



Dear editor,
We read with interest the recently published article “An Anatomical Perspective to Botulinum Toxin Injection of Flexor Digitorum Profundus” by Campisi et al. Reference Campisi, Khan and Agur1 We would like to congratulate the authors for demonstrating how the anatomical findings are translated to a clinical setting to enhance injection protocols specifically of botulinum toxin A (BoNT-A) for the management of flexor digitorum profundus (FDP) muscle spasticity post-stroke. However, we propose an alternative technique, using ultrasound (US) guidance, to specifically target the innervation zones (IZ).
First and foremost, we second the aforementioned study in their belief that is well established that injections are performed with better precision under US imaging. Reference Campisi, Khan and Agur1 Next, we would like to highlight important anatomical locations in the skeletal muscle which are the IZ. These zones are defined as the three-dimensional band-like portion of the skeletal muscle in which neuromuscular junctions densely exist. Reference Rodríguez Cruz and Cossins2,Reference Kaymak, Kara and Yağiz On3 Their intramuscular nerve distribution in skeletal muscles has been heavily researched and determined using many techniques, including cadaver dissection, Sihler’s staining techniques and histochemistry. Reference Kaymak, Kara and Yağiz On3–Reference Won, Hur and Rha5
Since BoNT-A can only be taken into the nerve terminals at the neuromuscular junctions, IZ-targeted BoNT-A injections are highly recommended to achieve an optimal therapeutic goal with lower doses and fewer side effects. Thus, transport of the BoNT-A in the muscle tissue is ensured by restricting the intramuscular injection near the muscle portion in which the IZ reside. It has been reported that BoNT-A injection 1 cm away from the end plate zone (in biceps brachii muscle) yielded an almost 50% reduction in its effect. Reference Kaymak, Kara and Yağiz On3,Reference Kara, Kaymak and Ulaşli4 For that reason, injections should not only be performed under US guidance to target the correct muscle while protecting nearby neurovascular structures, but should also target the accurate location of IZ.
In this context, as proven by the Modified Sihler staining Reference Won, Hur and Rha5 , we recommend BoNT-A injection of the FDP differently. It has been found that the reference line is between the interepicondylar-interstyloid, with the IZ being at 13–75% and 35–91% with two injections being given at 40% medially and 60% laterally. Reference Kara, Kaymak and Ulaşli4 In this regard, the location of two BoNT-A injection sites were found to be 4.8 cm apart in a 24-cm forearm length (Fig. 1). This also allows adequate dissemination of the toxin along the width of the muscle, keeping in mind that in an animal study, distribution of the BoNT-A was detected up to 4.5 cm. Reference Kaymak, Kara and Yağiz On3,Reference Dodd, Rowell and Vrabas6
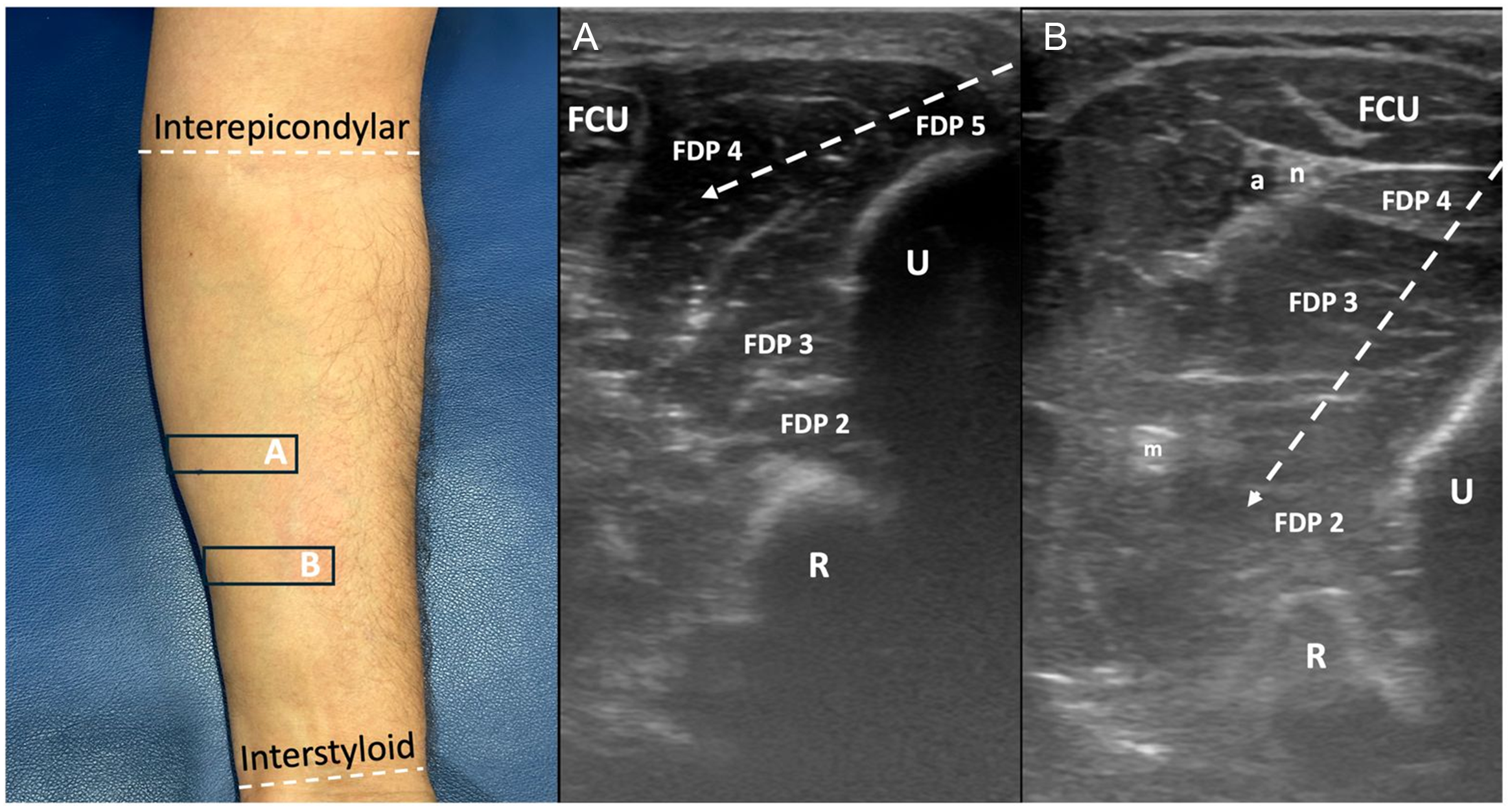
Figure 1. The appropriate probe positionings (rectangles) and the corresponding ultrasound images revealing the flexor digitorum profundus muscle (FDP) 4th and 5th (at the 40% level) (A) and 2nd and 3rd (at the 60% level) (B) of the reference line between the interepicondylar and interstyloid. At the proximal-medial level, the needle is directed more superficially to inject the 4th and 5th muscle bellies, and at the distal-lateral level, the needle is directed more superficially to inject the 2nd and 3rd muscle bellies. R = radius; U = ulna; n = ulnar nerve; a = ulnar artery; m = median nerve; FCU = Flexor carpi Ulnaris.
Acknowledgments
None.
Author contribution
All authors contributed equally to this manuscript.
Funding statement
None.
Competing interests
None.
Ethical approval
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.

