



Introduction
Epilepsy is a chronic neurologic disorder that affects over 50 million people worldwide, independent of an individual’s age, race, or socioeconomic background. Reference Wiebe, Blume, Girvin and Eliasziw1–Reference Meinardi, Scott, Reis and Sander4 The principal manifestation is a spontaneous recurrence of unprovoked seizures, which can be classified as generalized or focal onset. Reference Fisher, Cross and French5
The treatment of patients with epilepsy most commonly involves anti-seizure medications. While these are the first line therapeutic intervention, they are only effective in preventing seizures in around 70% of individuals. In people with focal epilepsy where medication cannot provide seizure freedom, epilepsy surgery provides a greater likelihood of seizure remission than ongoing medical treatment. Reference Wiebe, Blume, Girvin and Eliasziw1,Reference Englot and Chang6 Epilepsy surgery should be offered to individuals where the long-term consequences of seizures overshadow the immediate risks of an invasive operation. Reference Wiebe, Blume, Girvin and Eliasziw1,Reference Engel7
Presurgical evaluation, such as identifying a patient’s language lateralization, is essential in determining surgical candidacy. Language lateralization is the extent to which an individual’s language functioning demonstrates a hemispheric specialization within the brain. Reference Bradshaw, Thompson, Wilson, Bishop and Woodhead8 Identifying a patient’s dominant language hemisphere allows clinicians to infer the side of seizure onset, for instance if the semiology of focal seizures involves prominent language impairment, seizure onset is likely within the language dominant hemisphere. Reference Ni, Wang, Yu, Wu and Wang9 Clinicians can also use this information to predict the potential postsurgical language deficits that may occur as a result of the resection of epileptogenic areas, communicate these surgical complications to the patient, and obtain patient consent that is fully informed. Reference Bernat and Peterson10,Reference Szaflarski, Gloss and Binder11
Past techniques to lateralize language include the dichotic listening test and the intracarotid amobarbital (Wada) test. The Wada test was the previous gold standard for the preoperative assessment of language laterality in patients undergoing epilepsy surgery. However, it has been gradually phased out of preoperative evaluations and replaced by functional magnetic resonance imaging (fMRI) which is a more cost-efficient, noninvasive and safer alternative. Reference Janecek, Swanson and Sabsevitz12 Several studies have shown a significant concordance between the two techniques, with one study reporting a 90% agreement for the calculation of language laterality indices. Reference Janecek, Swanson and Sabsevitz12–Reference Bauer, Reitsma, Houweling, Ferrier and Ramsey15 The use of fMRI for language lateralization as a presurgical tool has many benefits in its ability to predict postoperative deficits. Studies have demonstrated that patients with epilepsy who have a greater left lateralization of language functioning, evaluated by fMRI, show poorer naming performance one year following left temporal surgery. Reference Bonelli, Powell and Thompson16–Reference Trimmel, van Graan and Gonzálvez18
Language lateralization using fMRI can be assessed by many paradigms that are not equivalent and may produce different patterns of fMRI activation which will directly impact a patient’s lateralization results. Despite the clinical relevance and growing acceptance of fMRI for language lateralization, this technique is not standardized as the design of paradigm sequences varies significantly worldwide. Reference McAndrews and Cohn14 While the heterogeneity of fMRI paradigms used in clinical practice can provide effective laterality assessments for patients within an epilepsy surgery center, challenges arise when making quantitative comparisons between centers. While each epilepsy surgery center may have a completely effective paradigm series for the presurgical assessment of language laterality, attempts at standardization would increase the communicability, reproducibility and interpretability of laterality results between centers which in turn may reveal current disparities and opportunities for improvement. The extent of variation around the world, particularly in Canada, likely stems from competing scientific approaches that may evaluate certain paradigms more useful than others. Some organizations, such as the American Society of Functional Neuroradiology (ASFNR), have taken great strides to provide well-informed and reliable recommendations for fMRI paradigms to efficiently lateralize language abilities in patients with various neurological disorders. Reference Black, Vachha and Mian19 Through institutional polling, broad literature reviews and expert opinion, the ASFNR designed a three-tier fMRI sequence of the most commonly employed language paradigms (Figure 1). However, to increase the willingness of institutions to adopt standardized fMRI language lateralization practices, additional scientific and clinical evidence regarding the efficiency of language paradigms must be acquired and shared across communities.
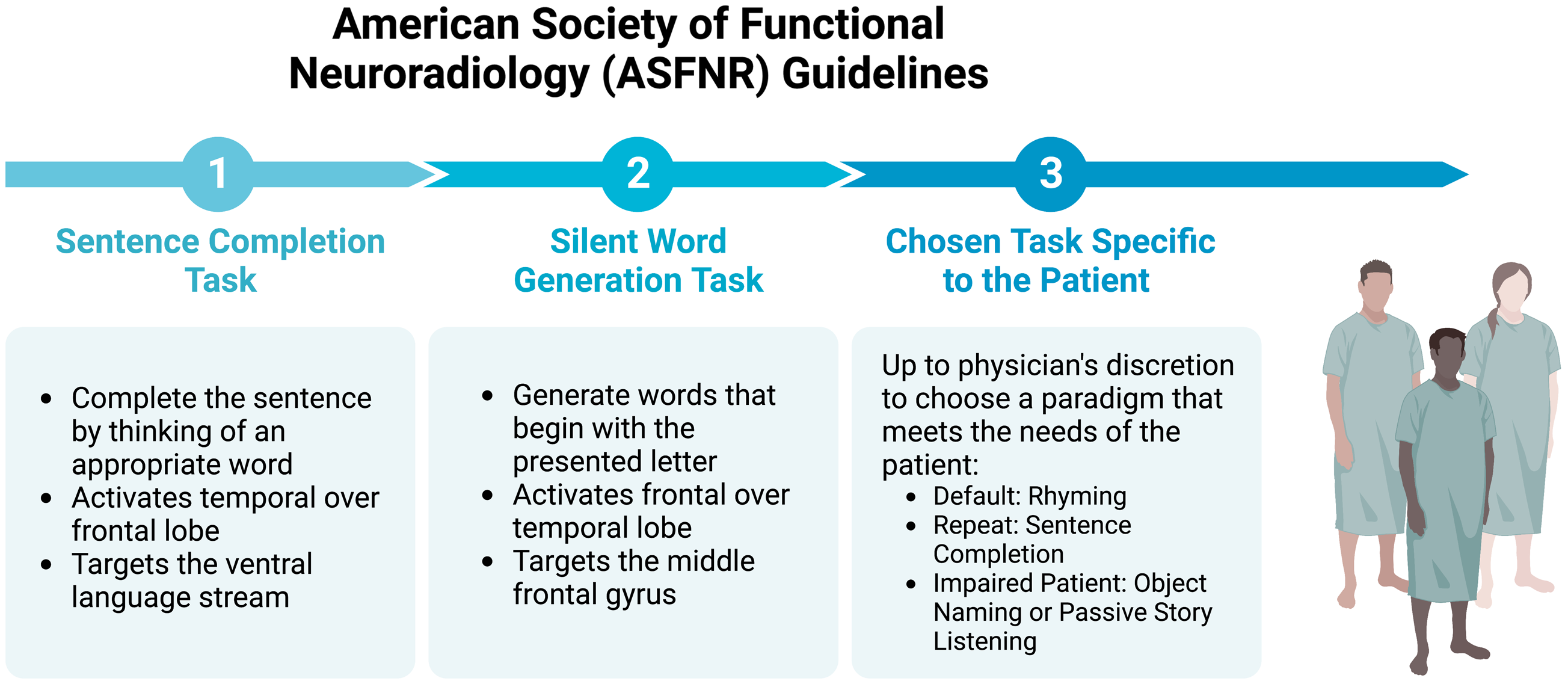
Figure 1. American Society of Functional Neuroradiology (ASFNR) three-tier functional magnetic resonance imaging (fMRI) language lateralization guidelines. According to the ASFNR, language laterality assessments using fMRI should follow a default algorithm consisting of a sentence completion task, a silent word generation task and a third task chosen by physicians to best meet the specific needs of their patients. Created with BioRender.com.
To ensure the appropriate acquisition of language lateralization results, language paradigms must fulfill certain criteria. Since language functioning is composed of many types of skills including pragmatics, semantics and syntax, there is general agreement that at least two paradigms should be employed to sufficiently assess language lateralization. Reference Black, Vachha and Mian19 Furthermore, the paradigms should be designed such that they are able to effectively determine the interhemispheric lateralization of both receptive and expressive language ability. Therefore, to be successful as a preoperative technique, fMRI for language lateralization must involve standardized paradigms that are reproducible and efficient.
In this study, we survey epilepsy surgery programs across Canada and collect information on their current fMRI paradigms, discuss the limitations of heterogeneity in language lateralization fMRI paradigms, and set forth two adoptable paradigms for language lateralization with the goal of solidifying a best-validated approach.
Methods
Review of existing literature
To understand the various perspectives and approaches to lateralizing language using fMRI, a review of the existing literature was performed using PubMed. Search terms included the following: functional magnetic resonance imaging (fMRI), language lateralization, epilepsy, language paradigms, presurgical language fMRI, laterality indices and clinical language fMRI protocols. The selection criteria for publications included controlled clinical trials as well as systematic reviews with no limitations placed on the publication’s country or date. Additional articles of relevance were identified through backward reference searching and forward reference searching. Information was extracted on the cognitive design and efficacy of fMRI language paradigms, software for the analysis of fMRI results, the use of programing tools for the calculation of laterality indices, as well as established consensus statements.
Survey of canadian epilepsy centers
Canadian centers with epilepsy surgery programs that may utilize fMRI for language lateralization were contacted to participate in an interview regarding their practices. Through video conferencing, data were collected from six epilepsy surgery programs in Nova Scotia, Quebec, Ontario and Alberta. Two additional centers in British Columbia and Alberta were approached for participation but did not respond.
Using a survey, professionals speaking on behalf of their institution’s practices answered questions regarding the cognitive design of fMRI language paradigms, protocol structure, image acquisition, data analysis, the use of software and/or programing tools, interpretation of the results, the use of alternative methods for assessing language laterality and the clinical application of the lateralization results. The questions were designed to be comprehensive and flexible to allow respondents to elaborate on their answers (Supplementary Table 1).
Optimal language paradigms and protocols
To establish optimal fMRI paradigms for the purpose of lateralizing language, information acquired through the literature review and surveying of Canadian epilepsy surgery programs was considered. To develop the most pragmatic approach, language tasks have to fulfill specific criteria: (1) the paradigm must be validated by various epilepsy surgery centers, (2) the paradigm should demonstrate a high degree of reliability and efficacy in lateralizing language functioning for both patients with epilepsy and healthy volunteers, (3) the paradigm must be appropriately challenging for individuals with average or near-average IQ and normal literacy skills, and (4) the use and implementation of the paradigm should be time and cost-efficient. The development of protocol for fMRI language lateralization was also guided by existing literature and information from Canadian epilepsy surgery programs. This included the specifics of each paradigm’s block design and sequence, the time allotted to each paradigm, the presentation of stimuli along with the corresponding software, methods to ensure compliance and the use of control tasks that effectively differentiated language functioning from unrelated brain activity.
Results
Canadian Epilepsy Centre survey
Among the six Canadian Epilepsy Centres that were surveyed, there was variation observed between each institution’s respective ‘standard’ fMRI language practices (Table 1 and Table 2). The fMRI language lateralization assessments across all respondents consisted of three different paradigms.
Table 1. Standard fMRI parameters among Canadian Epilepsy Centres compared to the American Society for Functional Neuroradiology Guidelines
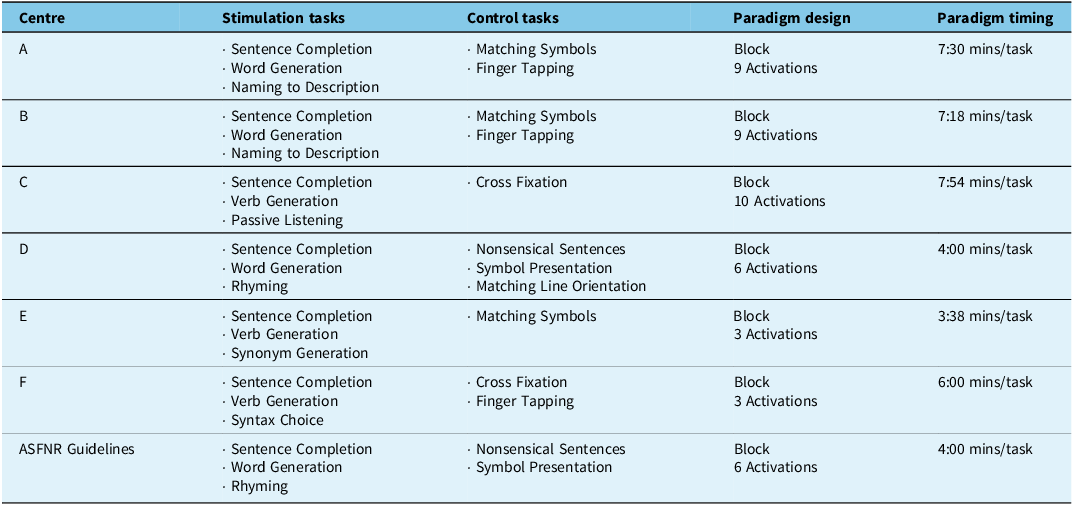
ASFNR = American Society of Functional Neuroradiology.
Table 2. Information regarding fMRI contrast analysis, calculations of laterality indices and chosen threshold values among the Canadian Epilepsy Centres
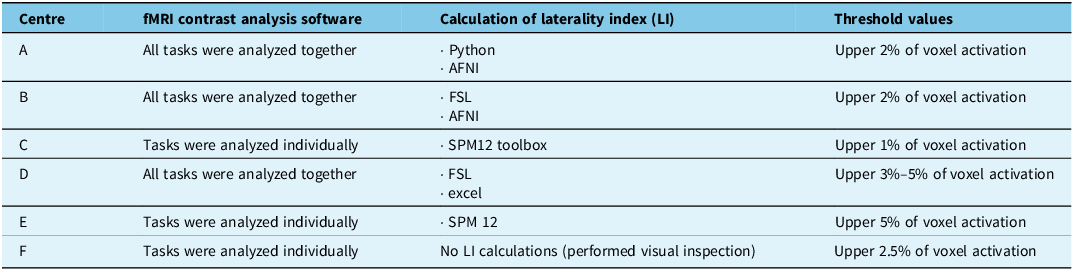
AFNI = Analysis of Functional NeuroImages; fMRI = functional magnetic resonance imaging; FSL = FMRIB Software Library; SPM = Statistical Parametric Mapping.
The collected data demonstrated that the Sentence Completion Paradigm was the most frequently employed language task among respondents (5/6) while the Word Generation and Verb Generation Paradigms were equivalently used among half the respondents (3/6) (Figure 2). While similar forms of the Sentence Completion, Word Generation and Verb Generation paradigms were used by the majority of Canadian Epilepsy Surgery Centres, these paradigms showed heterogeneity in their structure, timing and choice of stimuli content between centers (See Discussion Section B. Potential Pitfalls of Stimuli Variation). Alternative tasks that did not demonstrate widespread utility included the Naming to Description, Rhyming, Synonym Generation, Passive Listening and Syntax Choice Paradigms. To compensate for individuals who may have intellectual deficits or below average literacy skills, respondents reported slowing down the language paradigms or replacing challenging stimulation tasks for more manageable alternatives.
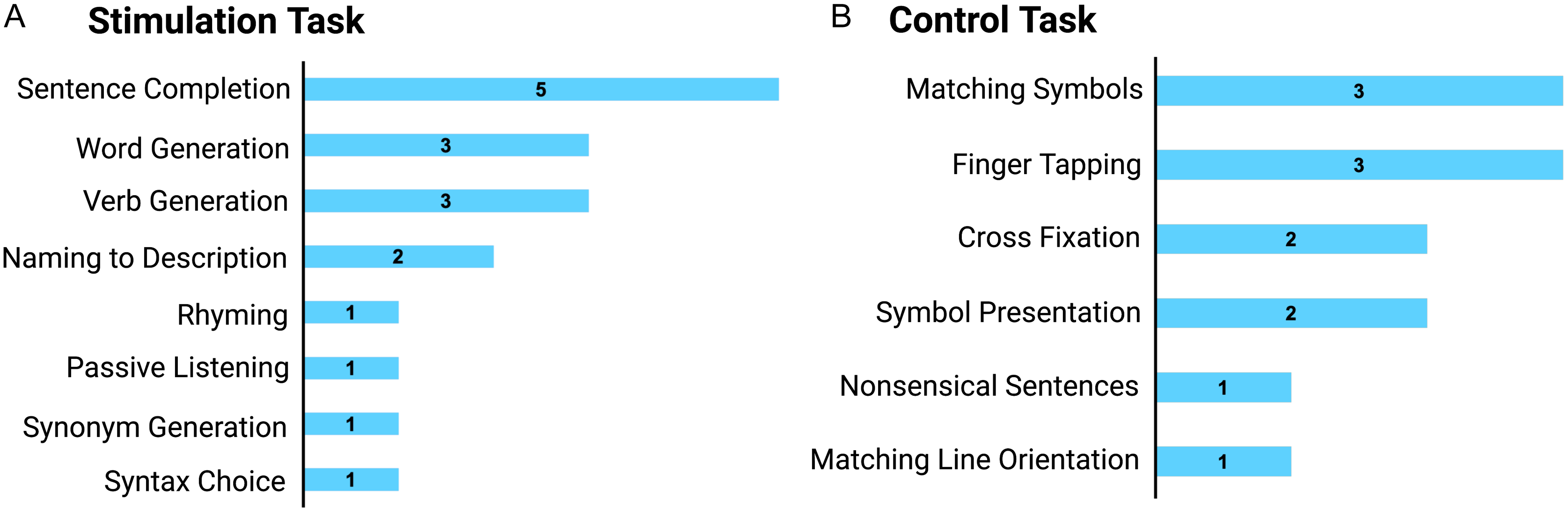
Figure 2. Frequency of various stimulation tasks (A) and controls tasks (B) among the language paradigms implemented at the surveyed Canadian Epilepsy Centres. Created with BioRender.com.
The choice of control tasks, which were used to provide contrast for the fMRI analysis, also demonstrated variation among the Canadian Epilepsy Centres. All respondents acknowledged that their control tasks were designed to eliminate visual sensory processing or motor activations such that the language functioning demands present in the active task could be sufficiently isolated during fMRI analysis. The most commonly employed control tasks that were generalized to various stimulation tasks included the Matching Symbols (3/6), Finger Tapping (3/6) and Cross Fixation tasks (2/6) (Figure 2). These tasks were not designed to eliminate specific patterns of brain activity one might expect to see between various active language tasks. In contrast, complementary control tasks, such as the Nonsensical Sentences and Symbol Presentation, were employed alongside the Sentence Completion and Word Generation tasks, respectively. By designing control tasks that were as similar to the activation tasks as possible, the Nonsensical Sentences and Symbol Presentation control tasks were reported to dissociate unrelated activity, inherent to the task, from patterns of activity indicative of language functioning. Control tasks that were specifically designed to the stimulation tasks were less often implemented by the various Canadian Epilepsy Centres.
The paradigm design always consisted of a block structure with a varying number of blocks. There was no consensus regarding the timing of various paradigms which reportedly ranged between three minutes, 38 s (3:38) to seven minutes, 54 s (7:54). Furthermore, the choice of fMRI data analysis, the use of software and/or programing tools, and interpretation of the results were unique to each institution (Table 2).
All survey responses regarding fMRI practices were compared to supporting literature, which included the recommendations made by the American Society of Functional Neuroradiology (ASFNR). Reference Black, Vachha and Mian19 Through polling all surgical centers that held ASFNR memberships, this organization evaluated the convergence of language paradigms across various institutions. With this information, they recommended a default 3-tier paradigm series for the presurgical evaluation of language lateralization. The paradigm series consisted of a Sentence Completion, Word Generation and a Rhyming task. Reference Black, Vachha and Mian19 For all ASFNR members, the respective stimuli for each paradigm were made freely available on their website.
Outlining a sentence completion and word generation paradigm series
Using information acquired through the Canadian Epilepsy Centre Survey, in combination with consensus statements in supporting literature, we outlined, with the intention to implement and test the efficacy of versions of the Sentence Completion (SC) and Word Generation (WG) language paradigms. These paradigms, in addition to a Rhyming task, are involved in the formal recommendation made by the ASFNR to evaluate language laterality in patients with various neurological disorders. Rather than recreating the slightly more complex ASFNR paradigm series, we were motivated to outline a paradigm series that could reliably assess laterality in various language areas while balancing simplicity and considering resource efficiency such that Canadian Epilepsy Surgery Centres may adopt them with ease.
Both paradigms were produced using PsychoPy, a free open-source programing software based on the Python coding language. Each language paradigm routine was formulated as a block design consisting of two consecutive blocks, each representing a different condition for 30 s: the stimulation task and the corresponding control task (Figure 3). For the choice of paradigm stimuli, prompts recommended by the ASFNR guidelines were supplemented with local additions. The two-block routine was repeated six times such that each condition was presented for a total of 180 s. Each paradigm routine was preceded by a 10 s baseline, which provided the participant with an instructional prompt, either “Sentence Completion” or “Word Generation”, before the task began. After the completion of the paradigm routine, a 5 s exit screen was presented which thanked the volunteer for their participation.
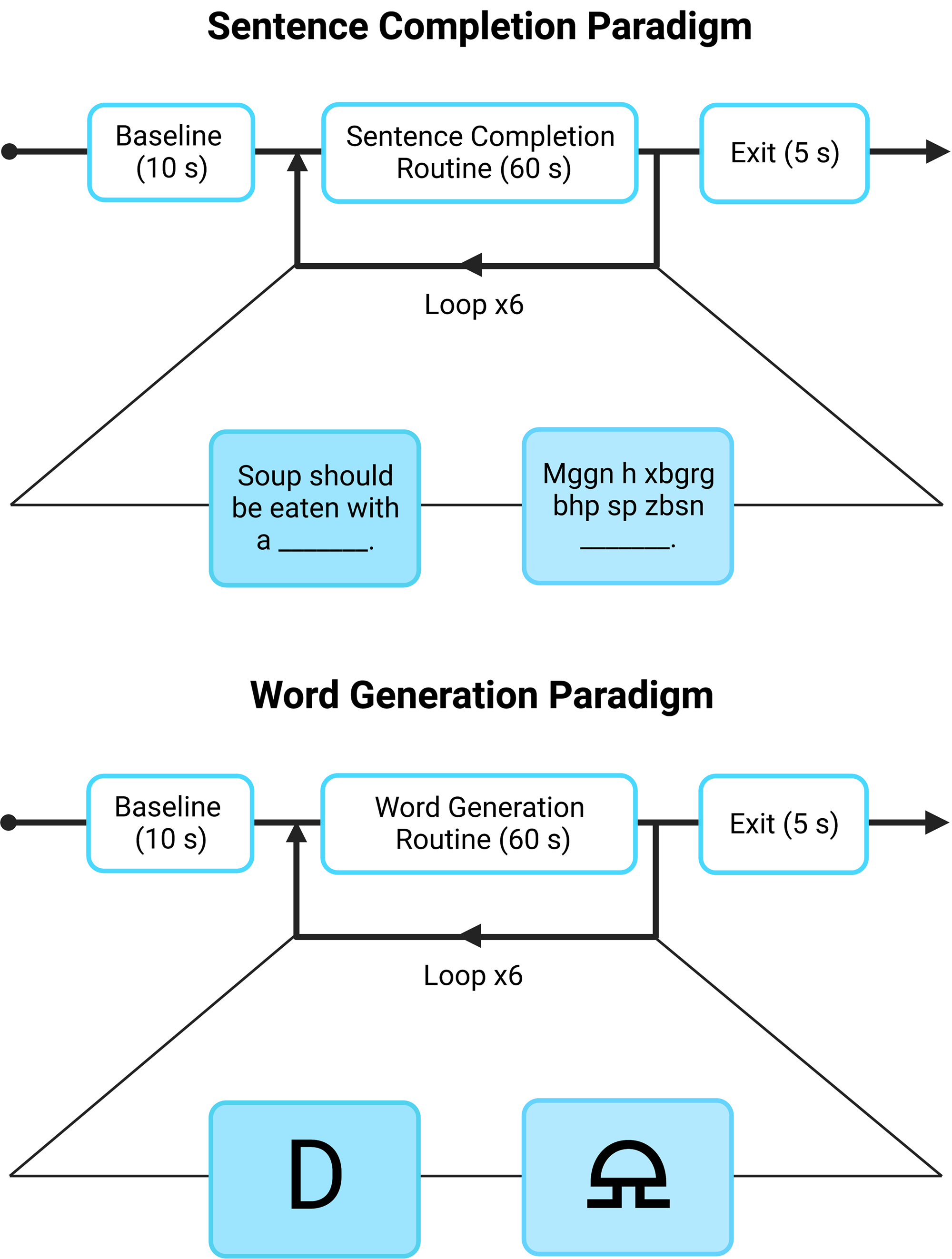
Figure 3. Illustration of the functional magnetic resonance imaging sentence completion and word generation paradigm. (A). Examples of potential sentence and nonsense condition stimuli are demonstrated. The entire paradigm lasts 6 minutes and 10 s with a total of 180 s being spent in condition. (B). Examples of potential letter and symbol condition stimuli are demonstrated. The entire paradigm lasts 6 minutes and 10 s with a total of 180 s being spent in each condition. Created with BioRender.com.
The SC routine involved the consecutive presentation of the sentence and nonsense conditions (Figure 3). The sentence stimulation task involved the presentation of incomplete sentences where participants would be instructed before the fMRI session to think of a grammatically correct word, without vocalizing their answer, that could appropriately complete the sentence. Each sentence stimulation block presented five stimuli for six seconds each. In contrast, the complementary nonsense control task involved the presentation of nonsensical sentences based on “gibberish” control sentences provided by the ASFNR. During the nonsense condition, participants would be instructed before the fMRI session to move their gaze over the presented gibberish text without demonstrating phonological or phonemic practices which include naming the letters or segmenting the gibberish into separate sounds. These nonsensical sentences are designed to exclude semantic, syntactic and lexicalization activity that would be present and required in the active task while also controlling for the activation in the frontal eye fields responsible for moving one’s gaze over a sentence when reading. Reference Black, Vachha and Mian19 Each nonsense control block presented five stimuli for six seconds each.
The WG routine involved the consecutive presentation of the letter and symbol conditions (Figure 3). The letter stimulation task involved the presentation of letters where participants would be instructed before the fMRI session to think of as many words as they could that began with that letter, without vocalizing their answer. Each letter stimulation block presented two stimuli for 15 s each. Alternatively, the complementary symbol control task involved the presentation of nonsense symbols where the participants would be instructed before the fMRI session to gaze at the nonsense symbol and refrain from thinking of any letters or words. The nonsense symbols are intended to eliminate the verbal fluency activity involved in the word generation task while also controlling for the activation in areas involved in visual activation. Reference Black, Vachha and Mian19 Each symbol control block presented two stimuli for 15 s each.
Discussion
We demonstrate significant variation regarding fMRI practices for lateralizing language function in people with epilepsy across Canadian centers. This suggests that clinical practices could benefit from standardized practices to improve communicability between institutions, enhance patient outcomes and enhance methodologies in the surgical treatment of epilepsy. A set series of paradigms for language lateralization, chosen with guidance from literature and clinical utility, were outlined.
The functional delineation of the sentence completion and word generation tasks
The SC task, the most widely employed task across Canadian Epilepsy Centres, has been found to effectively lateralize activity in Wernicke’s Area (WA). Reference Black, Vachha and Mian19–Reference Zacà, Jarso and Pillai21 This region, located in Brodman area 22, is responsible for receptive language abilities including comprehension, semantic processing and language production. Reference Salek, Hassan and Kotrotsou20 Studies that investigated the SC task in lateralizing receptive speech areas demonstrated its effective robustness compared to alternative speech paradigms in right-handed, left-handed and ambidextrous individuals. Reference Salek, Hassan and Kotrotsou20
In contrast, verbal fluency tasks such as the word generation and verb generation tasks were the second most common type of paradigm implemented across Canadian Epilepsy Centres. The subtle difference between these two tasks involves the participant receiving a specific letter cue and being asked to covertly think of any word, such as a noun, verb, or adjective, or receiving a noun and being instructed to exclusively think of associated verbs, respectively. However, performance measured in reaction times between these two similar verbal fluency tasks is related to vocabulary size and access speed into one’s orthographic lexicon, which is a storage system for the spelling of familiar words. Reference Friedman, Kenny and Wise22,Reference Shao, Janse, Visser and Meyer23 As a result, by limiting the participant’s responses to just the verbs, as directed in the verb generation task, one may expect to see poorer performance than the word generation task that accepts more inclusive responses.
The WG task and has been validated as an effective paradigm for lateralizing expressive aspects of language in Broca’s Area (BA) as well as the inferior, middle and superior frontal gyri. Broca’s area, found in Brodmann’s areas 44 and 45, mediates expressive aspects of language such as speech production. Reference Black, Vachha and Mian19,Reference Brannen, Badie, Moritz, Quigley, Meyerand and Haughton24 The frontal gyri exhibit robust activity during this paradigm as well since this form of verbal fluency requires phonological processing, working memory and novel search strategies into an individual’s orthographic lexicon. Reference Zacà, Jarso and Pillai21
Overall, the widespread acceptance of the SC and WG paradigms across Canadian Epilepsy Centres, as well as the supporting evidence provided from relevant literature, validate this two-part paradigm series presented here as a standardized method in lateralizing language. By providing a thorough engagement of receptive and expressive aspects of language, through covert tasks that are designed to optimize performance for individuals with average or near-average IQ and normal literacy skills, the fMRI results will likely yield lateralizing activity in primary and secondary language areas.
Potential pitfalls of stimuli variation
The exact choice of stimuli used for language fMRI paradigms was largely dictated by individual centers, thereby contributing to an additional source of heterogeneity. For example, using the SC task as an example, stimulus prompts may differ such that the missing word from the sentence may be concrete or abstract nouns and/or verbs. Concrete nouns and verbs refer to an object that exists in the real word such as “spoon,” “ice” or “airplane” or a literal action such as “stop,” “melt” or “pay.” Reference Mitchell, Shinkareva and Carlson25,Reference Moseley and Pulvermüller26 Importantly, studies have identified common neural activations of concrete nouns across individuals to the extent that one can predict a pattern of activity generated by a specific concrete noun. Reference Mitchell, Shinkareva and Carlson25–Reference Just, Cherkassky, Aryal and Mitchell27 Therefore, by designing standardized stimuli for the SC task where the missing words are concrete nouns or verbs, the variation of neural patterns between different brains will be minimized.
Minimizing variation between individual’s neural activity for the WG task proves more challenging due to the unconstrained nature of the stimuli. When presenting a letter to an individual and allowing them to think of any word that begins with that letter, the patterns of activity generated from this task may vary between people due to their unique responses. While the effect may be negligible when determining laterality and comparing results between individuals, one may also consider modifying this task to include a semantic component. Instead of presenting a letter, a semantic category could be presented where an individual would generate words within that category. Reference Hwang, Palmer, Basho, Zadra and Müller28 For example, when presented with a stimulus such as “clothing”, appropriate answers would be “skirt”, “jacket”, or “blouse”. Since semantic categories have neural patterns that are similarly distributed between individuals, the extent to variation in fMRI activations can be minimized. Reference Moseley and Pulvermüller26–Reference Hwang, Palmer, Basho, Zadra and Müller28
Choice of control tasks
The choice of control task is an additional component to consider when designing paradigms to lateralize language ability fMRI lateralization. An effective control task must be designed to minimize the effects of other variables, such as non-language activity, from the independent variable, language activity, that is being evaluated by a paradigm. As demonstrated in Table 1, Canadian Epilepsy Centres demonstrate variation when it concerns their choice of control tasks. Examples of control tasks for language paradigms have varying levels of engagement, ranging from finger tapping and matching symbols to viewing a cross fixation. The goal of designing any control task is to subtract out non-language components from a task such as visual activation. For the SC and WG tasks, examples of control tasks are shown in Figure 3 and include a nonsensical sentence and the presentation of a symbol.
The inclusion of the nonsensical sentence as the control condition is designed to mimic processes involved in the SC task that are irrelevant to lateralizing language including eye movements for scanning a sentence and subsequent visual processing. Reference Ashtari, Perrine and Elbaz29 Since these nonsensical sentences do not include real words with underlying semantic concepts, the lateralizing patterns of receptive aspects of language can be effectively analyzed. In addition, they are designed to exclude semantic, syntactic and lexicalization demands involved in the SC task such that these language processes can be effectively lateralized when examining condition-control contrasts. Similarly, for the WG task, the presentation of the symbol as the control task is designed to eliminate areas of activity not involved in verbal fluency, such as visual processing. Reference Black, Vachha and Mian19 Unlike control tasks that require more engagement and decision-making, such as matching symbols, the presentation of nonsense symbols is most similar to the active task with the only difference being the presence of verbal fluency requirements. Therefore, the subtraction procedures involved in fMRI analysis for each task will strongly enhance the lateralizing patterns of receptive and expressive language functioning by diminishing activity involved in visual demands.
Heterogeneity in fMRI analysis tools and techniques
While the choice of language tasks among the Canadian Epilepsy Surgery Centres is a source of variation within the evaluation of language laterality, the fMRI analysis tools and techniques also contribute to the heterogeneity of this clinical practice. In turn, both the paradigm design and subsequent methods of analysis would benefit from a standardized approach across Canadian Epilepsy Surgery Centres to improve the reproducibility and interpretability of language laterality results.
To assess the extent of lateralization of language functioning from fMRI results, a laterality index (LI) is typically evaluated. An LI is a measure of the number of voxels that are active above a fixed threshold in the right hemisphere versus the left hemisphere. Reference Seghier30 In turn, this value is therefore subject to change depending on the thresholding value an institution decides to use. As demonstrated in Table 2, each center reported using a different threshold of activation for their LI calculations, ranging from the top 1 to 5% of activated voxels. While the range of threshold values used by the various Canadian Centres is considered stringent, there is no strong consensus which may contribute to challenges when interpreting and comparing results between centers. For example, if a conservative threshold value is chosen, one may unintentionally exclude relevant voxels involved in language functioning. However, a more lenient threshold value may include irrelevant activity in the LI analysis that may inappropriately skew the individual’s results and mislead a clinician’s evaluation. However, there are many different methods of thresholding. The most common method of thresholding involves applying a p-value cutoff from a t- or F-value statistic to each voxel’s activity. Reference Gross and Binder31 Alternatively, or in combination with a p-value cutoff, a cluster size threshold approach may be employed which requires a minimum number of adjacent voxels to be activated and show spatial correlations. Reference Gross and Binder31 While the thresholding method of each Canadian Epilepsy Centre was out of the scope of our questionnaire, a combination of these two approaches, both the p-value cutoff on spatially correlated voxels, will likely produce acceptable maps that demonstrate areas of lateralized language activity and significant LI calculations.
In addition, many different forms of software are used across Canadian Epilepsy Centres for LI calculations. These include Python, Analysis of Functional NeuroImages (AFNI), FMRIB Software Library (FSL), Statistical Parametric Mapping (SPM) 12 and Microsoft Excel. One center chose to perform only visual inspections on each individual’s fMRI results. Moreover, whether each center chose to analyze their tasks together or independently also revealed variability. Therefore, while we cannot confirm which thresholding value and approach, software, or analysis method is most advantageous and reliable in determining language lateralization in individuals with epilepsy, our future directions will investigate these questions. Importantly, a standardized analysis across Canadian Epilepsy Centres will improve communicability between institutions regarding fMRI results, enhance patient outcomes and enhance methodologies in the surgical treatment of epilepsy.
Study strengths and limitations
In this study, a comprehensive assessment of Canadian Epilepsy Surgery centers and their practices concerning fMRI language lateralization were provided. By summarizing the cognitive design of fMRI language paradigms, protocol structure, image acquisition, data analysis, the use of software and/or programing tools, and the interpretation of the results across various national centers, we were able to identify components of fMRI language lateralization practices that demonstrated the most consistency and also the most variability (Table 1 and Table 2). Using this information in combination with a literature-based selection of language paradigms, we suggest a two-part series of paradigms, sentence completion and word generation tasks, that met the following criteria: (1) demonstrated widespread acceptance and employment by other centers, (2) showed consistent activations in well-established language areas targeting receptive and expressive aspects, and (3) designed for individuals with average or near-average IQ and normal literacy skills.
Future directions will assess the two-part series of language paradigms presented in this study in both healthy controls and individuals with epilepsy to determine their accuracy, reliability and success in lateralizing areas involved in receptive and expressive aspects of language functioning. By further evaluating LI values, a more thorough recommendation for an appropriate thresholding value and approach, software, or analysis method can be made. While a definitive standardized fMRI language lateralization approach for individuals with epilepsy cannot be made at this time, we hope these further investigations will yield strong conclusions that will reduce the current heterogeneity in practice across Canada.
Conclusions
The results of this study demonstrated extensive variation in fMRI language lateralization practices across many Canadian Epilepsy Centres. Using this information and supporting literature, we designed a two-part language paradigm series consisting of the SC and WG tasks aimed at lateralizing both receptive and expressive language abilities, respectively. Based on the findings from the Canadian Epilepsy Centres and support from literature, we suggest that these two paradigms be applied to healthy volunteers and patients with epilepsy to evaluate whether this approach of fMRI language lateralization demonstrates reliable clinical utility as a preoperative tool. Only then can we recommend the formal standardization of these paradigms into fMRI language lateralization practices in Canada to minimize the extent of clinical heterogeneity. Importantly, by laying the foundation of standardizing fMRI language lateralization practices across Canada, we hope to encourage the reproducibility, transparency and collective progression of using fMRI paradigms to assess language laterality and improve methodologies and patient outcomes in the surgical treatment of epilepsy.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/cjn.2024.56
Author contributions
G.P.W. and M.F. designed the study, and G.P.W. obtained funding. M.F. was involved in data collection, drafting the manuscript and producing the figures and tables. G.P.W. and D.B. developed the MRI protocol and acquisition settings. G.P.W., G.S. and L.B.L revised the manuscript.
Funding statement
This study was funded by the Queen’s University Faculty of Health Sciences.
Competing interests
M.F. and D.B. have no conflict of interest to disclose. L.B.L has received grants from CFI and accepts consulting fees from Eisai, UCB and Paladin. L.B.L. also received honorarium from Eisai, UCB, Sunovion and Paladin and support for attending meetings from Eisai and UCB. Finally, L.B.L. also has a role in the advisory boards of UCB and the Canadian League Against Epilepsy (CLAE). G.S. holds grants from the Canada Foundation of Innovation (CFI) at the Kingston General Hospital Research Institute and PSI Foundation and has received an honorarium from Paladin Pharmaceuticals for an invited lecture and expert panel discussion as well as an honorarium from Elsevier for editorship of Sleep Medicine. G.P.W. holds grants from the PSI Foundation and Canadian Institutes of Health Research, has received speaker honoraria from Eisai, UCB and Sunovion, travel support from Paladin Pharmaceuticals and has acted on the advisory board for Paladin Pharmaceuticals and Jazz Pharmaceutical.








 Open access
Open access