



Introduction
Please suggest whether the first affiliation (affiliation 1) needs to be set as two separate affiliations (affiliations 1 and 2).Please provide city/state for the affiliation “2”.Per journal style, abstract should be no more than 250 words. Please edit accordingly.Please check whether the head levels are identified correctly.While exercise has numerous health benefits, excessive exercise for some individuals may have untoward mental and/or physical health consequences.Reference Petit and Lejoyeux1 For example, continuing to engage in exercise despite an injury could lead to worsening or permanence of that injury, and excessive time spent on exercise could lead to neglect of other areas of life, for example, interpersonal relationship.Reference Berczik, Szabo and Griffiths2 Excessive exercise could also have a negative impact in relation to other mental health disorders, such as people with eating disorders exercising in order to maintain unhealthily low body mass indices,Reference Schlegl, Dittmer, Hoffmann and Voderholzer3 or people with muscle dysmorphia who strive to increase muscle mass with exercise and steroids.Reference Segura-Garcia, Ammendolia and Procopio4 Other consequences of excessive exercise reported in the literature include immune dysfunction and chronic fatigue arising from excessive exercise.Reference Chen5 The concept of “negative exercise” or “exercise addiction” was first developed in the 1980s, drawing contrast with the earlier concept of “positive exercise” indicating positive health benefits.Reference Lichtenstein, Hinze and Emborg6–Reference Lejoyeux, Guillot and Chalvin8 Here, we use the term “problematic exercise” to describe these phenomena, since this term focuses on the behavior rather than assuming it to be contained within a particular theoretical framework of, for example, addiction or compulsivity. Nonetheless, current measures of problematic exercise tend to utilize questions relating to addiction.
Two concepts that have proven to be useful in understanding other types of repetitive behavior, and which may be relevant for excessive exercise, are impulsivity and compulsivity.Reference Chamberlain and Grant9–Reference Brooks, Lochner and Shoptaw13 Impulsivity refers to hasty premature actions, without due forethought, which have untoward longer-term consequences. Compulsivity refers to repetitive habitual behaviors that have lost their relationship with the original intent or goal. While studies have examined impulsivityReference Kotbagi, Morvan and Romo14 and compulsivityReference Goodwin, Haycraft and Meyer15 in problematic exercise, the interplay between these two constructs has seldom been examined in the same setting or using statistical techniques that are resilient to expected issues such as collinearity (correlations) across variables of interest. Another concept important in understanding excessive exercise is emotional dysregulation, which has been found to predict subsequent excessive/compulsive exercise.Reference Goodwin, Haycraft and Meyer15 Furthermore, acute exercise has been found to dampen emotion regulation deficits.Reference Bernstein and McNally16 Understanding the roles of impulsivity, compulsivity, and emotional dysregulation in problematic exercise may help to identify predisposing factors and implicated mechanisms, as well as help account for overlap with other disorders such as eating disorders.Reference Di Lodovico, Dubertret and Ameller17
Therefore, the aims of this study were (i) to explore the factor structure of problematic exercise (measured using the Exercise Addiction Inventory, EAI) in young adults; (ii) to assess the impact of identified EAI factor scores on quality of life; and (iii) to evaluate the potential contribution of impulsive and compulsive psychological mechanisms to problematic exercise. We hypothesized that all EAI factor scores would be associated with elevated occurrence of impulsivity, compulsivity, and emotional dysregulation.
Methods
Participants
Participants were recruited from the Neuroscience in Psychiatry Network, which is an established cohort of young adults being followed over time to explore brain development and mental health.Reference Kiddle, Inkster and Prabhu18 The sample was originally recruited on a stratified basis, in order to maximize representativeness of the normal population in the catchment areas covered (Cambridge and London). We contacted all individuals who were still enrolled in this cohort at the time of data collection (2017–2018) via email and invited them to take part in an online study being conducted using SurveyMonkey. Prior to participation, individuals read an information sheet, indicated consent, and had the opportunity to contact the study team to address any queries/concerns they might have. The study was approved by research ethics committee, and the people taking part received £15 compensation in the form of a gift voucher.
Measures
The following demographic information was collected: age, gender, ethnicity, and education level. Problematic exercise was assessed using the EAI.Reference Griffiths, Szabo and Terry19 This is a six-item screening tool that was previously shown to have good psychometric properties and sound concurrent validity against other established scales for problematic exercise. The scale enquires about: conflicts occurring with one’s partner/family due to exercise, using exercise to change one’s mood (e.g., obtain a “buzz”), escalating participation in exercise over time, irritability if missing exercise, and failed attempts to cut back. For each question, the individual responses on a scale of 1–5, ranging from “strongly disagree” to “strongly agree.” Thus, the scale gives a total score out of 60.Reference Griffiths, Szabo and Terry19 In addition to the EAI, the following scales were completed, focusing on quality of life, impulsivity, compulsivity, and emotional regulation.
Brunnsviken Brief Quality of Life Scale (BBQ).Reference Lindner, Frykheden and Forsstrom20 BBQ is a previously validated self-report quality-of-life scale, which covers six life areas (leisure time, view of life, creativity, learning, friends/friendship, and view of self) that are important determinants of the overall quality of life. This scale has been validated in various normative and clinical population settings.Reference Lindner, Frykheden and Forsstrom20 The measure of interest was the total quality of life score.
SUPPS.Reference Cyders, Littlefield and Coffey21 SUPPS is a short version of the UPPS, which is a questionnaire capturing different aspects of impulsivity, namely sensation seeking, lack of premeditation, lack of perseverance, negative urgency, and positive urgency.Reference Cyders and Smith22 There are 20 items, each responded to on a scale of 0–3. Measures of interest were summed for each domain, yielding five measures of impulsivity, each out of a maximum of 12 points.
SCOFF Eating Disorder Questionnaire.Reference Luck, Morgan and Reid23 This is a previously validated screening tool for detection of disordered eating. The scale is sensitive to the presence of different aspects of disordered eating, such as deliberately making one’s self sick, distorted body image, and loss of control over eating. We included the SCOFF as we were interested in a possible relationship between exercise and eating disorder-related symptoms.Reference Schlegl, Dittmer, Hoffmann and Voderholzer3, Reference Renz, Fisher and Vidair24 The measure of interest was total items endorsed on the SCOFF.
Cambridge–Chicago Compulsivity Trait Scale (CHI-T).Reference Chamberlain and Grant9 This is a recently developed scale designed to capture the comprehensive aspects of compulsivity, viewed trans-diagnostically. The scale comprises 15 items, each scored on a Likert scale of 1–4, from “strongly disagree” to “strongly agree.” The total score is 60, with higher scores indicating higher compulsivity. The scale is sensitive to compulsivity across a range of pathologies, such as disordered gambling, substance use, and obsessive-compulsive symptoms.Reference Chamberlain and Grant9 The measure of interest was the total score.
Padua Obsessive-Compulsive Inventory (Washington State Revision).Reference Burns25, Reference Sanavio26 This is a 39-item questionnaire measuring the broad range of obsessive-compulsive symptoms, designed for use in normative and clinical populations. Each item has a Likert scale (0–4), with higher scores indicating more symptoms. The scale gives a total score out of maximum of 156, which was the measure of interest.
Difficulties with Emotion Regulation Scale (DERS).Reference Gratz and Roemer27 This is a 36-item questionnaire encompassing multiple aspects of emotional dysregulation, indicating difficulties controlling one’s emotional responses relating to social interactions.Reference D’Agostino, Covanti and Rossi Monti28 Each question is responded to on a scale of 0–5, ranging from “almost never” to “almost always.” The measure of interest was the total score out of 180, with higher scores indicating more emotional dysregulation.
Data analysis
The demographic characteristics of the sample were summarized. The structure of the EAI was explored using exploratory factor analysis, with the optimal number of factors selected using scree plot combined with the inspection of eigenvalues. The potential clinical relevance of EAI factor scores was considered by undertaking Spearman’s r correlations against quality-of-life scores on the BBQ, with p < 0.05 uncorrected being defined as statistically significant.
To evaluate the links between problematic exercise and impulsivity/compulsivity, and emotional dysregulation (plus relevant demographic characteristics), we used the statistical technique of partial least squares (PLS). PLS is a multivariate statistical technique that models the relationship between a number of X (explanatory) variables and one or more outcome (Y) variables through an iterative process.Reference Wold, Sjöström and Erikkson29–Reference Wold31 This statistical approach is highly suited to situations such as cross-sectional analyses, in which there are relatively large numbers of variables, and these variables are correlated, hence breaching statistical assumptions of many typical statistical approaches. Here, the Y variable of interest was factor score on the EAI, and the X variables of interest were all other measures (demographic characteristics and questionnaire scores). A separate PLS model was run for each EAI factor score type identified. The optimal model was selected using leave-one-out cross-validation and by minimizing the PRESS statistic. We used a two-stage process in order to identify measures significantly associated with problematic exercise, per previously established methodologies.Reference Chamberlain, Cavanagh and de Boer32 First, X measures with variable importance parameter (VIP) < 0.8 were removed from the initial PLS model. Second, the distributions of model coefficients were characterized using bootstrap (1000 iterations). Explanatory variables with VIP > 0.8 whose 95% confidence intervals did not cross the null line in the final PLS model were deemed statistically significant. All statistical analyses were conducted using JMP Pro.
Results
In total, 642 people completed the study. The sample had mean (standard deviation) age of 23.4 (3.2) years, were mostly female (64.7%), and were mostly of self-defined White Caucasian ethnicity (78.7%). The distributions of EAI item responses and total scores are provided in the Supplementary Material. Factor analysis based on scree plot inspection and eigenvalues (see Supplementary Material) indicated two factors for the EAI, accounting for 57.9% and 14.8% of the variance, respectively (cumulatively 72.3% of the variance). The loadings of each individual scale item onto these two factors are shown in Figure 1. It can be seen that factor 1 related to the majority of scale items (hereafter termed “general factor”) and that factor 2 related more specifically to conflicts arising between the individual and their partner/family members due to exercise (hereafter termed “relationship conflict factor”). EAI general scores did not correlate with quality of life on the BBQ (r = 0.013, p = 0.740), whereas EAI relationship conflict scores did (r = −0.120, p < 0.001). The latter was also significant for all domains of functioning on the BBQ considered separately (all p < 0.001 per domain, except for creativity-related quality of life, which was significant but less so with p = 0.0324).
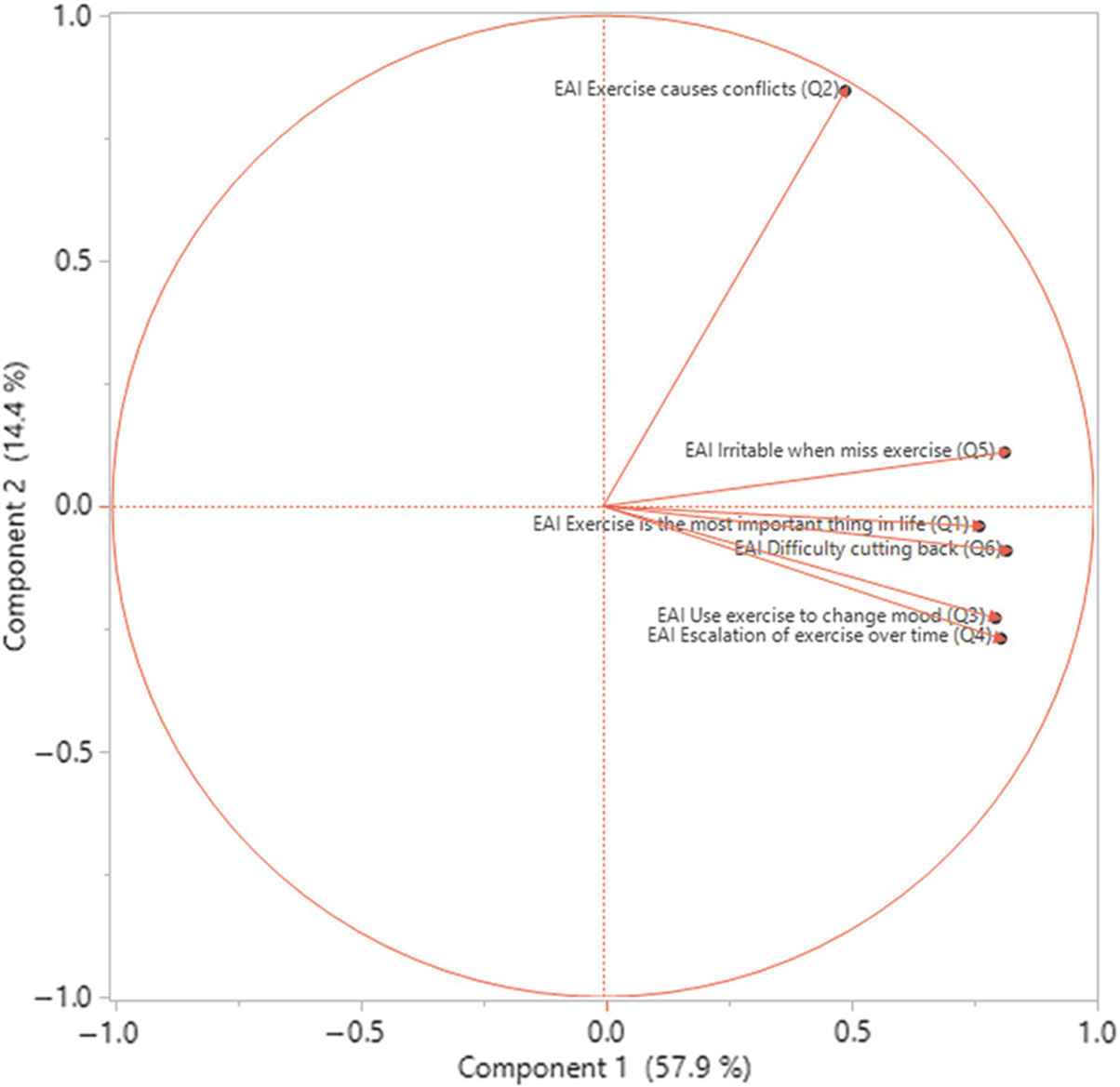
FIGURE 1. Loading of individual EAI items onto the two factors.
PLS yielded an optimal model capturing 58.6% of variance in the explanatory (X) variables and 13.2% of variance in problematic exercise general factor. Figure 2 shows variables retained in the final model (i.e., those with VIP > 0.8); those explanatory variables that were statistically significant (p < 0.05, bootstrap) are shown with an asterisk. PLS yielded an optimal model capturing 47.1% of variance in the explanatory (X) variables and 6.2% of variance in problematic exercise relationship conflict factor. Figure 3 shows variables retained in the final model (i.e., those with VIP > 0.8); those explanatory variables that were statistically significant (p < 0.05, bootstrap) are shown with an asterisk.
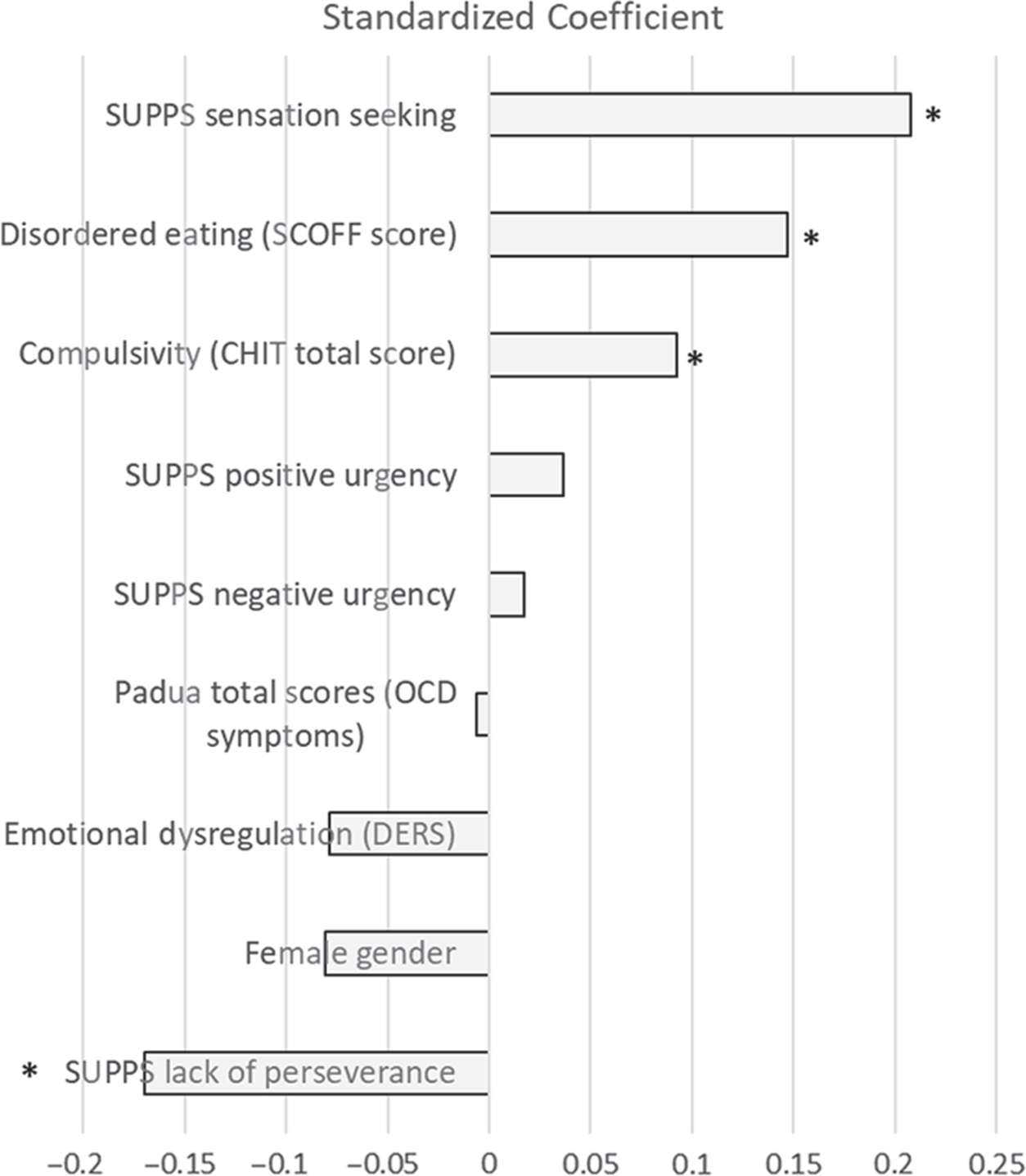
FIGURE 2. Variables in the PLS model predicting EAI general factor scores (VIP > 0.8). * indicates statistically significant predictor (p < 0.05 using conservative bootstrap).
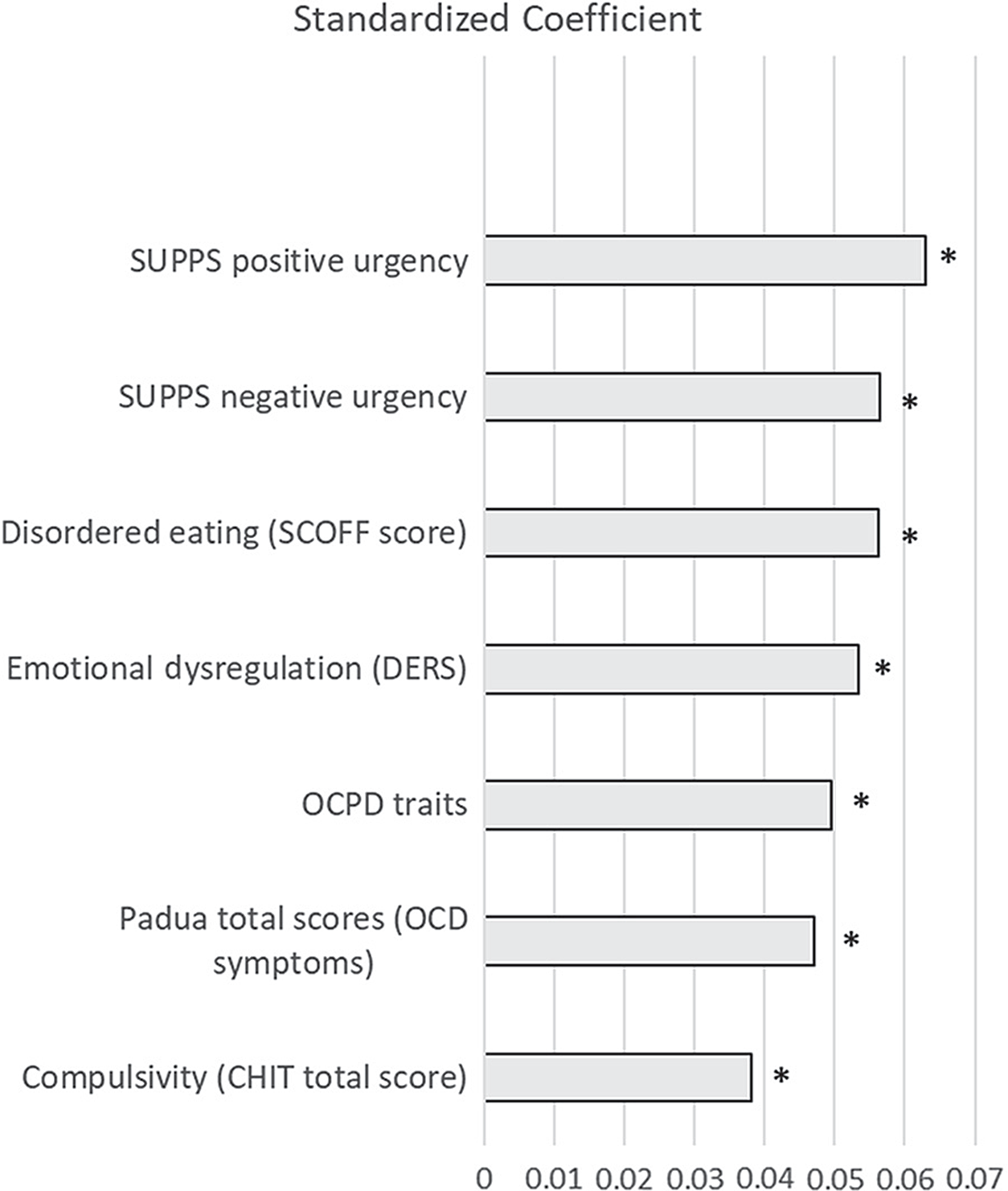
FIGURE 3. Variables in the PLS model predicting EAI relationship conflict factor EAI scores (VIP > 0.8). * indicates statistically significant predictor (p < 0.05 using conservative bootstrap).
Discussion
This study used a dimensional approach to investigate problematic exercise in young adults recruited from a cohort of young adults recruited from the general population. The percentage of the sample with an EAI total score >24, suggestive of overt exercise addiction based on previous validation, was 1.1%. As expected due to the epidemiologic nature of the cohort, this is slightly lower than the prevalence rate of 3% found in a sample of habitual exercisers.Reference Griffiths, Szabo and Terry19 In young people, prevalence rates based on an equivalent version of this instrument have been estimated at 4% in school athletes, 8.7% in fitness attendees, and 21% in people with eating disorders.Reference Lichtenstein, Griffiths and Hemmingsen33 Hence it should be born in mind that the current sample mainly focused on exercise that fell short of the full definition of exercise addiction. Nonetheless, this dimensional approach that includes subsyndromal people may provide useful insights into the full range of behaviors and their associations.
We focused on the factor structure of a standard assessment tool for problematic exercise and how scale factor scores related to quality of life and psychological mechanisms. Factor analysis of the EAI indicated the existence of a “general“ factor and a “relationship conflict” factor. Both factors were associated with disordered eating (SCOFF questionnaire), impulsivity (several SUPPS subscales), and compulsivity (CHI-T scores). The relationship conflict factor score was additionally associated with worse quality of life, emotional dysregulation, and obsessive-compulsive personality traits. Problematic exercise scores were not significantly influenced by demographic characteristics of age, gender, or ethnic grouping.
The significant relationship between disordered eating as measured by the SCOFF instrument and problematic exercise is in keeping with a substantive body of literature. Studies have found elevated rates of excessive exercise in people with eating disorders or disordered eating, for example, ref. [Reference Schlegl, Dittmer, Hoffmann and Voderholzer3]. In some studies, the prevalence of eating disorders has been found to be elevated in athletes as compared to the background population,Reference Di Lodovico, Dubertret and Ameller17 though this relationship may not be universal. For example, disordered eating has been found to be higher in sports such as dancing, wrestling, and body building, but not necessarily equally so across genders.Reference Chapman and Woodman34–Reference Devrim, Bilgic and Hongu36 In a sample of runners, those at risk of eating disorder, based on a SCOFF cut-off, had significantly higher problematic exercise scores on the EAI.Reference Di Lodovico, Dubertret and Ameller17 Here, disordered eating on the SCOFF was significantly associated with both problematic exercise factors on the EAI.
Impulsivity is not a unitary phenomenon but rather encompasses a number of separable domains. We used the SUPPS, which dissects sensation seeking, lack of premeditation, lack of perseverance, negative urgency, and positive urgency.Reference Cyders, Littlefield and Coffey21 In a prior study using the UPPS, sensation seeking, positive urgency, and negative urgency, all appeared to play a role in problematic exercise.Reference Kotbagi, Morvan and Romo14 Here, on the SUPPS, the EAI general factor was associated with higher sensation-seeking and with lower lack of perseverance (i.e., with higher perseverative tendencies). Thus, this propensity toward excessive exercise per se may be more common in people who enjoy the risky element of sports, and in those who have a tendency toward perseveration, that is, repetition of habits, which would be more related to the construct of compulsivity than impulsivity. The relationship conflict EAI factor had different associations with impulsivity; this was significantly related to positive and negative urgency, as well as to emotional dysregulation. Positive urgency refers to the tendency to engage in acts due to a positive mental state (e.g., excitement), whereas negative urgency refers to a tendency to engage in acts due to unpleasant emotional states (e.g., low mood or anxiety).Reference Billieux, Gay and Rochat37 Emotional dysregulation reflects difficulties handling emotionally charged social situations.Reference D’Agostino, Covanti and Rossi Monti28, Reference Lavender, Wonderlich and Engel38 Collectively these data indicate that the relationship conflict component of problematic exercise is associated with impulsive responses to extreme emotions (positive and negative urgency), which indeed may be more commonly experienced in people with emotional dysregulation (short-term emotional lability). In a prior longitudinal study conducted in adolescents, emotional dysregulation predicted problematic exercise 12 months later.Reference Goodwin, Haycraft and Meyer15 This raises the possibility that, in fact, those with problematic exercise are undertaking said exercise in order to deal with emotional dysregulation.
Turning to compulsivity, trans-diagnostic compulsivity on the CHIT was significantly associated with both general and relationship conflict factor scores from the EAI. This tendency toward repetitive ingrained habits could reflect a propensity (vulnerability) toward the development of problematic exercise. Longitudinal research would be valuable to test the idea that elevated compulsivity may predispose toward a range of later problem behaviors, including excessive exercise. The number of diagnostic items endorsed for obsessive-compulsive personality disorder was significantly associated with higher relationship conflict problematic exercise scores, but not general scores. This highlights that the use of trans-diagnostic markers, rather than scales specifically relating to one disorder, may be more sensitive to the detection of vulnerability issues.
Several limitations should be considered. Online surveys have limitations compared to in-person clinical assessments – instruments may be less accurate for measuring psychopathology, and there may be less quality control. Therefore, the findings should be replicated using more rigorous in-person clinical assessments. Online surveys are subject to potential sampling bias (e.g., more extensive users of the Internet may be more likely to participate in online surveys, whereas this may not impact participation in an in-person study). In contrast, online assessment has the advantage of being extremely convenient for study participants, since it does not involve travel and can be done at a convenient time. We assessed problematic exercise using the EAI. However, in future work it would be valuable to include a broader range of rating scales pertaining to the measurement of different aspects of problematic exercise. While this study identified two factors as the optimal structure to account for the current EAI data, prior work suggested a one-factor solution.Reference Griffiths, Szabo and Terry19 Our current data do not contradict this previous finding because (i) a one-factor solution would have been reasonable with the current dataset if one focused solely on eigenvalues as the selection criteria; (ii) the majority of variance here was captured within the first extracted factor; and (iii) in some populations, a one-factor solution may be preferred.Reference Lichtenstein, Griffiths and Hemmingsen33 Hence, depending on the focus of a given study and its purpose, one- or two-factor solutions would both appear reasonable. Nonetheless, we believe that the two-factor solution here revealed some interesting insights in relation to how distinct aspects of problematic exercise may have different associations with quality of life and underlying psychological processes. Our use of a normative sample can be viewed as being a positive feature, since results may be more likely to generalize to the background population as compared, for example, to studies that recruit people in particular clinical settings, or from gyms. The current cohort was largely free from full “exercise addiction” by conventional criteria. Future studies should also use case–control designs to explore the full disorder rather than a dimensional measure of exercise. Another limitation is that we did not evaluate the psychometric properties of various instruments. Further research is needed to confirm if these current findings do indeed generalize to other groups, including cohorts with higher degrees of pathology. Finally, we did not examine whether problematic exercise was secondary to body dysmorphic disorder or eating disorders.
Conclusions
We found that problematic exercise is associated with both impulsivity and compulsivity, even controlling for the interplay between these and other variables using the statistical technique of PLS. The aspect of problematic exercise relating to relationship conflict was additionally associated with worse quality of life and with more maladaptive personality traits (obsessive-compulsive personality disorder and emotional dysregulation). An interesting possibility suggested by these data is that people with emotional dysregulation, and perhaps impulsive/compulsive tendencies, may engage in exercise as a compensatory mechanism or coping strategy, and that exercise – even when scoring on the EAI – need not necessarily be viewed as pathological. In a laboratory-based study, acute exercise (30 min stretching or running) dampened down emotional dysregulation due to later mood challenge.Reference Bernstein and McNally16 The definition of “problematic exercise” and its potential clinical utility, therefore, requires more research, and it is for this reason that we used a dimensional approach in this study. As with many repetitive behaviors, drawing guidelines as to what is healthy or moderate versus pathological remains challenging.
Disclosures
Dr. Grant has received research grants from NIDA, National Center for Responsible Gaming, TLC Foundation for BFRBs, American Foundation for Suicide Prevention, Brainsway, and Psyadon, and Takeda Pharmaceuticals. He receives yearly compensation from Springer Publishing for acting as Editor-in-Chief of the Journal of Gambling Studies and has received royalties from Oxford University Press, American Psychiatric Publishing, Inc., Norton Press, and McGraw Hill. Dr. Chamberlain consults for Cambridge Cognition, Shire, and Promentis. His involvement in this project was funded by a Wellcome Trust Fellowship (110049/Z/15/Z).
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1092852919000762






 Open access
Open access