



Introduction
Anatomic variations of the aortic arch are common in the general population and are often only incidentally discovered. A left-sided aortic arch with aberrant right subclavian artery represents the most common congenital subclavian anomaly, arising in 0.5–2% of the population. Reference Jakanani and Adair1 Associated anatomic configurations vary, coursing posterior to the oesophagus (80%) (Figure 1A), between the oesophagus and trachea (15%) (Figure 1B), or anterior to the trachea (5%) (Figure 1C). Reference Myers, Fasel, Kalangos and Gailloud2 Notably, a right-sided aortic arch with aberrant left subclavian artery is even more uncommon, yet represents a complete vascular ring and is often operatively managed. Reference Shuford, Sybers, Gordon, Baron and Carson3 While most individuals with aberrant arterial anatomy remain asymptomatic, dysphagia is a common presenting symptom. For patients with an incomplete ring defined by a left aortic arch and aberrant right subclavian artery, textbooks suggest these should not be intervened upon surgically. Reference Epperson and Howell4,Reference Backer, Rigsby, Mavroudis, Backer and Mavroudis5 Our case series challenges this previously held notion, with four children having successful mitigation of profound dysphagia resulting from an aberrant right subclavian artery following operative repair.

Figure 1. Anatomic Configurations associated with aberrant right subclavian artery.
Materials and methods
Approval from the Institutional Review Board at Duke University was obtained, followed by a comprehensive search of the electronic medical record. This identified four patients who underwent successful reimplantation of an aberrant right subclavian artery between November 2018 and November 2023. Further query of the electronic medical record targeted inpatient and outpatient records, intraoperative documentation, perioperative course, and postoperative complications where applicable. These data were further supported by a comprehensive literature review pertaining to aberrant right subclavian artery management.
Results
Four patients underwent reimplantation of an aberrant right subclavian artery with our congenital cardiac team and were included in the study. All cases were approached via a right posterolateral thoracotomy. Specific details of each case are detailed below:
Case 1
An 8-year-old female weighing 21.6 kg presented with a three-year history of progressively worsening dysphagia, globus sensation, and cough. She was diagnosed with an aberrant right subclavian artery at age 2. Repair was not indicated at time of the original diagnosis given she was asymptomatic.
Considering the patient’s worsening dysphagia, surgical repair was advised. CT angiography of the chest demonstrated an aberrant right subclavian artery off of the descending aorta with a retroesophageal course (Figure 2). A barium swallow revealed extrinsic impression on the left posterior oesophagus with minimal luminal narrowing.
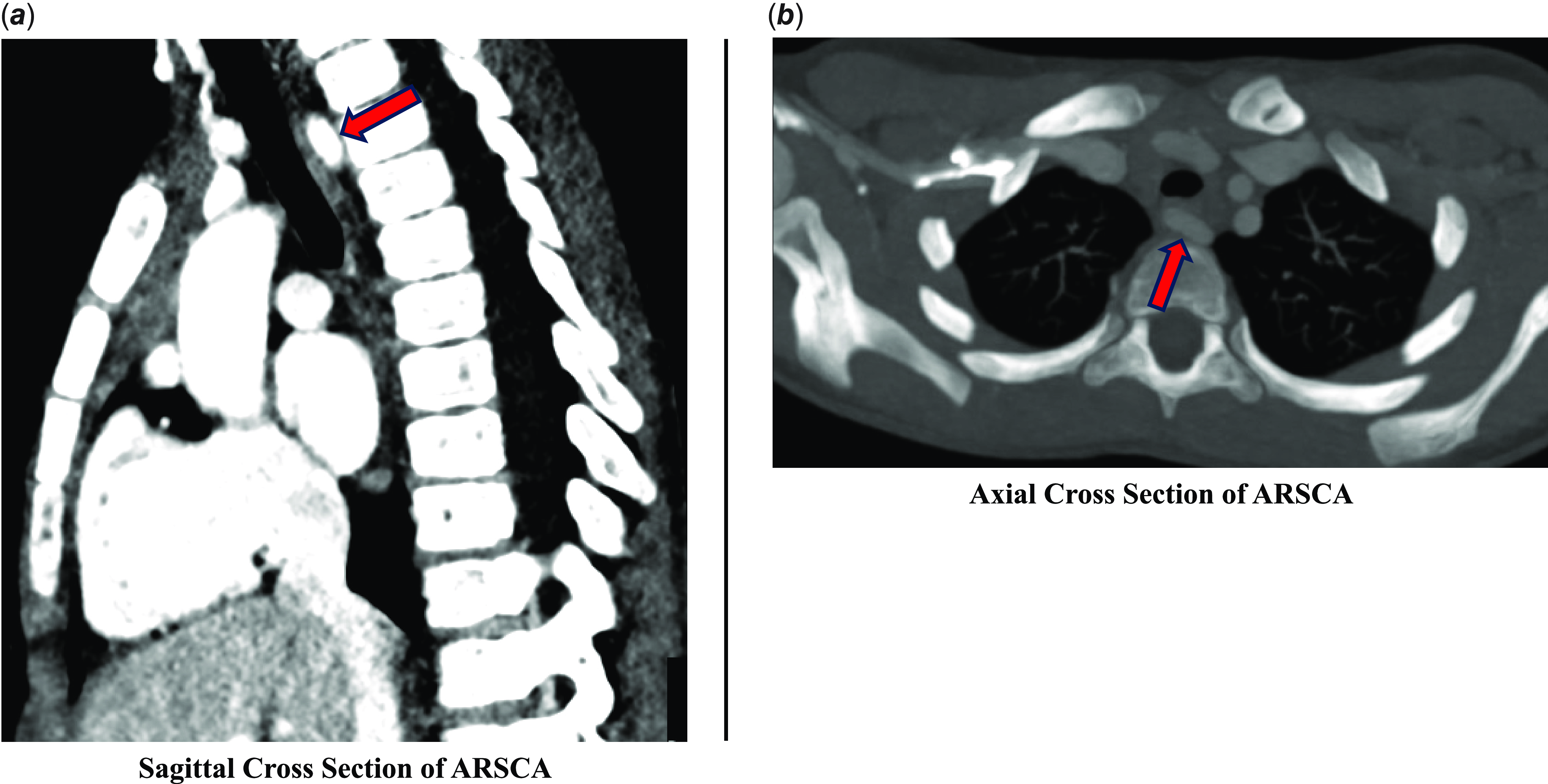
Figure 2. Case 1 Preoperative CT Imaging.
The patient was taken to the operating room for repair of the anomalous vessel via a right posterolateral thoracotomy. The right subclavian artery and the right common carotid artery were identified. The patient was heparinised, and the right subclavian artery was sharply transected, releasing the vascular ring. The aortic stump was oversewn, and hemostasis was ensured. Attention was then turned to the right common carotid artery, along which a side-biting clamp was placed. The right subclavian artery was spatulated and an end-to-side anastomosis was performed. A 19 Fr blake drain was placed and the incision was closed in layers. The patient was extubated in the operating room and transferred to the ICU in stable condition. The patient was weaned to room air on the night of surgery. The chest tube was removed on postoperative day 1. The patient was discharged home on postoperative day 2 and was last contacted four years later with complete resolution of dysphagia and normalised weight for age.
Case 2
An 8-year-old female weighing 23.2 kg presented to clinic with a one-year history of worsening dysphagia and severe globus sensation. This difficulty eating had caused her significant anxiety and oral aversion to the point where she was only tolerating a liquid diet. She underwent a gastrointestinal work up at an outside hospital, which demonstrated a seemingly pulsatile upper oesophagus during oesophagogastroduodenoscopy. A CT of the chest demonstrated an aberrant right subclavian artery with a retroesophageal course (Figure 3). Repeat upper gastrointestinal study confirmed extrinsic mass effect in the proximal thoracic oesophagus compatible with aberrant right subclavian artery. She was referred to our centre for further management. Given her severe symptoms, surgical repair was recommended.

Figure 3. Case 2 Preoperative CT Imaging.
The patient was taken to the operating room for repair of the aberrant right subclavian artery. The right subclavian artery reimplantation was performed via the same method as above. After the completion of the procedure, haemostasis was achieved, a pleural chest drain was placed, and the incision was closed in layers. Her postoperative course was complicated by a moderate left pleural effusion on postoperative day 2, which was managed conservatively with diuresis. The patient was discharged home on postoperative day 6 tolerating solid foods with significant improvement of dysphagia. The patient was last seen in clinic a year later with complete resolution of preoperative symptoms, normal oral intake and weight gain, and an interval barium swallow showing no evidence of oesophageal narrowing.
Case 3
An 11month-old male weighing 9.27 kg presented to clinic following 5 months of difficulty feeding, post-prandial emesis refractory to antiemetic therapy, and inability to gain weight. He underwent an echocardiogram concerning for an aberrant right subclavian artery, which was subsequently confirmed on upper gastrointestinal series and CT angiogram to be coursing posterior to the oesophagus, resulting in compression. He was referred to our centre, and surgical repair was recommended.
In the operating room, a successful transposition of the aberrant right subclavian artery was performed via the previously described method. He was extubated in the operating room and weaned to room air the night of surgery. His postoperative course was notable for a chyle leak resulting in chylothorax, diagnosed on the morning of postoperative day 1. He was made nil per os, total parenteral nutrition started, and diuresis initiated. This resulted in progressive improvement of his chylous chest tube output and eventual discharge to home on postoperative day 8. He was most recently evaluated at 3 months postoperatively in clinic with complete resolution of his symptoms and was found to be gaining weight appropriately.
Case 4
A 16-month-old male presented to clinic with persistent dysphagia and dyspnoea following diagnosis of an aberrant right subclavian artery at age 5 months. He had initially presented to an outside facility due to dysphagia and ultimately underwent an upper gastrointestinal series suggestive of oesophageal compression. CT angiogram demonstrated an aberrant right subclavian artery with retroesophageal course, creating compression. Upon presentation to our centre, he underwent an uncomplicated transposition of the aberrant right subclavian artery to his right common carotid artery via a right posterolateral thoracotomy. Post-procedurally, his diet was rapidly advanced, and he was discharged home on postoperative day 3. At time of most recent follow-up, 6 months after repair, he was tolerating his diet with no restrictions and gaining weight appropriately. His mother had not noted any recurrence of his dysphagia, and his dyspnoea ultimately was found to be due to asthma, which was managed appropriately with medication at the direction of paediatric pulmonology.
Discussion
Here, we present a case series of four patients where the presence of an aberrant right subclavian artery manifested as severe dysphagia. In each case, operative repair consisting of a right posterolateral thoracotomy with subclavian and associated Kommerell’s diverticulum resection from the aorta and reimplantation demonstrated good postoperative outcomes and facilitated complete resolution of symptoms. The majority of current literature is limited to case reports, with textbooks stressing that these are largely not a surgical entity. Reference Backer, Rigsby, Mavroudis, Backer and Mavroudis5
The double aortic arch model was initially proposed by Dr Jesse Edwards in 1948. It describes the embryologic origin of the aorta via a hypothetical double aortic arch system. Should this become interrupted at any point, it results in various aortic arch anomalies. The development of a left aortic arch with aberrant right subclavian artery is the most common and is the result of interruption of the dorsal segment of the right arch between the right carotid and subclavian artery with regression of the right ductus arteriosus in the developing double aortic arch. Reference Edwards6
While there are a variety of aetiologies contributing to paediatric dysphagia, most are treated conservatively with anticipatory guidance for families. Reference Borowitz and Borowitz7 Our experience refutes what was previously thought of as central surgical dogma that an aberrant right subclavian artery is simply a “red herring” diagnosis for dysphagia. Reference Backer, Rigsby, Mavroudis, Backer and Mavroudis5 As discussed by Barone et al., early identification and treatment of dysphagia in the paediatric population is particularly important. It not only helps to avoid unnecessary testing, but given the rapid growth and development of children, swallowing difficulties can interrupt physical and cognitive development, potentially leading to serious long-term sequelae. Reference Barone, Carucci and Romano8 Dranseika et al. also note that operative management of aberrant right subclavian arteries in children tends to have more positive outcomes compared to that of adults, as arteries in children are more elastic and less likely to have any vascular disease that may complicate recovery. Reference Dranseika, Erdil, Schweiger, Balmer, Pretre and Dave9 While an aberrant right subclavian artery is one of the more common congenital vascular malformations, our experience along with other single case reports demonstrate that early and thorough investigation for causes of dysphagia along with appropriate operative intervention when warranted are essential for achieving optimal outcomes in these patients. Reference Barone, Carucci and Romano8,Reference Dranseika, Erdil, Schweiger, Balmer, Pretre and Dave9
In conclusion, this paediatric case series demonstrates the utility of early consideration of a right aberrant subclavian artery in the workup of persistent dysphagia. Considering this diagnosis early can minimise unnecessary testing and decrease the amount of time that physical discomfort and psychological distress have to be endured. This case series suggests that although the overwhelming majority of patients with this anatomy require no intervention, there are exceptions that might not be as rare as previously thought. The children in this series have greatly benefitted from never saying never.
Author’s statement
Permission was granted by the subject patients’ respective parents or guardians to publish this case series.
Financial support
None.
Competing interests
None.




 Open access
Open access