



INTRODUCTION
As of 2014, the e-cigarette industry in North America reported revenues of $1.5 billion, compared to just $20 million in 2008.Reference Campbell 1 In Canada, 9% of adults have smoked e-cigarettes at least once in the last 5 years, and use is expected to rise further.Reference Czoli, Reid and Rynard 2 Despite the marketing of electronic cigarettes as safer, smoke-free counterparts to regular cigarettes, new consumer risks are being recognized and reported. Explosions of lithium ion batteries have been well documented in relation to their use in laptop computers and cellular phones. 3 - Reference Mankowski, Kanevsky and Bakirtzian 5 The electrolyte liquid within the lithium ion battery cells is at risk for overheating, thus building pressure that may exceed the capacity of the battery casing. This “thermal runway” can ultimately result in cell rupture or combustion. 3 , Reference Ebbert, Agunwamba and Rutten 6
The purpose of this publication is to review e-cigarette battery explosions as an emerging aetiology of burn injury and to describe two cases requiring admission to an American Burn Association verified regional burn centre.
CASE REPORT I
A 31-year-old, previously healthy male was driving a motor vehicle when an e-cigarette battery ignited spontaneously in the pocket of his pants. The battery had been placed with several coins in the pocket. He was able to steer safely off of the road, remove his pants, and extinguish the flames with his hands. He was transported directly from the scene to the regional burn centre by Emergency Medical Services.
The patient sustained mixed partial thickness and full-thickness flame burns to his right anterolateral thigh, buttock and leg, as well as his left inner thigh (Figure 1, A and B). These findings were consistent on reassessment of possible progression after 24 hours. The total body surface area (TBSA) of the burn injury was calculated to be 10%, according to the Lund and Browder chart. The burn wounds were thoroughly irrigated with water on presentation to remove debris and to cool the burned surface area. The patient was sedated with ketamine, fentanyl, and midazolam during this procedure. The thigh wounds were dressed with silver sulfadiazine cream in sterile gauze and wrapped with cling. He received a tetanus vaccination. His burns were debrided and successfully covered with autologous split thickness skin grafts on Day 3 of a 7-day admission. The patient’s pain was adequately controlled with oral hydromorphone, ibuprofen, and acetaminophen, and supplemented by intravenous hydromorphone or fentanyl postoperatively and for dressing changes. Gabapentin was added as an analgesic adjunct postoperatively, to address neuropathic pain after skin grafts were harvested. His postoperative recovery was uneventful. He received outpatient physiotherapy and recovered full function within 2 months.

Figure 1 A) Right buttock and thigh burns of the patient in Case I. B) Bilateral anterior thigh burns in the patient in Case I, on the day of the burn injury.
CASE REPORT II
A 36-year-old previously healthy male had been storing an e-cigarette battery in the pocket of his pants along with several coins and keys. The patient was not aware that lithium ion batteries carried any risk of explosion. He recalls hearing a sound like a sparkler or firework when the battery spontaneously ignited and engulfed his pants in flame. He put the flames out with his hands and by dousing his pants with water. The patient was initially taken to a community hospital by Emergency Medical Services before a same day transfer to the regional burn centre for further management.
The patient sustained deep partial and full thickness burns to his right anteromedial thigh and superficial partial thickness burns to his right hand, cumulating in 3% TBSA (Figure 2, A). Part of the battery case was embedded in his thigh and was removed at the burn centre on arrival (Figure 2, B). The wounds were thoroughly irrigated with sterile water and dressed with silver sulfadiazine cream in sterile gauze. Two days following the injury, the patient was noted to have developed cellulitis of the burn wounds, manifesting as tachycardia and a low-grade fever. He was treated with a course of cefazolin. His wounds were debrided on the third day following the injury. The underlying deep tissue injury necessitated excision of deep fascia overlying part of the sartorius and rectus femoris muscles. Due to the extent of the injury and the presence of burn wound infection, the wound was closed in two stages. Meshed, deceased donor allograft skin and negative pressure wound therapy were used to cover the wound in the first surgery. At the second operation, the allograft was found to be adherent, and no further debridement was deemed necessary. Meshed autograft was used to definitively close the wound, again bolstered by negative pressure wound therapy to optimize graft take. The patient required a 12-day hospital stay and returned to full function within 2 months of his injuries. He continues to be followed in the outpatient setting for scar management and uses pressure garments.

Figure 2 A) Anterior right thigh burn of the patient in Case II on the day of the burn injury. B) E-cigarette battery device and fragment of the casing removed from the thigh of the patient.
REVIEW OF LITERATURE AND MEDIA REPORTS
An electronic search was conducted using the MEDLINE database in May 2016. Search terms included “e-cigarette” AND “injury” OR “burn” OR “explosion” OR “trauma,” “vaping and burn,” “vaping and injury,” and “cigarette and battery and burn.” Articles were excluded for lack of relevance or for descriptions of chronic health effects of e-cigarettes rather than burns or explosions. Sixteen cases of spontaneous e-cigarette or e-cigarette battery ignition were retrieved. The Google search engine was used to identify news media reports of accidental e-cigarette or e-cigarette battery ignitions from 2015 to 2016 using the same terms listed previously. The media search was initially conducted in May 2016 and updated in June 2016.
The academic literature review yielded four case reports, two case series, and one published abstract describing injuries sustained from overheating or explosion of an e-cigarette device (Table 1). Six incidents involved isolated explosions of a lithium ion battery, similar to the cases presented in this series. Three e-cigarette devices exploded while in use, and one device exploded while not in use.
Table 1 Academic reports e-cigarette explosions, 2015-2016
There has been a sharp increase in the number of e-cigarette-related reports in the literature (Figure 3). All reports involving explosion of e-cigarette batteries resulted in burn injuries, primarily to the lower extremities and hands. When reported, the extent of the burn injuries ranged from 1% to 8% TBSA and most commonly involved the lower extremity, hands, head and neck, and genitalia. Burn depth was predominantly deep partial and full thickness. In keeping with the depth of the injuries, at least 50% required surgical management of the burn wound. This report features a burn injury involving 10% TBSA, which at the time of writing is the most extensive burn resulting from an e-cigarette battery explosion published to date.
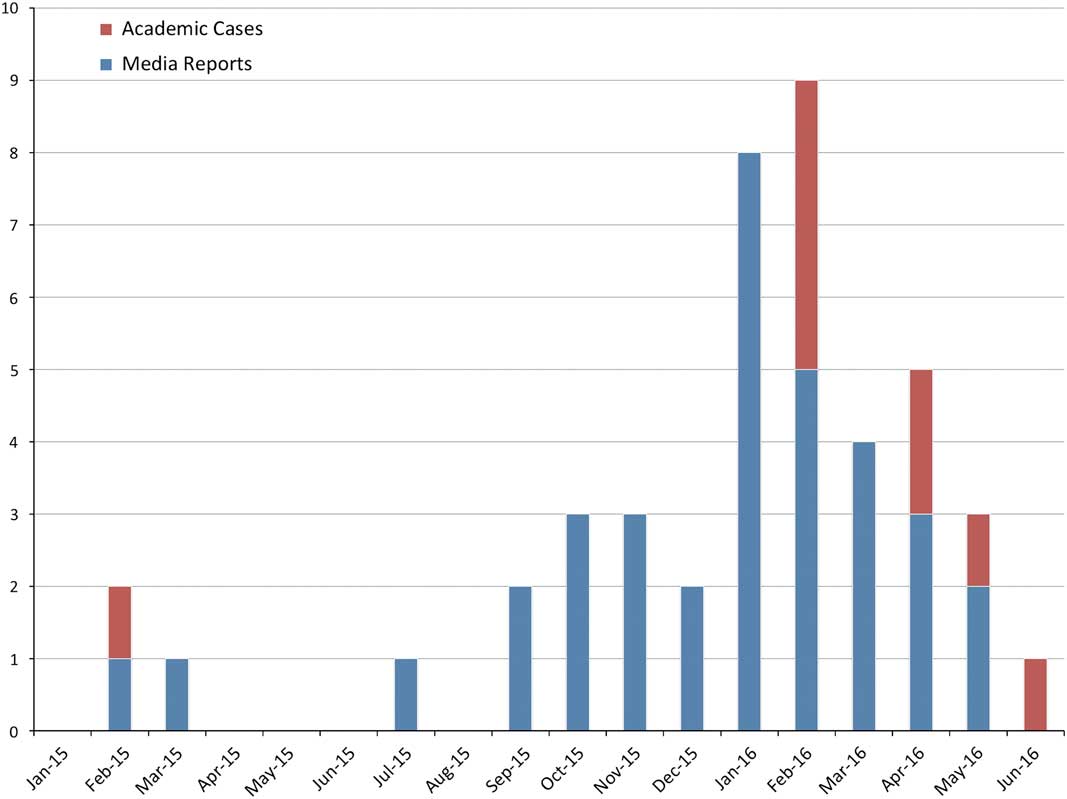
Figure 3 Incidence, by media and academic reports, of e-cigarette explosion-related injuries, 2015-2016 (as of June 26, 2016).
A search of general public media reports revealed 35 burns and associated injuries related to e-cigarette explosions between January 2015 and May 2016 (Table 2). Remarkably, over 60% of these incidents occurred in 2016 alone (see Figure 3).
Table 2 Media reports of e-cigarette explosions, 2015-2016
The U.S. Federal Emergency Management Agency (FEMA) published a report in October 2014 documenting all media reports of e-cigarette battery explosions from 2009 to 2014. The search revealed 25 cases, resulting in 9 injuries, including 2 serious burns. 3 The U.S. National Fire Protection Association (NFPA) published the only other review of incidents related to e-cigarette explosions in April 2016. From January to December 2015, a total of 15 cases of burns and/or explosions related to e-cigarettes were found, with 12 incidents involving injuries to a person.Reference Campbell 1 Our media search yielded 22 additional cases between January and June 2016. Although growing media attention may account for some of this upsurge in reports, the rising popularity of e-cigarettes is almost certainly contributory.
DISCUSSION
As more cases are reported, the spectrum of injury following e-cigarette battery explosions will be better delineated, thus allowing for targeted management approaches. The most frequent sites of injury observed with e-cigarette battery burns involve the lower extremities and hands. Nearly half of the reported incidences, including the two cases reported herein, required surgical management as a result of the depth of injury. Burns are typically less than 10% TBSA and therefore do not meet the threshold for formal fluid resuscitation. As with all burns, acute care physicians should follow the Advanced Trauma Life Support guidelines on patient arrival. Important adjunctive treatments include cleaning and cooling all burned areas with water prior to application of a non-adherent dressing. Importantly, burns to the hand, the genitalia, the face, chemical burns, and deep burns require a consultation with a burn surgeon, as per the referral guidelines of the American Burn Association.
First aid for exposure to the contents of lithium ion batteries includes a thorough irrigation of the affected site with water. 40 Rechargeable lithium ion batteries do not contain lithium metal and thus the use of water is safe and appropriate. 41 - 42 Nonetheless, medical staff should always don appropriate personal protective equipment because the other components of lithium ion batteries may cause skin or eye irritation. In addition to flame burns, a recent case report by Nicoll et al.Reference Mankowski, Kanevsky and Bakirtzian 5 discusses a patient who presented with features of both flame and alkali burns. The authors verified the alkali component of the burn through skin pH testing.Reference Nicoll, Rose and Khan 11 With suspicion of a chemical or mixed burn pattern, acute care physicians are urged to contact the regional burn centre for early, specialized management.
Metal objects, such as coins or keys, can create a short circuit when stored with batteries, which initiates battery overheating.Reference Khundkar, Malic and Estela 43 Khundkar et al.Reference Khundkar, Malic and Estela 43 presented a report where loose change in the pocket of their patient created a short circuit by connecting the positive and negative electrodes of a non-rechargeable battery. Walsh et al.Reference Walsh, Sheikh and Johal 9 also reported a case where an e-cigarette battery stored with keys ignited in a patient’s pocket, resulting in a mixed depth burn of the thigh.
The regulatory landscape for e-cigarette sales in Canada lags behind their rapid spread of use. At present, if an e-cigarette device or liquid contains nicotine or makes a health claim, they fall under the Food and Drugs Act. Because Health Canada has not yet approved e-cigarettes as delivery vehicles for nicotine, they are illegal to sell in Canada.Reference Czoli, Reid and Rynard 2 Regardless, both nicotine and non-nicotine containing e-cigarette products are widely available for purchase in Canada. Manufacturing guidelines established by the United Nations require lithium ion batteries and battery components to be tested to meet specific safety criteria, but batteries purchased through unreliable distributors or manufacturers of counterfeit products may not meet these guidelines and are thus at greater risk of igniting or exploding. 42 Without regulation or control of the sale of these products, consumers must rely on safety advice that they receive at the point of sale or on the Internet, which is inconsistent at best. Furthermore, given the lack of a user manual and product labeling regulations for e-cigarettes, consumers are often unaware of the risks of improper lithium ion battery storage or charging.
CONCLUSION
As e-cigarette use continues to rise in popularity, burns resulting from e-cigarette battery explosions will become a more prevalent presentation in the acute care setting. For acute care physicians, the recognition of these injuries is paramount in initiating an appropriate management algorithm, which often includes referral to a regional burn centre. This case series and literature review highlight the need for improved regulation of e-cigarette devices and advocate for clear warnings on product labels, to make e-cigarette users aware of the risks of battery explosion.
Competing interests: None declared.





