


Introduction
Family caregivers have been considered an integral part of geriatric care since the 1960s (Scharlach, Reference Scharlach2008). Their economic contribution to maintaining quality care for today’s aging population has been well documented (Chappell & Hollander, Reference Chappell and Hollander2011; Hollander, Liu, & Chappell, Reference Hollander, Liu and Chappell2009). According to the 2007 Eldercare report by Statistics Canada, 25 per cent of caregivers were over the age of 65, and had been providing care for an average of 6.5 years (Cranswick & Dosman, Reference Cranswick and Dosman2008). Also, the majority of the caregivers over the age of 45 had to balance caregiving with other responsibilities, such as parenting, household management, spousal duties, and employment. As caregivers age alongside their care recipients, they assume increasing physiological, psychosocial, and financial burden because of the greater health complications experienced by the frail elderly. These negative consequences expose caregivers to significant health risks (Ampalam, Gunturu, & Padma, Reference Ampalam, Gunturu and Padma2012; Tramonti, Bongioanni, Leotta, Puppi, & Rossi, Reference Tramonti, Bongioanni, Leotta, Puppi and Rossi2015). Although substantial research exists on caregiver burden in diverse settings, there is little available literature addressing older adults with multiple chronic conditions (MCC), a population that comprises one in three community-living older adults in Canada (Canadian Institute for Health Information, 2011). With the continued growth in the aging population, there are an increasing number of older adults living with MCC, such as diabetes, dementia, and stroke (Canadian Institute for Health Information, 2011). These individuals often require care by professionals and/or family members. This added responsibility of caring for another person with complex medical needs can affect the caregiver’s quality of life, which may result in caregiver burden.
Research has shown that patients with MCC have complex health care experiences (Ploeg et al., Reference Ploeg, Matthew-Maich, Fraser, Dufour, McAiney and Kaasalainen2017; Van Merode, van de Ven, & van den Akker, Reference Van Merode, van de Ven and van den Akker2018). They usually consult a number of specialists for their different conditions and are more likely to be given a variety of different medications, which sometimes interact with each other (Van Merode et al., Reference Van Merode, van de Ven and van den Akker2018). Their conditions often worsen, leading to more functional limitations and frequent transitions between hospital and home (Van Merode et al., Reference Van Merode, van de Ven and van den Akker2018). They rely heavily on their family and friend caregivers for support in areas including assistance with activities of daily living, medication management, care coordination, and transportation to appointments (Ploeg et al., Reference Ploeg, Matthew-Maich, Fraser, Dufour, McAiney and Kaasalainen2017). Caregivers, particularly women, provide 80 per cent of the care that Canadians receive in their homes. Caring for persons with MCC is more stressful because of the complex care demands of their loved ones (Ploeg et al., Reference Ploeg, Matthew-Maich, Fraser, Dufour, McAiney and Kaasalainen2017; Turcotte, Reference Turcotte2013).
Caregiver burden can be described as the “physical, financial, and psychosocial hardships of caring for a loved one”, who often has a medical condition (Garlo, O’Leary, Van Ness, & Fried, Reference Garlo, O’Leary, Van Ness and Fried2010). Despite the health risks implied in its definition, much about the topic is still unclear or is being contested. One example is the effect that the experience has on the caregiver. Mausbach et al. (Reference Mausbach, Roepke, Chattillion, Harmell, Moore and Romero-Moreno2012) suggest that the stress of caregiving may lead to depression in the caregiver through the loss of personal wealth or inability to respond appropriately to new situations. Conversely, Van Puymbroeck, Hinojosa, & Rittman (Reference Van Puymbroeck, Hinojosa and Rittman2008) propose that increased ability to find comprehensibility and meaning, and to manage stressors in caregivers of stroke patients can protect against role strain and the development of depression.
Caregiver burden is an ever-present issue that demands attention and interest to be properly addressed. There is a growing body of evidence of factors that contribute to – and may eventually predict – the level of burden associated with a caregiver. Currently, the determinants of significance may vary according to context, such as culture, policy, and the patient population, but there are also more pervasive characteristics that are universal, which include gender, income, and the caregiver’s relationship to the patient.
There is strong evidence that gender plays a significant role in the experience of burden (Papastavrou, Kalokerinou, Papacostas, Tsangari, & Sourtzi, Reference Papastavrou, Kalokerinou, Papacostas, Tsangari and Sourtzi2007; Reckrey, Decherrie, Kelley, & Ornstein, Reference Reckrey, Decherrie, Kelley and Ornstein2013). Across different populations, female caregivers usually report greater burden than their male counterparts, which is suggested to be a result of social pressure (Chappell, Dujela, & Smith, Reference Chappell, Dujela and Smith2015; Papastavrou et al., Reference Papastavrou, Kalokerinou, Papacostas, Tsangari and Sourtzi2007). A conflict between the traditional views of women as nurturers and the more recent perception of them as income providers, brought about by the changing family dynamics and economy, adds to the pressure (Chappell et al., Reference Chappell, Dujela and Smith2015).
Age is implicated in caregiver burden as well. In 1996, more than two thirds of caregivers were 30–59 years of age, with the average female caregiver age being 46 years and the average male caregiver age being 44 years. Given that the majority of caregivers are middle-aged, more than two thirds are also in the paid workforce and more than one quarter are simultaneously taking care of children under 15 years of age (Frederick & Fast, Reference Frederick and Fast1999). Women do the vast majority of caregiving (61%), and spend more time caregiving than men (Frederick & Fast, Reference Frederick and Fast1999). Young (caregivers less than 50 years old) and, increasingly, middle-aged female caregivers have to balance caregiving with other responsibilities, such as parenting, household management, spousal duties, and employment. Consequently, younger caregivers are more likely to report caregiver burden than are older caregivers.
Low income is another factor that leads to experiencing greater caregiver burden. According to Akkus (Reference Akkus2011), the caregiver’s income has a positive correlation with that person’s overall life satisfaction. Therefore, those who feel stressed by the lack of financial security are expected to experience greater stress in fulfilling their roles as caregivers. Some of the other predictors of caregiver burden are employment (Akkus, Reference Akkus2011; Choi-Kwon, Kim, Kwon, & Kim, Reference Choi-Kwon, Kim, Kwon and Kim2005); education level (Papastavrou et al., Reference Papastavrou, Kalokerinou, Papacostas, Tsangari and Sourtzi2007), and ethnicity and availability of support (Reckrey et al., Reference Reckrey, Decherrie, Kelley and Ornstein2013).
Controversy exists in the literature regarding the impact of time spent caregiving on caregiver burden; other areas that merit further investigation include specific aspects of care (Garlo et al., Reference Garlo, O’Leary, Van Ness and Fried2010), and caregiver characteristics that contribute to the burden (Saunders, Reference Saunders2008). The literature has also yet to fill the gap in how gender, age, employment status, and social interference (impact on social life) all interplay to impact burden. These are important factors when examining the caregiving experience, and can be addressed using the intersectionality approach, which has the ability to illuminate the unique experiences resulting from the intersection of diverse variables.
Given the lack of longitudinal evidence in the literature, this study is particularly unique in that it captures the caregiving experience across a six-month period. The longitudinal nature of the survey data, where the same caregiver was surveyed twice over a six-month period, allows for the study of change in caregiving experience over time, while determining how the dependent variable (caregiver burden) is affected by the dynamic states of both the caregiver and the care recipient.
A quantitative approach to intersectionality helps researchers to understand the health and social inequities (Hankivsky, Reference Hankivsky2012; Veenstra, Reference Veenstra2011). As a framework, intersectionality theory focuses on interconnected systems of domination based on race, class, gender, sexuality, and other social constructions, which simultaneously impact the lives of all people (Crenshaw, Reference Crenshaw1989, Reference Crenshaw1991). Intersectionality analysis using a quantitative framework helps to identify the dimensions, combined with other factors that produce the pattern of observed inequality (Scott & Siltanen, Reference Scott and Siltanen2012). With the focus on the quantitative intersectionality, analysis helps to identify the intersecting pattern of gender with other variables of interest and also to move beyond simple two way interactions (Scott & Siltanen, Reference Scott and Siltanen2012). Based on intersectionality theory and the reviewed literature on caregiver burden, we hypothesized that age, gender, employment status, and social interference simultaneously have a potential impact on caregiver burden. The present study uses a quantitative intersectionality approach to analyze the association between reported caregiver burden with age, gender, employment status, and social interference experienced by family caregivers caring for an adult, 65 years of age and older, with MCC.
The major problems faced in implementing an intersectionality analysis are sample size and the complexity of interpreting the results (Bauer, Reference Bauer2014; Dubrow, Reference Dubrow2008; Kohlman, Reference Kohlman2006; Scott & Siltanen, Reference Scott and Siltanen2012). The present study helps to overcome both of these challenges faced by quantitative intersectionality analysis. A repeated measures model was used to explore the effects of the caregiving experience over time on caregiver burden (primary dependent measure), as impacted by numerous caregiver characteristics, including gender; age; employment status, and degree of social interference experienced. Social interference captures impact on caregivers’ social life; it was determined to be an important caregiver characteristic to capture given its impact on the social lives of caregivers, and ultimately, their experience of social isolation. This type of intersectionality analysis pays attention to the multiplicative (interaction) effects of the major variables, as intersectionality is not simply additive. Based on the literature review, the group that would report the greatest caregiver burden was hypothesized to be younger employed females, who were experiencing a high degree of social interference.
Methods
Study Design and Participant Recruitment
The present study is part of a pan-Canadian program of research from the Aging, Community and Health Research Unit (Markle-Reid et al., Reference Markle-Reid, Ploeg, Valaitis, Duggleby, Fisher and Fraser2018). The goal of the research study was to promote optimal aging at home for older adults with multi-morbidity (two chronic conditions) and to provide support to their family/friend caregivers. A repeated-measures embedded, mixed-method, intersectionality design was used to address the research objective. The present study focuses on the intersectionality quantitative analysis of the data.
Participants
The target sample size was 200 caregivers of older adults with MCC, with 100 caregivers sampled from each province. According to Cohen’s (Reference Cohen1988) formula for calculating sample size using a moderate effect size (0.15) and a power of 80 per cent for regression with 15 independent variables (age, gender, employment status, social interference, age*gender, age*employment status, age*social interference, gender*employment status, gender*social interference, social interference*employment, age*gender*employment status, age*employment*social interference, age*gender*social interference, gender*employment status*social interference, age*gender*employment status*social interference), the required sample size is 139. Assuming a 10 per cent rate in loss to follow-up, we would need an additional 14 observations, hence bringing the total sample size to approximately 154 patients.
Inclusion criteria for the study were: (1) care recipient must be diagnosed with dementia, diabetes, or stroke in addition to a minimum of two other chronic conditions (Barnett et al., Reference Barnett, Mercer, Norbury, Watt, Wyke and Guthrie2012) (taken from a long list of more than 20 conditions) in the last six months prior to the caregiver participating in the research; (2) participant must be actively providing care to an older adult (65 years or older) with MCC living in the community; (3) participant must be 18 years of age or older; and (4) participant must be English speaking. Informal caregivers are defined as family and/or friends providing unpaid support to a person with MCC. Quantitative data were collected via telephone or face-to-face interviews over two time points: at the start of the study and after approximately six months. Qualitative data were also collected, but are reported elsewhere (Williams et al., Reference Williams, Sethi, Duggleby, Ploeg, Markle-Reid and Peacock2016).
A total of 194 caregivers of older persons with MCC were recruited into the study. A wide range of organizations in both Alberta and Ontario assisted with participant recruitment. In Alberta, key community partners included the Alzheimer’s Society and the Alberta Caregiver’s Association. In Ontario, the research team contacted home care organizations that provide services for seniors with MCC, such as Saint Elizabeth Health Care, and also contacted various research organizations working on seniors’ issues, such as the Gilbrea Centre for Studies in Aging at McMaster University.
With community partners, participant recruitment was facilitated through inclusion of advertisements in newsletters, short introductory presentations at support groups, and distribution of recruitment posters. Recruitment was also accomplished through circulation of recruitment materials, such as brochures, posters, and flyers, to the general public at local businesses and organizations. Advertisements were also placed in local newspapers, such as the Metro Edmonton, Hamilton Mountain News, and Coffee News, and were also posted on social media and Web sites. In order to best reach eligible participants, the research team targeted advertisements in selected neighborhood communities known to have a relatively high volume of seniors. Survey data were collected simultaneously with the recruitment process, which was conducted over a period of 12 months. Initial T1 surveys began in July 2013 and final T2 surveys were completed by June 2014.
Demographic Information
The variables that provide information on baseline characteristics of the caregiver population include: care recipient’s age, caregiver’s educational level, province of residence (Alberta or Ontario), financial needs met (yes or no), household income, employment status, marital status, relationship with care recipient (husband/wife/life partner or others), length of caregiving experience (in months), and number of chronic conditions.
Social Interference
Social interference is a category specifically designed to represent the level of interference that caregiving duties have on a caregiver’s social life. The following question taken from the SF-12 questionnaire (Ware, Kosinski, & Keller, Reference Ware, Kosinski and Keller1996) was used to capture the social interference experienced: “During the past 4 weeks how much of the time have your physical health or emotional problems interfered with your social activities, like visiting with friends, relatives etc.?” The possible responses to this question were: “All of the time”, “Most of the time”, “Some of the time”, “Very little of the time”, and “None of the time”. For analysis, the categories were further collapsed into high social interference (included “All of the time”, “Most of the time”), moderate social interference (“Some of the time”), and low/no social interference (“Very little of the time” and “None of the time”). Low or no social interference score describes caregivers who do not feel that their caregiving duties impede their social life, whereas high social interference indicates that caregivers are experiencing difficulty managing their social life as a direct consequence of their caregiving role. We hypothesized that the group of individuals with high social interference would experience a negative impact on their caregiver burden.
Zarit Burden Inventory (ZBI)
The ZBI (dependent variable) is a self-administered questionnaire and a popular method used to measure caregiver burden. Multiple versions of the ZBI exist to accommodate different study settings. The original ZBI consists of 29 items and produces a burden score between 29 and 145 (Martin-Carrasco et al., Reference Martin-Carrasco, Otermin, Perez-Camo, Pujol, Aguera and Martin2010). A shorter version of the ZBI has been developed and tested. It consists of 12 items, and the score ranges from 0 to 48 (Garlo et al., Reference Garlo, O’Leary, Van Ness and Fried2010; Ware et al., Reference Ware, Kosinski and Keller1996). In either version of the ZBI, the items are quantified, using a five-point Likert scale, with zero representing “never” and four representing “nearly always” (Gort et al., Reference Gort, Mingot, Gomez, Soler, Torres and Sacristan2007). Therefore, the scores are generally interpreted as a low score representing a low caregiver burden, and a high score reflecting that a caregiver is experiencing extreme emotional and role strain. The ZBI has been proven to be a valid and reliable tool for determining caregiver burden by Seng et al. (Reference Seng, Luo, Ng, Lim, Chionh and Goh2010). The authors used a 22-item ZBI on caregivers of patients with dementia in Singapore, and have reported scores of 0.93 for the Cronbach’s α value, and 0.89 for the intraclass correlation coefficient for the test–retest reliability, in a sample size of 149 participants (Seng et al., Reference Seng, Luo, Ng, Lim, Chionh and Goh2010). Although the main objective of using a ZBI is to measure the caregiver burden, Gort et al. (Reference Gort, Mingot, Gomez, Soler, Torres and Sacristan2007) and Martin-Carrasco et al. (Reference Martin-Carrasco, Otermin, Perez-Camo, Pujol, Aguera and Martin2010) have discovered that it can also be used to predict caregiver collapse, especially for those caring for someone with dementia. Overall, the ZBI is a feasible and reliable method to measure caregiver burden among different types of caregivers. ZBI score was treated as a continuous variable for the analysis.
Data Collection
Prior to data collection, ethics approval was received from the University of Alberta Health Research Ethics Board (Pro00039895) and the McMaster University Research Ethics Board (2013 104). Survey data were collected from each caregiver participant by trained research assistants at two time points: at baseline (T1) and again after six months (T2). The purpose of this timed collection was to capture the dynamic nature of caregiving for older adults with MCC. Surveys were conducted with participants over the phone, via Skype, or in person. Informed consent was obtained from participants who participated in a face-to-face interview as well as by telephone interview. Each participant was given one copy of the consent form to keep and another was completed and retained by the researchers. Consent forms were sent by mail to the participants who chose the telephone or Skype interview. A small number of participants (∼ 4–6 in total) completed the surveys by hand and returned them through regular mail. Individuals in the study were compensated for each session in the form of cash or gift card, valued at $25.
During T1 and T2, caregivers were asked to complete a health-related quality of life survey (SF-12 and McGill Quality of Life), General Self-Efficacy (GSE), 12-item Short-form ZBI, the Bem Sex Role Inventory, a Work Interferences Scale (Reid, Stajduhar, & Chappell, Reference Reid, Stajduhar and Chappell2010), and a constructed survey on frequency and types of formal services accessed. Demographic information was also collected during the T1 survey. For the purpose of this article, only the short-form ZBI will be examined, which employs a 5-point Likert scale format. The dependent variable was the ZBI score.
Study Variables
The intersectionality analysis took into account five categorical variables, which were chosen to be most common factors that could be associated with caregiver burden: age, gender, education, employment, and social interference. The age of the caregiver was split into younger caregiver (less than 65 years) versus older caregiver (65 years or age or older; reference). Gender was male versus female (reference), education was categorized into no university (includes no high school and high school) versus university (reference), employment status was employed (includes full time, part-time, self-employed) versus unemployed or not working (reference). Social interference was categorized into high social interference, moderate social interference, or low/no social interference (reference). For the additive and multiplicative model, the variables that were analyzed were from the T1. Restricting the variables to the T1 variables only was for three main reasons. First, the changes measured between the two time points for social interference and employment status were not significantly different. Second, similar models were run for T2 as well and the results were similar. Third, as the results were similar between T1 and T2, T1 values were used because we had complete data on 194 subjects.
Data Analysis
A standardized code book was used for all data entry to minimize error across the two participating centers. Each categorical variable was assigned a code, which was used to keep consistency between the two study centers.
Demographic characteristics were analyzed using descriptive statistics. Means and standard deviations were reported for continuous variables, and frequencies and proportions were reported for categorical variables. The change in ZBI was assessed using paired t-tests, and the change in categorical variables (employment status and social interference) was calculated using McNemar’s test.
The percent change was calculated using the formula:
 $$Percent\,change = {{Change\,in\,score\,from\,3\,months\,to\,baseline} \over {Baseline\,values}}$$
$$Percent\,change = {{Change\,in\,score\,from\,3\,months\,to\,baseline} \over {Baseline\,values}}$$
A generalized linear model (GLM) was used to analyze the caregiver ZBI score, which was treated as a continuous variable. Univariate GLM was conducted to determine the main effects of the additive model. Model 1 included caregiver age, model 2 included caregiver gender, model 3 included caregiver education, model 4 included caregiver employment, and model 5 included caregiver’s social interference. The final model 6 included all of the variables together.
For the intersectionality analysis, the multiplicative approach was used (Dubrow, Reference Dubrow2008). For this approach, two-way, three-way, four-way, and five-way interaction terms were used to account for the conditional effects of the intersecting variables with caregiver burden. The model helped us to determine the multiplicative effects of caregiver burden related to the caregiver: age, gender, employment status, education, and social interference experienced. The estimate for the multiplicative model was calculated using the following formula, where β0 = intercept, g = gender, a = caregiver’s age, e = caregiver’s education, si = social interference and emp = employment status. X represents the interaction terms.
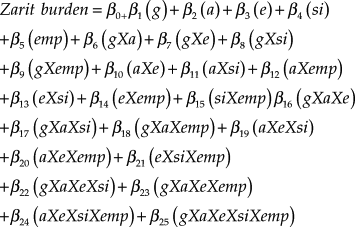 $$Zarit\,burden = {\beta _{0 + }}{\beta _1}\left( g \right) + {\beta _2}\left( a \right) + {\beta _3}\left( e \right) + {\beta _4}\left( {si} \right) + {\beta _5}\left( {emp} \right) + {\beta _6}\left( {gXa} \right) + {\beta _7}\left( {gXe} \right) + {\beta _8}\left( {gXsi} \right) + {\beta _9}\left( {gXemp} \right) + {\beta _{10}}\left( {aXe} \right) + {\beta _{11}}\left( {aXsi} \right) + {\beta _{12}}\left( {aXemp} \right) + {\beta _{13}}\left( {eXsi} \right) + {\beta _{14}}\left( {eXemp} \right) + {\beta _{15}}\left( {siXemp} \right){\beta _{16}}\left( {gXaXe} \right) + {\beta _{17}}\left( {gXaXsi} \right) + {\beta _{18}}\left( {gXaXemp} \right) + {\beta _{19}}\left( {aXeXsi} \right) + {\beta _{20}}\left( {aXeXemp} \right) + {\beta _{21}}\left( {eXsiXemp} \right) + {\beta _{22}}\left( {gXaXeXsi} \right) + {\beta _{23}}\left( {gXaXeXemp} \right) + {\beta _{24}}\left( {aXeXsiXemp} \right) + {\beta _{25}}\left( {gXaXeXsiXemp} \right)$$
$$Zarit\,burden = {\beta _{0 + }}{\beta _1}\left( g \right) + {\beta _2}\left( a \right) + {\beta _3}\left( e \right) + {\beta _4}\left( {si} \right) + {\beta _5}\left( {emp} \right) + {\beta _6}\left( {gXa} \right) + {\beta _7}\left( {gXe} \right) + {\beta _8}\left( {gXsi} \right) + {\beta _9}\left( {gXemp} \right) + {\beta _{10}}\left( {aXe} \right) + {\beta _{11}}\left( {aXsi} \right) + {\beta _{12}}\left( {aXemp} \right) + {\beta _{13}}\left( {eXsi} \right) + {\beta _{14}}\left( {eXemp} \right) + {\beta _{15}}\left( {siXemp} \right){\beta _{16}}\left( {gXaXe} \right) + {\beta _{17}}\left( {gXaXsi} \right) + {\beta _{18}}\left( {gXaXemp} \right) + {\beta _{19}}\left( {aXeXsi} \right) + {\beta _{20}}\left( {aXeXemp} \right) + {\beta _{21}}\left( {eXsiXemp} \right) + {\beta _{22}}\left( {gXaXeXsi} \right) + {\beta _{23}}\left( {gXaXeXemp} \right) + {\beta _{24}}\left( {aXeXsiXemp} \right) + {\beta _{25}}\left( {gXaXeXsiXemp} \right)$$
All statistical analyses were conducted using the Statistical Package for the Social Sciences v21 (SPSS; http://www.spss.com). Two-sided tests were used for all statistical comparisons and a p value of < 0.05 was used for all statistical significance.
Results
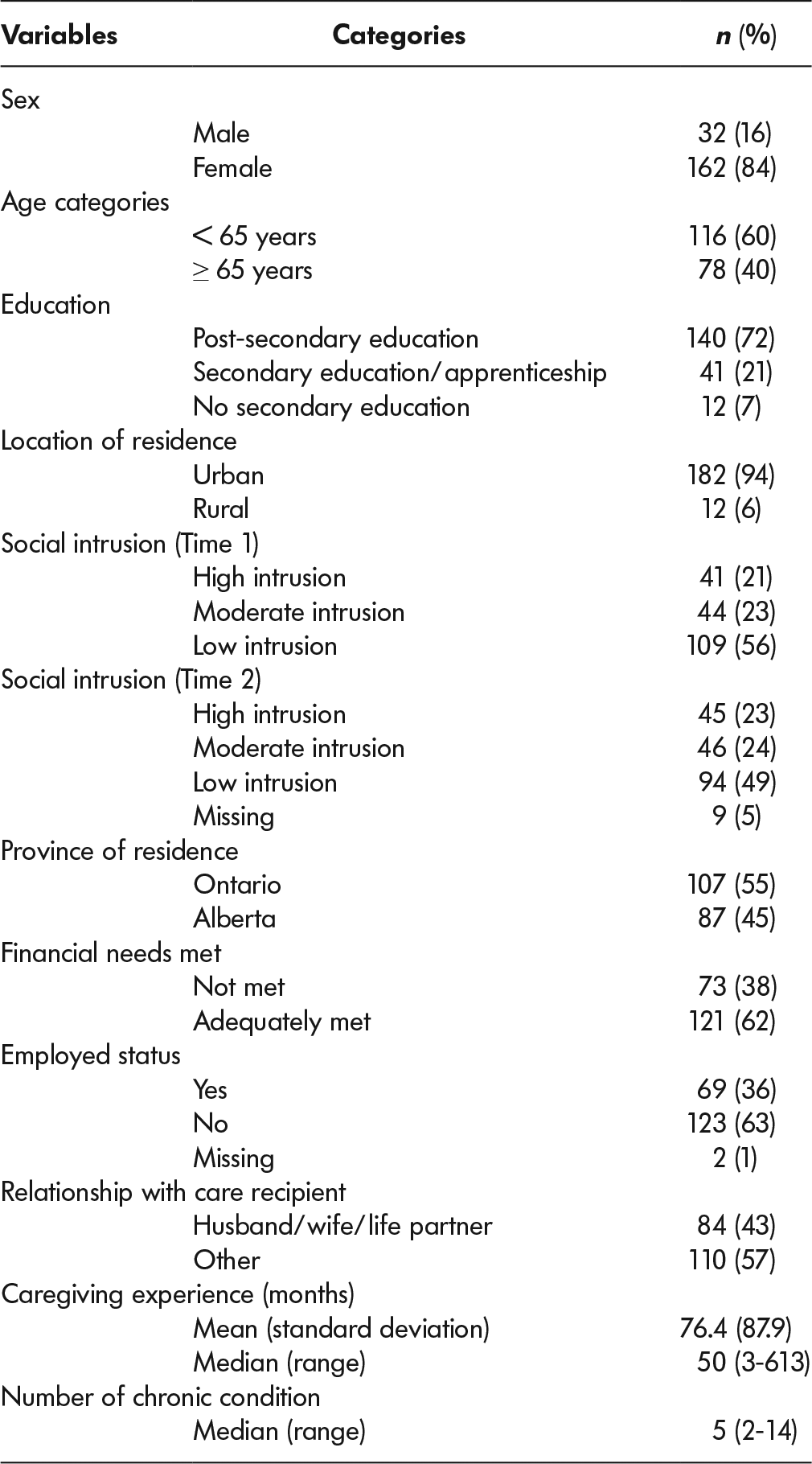
A total of 194 participants who met the inclusion criteria were recruited from both Alberta (45%) and Ontario (55%). The proportion of caregivers less than 65 years of age was 59.8 per cent (n = 116) and those 65 years of age and older was 40.2 per cent (n = 78). The majority of the care recipients were 71 years of age and older (92.3%). The majority of the caregiver participants were female (n = 162, 84%), which is typical in a caregiver setting. Approximately 69 per cent of the caregivers were married, and 67.5 per cent were living with the care recipient. The relationships of the caregiver with the care recipient were of spouse (husband/wife) (43%) or adult child (son/daughter) (45%). Annual household incomes of the caregiver were more than $70,000 for approximately 31 per cent, less than $70,000 for approximately 51 per cent, and 18 per cent preferred not to answer. Financial needs were met with some difficulty or not very well for approximately 36 per cent of the caregivers. A majority of the participants had completed a post-secondary education (72.2%, n = 140) and were living in urban geographical communities (93.8%, n = 182). Only 36 per cent of the caregivers were employed (included self-employed and employed full time or part time) and approximately 63 per cent were unemployed. The median number of multiple chronic conditions reported by the care recipients was 5, ranging from 2 conditions to a maximum of 14. The median length of caregiving time was approximately 50 months, ranging from 3 months to a maximum of 613 months. Table 1 lists the details of the participant demographics.
Table 1: Participant demographics at baseline (Time 1)
As for the caregiver burden, the average ZBI score at T1 was 21.27 (standard deviation [SD] = 9.14), and at T2, the score decreased to 19.64 (SD = 9.16). There was an 8.4 per cent decrease Zarit burden score from baseline to 6 months. This change in the ZBI score was statistically significant (p < 0.0001). However, the ZBI at both time points indicates that the burden score was severe/high (Bedard et al., Reference Bedard, Molloy, Squire, Dubois, Lever and O’Donnell2001). Employment status also showed a minimum decrease of 2.89 per cent from T1 to T2, but the change was not statistically significant (p = 0.238). Social interference as defined by the SF12 question “physical health or emotional problems interfered with social activities categories” showed a positive change of 23 per cent for the category “all of the time”, the category “most of the time” showed a positive change of 3.57 per cent, the category “some of the time” showed a change of 4.55 per cent, the category “a little of the time” showed a decrease of 13.04 per cent, and the category “none of the time” showed a decrease of 14.29 per cent. The change in social interference was not statistically significant between baseline and the 6 months time point (p = 0.532). Table 2 summarizes the changes over time.
Table 2: Descriptive statistics for the study variables at the two study time points
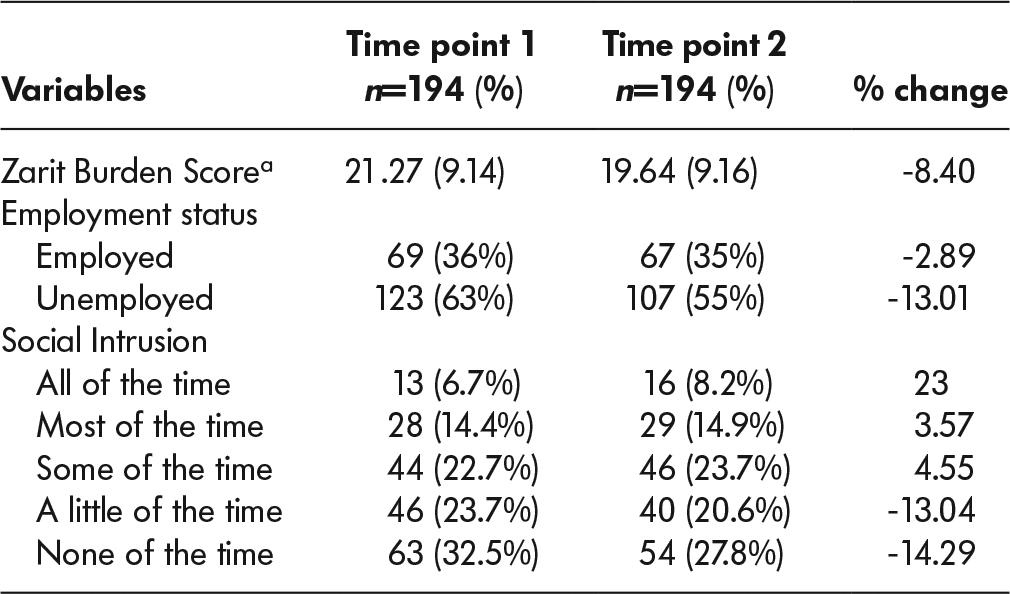
Note. aMean and standard deviation is provided for the continuous variable.
The subjective burden of the study participants was the dependent variable for the present study. Table 3 provides the additive model along with beta estimates and standard error (SE) and the respective p values. Males had significantly lower ZBI scores (-5.30) than females (model 1), younger caregivers (less than 65 years of age) had 5.65 units of significantly higher burden scores than older caregivers (model 2). Caregivers who had a high school education or less had 2.89 units of significantly less Zarit burden than university-educated caregivers (model 3). Full-time or part-time employed caregivers also showed 3.14 units of significantly higher Zarit burden than unemployed caregivers (model 4). Caregivers with high social interference had 10.85 units of significantly higher burden score, and caregivers with medium social interference had approximately 8.08 units higher Zarit burden score than caregivers with low social interference.
Table 3: Additive model
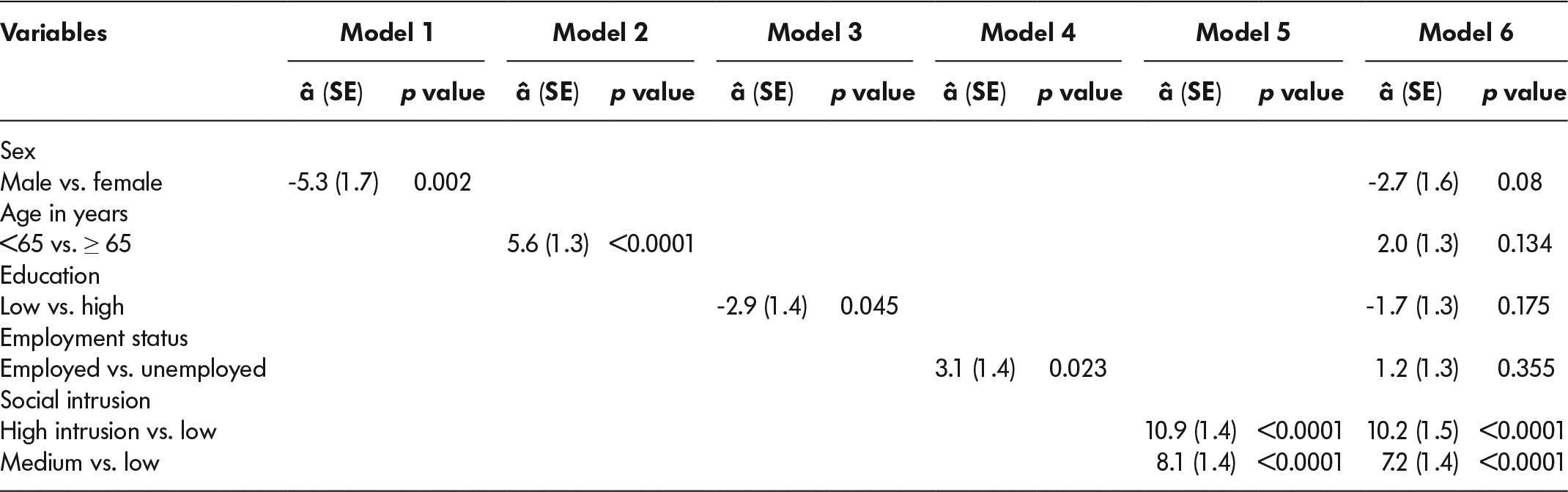
Note. SE = standard error.
Model 6 presents multivariate analysis with all five variables. Social interference was an independent predictor of Zarit burden score. The results show that when adjusted for age, gender, education, and employment status, medium-high social interference categories were significantly associated with higher burden compared with lower levels of social interference.
Table 4 presents the results of the multiplicative model. Our model includes the two-way, three-way, four-way, and five-way interaction model. Figure 1 summarizes the major findings of the multiplicative model. The ZBI score is presented on the y axis. The results indicate that the highest burden was experienced by males younger than 65 years with a university education, and males who reported high social interference. Burden was very high in both employed (a score of 35.45) and unemployed males (a score of 34.45). Educated employed older females with medium social interference had a burden score of 32.93. Younger unemployed females with high social interference and low education, as well as younger employed females with high education and high social interference, also reported very high burden scores, 31.8 and 31.36, respectively. The burden scores were above 30 units in these categories, suggesting severe burden. A high burden score (a score above 20) was also observed mostly in females with medium-high social interference, irrespective of their age, education, or employment status. A mild to moderate burden score (score 10–20) was observed in most of the groups. The no to mild burden scores (score 0–10) were observed among males only. Scores for unemployed younger males with low education and no social interference were approximately 2.36 units, followed by older employed, educated males with no social interference who had a score of approximately 7. The overall results of the five-way interaction suggest that males in general had lower burden scores than females. Irrespective of their education and employment status, females had generally higher burden scores.
Table 4: Multiplicative model representing the parameter estimated calculated using the interaction method
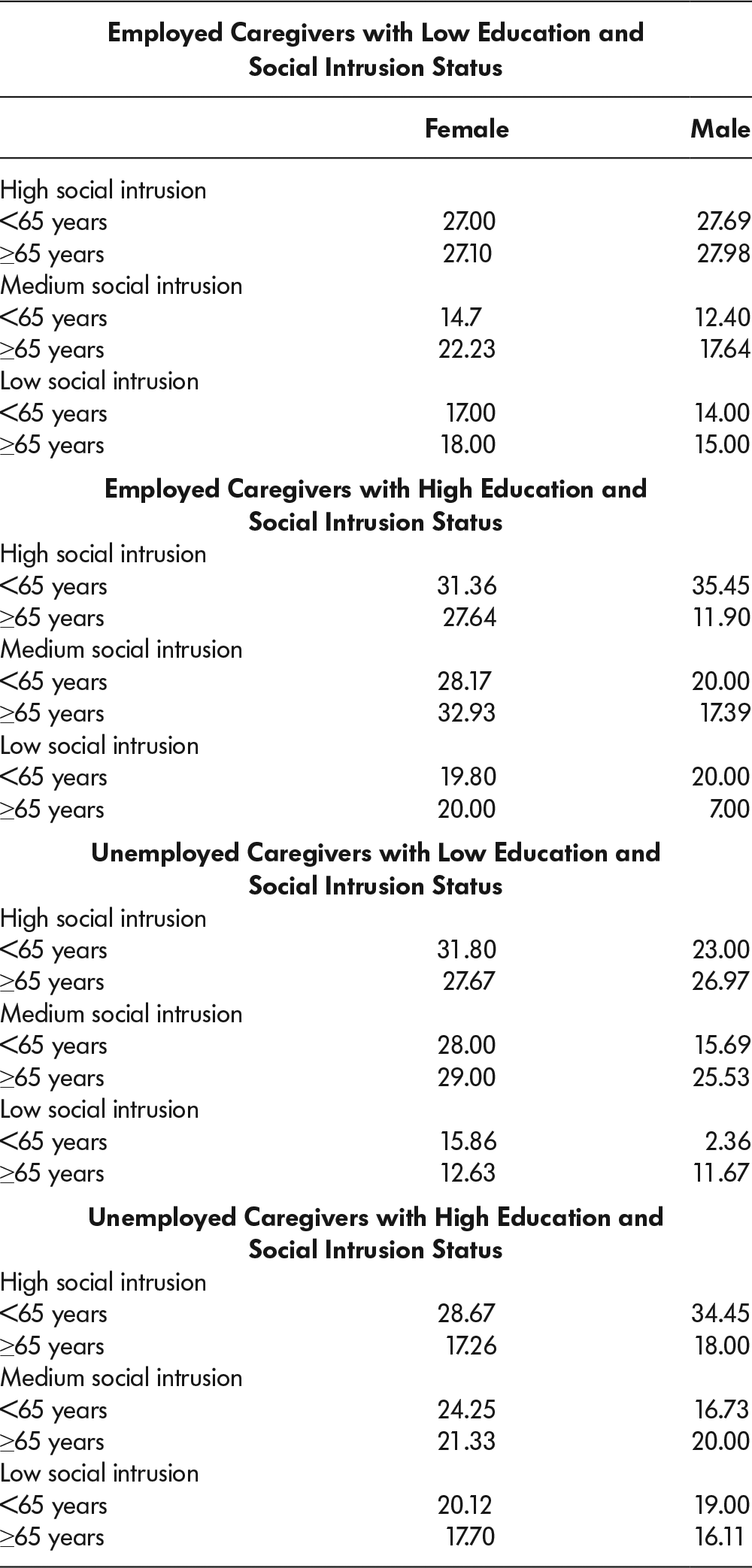
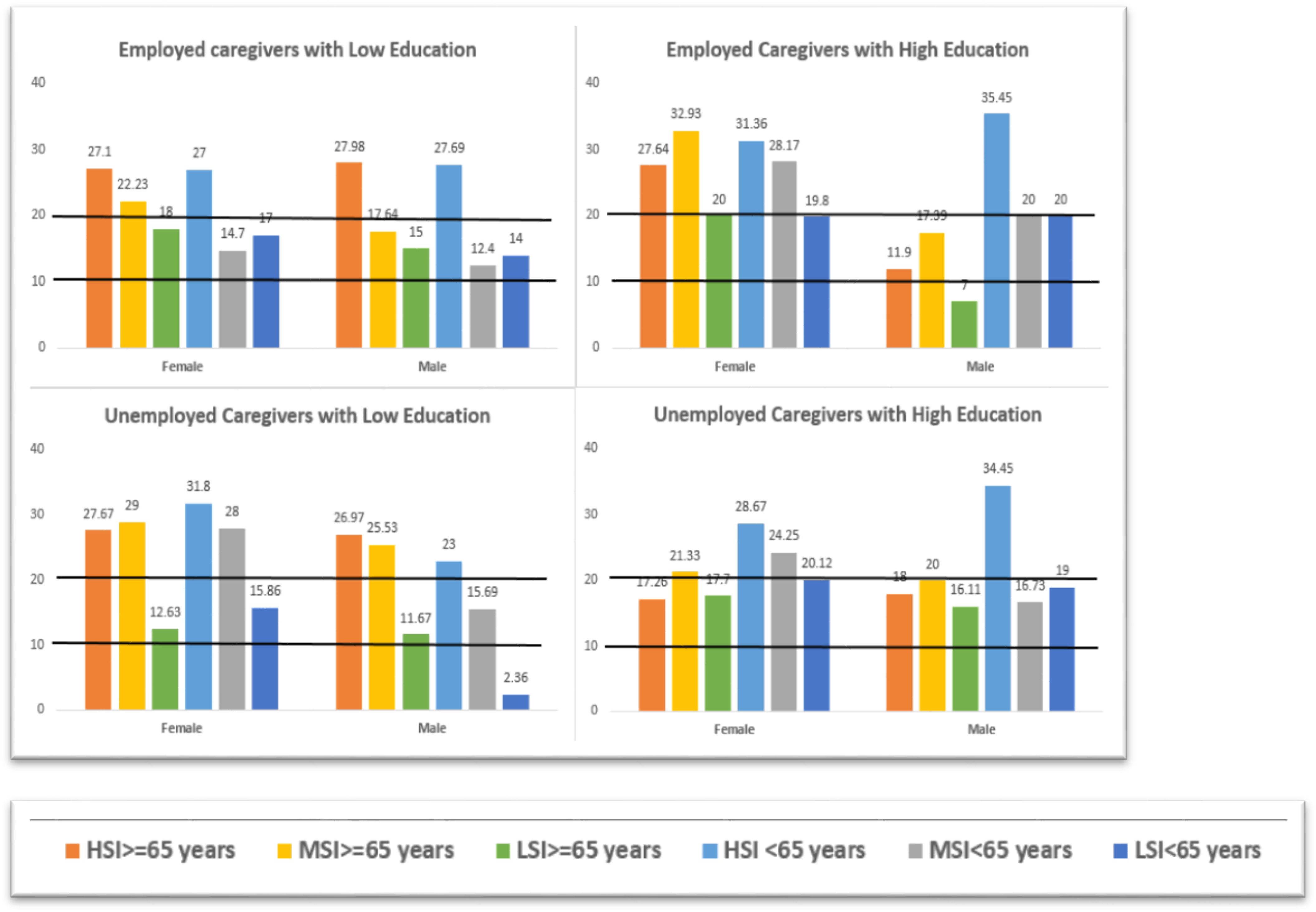
Figure 1: Zarit burden score derived from the multiplicative model representing the severity of burden by employment status, education level, and gender. The solid line at the score of 20 represents severe burden, and solid line at the score of 10 represents mild burden. HSI = high social interference; MSI = moderate social interference; LSI = low/no social interference.
Discussion
Educated males less than 65 years of age with high social interference experienced a significantly higher caregiver burden, irrespective of their employment status. Employed or unemployed females with medium-high social interference also experienced severely high burden scores, which was true irrespective of their age or education status. Unemployed or employed males with no social interference had the lowest burden score, which was true irrespective of their age or education. Overall, the caregiver burden was higher for females in almost all the categories compared with males, with few exceptions. One of the other factors that added to the higher level of burden was associated with the out-of- pocket expenses incurred by the caregiver, which affects a caregiver irrespective of gender (Duncan, Shooshtari, Roger, Fast, & Han, Reference Duncan, Shooshtari, Roger, Fast and Han2016; Shooshtari, Duncan, Roger, Fast, & Han, Reference Shooshtari, Duncan, Roger, Fast and Han2017). The Zarit burden score was in the mild to moderate range for males and females with low social interference, indicating that support and help from family and friends definitely assisted in their ability to manage. Employed females with high education had a higher burden score, indicating that the pressure at work, together with caregiving, as well as a limited social life, has a negative impact on the caregiver. Similarly, unemployed females with low education and medium-high social interference also had high burden scores, suggesting a negative impact on these caregivers. The results do indicate that social interference has a negative impact on caregivers.
The intersectionality approach had been valuable in critically examining the role of employment and social interference factors, which can vary according to cultural and geo-social contexts. Unlike a binary understanding of the variables, the intersectionality approach has fostered a better understanding of the intricate relationship provided by the different factors making up the collective experience of caregiver burden. However, the five-way interactions may introduce complexity and uncertainty into the conclusions, as multiple interactions involve multiple comparisons.
Compared with other caregiver populations who deal with patients with chronic conditions, current participants’ average ZBI score on the shorter version with 12 items was 21.3 (SD = 9.14); this was greater than for those who care for cancer patients (12.0; SD = 8.5) (Higginson, Gao, Jackson, Murray, & Harding, Reference Higginson, Gao, Jackson, Murray and Harding2010), patients with dementia (15.1; SD = 10.0) (Higginson et al., Reference Higginson, Gao, Jackson, Murray and Harding2010), and similar to the score for those who care for patients with acquired brain injury (21.7; SD =10.1) (Higginson et al., Reference Higginson, Gao, Jackson, Murray and Harding2010). Whereas caregivers who care for persons with cancer or dementia fall into the “little to no” burden category, other chronic condition scenarios – such as acquired brain injuries and MCC, place caregivers in the “high to severe” category, as predicted by Bedard et al., (Reference Bedard, Molloy, Squire, Dubois, Lever and O’Donnell2001).
Younger employed male caregivers who have high social interference suffer the most and have very high/severe caregiver burden. Female caregivers, irrespective of their age and employment status, who have medium-high social interference, also experience very severe burden. These populations need to be flagged for additional supports. However, further studies are needed to confirm these results. Further research that includes the addition of income in the model will be helpful to further understand this population.
Limitations
While recognizing the strengths of the study’s longitudinal design, the quantitative intersectionality analysis, and the appropriate sample size, there are a number of limitations to be considered. The present study contributes to the understanding of caregiver burden in relation to caregiver characteristics, as well as to care recipient traits, but it is limited by both internal and external factors, emphasizing the need for continued research. The sample was a convenience sample, which limits the generalizability of the study findings. However, the feasibility of a random sampling of caregivers is very difficult, as population registries typically do not include data about who is a caregiver, or whether the care recipient has MCC (Markle-Reid et al., Reference Markle-Reid, Ploeg, Valaitis, Duggleby, Fisher and Fraser2018). The study was part of a pan-Canadian program of research, hence, we included two provinces in the study. Recruiting participants over a longer period could potentially reduce biases arising from selective attrition, and also address the severely burdened individuals who may have been excluded during the first round of recruitment. Additionally, the number and the intensity of MCC of both the caregiver and the care recipient may have influenced the data and study results. For example, a patient with diabetes would require different services and time commitment than those recovering from stroke, or if the caregiver and the recipient both have identical diagnoses, they may be more likely to share the burden. The variance in the method of data collection as well as among researchers (e.g., style of interviewing) could have also influenced the results. Furthermore, a more rigorous approach to measuring social interference would provide confirmation of the findings presented herein.
Another limitation of the study is that because of the complexity of the multiple co-morbidity data, we were unable to collect data on functional and cognitive status and hence could not adjust accordingly in the analysis. We had a higher proportion of persons with dementia; hence we could not run the analysis adjusting for different MCC separately.
Conclusion
The aging population will continue to be a growing concern as people begin to live longer with MCC. The aim of this research was to better understand the reported burden of family caregivers caring for older persons with MCC over time. The analysis of individual and compound characteristics in relation to caregiver burden corroborated much of the existing research, as well as adding to the knowledge base with new evidence. Although age, gender, employment, and social interference each had statistical significance, the interaction among the variables also demonstrated a significant effect. Although age and gender usually serve as confounders, they were the most influential on the model, indicating that the dominant effects of age and gender, along with modifications by employment and social interference, might be replicated in the larger population. Paying particular attention to the needs of younger male caregivers who are employed and have moderate or high social interference, as well as older and younger female caregivers, would be highly recommended for health care providers, because these target populations have shown greater likelihood of experiencing aggravated role strain. Although this finding may be useful in Alberta and Ontario, there remains a significant gap in research to confidently apply this discovery to other geo-social contexts.





