



Lesions at the cranio-cervical junction, specifically the occipital condyle, are rare. These patients often present with occipital condyle syndrome (OCS), a unilateral occipital pain with ipsilateral tongue paresis exacerbated by contralateral head rotation. Reference Greenberg, Deck and Vikram1 This presentation is typically due to metastasis from another site and less frequently a primary malignancy, which can be regionally invasive and carry a poor prognosis. Reference Rodríguez-Pardo, Lara-Lara and Sanz-Cuesta2 Though rarer, a lesion in the cranio-cervical junction may also be a meningioma. Reference Rushing, Bouffard and McCall3 The proximity of vital structures such as the vertebral artery makes surgically accessing tumors in the occipito-atlanto region difficult, making obtaining a biopsy challenging. Reference Rhoton4 However, to optimize patient outcomes, confirmation of the diagnosis is crucial in tailoring patient management and to determine if the benefits of surgery outweigh the risks.
Here, we outline the technique for a percutaneous fluoroscopically guided transoral left occipital condyle biopsy with CT angiogram guidance. This revealed an unexpected primary meningioma and altered the patient’s care trajectory. To our knowledge, this is among the first reports of a primary extracranial meningioma centered on the occipital condyle.
A 68-year-old woman with no prior history of malignancy presented with 2 months of progressive left-sided neck pain radiating to her shoulder accompanied by a deep headache in her left ear. Neurologic exam revealed mild left hypoglossal nerve palsy and left tongue atrophy. The patient reported a loss of taste, dysphagia, and voice hoarseness. She also noticed increased drooling and biting on the inside of her cheek.
An MRI revealed a lytic lesion in the left anterior petrous bone, replacing the left occipital condyle, with the involvement of the left jugular foramen. This was hypointense on T2 and was homogenously enhanced with gadolinium (Figure 1). Metastatic workup including further imaging of the chest, abdomen, and pelvis was unremarkable.
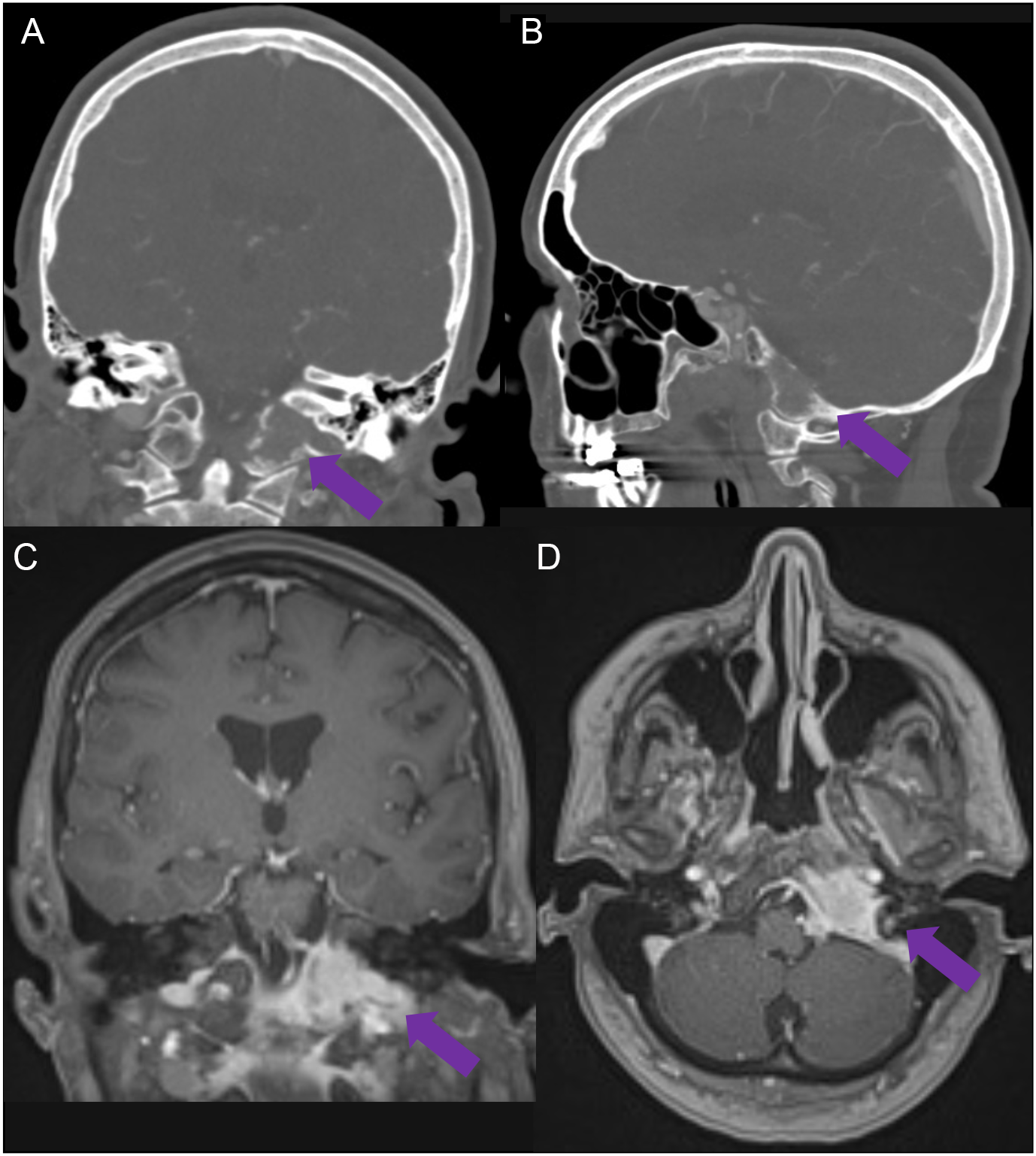
Figure 1: Coronal and sagittal bone window CT scans demonstrating a lytic lesion centered at the left occipital condyle with anterior extension and involvement of the left jugular foramen (A,B). Contrast-enhanced MRI demonstrates avid enhancement of the lesion with significant bone involvement (C,D).
Percutaneous fluoroscopically guided transoral biopsy in the biplane neuroangiography suite (Allura Clarity, Philips Electronics, Eindhoven, Netherlands) under general anesthesia was performed to obtain pathologic diagnosis. The patient was supine and intubated via nasal route, with a large bite block and lip spreaders employed to maximize mouth opening and visualization. Non-contrast cone beam CT was used to plan needle placement and confirm satisfactory patient position and orientation. This was followed by a contrast-enhanced cone beam CT scan to visualize head and neck vasculature, focusing on the left internal carotid artery. Biopsy needle trajectory was planned based on this combined data set, which created an XperCT in the XperGuide software (XperGuide, Philips Electronics, Eindhoven, Netherlands) (Figure 2).

Figure 2: Completion axial (A) and sagittal (C) cone beam CT scan confirming final position of biopsy needle with needle trajectory overlay as a comparator. Fluoroscopic AP (B) and lateral (D) images acquired with needle in final position prior to biopsy acquisition. Coronal (E) and axial (F) contrast-enhanced CT scans captured in the arterial phase of imaging allow for planning of the needle entry trajectory (magenta line). Arterial contrast allows for avoidance of local vascular anatomy and minimizes potential hemorrhagic complications. Projected needle tip end point is represented by the final green circle. Green circle mid-way along the trajectory represents needle location on the current slice.
Using XperGuide, a 4 cm 13-gauge SuperCore guiding cannula (Argon Medical Devices, Plano, Texas, USA) was advanced transorally into the soft tissue overlying the left occipital condyle. A 14-gauge, 2 cm throw length, and 9 cm total length side cutting biopsy needle was inserted through the cannula to retrieve two 1 cm long biopsies (Figure 2).
Only minor bleeding was encountered, which was controlled using autologous blood clot embolization via the guiding cannula and manual compression upon needle removal. The postoperative course was uneventful, and the patient was admitted for observation overnight as a precaution and discharged the following day.
The biopsy was consistent with a WHO grade 1 meningioma. Surgery was not recommended due to the low tumor grade and its involvement of jugular and hypoglossal foramen. Surgical intervention for this lesion would require a complex skull base approach to access, likely with significant associated morbidity. The patient was ultimately referred for radiation therapy.
Due to its association with disseminated metastasis or development of a primary tumor, OCS is a red flag for malignancy. Reference Rodríguez-Pardo, Lara-Lara and Sanz-Cuesta2 Primary tumors of the upper cervical spine tend to have a poor prognosis and include chondrosarcomas, osteosarcomas, and chordomas, which are regionally invasive and difficult to treat. Reference Abdu and Provencher5 However, other types of primary tumors in this region exist and may rarely include extracranial meningiomas, which account for 1–2% of all meningiomas. Reference Rushing, Bouffard and McCall3 Due to their rarity, these tumors are often misdiagnosed and not managed adequately.
Although these tumors can be atypical or malignant, extracranial meningiomas are usually associated with a benign natural history. Reference Rushing, Bouffard and McCall3 More common primary tumors such as chordomas have a mean survival time without surgery of less than 1 year and post-surgical 5- and 10-year survival times of 62 and 39%, respectively. Reference Eriksson, Gunterberg and Kindblom6,Reference Choi and Gleeson7 While life expectancy survival rates for cranio-cervical meningiomas are not well reported, extracranial meningiomas as a group have an overall medial survival of 28 years. Reference Rushing, Bouffard and McCall3 Because both benign and malignant tumors of the upper cervical spine can share the same clinical and radiographic presentation, the ability to obtain a biopsy can drastically change the treatment plan and can help confirm the prognosis of the suspected tumor.
Historically, accessing the cranio-cervical junction requires a complex approach and mobilization of critical structures such as the V3 segment of the vertebral artery, dislocation of the mandible, and/or drilling of the occipital condyle. Reference Rhoton4 The associated morbidity means that malignancies in this region are often treated empirically with radiation, chemotherapy, or resection without pathologic diagnosis. Reference Russo, Morana and Mistretta8
Recently, less invasive approaches such as tubular and transoral approaches have been devised, marking a potential shift in the management of occipital condyle malignancies. Reference Russo, Morana and Mistretta8 The ability to safely retrieve a biopsy enables diagnostic confirmation and provides details of tumor characteristics to guide management and treatment. This may minimize overall morbidity by allowing tailored management and confirming if an invasive surgical procedure is necessary. A recent report from Russo and colleagues describes the use of angiography to identify local vasculature to ensure avoidance of a hemorrhagic complication. Reference Russo, Morana and Mistretta8 We suggest that in a stable, intubated patient, an on-table, contrast-enhanced CT scan taken with care to ensure arterial phase of contrast serves as a less invasive alternative to localize key arterial structures in the region. The current method allows the clinician to forego the need for arterial access and direct catheterization of cerebral vasculature. If there is heightened concern regarding carotid or vertebral artery bleeding, the alternative approach utilizing direct arterial access and contrast administration described by Russo and colleagues may be performed as this would allow for intra-arterial balloon placement that allows for direct control of a potential vascular injury. Reference Russo, Morana and Mistretta8
To highlight the utility of a biopsy in the management of OCS, we describe an up-front transoral biopsy of the lesion, which enabled the diagnosis of a low-grade meningioma. After consideration of the risks of surgery and alternative therapies, this diagnosis did not necessitate surgical management. This information contributed to the decision to treat the patient with radiation instead of surgical resection, thus minimizing up-front surgical morbidity.
Competing interests
None.
Statement of authorship
M.R.: Conceptualization, Methodology, Data Collection, Supervision, Writing – Original Draft, Writing – Review & Editing, Resources, Investigation
K.O.: Methodology, Data Collection, Writing – Original Draft, Writing – Review & Editing, Visualization, Investigation
R.A.: Conceptualization, Project Administration, Supervision, Writing – Review & Editing, Resources, Data Curation, Investigation
M.H.: Conceptualization, Methodology, Project Administration, Supervision, Writing – Review & Editing, Resources, Data Curation, Investigation
Ethics
This study has been approved by the local research ethics board.



 Open access
Open access