from the Early Intervention Hub, a crime prevention program set up by Northamptonshire Police Force in the UK, were referred into the study. Children in the Hub were those deemed to be at risk for future antisocial and/or criminal behavior. Although the children had no formal clinical diagnosis, they showed considerable disruptive behavior and had been exposed to several risk factors associated with future criminal behavior (e.g., parental mental illness, domestic violence, and/or family member in prison; Children's Commissioner for London England, 2018). Children were referred into the Hub through a multiagency process, which included social workers, school officials, and police officers (Hunnikin et al., Reference Hunnikin, Wells, Ash and van Goozen2019).
As part of the Hub, Police Community Support Officers (PCSOs) are assigned to primary (i.e., elementary) schools to work with the children and their families. The child's PCSO or family support worker referred children into the current study. The child's teacher confirmed the child's behavioral status using the Strengths and Difficulties Questionnaire (SDQ; Goodman, Reference Goodman1997). Eligible children scored ≥3 out of 10 for conduct or peer problems or ≤5 out of 10 for prosocial behavior. These scores are based on the SDQ scoring and represent “slightly raised” conduct or peer problems and “slightly lowered” prosocial behavior (Goodman, Reference Goodman1997). It is estimated that only 20% of the UK population would be classified as slightly raised/lowered or above/below on these subscales (Goodman & Goodman, Reference Goodman and Goodman2011). In the current sample, 70% and 67% of children were classified as slightly raised or above for conduct or peer problems, respectively, while 67% were classified as slightly lowered/below for prosocial behavior. Twenty-three per cent of the sample met the criteria for one SDQ subscale, 50% met the criteria for two subscales, and 27% met the criteria for three subscales. An exclusion criterion was an estimated IQ of less than 70. Fourteen children were excluded from the study based on the SDQ and IQ eligibility criterion. A further seven children were excluded because they did not complete a posttest assessment; this was typically due to the child being unavailable due to moving schools.
To ensure a targeted approach to intervention, children were classified by emotion recognition ability after completing an emotion recognition test. Those scoring less than or equal to 66.67% for the recognition of sadness, and/or fear, and/or anger were assigned to the “disruptive behavior with emotion recognition impairments” group (DB+, n = 54, 59%), and completed the CERT. The threshold for identifying an emotion recognition impairment represents 1.5 standard deviations below the average performance of a sample of typically developing children (Hunnikin et al., Reference Hunnikin, Wells, Ash and van Goozen2019). The remaining children were assigned to the “disruptive behavior without emotion recognition impairments” group (DB−, n = 38, 41%); although they did not receive the CERT, they continued to receive their usual intervention support from the Hub.
Materials
Demographic and behavioral characteristics
The two-subtest Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, Reference Wechsler1999) provided an estimated IQ score. Socioeconomic status (SES) was estimated using the Office of National Statistics estimates of average household total weekly income based on each participant's postcode (Low = £0–£520; Middle = £521–£670; High = £671+).
The SDQ is a 25-item questionnaire assessing problematic and prosocial behavior (Goodman, Reference Goodman1997). It is scored on a three-point scale (0, 1, 2), giving a sum of between 0–10 for each 5-item subscale, along with an overall total difficulties score (out of 40, after removal of prosocial subscale). A score between 19 and 40 for “total difficulties” indicates an increased risk for developing a mental health disorder. For the purposes of this study, we focused on conduct, peer, and total problems, together with prosocial behavior, given that these behaviors are most commonly associated with emotion recognition problems (Marsh & Blair, Reference Marsh and Blair2008). Teachers completed the SDQ before the children took part in the study and they were blind to the interventions received.
Facial emotion recognition
The facial emotion recognition (FER; Bowen et al., Reference Bowen, Morgan, Moore and van Goozen2014) measure consisted of 60 photographs of males and females of varying ethnicities and ages, including children, displaying four emotions (happiness, sadness, fear, and anger) plus a neutral expression. The photographs came from the Radboud Faces Database (Langner et al., Reference Langner, Dotsch, Bijlstra, Wigboldus, Hawk and van Knippenberg2010). Children viewed the faces on a laptop. For the first three seconds, the face was presented alone and then with the question “what emotion (if any) is this person showing?” along with the five response options (see Figure 1). Children were asked to indicate their response on the computer by using the mouse to click the emotion label, selecting the appropriate key press (e.g., 1 – happy). Children could only choose one response option and there was no time limit to provide a response; they could change their response if the photograph was still displayed on the screen. The same stimuli were used in the pre- and posttests and children received no feedback about their performance. Although the researchers were not blind to the child's group allocation, they were not involved in the delivery of the CERT and children completed the recognition tasks without interacting with the researcher.
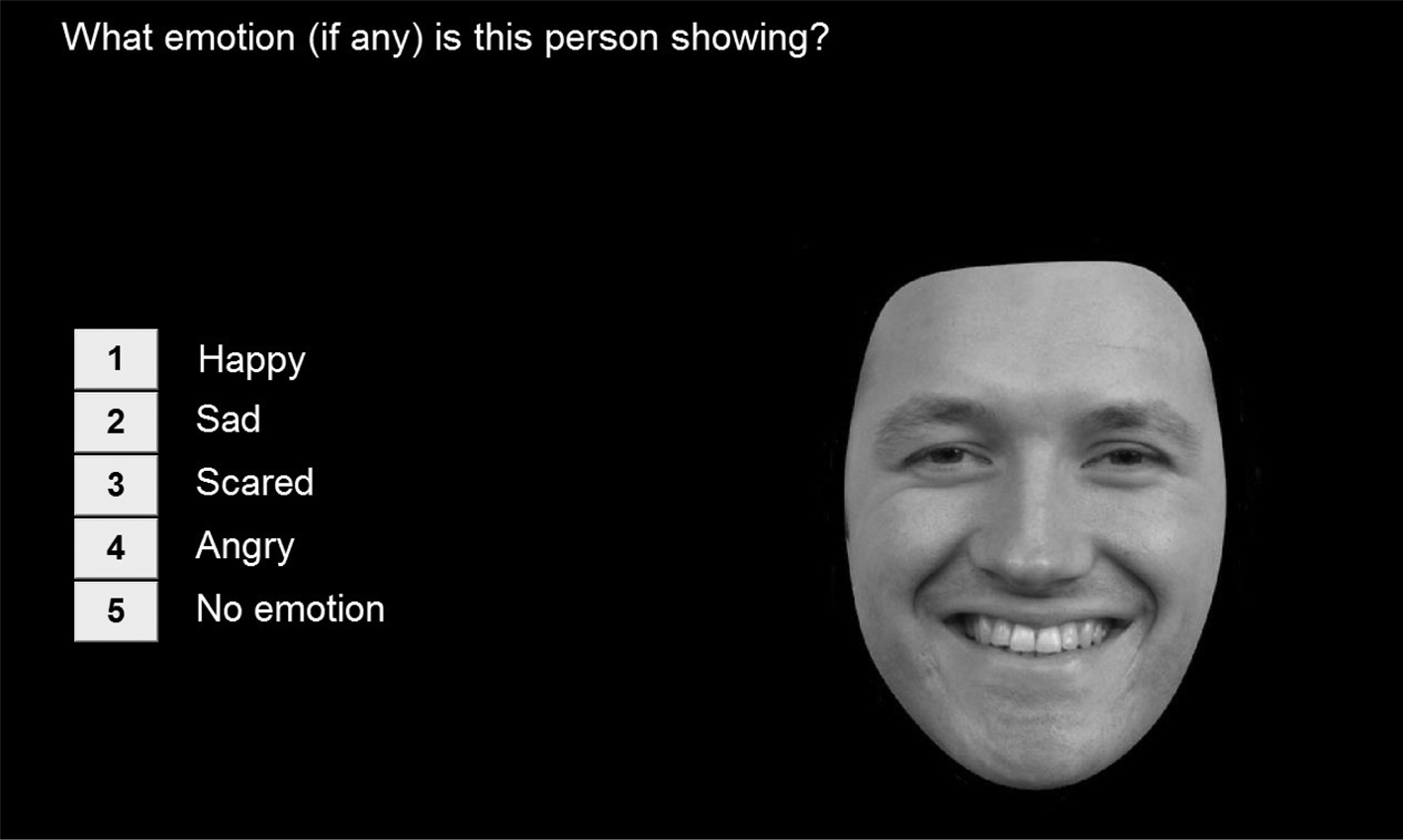
Figure 1. Example of a screen from the facial emotion recognition (FER) task.
Eye tracking
For practical reasons relating to the availability of the eye tracker, eye tracking was only assessed in a subsample of children (DB−: n = 27; DB+: n = 26). This subsample consisted of children who were randomly allocated to one of the two researchers collecting the data for this study. A portable Tobii X2-60 compact eye tracker sampling at 60 Hz with a screen resolution of 1920 × 1080 was used. Children were positioned 60–65 cm away from the 15″ laptop screen. Calibration quality was checked and repeated, if necessary. An I-VT fixation filter with a minimum fixation criterion of 60 msec sampled average raw data of both eyes to produce information on eye position and duration. Eye-gaze validity was checked for all recordings using a sample rate percentage that gives an estimate of the quality of eye tracking by providing a percentage score of successfully recorded data. Where this could not be confirmed, individual recordings were further analyzed. Overall, the validity ranged from 60% to 99% (mean accuracy: 80%). Total fixation time to the eyes of the presented faces was recorded.
Cardiff Emotion Recognition Training (CERT)
The CERT is a computerized intervention designed to improve the identification of facial expressions of happiness, sadness, fear, and anger (see Figure 2). The website for the CERT can be found here: https://emotionrecognition.cardiff.ac.uk/index.php. In addition to improving emotion recognition, the CERT aims to (a) improve the ability to understand when certain emotions are shown, (b) improve the understanding that someone can have more than one emotion in response to the same situation, and (c) provide an understanding of how it is appropriate to respond to someone displaying a certain emotion.
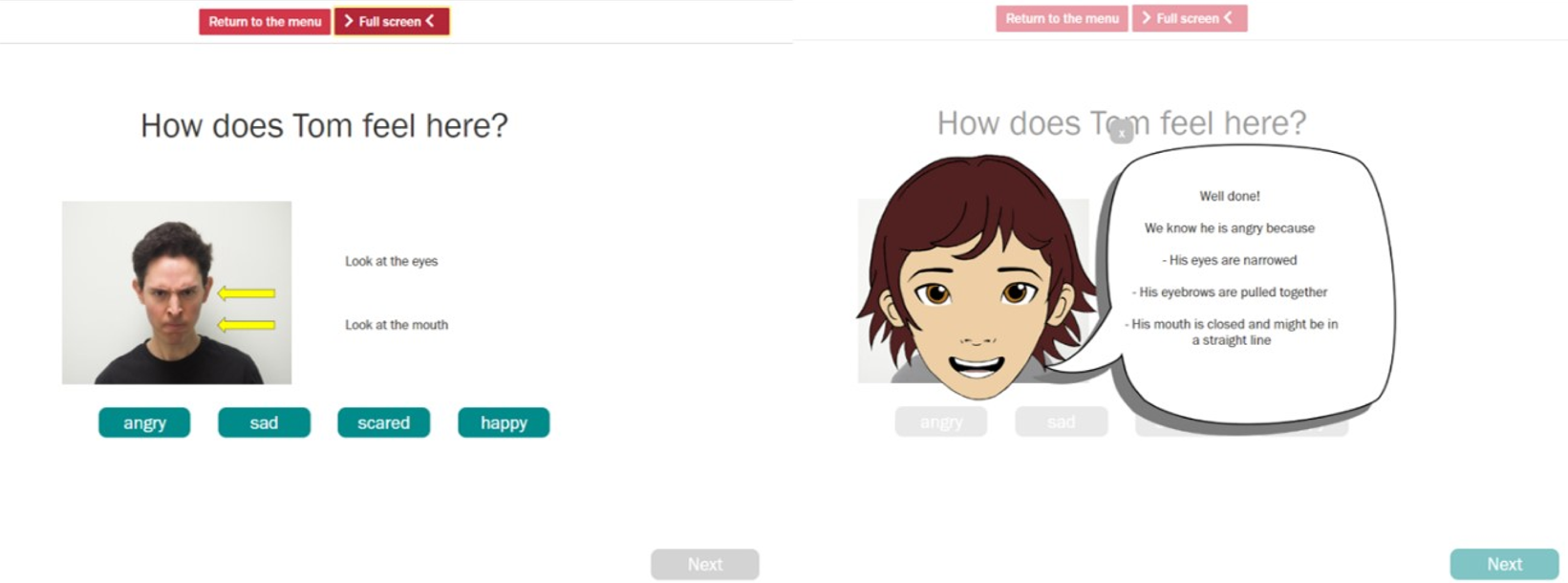
Figure 2. Screenshot from the Cardiff Emotion Recognition Training (CERT).
The CERT was created for the purpose of this study and has not been used previously. However, its design and content is based upon a previous training program (Neumann, Babbage, Zupan, & Willer, Reference Neumann, Babbage, Zupan and Willer2014) used by Hubble et al. (Reference Hubble, Bowen, Moore and van Goozen2015). Because Hubble et al.'s intervention was used with juveniles with a mean age of 16 years, the CERT was adapted to be suitable for use with young children. The changes involved photos, items, and activities suitable for younger children. This means that the CERT has not been used previously but is nevertheless based on previous research. The CERT was developed because the training used by Penton-Voak et al. (Reference Penton-Voak, Thomas, Gage, McMurran, McDonald and Munafò2013) only involves anger, whereas we know that other emotions are more commonly impaired, specifically fear and sadness (Marsh & Blair, Reference Marsh and Blair2008). Furthermore, the intervention used by Hubble et al. has been shown to improve emotion recognition, whereas the one by Dadds et al. (Reference Dadds, Cauchi, Wimalaweera, Hawes and Brennan2012) did not improve emotion recognition.
The activities within the CERT direct attention to key facial features for each emotional expression and provide hints to assist with the interpretation of such features. Further details about the activities within the CERT can be found in the program manual, which can be accessed at https://emotionrecognition.cardiff.ac.uk/info/.
The training consists of three 30-minute sessions. The sessions become progressively harder due to a reduction in the intensity of the facial expressions and in the number of hints given. Different target persons are used in order to expose children to a range of faces and varying levels of emotional displays. Target persons vary in gender, ethnicity, and age and include children for the final training session.
Procedure
The study was completed at the child's school, during school hours; children were removed from their lesson to participate in the study and all teachers agreed to this. In the pretest session, children completed the FER with concurrent eye tracking. Scores on the FER task were generated and examined postsession to establish whether the child did or did not have emotion recognition impairment. The family support worker or PCSO carried out the three CERT sessions with the children assigned to the DB+ group. In the posttest research session, children repeated the emotion recognition test (with concurrent eye tracking for a subsample) with the same researcher who completed the pretest research session (see Figure 3).
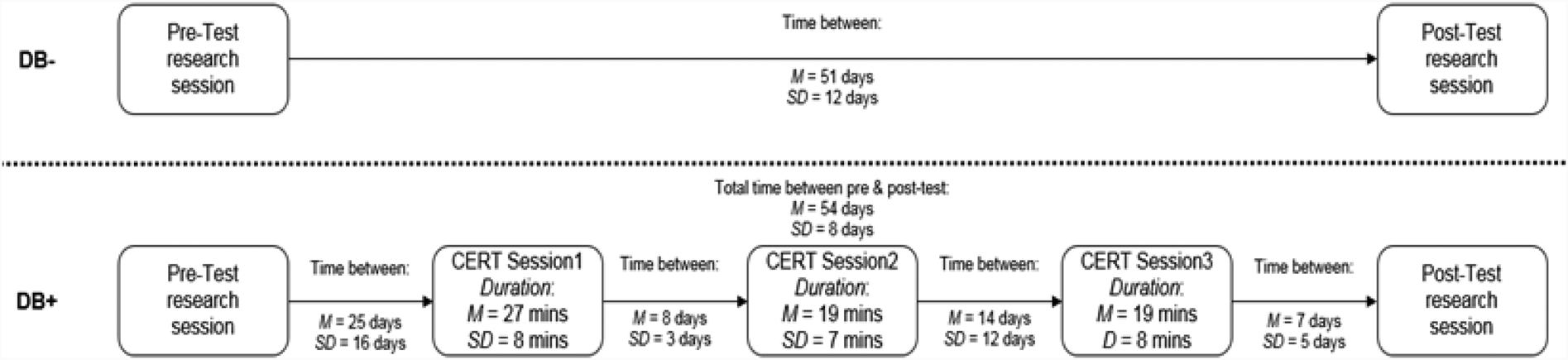
Figure 3. Schematic representation of the research procedure.
Children in the DB− group also completed the pre- and posttest research sessions but did not receive the CERT; however, they continued to receive their usual intervention support from family support workers or PCSOs.
Statistical analyses
Demographic and behavioral variables
Differences in demographic and behavioral characteristics between groups were analyzed using t tests for continuous variables and χ2 tests for binary variables. To reduce the number of analyses, average percent correct scores were calculated for negative emotions and then correlated with the pretest SDQ scores, using Spearman's correlations.
Emotion recognition
Percent correct for each emotion in the FER task was calculated and entered into a three-way mixed analysis of variance (ANOVA) (within-subjects factors: emotion and time; between-subjects factor: group). Where follow-up tests were required, Bonferroni correction was applied. Effect sizes for ANOVAs were calculated as partial eta squared $\lpar {\rm \eta }_{\rm p}^2 \rpar$ .
.
Eye gaze
Tobii Studio was used to analyze eye gaze. Areas of interest (AOIs) were created around the eyes, mouth, face as a whole, and the entire screen for the emotion recognition task (see Figure 4). While the other AOIs were created, the present analysis focuses on the eyes AOI because of the hypothesized importance of attention to the eyes in emotion recognition (Dadds et al., Reference Dadds, Perry, Hawes, Merz, Riddell, Haines and Abeygunawardane2006). Percentage dwell time to the eyes was calculated by summing all fixations to the eyes divided by the total duration of time spent looking at the face. This reflects the percentage of time that the children spent looking specifically at the eyes when they were looking at the face. A three-way mixed ANOVA (within-subjects factors: emotion and time; between-subjects factor: group) was conducted and where follow-up tests were required, Bonferroni correction was applied. The relationship between negative emotion recognition and eye gaze at pre- and posttest was also assessed using Spearman correlations.
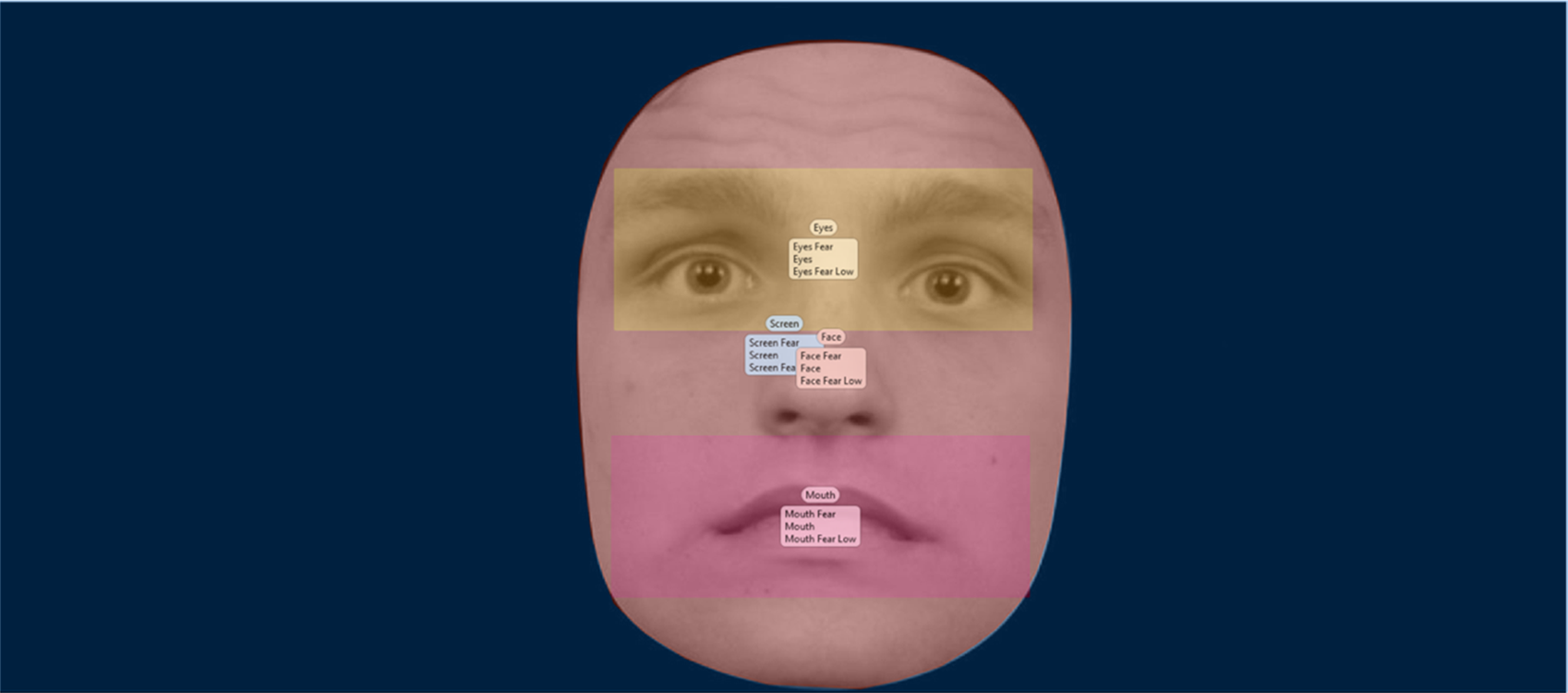
Figure 4. Example of areas of interest for the emotional stimuli included in the facial emotion recognition (FER) task.
Covariates
Although the DB+ and DB− groups differed in IQ (see Table 1), IQ was not significantly correlated with negative emotion recognition at pretest (r = .20, n = 92, p = .06); nor did IQ predict negative emotion recognition at posttest, F (1, 91) = 2.996, p = .087, adj. R2 = .02. A hierarchical regression analysis showed that emotion recognition ability (FER scores) significantly predicted behavioral problems, ß = −.334, p < .001, when controlling for IQ. IQ was therefore not controlled for in the three-way mixed ANOVAs reported below (but see footnote 1).
Table 1. Demographic and behavioral characteristics of participants

Notes: Standard deviations in parentheses. IQ = intelligence quotient (two-subtest WASI); SES = socioeconomic status; SDQ = Strengths and Difficulties Questionnaire.
Results
Demographic and behavioral data
The majority of children in both groups were male (DB− 84% and DB+ 78%) and White British (DB− 68% and DB+ 78%). At pretest, the two groups did not statistically differ in age, gender, SES, prosocial behavior, or conduct problems (see Table 1). However, children in the DB− group had a significantly higher IQ, and lower scores on the peer and total problems SDQ subscales than children in the DB+ group. There were no gender differences in emotion recognition accuracy, t (90) = −.41, p = .68.
Relationship between emotion recognition and disruptive behavior at pretest
Spearman correlations were conducted to establish the role of emotion recognition in severity of disruptive behavior. Consistent with expectations, the recognition of negative emotions was significantly negatively correlated with total SDQ scores (r = −.30, n = 92, p = .003), and SDQ peer problems (r = −.32, n = 91, p = .002) in particular. Negative emotion recognition was not significantly correlated with SDQ conduct problems (p = .56) at pretest.
Emotion recognition
There was a statistically significant three-way interaction between time, emotion, and group, F (3.49, 313.74) = 3.71, p = .008, ${\rm \eta }_{\rm p}^2$ = .04. The two-way interaction between time and emotion was statistically significant for the DB+ group only, F (3.23, 171.40) = 5.79, p = .001. Follow-up analyses showed that there was no significant improvement in happiness recognition for either the DB+ or DB− group (both ps > .05). However, the DB+ group significantly improved in their recognition of sadness, F (1, 53) = 9.71, p = .003 ${\rm \eta }_{\rm p}^2$
= .04. The two-way interaction between time and emotion was statistically significant for the DB+ group only, F (3.23, 171.40) = 5.79, p = .001. Follow-up analyses showed that there was no significant improvement in happiness recognition for either the DB+ or DB− group (both ps > .05). However, the DB+ group significantly improved in their recognition of sadness, F (1, 53) = 9.71, p = .003 ${\rm \eta }_{\rm p}^2$ = .16, fear, F (1, 53) = 38.56, p < .001, ${\rm \eta }_{\rm p}^2$
= .16, fear, F (1, 53) = 38.56, p < .001, ${\rm \eta }_{\rm p}^2$ = .42, anger, F (1, 53) = 37.96, p < .001 ${\rm \eta }_{\rm p}^2$
= .42, anger, F (1, 53) = 37.96, p < .001 ${\rm \eta }_{\rm p}^2$ = .42, and neutral expressions, F (1, 53) = 19.75, p < .001 ${\rm \eta }_{\rm p}^2$
= .42, and neutral expressions, F (1, 53) = 19.75, p < .001 ${\rm \eta }_{\rm p}^2$ = .27 (see Figure 5). In the DB− group, there was no significant change in emotion recognition across time for any emotion (all ps > .05).Footnote 1
= .27 (see Figure 5). In the DB− group, there was no significant change in emotion recognition across time for any emotion (all ps > .05).Footnote 1

Figure 5. Mean emotion recognition scores for expressions of happiness, anger, sadness, fear, and neutral at pre- and posttest. Error bars are set at ±1 standard error. *p < .05. DB: disruptive behavior.
Because FER scores were not normally distributed, we also run this analysis on transformed variables, after applying a reflect and square root transformation. The results were similar: the three-way interaction between time, emotion and group was significant, F (4, 360) = 2.94, p = .020, ${\rm \eta }_{\rm p}^2$ = .03, and the simple two-way interaction between time and emotion was significant for the DB+ group only, F (4, 212) = 6.32, p < .001.
= .03, and the simple two-way interaction between time and emotion was significant for the DB+ group only, F (4, 212) = 6.32, p < .001.
To rule out the possibility that regression to the mean could account for these emotion recognition improvements, we also assessed group differences in FER change scores, controlling for pretest FER scores. The mean difference score for the DB+ group was 12.9 (SD = 12.29) and for the DB− group it was −.0002 (SD = 5.73); an analysis of covariance (ANCOVA) showed that the difference in difference scores between the groups, controlling for pretest FER scores, was statistically significant, F (1, 89) = 5.81, p = .018, ${\rm \eta }_{\rm p}^2$ = .06. This suggests that the findings represent a true improvement in emotion recognition, rather than regression to the mean.
= .06. This suggests that the findings represent a true improvement in emotion recognition, rather than regression to the mean.
Eye gaze
The percentage of time that the children spent looking at the eyes while looking at the face was assessed to understand whether eye gaze changed over time. A three-way mixed ANOVA (within-subjects factors: emotion and time; between-subjects factor: group) was conducted. The relevant means are shown in Table 2. The interaction between group and time was not significant, F (1, 51) = .007, p = .93, ${\rm \eta }_{\rm p}^2$ < .001. There were no other significant interactions (all ps > .05). Although not hypothesized, we also analyzed whether there was a difference in time spent looking at the mouth, given that this formed part of the CERT training. There was no significant interaction between group and time when assessing dwell time to the mouth, F (1, 51) = .68, p = .412, ${\rm \eta }_{\rm p}^2$
< .001. There were no other significant interactions (all ps > .05). Although not hypothesized, we also analyzed whether there was a difference in time spent looking at the mouth, given that this formed part of the CERT training. There was no significant interaction between group and time when assessing dwell time to the mouth, F (1, 51) = .68, p = .412, ${\rm \eta }_{\rm p}^2$ = .013. There were no other significant interactions (all ps > .05).
= .013. There were no other significant interactions (all ps > .05).
Table 2. Mean percentage of time spent looking at the eyes at pre- and posttest

Notes: Standard deviations in parentheses. DB = disruptive behavior.
In order to understand whether there was a relationship between emotion recognition and eye gaze, a Spearman's correlation was calculated. There was no significant relationship between eye gaze and negative emotion recognition at pretest (r = .21, n = 53, p = .130), or posttest (r = .21, n = 53, p = .126).
Discussion
The aim of this study was to establish the efficacy of a brief and computerized tailored intervention (the CERT), administered in a school setting, in improving emotion recognition in young high-risk children, and to examine the possible role of visual attention in accounting for observed performance impairments or improvements. This study shows that extent of impairment in negative emotion recognition was significantly related to severity of disruptive behavior, especially problems in peer relations, and that children with disruptive behavior significantly improved in emotion recognition after completing a targeted training, in this case the CERT. However, we found no evidence to suggest that eye gaze plays a role in emotion recognition impairments or in the observed improvements in emotion recognition. The fact that we found significant improvements in emotion recognition in the group that received the training and not in the other group suggests that these improvements were not due to repeated testing or other aspects of the interventions received by children in both groups.
In previous studies, children were not allocated to receive emotion training based on evidence of an impairment. In the current study, we initially assessed the extent of emotion recognition impairments and found that 59% of the referred children exhibited emotion recognition impairments, consistent with the notion of variability in underlying processes that influence behavioral and emotional problems (Glass & Newman, Reference Glass and Newman2006; Woodworth & Waschbusch, Reference Woodworth and Waschbusch2008). This is also consistent with the RDoC claim that it should not be assumed that impaired processes are present in all those who display similar behavioral problems, and that interventions should be targeted at those who really need support (Insel et al., Reference Insel, Cuthbert, Garvey, Heinssen, Pine, Quinn and Wang2010).
We found that children who completed the CERT showed a significant improvement in recognition of sadness, fear, anger, and neutral expressions. Fear and sadness recognition have been most consistently found to be impaired in antisocial populations (Marsh & Blair, Reference Marsh and Blair2008), but more recent evidence suggests that antisocial populations may also struggle to detect expressions of anger (Bowen et al., Reference Bowen, Morgan, Moore and van Goozen2014).
When considering the mechanism underlying variation in emotion recognition, we found no evidence that visual attention is an important process. Attention to the eye region was unrelated to emotion recognition at pretest and posttest. Research comparing eye gaze in disruptive children participating in the same intervention program and typically developing comparison children also found no role for eye gaze in accounting for the group difference in emotion recognition (Hunnikin et al., Reference Hunnikin, Wells, Ash and van Goozen2019). This is important for our understanding of what the CERT does. Although the CERT directs attention to key facial features and provides hints to assist with the interpretation of facial features, we found no change in percentage of time spent looking at the eyes during the emotion recognition task. In light of this, we argue that the CERT helps children to interpret facial features, rather than simply redirecting attention to certain parts of the face. In a similar way, individuals with schizophrenia have been found to improve in emotion recognition when they were taught how to interpret emotion expressions, but not when they were instructed where to direct their attention (Tsotsi, Kosmidis, & Bozikas, Reference Tsotsi, Kosmidis and Bozikas2017).
We have also shown that emotion recognition was negatively related to peer problems. This is consistent with the claim that there is a relationship between impaired emotion recognition and social relationships (Corden, Critchley, Skuse, & Dolan, Reference Corden, Critchley, Skuse and Dolan2009). Given that having better friendships with others is a protective factor in preventing further behavioral issues (Hodges, Boivin, Vitaro, & Bukowski, Reference Hodges, Boivin, Vitaro and Bukowski1999), this is further evidence of the utility of emotion recognition training.
We should acknowledge some limitations of the present research. First, children were not randomly allocated to groups. Children in the DB− group acted as comparison children; they were allocated to this group because they had no emotion recognition impairment, even though they had been referred into the early intervention hub because of disruptive behavior. As argued earlier, interventions that are tailored and target an individual's impairments are more effective (van Goozen & Fairchild, Reference van Goozen and Fairchild2008; Wilkinson et al., Reference Wilkinson, Waller and Viding2015) and the objective of the present study was to deliver an emotion intervention according to objectively assessed need (Insel et al., Reference Insel, Cuthbert, Garvey, Heinssen, Pine, Quinn and Wang2010). Therefore, only children who displayed an emotion impairment were offered the CERT and the purpose of the study was to test the efficacy of the CERT in improving emotion recognition in these children. Now that we have established the effectiveness of the CERT, the next phase is to conduct an randomized clinical trial (RCT) in which children with disruptive behavior are randomly assigned to receive the CERT, regardless of emotion recognition impairments, so we can draw firmer causal conclusions about the impact of the CERT. Second, although the study shows that the CERT improves emotion recognition in children with an impairment, it does not establish whether improved emotion recognition results in improvements in longer-term behavior. Only a small number of studies have shown that improving emotion recognition is associated with reductions in aggression or severity of reoffending behavior (Hubble et al., Reference Hubble, Bowen, Moore and van Goozen2015; Penton-Voak et al., Reference Penton-Voak, Thomas, Gage, McMurran, McDonald and Munafò2013). Presumably, it takes time for improved emotion recognition to have positive effects on behavior and the quality of social relationships, especially where these have been poor. We are following up the current sample to find out more about longer-term outcomes. A third limitation is that the current sample was too small to enable us to investigate the role of different types of disruptive behavior and/or exposure to early risk factors, and their impacts on emotion recognition before and after training. For example, it is known that a history of physical abuse is associated with a reduced need for sensory input to accurately recognize expressions of anger (Pollak & Sinha, Reference Pollak and Sinha2002). This is an issue that should be examined in future research.
Conclusions and clinical implications
Emotion recognition problems are a common precursor in a range of psychopathologies, not only antisocial and criminal behavior (Copeland et al., Reference Copeland, Shanahan, Costello and Angold2009). The RDoC approach advocates the need to develop interventions based on the assessment of transdiagnostic processes. The current study shows that the recognition of negative and neutral emotional expressions can be improved relatively quickly in children with disruptive behavior. We have also shown that it is unlikely that eye gaze is the mechanism underlying impaired or improved emotion recognition. Instead, we suggest that our training helps children to appraise key emotional stimuli correctly. Given that emotion recognition is important in initiating and maintaining social relationships (Izard et al., Reference Izard, Fine, Schultz, Mostow, Ackerman and Youngstrom2001), the CERT has the potential to have a positive influence on the social lives of children with impairments in emotion recognition. Research is now needed to investigate the longer-term effects of this training.
Acknowledgments
We are extremely grateful to all children, their families and schools for taking part. We would like to thank Northamptonshire Police Early Intervention Team for their assistance with this study and Melanie Smith for help with recruitment.
Funding Statement
This work was supported by an Economic and Social Research Council studentship (awarded to AEW) and an ESRC Impact Acceleration grant (514845 awarded to SHMvG).
Conflicts of Interest
The funding sources had no role in the study design, collection, analysis or interpretation of data, the writing of the article or decision to submit the article for publication. The authors declare no other conflicts of interest.









 Open access
Open access