



Orientation
Abortion is one of the top healthcare procedures in the world, and it is performed globally at an annual rate of about 40 to 50 million per year.Footnote 1 Still, despite the desire for abortion healthcare services, provision to women-as-patients remains a contentious issue virtually everywhere.Footnote 2 The public policy debate often invokes the previous 1973 US Roe v. Wade liberalization of abortion provision in the United States (prochoice), juxtaposed against the 1975 West German Federal Constitutional Court decision to provide support for the fetus (prolife), with debates at the population level following similar prochoice versus prolife mantras. Over time, however, Roe has been used to bolster both sides of this debate as a balance of the reproductive rights of pregnant women and fetuses based on the gestational stage in question.Footnote 3 For example, early in her pregnancy a woman's needs relative to the fetus were more dominant, but the balance tilts toward the fetus as it moves closer to an estimated birth. A vacillation between these positions has led to an assortment of legislative mandates that restrict provision of abortion healthcare services, as the recent US Supreme Court decision reveals.
Such restrictions can have serious consequences for women that include greater financial costs for travel, lost wages, and potentially more expensive healthcare provision; as well as many negative emotional reactions like an increase in regret, guilt, or shame.Footnote 4 Of course, fostering these outcomes may be one underlying rationale of policy makers who seek to reduce usage of any legal right to this healthcare service. Unfortunately, restrictive abortion laws tend to increase the number of unsafe and illicit procedures, while dramatically escalating the maternal mortality rates by a factor of three to four. Johnson et al.Footnote 5 report that the restricted abortion law nations (both developing and developed) experienced 223 maternal deaths for every 100,000 live births, compared to 77 maternal deaths among 100,000 live births across countries with fewer restrictions. Thus, service legality is associated with all aspects of cost, safer alternatives, and lower maternal and infant mortality and morbidity.Footnote 6, Footnote 7, Footnote 8 Restrictive contexts not only reduce access generally, but they also expose differences within and between nation states for more affluent versus more impoverished women and deny reproductive justice to women facing intersectional and multiple oppressions.Footnote 9 In this sense, wealthy or more privileged women have flexibility and resources to overcome or circumvent legal dictates, but their more disadvantaged counterparts lack the requisite social and economic capital.Footnote 10 The latter, then, must endure substantial costs to themselves and their families, along with added burdens on healthcare systems that shoulder responsibility for negative mental and physical responses that require other remedial services.Footnote 11
With this backdrop in mind, our research purpose is to investigate the global abortion healthcare terrain to understand the variability in legislative mandates based on empirically validated factors that ultimately contribute to this diversity. The next section presents rationales behind different levels of service provision to capture legal manifestations of abortion service availability, and it yields a framework for further exploration of the underlying rationales and motivations for legislative decisions governing this critical service. This modeling reveals a connection between democratic versus authoritarian national leadership on abortion provision, and the capacity of citizens to express their moral viewpoints based on coercive governmental constraints versus ability to act according to their values. Together, these surrogates of societal freedom can influence gender equality within nation-states, and in turn determine where along this spectrum—from unavailable, to partially available, to available on demand—abortion services are provided to women in various countries. Our empirical findings present a novel perspective of how abortion provision exists and the explanatory variables for why it exists in the form that it does. Implications for policy makers and healthcare service providers are offered for this disputed domain.
Frame for abortion service provision
While researchers recognized the healthcare service implications of abortion provision;Footnote 12, Footnote 13 such work has not embraced the contextual nuances surrounding its availability by advocates and detractors on each polemic side of the debate.Footnote 14, Footnote 15 Interestingly, Patterson et al. (Reference Patterson, Hill and Maloy1995) found that abortion public policy did not reflect the considerations and concerns of women making these decisions, ignoring their lived experiences and potential trauma (see Janusz 2018 for one public policy to deal with this issue). Foundations for these diverse perspectives are articulated by Harris and Mills (Reference Harris and Mills1985). They are based on responsibility to others versus self-determination, and they concentrate attention on two competing sets of values. Consider that the former suggests loyalty and meeting one's commitments for the good of others, particularly those most vulnerable. The latter implies individual freedom to determine one's major life choices without interference from other parties, including government. These tenets have and continue to result in a jumble of public policy solutions that are reflective of these resulting tensions rather than citizens’ needs. Thus, service options vary along a spectrum based on this dichotomy that include the fact that there are no circumstances that justify abortion provision; extenuating circumstances like rape and incest or serious maternal health concerns that justify access to abortion; characteristics of the mother such as education, current number of children, financial status, and causes of pregnancy justify abortion services; health and well-being of the fetus and genetic abnormalities as justifications; and availability of abortion on demand without any rationale.Footnote 16
One way of understanding how this global variation in abortion policies manifests is to model underpinnings that lead to legislative mandates that govern provision of this healthcare service. Erdman (Reference Joanna N.2016, p. 40) recommends an “antipolitics” approach to policy solutions that calls for political decision makers to move away from their typical contextual basis and embrace “human rights [that] protect the individual against the indignity, suffering, and death inflicted by political power.” This approach is for an overarching global framework that is singularly appropriate for firms and governments as well as nongovernmental organizations like the United Nations and World Bank. As articulated, it recognizes international and intranational influences that come together as a cohesive whole to create an environment that results in abortion service levels previously outlined that either forbid, allow for under certain conditions, or make available abortion services.Footnote 17 To examine this issue, we posit that intranational influences include government forms that support various moral freedoms among their citizenry that can increase gender equality levels and women's development, which can then impact rights to abortion services (see Figure 1 for more details on the complete model and its embedded relationships).

Figure 1. Model of abortion public policies.
For our purposes, we use the government typology developed by The Economist (2020) and the report compiled by its Intelligence Unit. Their proffered Democracy Index positions governments using several descriptors of full democracies, flawed democracies, hybrid regimes, and authoritarian regimes. These monikers are based on the extent to which a country has free and fair elections, allows representative policy makers to legislate most decisions, and is devoid of foreign influence. According to their findings, only 22 countries are full democracies (e.g., Norway, Canada, Australia), 54 are flawed democracies (e.g., United States, Taiwan, India), 37 are hybrid regimes (e.g., Madagascar, Nepal, Pakistan), and 54 are authoritarian regimes (e.g., Iraq, Cameroon, China). This index's labels are determined by aggregating statistics across five variables that include the electoral process and pluralism, functioning of government, political participation, political culture, and civil liberties. The assumption is that national governments are increasingly available and dedicated to their citizenry and its needs as the scale moves from completely authoritarian to fully democratic. Further, political corruption decreases and economic growth increases as well.Footnote 18
Our frame suggests that variation from authoritarian to democratic governments has a significant impact on important individual freedoms.Footnote 19 These liberties come in many forms, but they are articulated here as the ability to express and act in a wide variety of ways in citizens’ personal and professional lives. Such opportunities support the heterogeneity of values and diversity of people that may exist within and across societies.Footnote 20 Accordingly, we have adopted the Moral Freedom Index as an outcome of governmental form. The composite statistic includes levels of individual freedoms in five areas— expressions of religion, bioethical decisions, drug usage, sexuality, and gender—that, pending the degree of state pluralism, are tolerated to a lesser or greater extent.Footnote 21 Taken together in equal parts, they give recognition to the heterogeneity of allowable moral frames. Functionally, we posit that more democratic governments lead to greater moral freedoms.
As the next step in our frame, we posit that nationwide gender equality is influenced by these moral freedoms since the latter impacts citizens and their general abilities to pursue self-determination and advance their quality of life (see Soukup Reference Soukup2019 for a prochoice perspective). The United Nations has now pioneered gender rights as human rights, encapsulating progress, or the lack thereof, in a variety of metrics that include the Gender Inequality Index .Footnote 22 The Gender Inequality Index is a composite of reproductive health as maternal mortality and adolescent birth rates, levels of empowerment as the share of governmental positions held by women and their share of the population with at least some high school education, and labor force participation by women relative to men. While written with a different purpose, Hill and Sharma (Reference Hill and Sharma2020) provides a framework for understanding moral freedom as the exercise of free will that is the proposed foundation on which issues such as gender equality are based, supporting our direction.
The fourth variable in our model is the legal status of abortion services as discussed previously. We use the Center for Reproductive Rights’ (2018) template for our purposes and as our guide for the provision of services. Additionally, we view the directionality of connections between Gender Inequality and service availability as the former to the latter (see Mucciaroni et al., Reference Mucciaroni, Ferraiolo and Rubado2019). Resulting policy options are organized into five categories that capture the spectrum of services from completely legally unavailable to available on demand. These include prohibited altogether—laws of countries in this category do not permit abortion under any circumstances; allowed to save the woman's life—national laws permit abortion when a woman's life is at risk; to preserve health—laws permit abortion based on general health and therapeutic grounds; broad social or economic bases—laws interpreted liberally and to permit abortion for a wide-ranging set of circumstances; and on request—with limits determined by a gestational timetable. Taken together, we posit the frame contained in Figure 1.
Nonetheless, while the logic of our model is clear and compelling, several caveats are worth noting. First, the measure selected to define every construct represents only one option among many. While we did not test these alternatives within our model or its parameters, our selections were far from arbitrary and are leading contenders in published research on women and human rights. Second, the direction of causality can be subject to scrutiny because measures coalign. Still, we have used every possible statistical method to ensure accuracy of our results and the logic of our theoretical arguments. Third, and finally, there are other possible indicators that are outside of the rubric presented that could prove important in the casual chain like cultural values and patriarchy. These options were not ignored, but the best path forward was eventually determined to be the one ultimately presented.
DataFootnote 23
Our intent was to examine the pathways of influence that exist between the practice of democracy and the legal status of abortion service provision. Hence, the dependent variable in our study is the Level of Abortion Service Provision. These data were obtained from the Center for Reproductive Rights (https://reproductiverights.org/worldabortionlaws). For our analysis, we operationalized Level of Abortion Service Provision as a five-level numeric variable where 1 represents the most restrictive and 5 represents the least restrictive national abortion laws. More specifically, the levels were 1 = Prohibited Altogether, 2 = Allowed to Save the Woman's Life, 3 = To Preserve Health, 4 = On Broad Social or Economic Grounds, and 5 = On Request, as presented in literature noted. There were 199 countries for which Level of Abortion Service Provision data were obtained. Table 1 provides the count of countries for each of the five levels.
Table 1. Country count of level of abortion service provision.

Consistent with our discussion of constructs, the antecedent variable in the study captures standing of countries in The Economist Intelligence Unit's Democracy Index 2019. Democracy Index is reported for 167 countries on a 0 to 10 scale. A country's Democracy Index is based on ratings for 60 indicators grouped into the five component categories previously detailed. Each category also has a rating on a 0 to 10 scale, and the Democracy Index is the simple average of the five category indices. Norway at 9.87 and North Korea at 1.08 have the highest and lowest Democracy Index scores, respectively.
The first of the two mediating variables in our study represents the extent of freedom available to the people of a country to make moral choices. Data for the Moral Freedom Index for 160 countries is obtained from the Foundation for the Advancement of Liberty World Index of Moral Freedom 2020 report by Álvarez, Kotera, and Pina (Reference Álvarez, Kotera and Pina2020). The index is reported on a 0 to100 scale. The Netherlands at 95.44 and Afghanistan at 9.59 have the highest and lowest Moral Freedom Index scores, respectively. The second mediating variable in our study measures extent of gender-based disadvantage along prior dimensions noted by the UNDP's Gender Inequality Index. The Gender Inequality Index is obtained from the Human Development Report 2020, downloaded from the weblink (http://www.hdr.undp.org/en/2020-report). The aggregated Gender Inequality Index scores for 162 countries are reported on a 0 to 1 scale. A low Gender Inequality Index value indicates low inequality between women and men, and vice versa. Switzerland with a Gender Inequality Index of 0.025 is ranked first and Yemen at 0.795 is last. The descriptive statistics for the four variables in the study are reported in Table 2.
Table 2. Descriptive statistics.

For our analysis, we merged the data from their four data sources mentioned in the preceding text. Care was taken to match data for countries that went by alternate names or spellings in the different data sources. Also, the sources in our study did not collect and/or report data for the same set of countries. Hence, observations across all four variables were not available for some countries. Our final analysis dataset thus consisted of 136 complete observations. We note that, while our analysis is not temporal in nature, our model specification is consistent with the time order in which the data for the four variables were published. To elaborate, the data for the antecedent variable Democracy Index comes from a 2019 study, the first mediating variable Moral Freedom Index values come from data released in early 2020, the second mediating variable Gender Inequality Index values come from data released in late 2020, and the consequent variable Level of Abortion Service Provision data is obtained from an interactive real-time data map and is therefore the most recent. The bivariate correlations for all four variables in the study are reported in Table 3.
Table 3. Correlation table.

The antecedent variable Democracy Index and the consequent variable Level of Abortion Service Provision are positively correlated (r = 0.337). The Democracy Index and Moral Freedom Index share the highest positive correlation at 0.789. The Gender Inequality Index and Level of Abortion Service Provision share the highest negative correlation at –0.645. The sizes and signs of the remaining correlations are also all consistent with our expectations.
Methodology and results
To test that the Moral Freedom Index and Gender Inequality Index are intervening variables that explain the mechanisms by which democracy exerts its effect on the Level of Abortion Service Provision, we ran a series of mediation models, each containing a different set of variables. This sequential approach helped us uncover the direct and indirect effects between variables in our study in a stepwise manner. We use the mediation and lavaan packages in R to estimate the possible mediation results.Footnote 24, Footnote 25 As described earlier, the three indices, Democracy Index, Moral Freedom Index, and Gender Inequality Index are reported on different scales. Therefore, we standardized data for these variables by mean centering and dividing by their standard deviations. We left the Level of Abortion Service Provision, the consequent variable, in its unstandardized form.
First, we examine the direct and indirect effects of the antecedent variable Democracy Index on the consequent variable Level of Abortion Service Provision, with the Moral Freedom Index as the sole mediating variable. The results of the Mediation Model 1 are reported in Table 4. A visual representation of the estimated indirect, direct, and total effects, and their confidence intervals are provided in Figure 2, Panel 1. The indirect effect of Democracy Index on Level of Abortion Service Provision is 0.790 and significant (p < 0.001). In other words, a one standard deviation increment in the Democracy Index increases the Level of Abortion Service Provision by 0.790 units using the mediating variable Moral Freedom Index. The remaining direct effect of the Democracy Index on the Level of Abortion Service Provision turns out to be not significant (–0.285, p = 0.10). Hence, the results from Model 1 suggest that there is a complete total mediation effect of the Moral Freedom Index on the influence of the Democracy Index as to the Level of Abortion Service Provision. In other words, as the Democracy Index scale moves from authoritarian to fully democratic, we expect to see an increase in levels of moral freedom that, in turn, is expected to result in increased levels of availability of abortion services.

Figure 2. Models of key variables.
Table 4. Mediation models of key variables.

Notes: Indirect or mediating effect is denoted by ACME and direct effect by ADE.
Sample Size Used =136, Simulations = 500.
Second, we examine the direct and indirect effects of Democracy as the antecedent variable on the consequent variable Level of Abortion Service Provision, with Gender Inequality as the sole mediating variable. In Mediation Model 2, we do not include Moral Freedom as an influencing variable. The indirect effect of the Democracy Index on the Level of Abortion Service Provision is 0.5402 and significant (p < 0.001), while the direct effect is not significant (–0.0424, p = 0.74). The results from our Mediation Model 2 support the inference that there is a total mediation effect of Gender Inequality on the influence of Democracy on the Level of Abortion Service Provision; we find that as the Democracy Index scale moves from authoritarian to fully democratic, there is a decrease in gender inequality, which in turn increases the availability of abortion services. The results from Mediation Models 1 and 2 independently suggest that Moral Freedom and Gender Inequality are both mediating variables between Democracy and the Level of Abortion Service Provision.
Third, we examine the direct and indirect effects of Democracy on the Gender Inequality Index, with the Moral Freedom Index as the mediating variable, to test whether the Democracy Index and/or Moral Freedom Index contribute to lower levels of Gender Inequality Index. Results of Mediation Model 3 indicate that the indirect effect of Democracy on Gender Inequality is –.343 and significant (p < 0.001), and the direct effect is –0.213 and is also significant (p < 0.05). The negative signs for the effects are consistent with the fact that the Gender Inequality Index represents gender inequality and is therefore expected to decrease with increased levels of democracy and moral freedom. In other words, Democracy influences Gender Inequality both directly and indirectly through Moral Freedom. The results from our Mediation Model 3 suggest that there is a partial mediation effect of Moral Freedom on the influence of Democracy on Gender Inequality.
Fourth, we examine the direct and indirect effects of Moral Freedom on the Level of Abortion Service Provision, with the Gender Inequality Index as a mediating variable. The results of Mediation Model 4 reveal that the indirect effect of Moral Freedom Index on Level of Abortion Service Provision is 0.467 and significant (p < 0.001), and the direct effect is 0.303 and significant (p < 0.001). The results from Model 4 suggest that Gender Inequality partially mediates the effect of Moral Freedom on the Level of Abortion Service Provision.
Last, we run a serial mediation model with the Moral Freedom Index and Gender Inequality Index as sequential mediators in the path between the Democracy Index and the Level of Abortion Service Provision. The statistical model for this analysis is depicted in Figure 3. This model is consistent with our conceptual model in Figure 1, but in addition depicts all the possible paths between the variables in our study. For this model, the effects were estimated using 5,000 bootstrap samples. The indirect effect of Democracy on the Level of Abortion Service Provision using Moral Freedom and Gender Inequality is 0.284 and significant (p < 0.01). The results from these analyses, therefore, indicate that both Moral Freedom and Gender Inequality significantly influence the pathway between Democracy and the Level of Abortion Service Provision. Higher levels of Democracy result in higher levels of Moral Freedom and lower levels of Gender Inequality. Higher and lower levels of Moral Freedom and Gender Inequality, respectively, lead to higher levels of Abortion Service Provision.

Figure 3. Serial mediation statistical model.
Alternative empirical models
We now report the findings from a comparison of our proposed model against other plausible empirical models that may support alternative explanations for the relationships between Democracy and the Level of Abortion Service Provision (see Appendix 1). First, we consider a parallel mediation model, wherein we assume that Moral Freedom and Gender Inequality independently, and not sequentially, mediate the relationship between Democracy and the Level of Abortion Service Provision. Because we assume the absence of a path between Moral Freedom and Gender Inequality, the parallel mediation is more restrictive than our proposed model (see Appendix 1, Alternative Model 1). While the indirect effect estimate from the parallel mediation model is significant and in the expected direction (0.969, p < 0.001), a Chi-Square Difference test (Chisq = 14.841, p < 0.001) indicates that the proposed serial mediation model is better and more complete at explaining the relationship between Democracy and the Level of Abortion Service Provision. Simultaneously, modification indices obtained from the parallel mediation model indicate a likely improvement in the model if we are to specify an additional path between Moral Freedom and Gender Inequality.
Second, we consider an alternative model wherein the path between Moral Freedom and Gender Inequality is reversed (see Appendix 1, Alternative Model 2). The number of variables and parameters estimated by this model is identical to the proposed serial mediation model. The indirect effect estimate from this reversed model is (0.085, p < 0.01). A direct comparison of the coefficients suggests the proposed serial mediation model has a stronger indirect effect and is therefore more supportive of the results recommended.
Last, we obtained bootstrap estimates for the model parameters for our proposed serial mediation model by respecifying the Level of Abortion Service Provision as a five-level ordinal variable, rather than a numeric variable. The model parameter estimates obtained (see Appendix 1, Alternative Model 3) were similar in sign and significance to the serial mediation model parameters originally obtained.
Considered jointly, the results from Models 1, 2, 3, 4, and 5 indicate that the Moral Freedom Index and Gender Inequality Index sequentially impact the relationship between the Democracy Index and the Level of Abortion Service Provision. The Alternative Models 2 and 3 provide a poorer explanation of the phenomenon being examined. The results from Alternative Model 3 are like the results from Model 5. Hence, results from Model 5 are consistent with the proposed conceptual model presented in Figure 1. In summary, our analyses indicate that increased democratization is not a guarantee of increased levels of abortion provision, unless accompanied by increased levels of moral freedom and decreased levels of gender inequality. We now proceed to discuss our findings and the policy implications of our study.
Discussion
The results support our posited relationships: More democratic societies where people can act on moral freedoms allow for higher levels of gender equity and create national contexts with more open-access policies permitting healthcare abortion services. These findings are consistent with prior literature, which has noted that the inherent quality of any democracy is based, in part, on gender representation in that democracy.Footnote 26 Further, the importance of having gender supportive freedoms likewise helps explain negative relationship between the Democracy Index and the Level of Abortion Service Provision. That is, the direct effect of Democracy on Level of Abortion Service is –.468 (p < 0.001). Effects of male-dominated institutions are one possible cause, especially without moderating impacts of moral freedom and gender (in)equality. Further, the ability of citizens to express the former ensures that democratic governments are willing to seek gender parity and support more gender-sensitive abortion laws.Footnote 27, Footnote 28 Representation of women in government similarly may not influence judicial realms in which some countries set their abortion standards.Footnote 29 Therefore, political and judicial systems need to be accompanied by an environment supportive of gendered moral freedoms.
It is also important to note that in many nations the ability to enact laws supportive of abortion service provision by healthcare providers may stem not from women but from men in positions of power who are held accountable to reflect moral resonance of a country. Thus, if a country's moral resonance is aligned with a drive for gender equality, and if those making laws can act on this moral resonance, abortion laws are more likely to be liberalized. For example, when the United States passed Roe vs. Wade and legalized abortion services across the country, this decision was made by male justices during an era in which women's rights were championed.Footnote 30 Likewise, in Ireland men and women were given the opportunity to decide abortion legislation through a democratically supported referendum in 2018. If an individual's ability to exercise moral freedom aligned with more gender-equality views of women, they were more likely to support a proabortion standard regardless of their gender.Footnote 31
Finally, our model underscores the importance of the democratic setup and separation of powers in influencing the ability of political and/or judicial realms of society to reflect the moral resonance of a country. If people hold moral views that support gender equality yet are based in less democratic societies where they are not allowed to exercise them the primacy of other moral views as determined by governments (e.g., based on religion or national cultural) result in more restrictive abortion-service policies.Footnote 32, Footnote 33 Some exceptions do exist, for example in countries where abortion is used to meet government goals such as in China with its one-child policy, although these nondemocratically enforced rulings are not inherently supportive of abortion rights. Given the nature of these political and judicial systems, the trend is opposite: Less gender-sensitive democratic systems or de-democratization processes often result in more restrictive abortion policies.Footnote 34 What is required is for the democratic processes of a country to uphold moral freedoms in support of gender equality.
Implications for public policy governing abortion services
Our findings reframe public policies governing abortion healthcare services away from perspectives that invoke prochoice versus prolife, to those that are about the type of society policy makers desire to create. Recent threats of backsliding from gender-equality progress in democracies should be of concern to women, service providers, and policy makers globally. Such societies may have regressed based on patriarchal assumptions that include desires to control families, reproduction, women's sexuality, and hierarchies of genders that are reinforced and institutionalized.Footnote 35, Footnote 36 Framing arguments as we outlined previously for or against abortion as a responsibility to othersFootnote 37 seem more indicative of several patriarchal assumptions prevailing in historic reproductive discussions. This is evident if one compares how expectations are not extended to other areas. For example, one can contrast if responsibility to others versus self-determination governs the productive sphere of capitalist systems to the same extend it is being wielded in arguments in the reproductive sphere. In this light, countries that restrict their abortion services may be open to criticisms that they are permitting a gender-biased frame to govern societies instead of striving for more inclusive and just practices that uphold human rights.
Preventing such backsliding and achieving gender equality requires policy makers to adopt gender-sensitive approaches to legislative decisions, and for these approaches to advance gender diversity. The former is bolstered by approaches like Inter-Parlimentary Union's (2020) gender equality efforts, which describes gender-sensitive institutions thusly:
[we a]re founded on gender equality, where women and men have an equal right to participate without discrimination or recrimination…by being sensitive to gender issues and favoring equal participation of women and men, parliaments are also more likely to achieve gender equality in society and to fulfil their democratic mandate. (n.p.)
Gender-sensitive institutions not only seek to increase representation of women in government and create conducive work environments for men and women but also to strengthen legislation and policies that promote gender equality. They adopt a gender mainstreaming lens, identifying groups that will most likely be affected by proposed policies or legislation. They work to ensure that discriminatory or unjust outcomes do not manifest.Footnote 38
Further, given that laws, policies, and enforcement are contributing factors to countries supporting or restricting abortion healthcare services, a society seeking to move toward more inclusivity demands gender-sensitive approaches that are adopted across levels. On the policy front, this includes international and national institutions, political and judicial systems, and mechanisms such as social media that they use to convey their viewpoints to women as well as providers and civil society influencing this service landscape. Such a perspective recognizes that the antipolitics approach can be used to justify the state remaining outside of the reproductive, human-rights debate (i.e., human rights are a matter of private vs. public life)Footnote 39 is not the solution. As Erdman (Reference Joanna N.2016, 40) aptly notes, “abortion rights do not escape politics, but rather become embedded in national democratic struggles.” To ignore this reality is not conducive to achieving more gender-equitable solutions in this service domain. Rather, we urge policy makers to recognize their powerful positions and the interplay of their influence. We see the power of this approach in how functioning governments, or their judicial systems, leverage international human rights laws or directives. For example, the United Nations and its monitoring bodies for these human rights support reform of abortion legislation to become less restrictive.Footnote 40
In contrast, cases of the Global Gag Rule imposed by the United States on organizations within and outside its national borders, and the experiences of citizens in countries backsliding from democracy, demonstrate how nationally mandated laws can be globally disruptive to abortion healthcare services. When a gender-sensitive approach is denied, governments and institutions with far-reaching powers over the localized service landscape can enact gender-blind decisions, which can undermine reproductive justice. The US government's power over international funding has left a chasm that has significantly restricted the infrastructure required to increase awareness of abortion services, assist women in accessing such services, and support healthcare providers of abortions, even in countries where abortions are legal .Footnote 41, Footnote 42 Likewise, although abortion was allowed in the United States, various states enacted policies that restrict access to abortion services, such as requiring parental approval for minors, mandating waiting periods, restricting public funds and Medicaid coverage, and obstructing access through requirements placed on abortion providers.Footnote 43, Footnote 44
Similar incidences occurred across the globe as governments lacking gender-sensitive approaches are prone to adopt requirements and conditions that can restrict provision and/or knowledge of safe abortion options.Footnote 45, Footnote 46, Footnote 47 These decisions not only reduce women's reproductive rights and cost many their lives, but they also disrupt ability of civil society to express moral freedoms as described herein. Studies find that the United States’ gag rule and governments that hold antiabortion stances can create an imbalance in information: proabortion organizations are silenced while antiabortion stances are encouraged through funding and politicized platforms.Footnote 48, Footnote 49 Gender-sensitive approaches can thus fall short if they lack acceptance and adoption, enabling a return to gender inequities, a lack of translation of law to fair provision of healthcare services, and a dampening of gendered moral freedoms.
Additionally, when assessing human rights, the need for an integrative gender-sensitive approach across issues, policies, and actors becomes apparent. The ability of various movements to position or frame their arguments and to channel monetary, political, and social resources into effective social campaigns can significantly influence societal beliefs and moral standings on gender equity and abortion rights.Footnote 50, Footnote 51, Footnote 52 In turn, they have implications for legal reforms, and the provision of services and knowledge related to the enactment of abortion rights. For example, antiabortion campaigns are often conditioned by a gender-stigmatizing versus gender-sensitive approach, framing women who seek abortions as deviant. They present arguments in a way that obfuscates consequences of abortion restrictions and incites what Herdt (Reference Herdt2009) calls “moral panic,” promoting regression to preferences of controls to enforce “tradition.”Footnote 53 Pushing against these conditions are campaigns by civil society groups that effectively harnessed gender and social justice appeals to promote abortion availability legislation or reforms.Footnote 54, Footnote 55, Footnote 56 However, given the historical legacy and conflicting social environment in the wake of political battles, if changes in legal reforms are to be effective, they need to include expansion of resources that build out this service landscape (e.g., abortion clinics, services, providers).
Finally, if supportive abortion legislation is to be effective in addressing the dark side of service provision, that is, in reducing unsafe procedures and maternal deaths and morbidity, an integrative gender-sensitive approach must be conditioned on an intersectionality lens that demands policy makers and service providers assess their actions from the perspective of those persons who may be most disadvantaged. As countries increase their restrictions on abortions (either through legislation, policies, or implementation), disparities in human rights and levels of gender inequality result. As presented, such conditions are linked to higher rates of maternal mortalityFootnote 57 and maternal morbidity (physical or mental illnesses or disabilities associated with pregnancy that can have significant consequences on quality of life)Footnote 58 and infant mortality and morbidity (effects of preterm birth and low birth weight).Footnote 59 As advocates for reproductive justice attest, these effects disproportionately affect those most marginalized in societies.Footnote 60 For example, in the United States, scholars found that restrictive state policies on abortion cross over with structural racism (e.g., discrimination in healthcare, jobs, education, housing), with Black women incurring more negative maternal and infant health outcomes relative to other women.Footnote 61
Global studies also point to women who are young, single, rural, and/or from lower socioeconomic households as those patients who struggle to gain access to or pay for services, and who thus are more likely to resort to unsafe abortion practices or who bear the consequences of negative health outcomes.Footnote 62, Footnote 63 Young women are disadvantaged by laws that mandate strict time limitations; their signs of pregnancy are often recognized too late,Footnote 64 and they face higher maternal and child health risks if forced to carry the pregnancy to term.Footnote 65 An intersectionality perspective thus reveals the true consequences of seemingly balanced abortion service policies that attempt to straddle the mother-fetus rights continuum: They may result in compromising the lives of both the woman and fetus. In sum, if countries want to achieve a more socially just and inclusive society that upholds human rights for all, abortion mandates and access need to be assessed from a gender-perspective that includes consideration of women who struggle the most in accessing this service landscape.
Future research and closing remarks
Our model has revealed key causal factors related to legislation governing abortion healthcare services. While we highlighted consequences of undemocratic, morally restrictive, and gender-inequitable societies on abortion laws and outcomes, we encourage future researchers to delve more into how these factors, at times, can be misaligned and affect abortion services’ legal status and women's reproductive rights. Importantly, our data focused on the relation of these variables to abortion legislation. As our article makes clear, however, legislation does not necessarily translate into securing desired accessibility of this service. Future research delving specifically into variances in abortion services between what is written versus what is enacted could shed further light on conditions that erode access. Likewise, looking at structural trends allows researchers to assess impacts of legal systems on new market formations of care, such as online telemedicine service provision by groups such as Women on Web (WoW) that have helped to bridge the gap in access to medicated abortion options (i.e., the pill) in a variety of countries around the globe.Footnote 66, Footnote 67 (Also consider Abortion | Guttmacher Institute as a potential resource.) Under what conditions do these service processes that circumvent restrictive laws and policies work, encounter resistance, or result in support for change?
Lastly, while we urge policy makers and healthcare providers to adopt integrated and gender-sensitive approaches, we recognize that cases in which this has been enacted are rare. The situation in Nepal prior to the US gag rule is the closest case we found.Footnote 68 Thus, understanding debilitating factors to achieving full human and gender rights is a key area of research that would help support countries’ policy makers, service providers, and civil society actors interested in more inclusive and informative legislative solutions and implementation. We firmly believe that abortion, healthcare access, and gender equality are important topics for policy makers governing gendered-service landscapes to study and recommend actions. Scholars have filled the pages of relevant journals with ideas and guidance that place the person/women at the center of the discussion. This interdisciplinary field of study recognizes that vulnerability is widespread and heterogeneous,Footnote 69 and entire categories of people demarcated by race, gender, ethnicity, and class suffer.Footnote 70 Democracy with a moral framework that is consistent with its historical roots should consider the method and findings herein to look at the underlying premises of legislation and who is advantaged and who is disadvantaged. We hope that this investigation motivates the continuation of similar assessments in other service-delivery landscapes.
Table 5. Serial Mediation Model (Model 5) (Democracy Index->Moral Freedom Index->Gender Inequality->Level of Abortion Service Provision).

Conflicts of interest
None.
Appendix 1
Alternative Model 1: Parallel Mediation Model 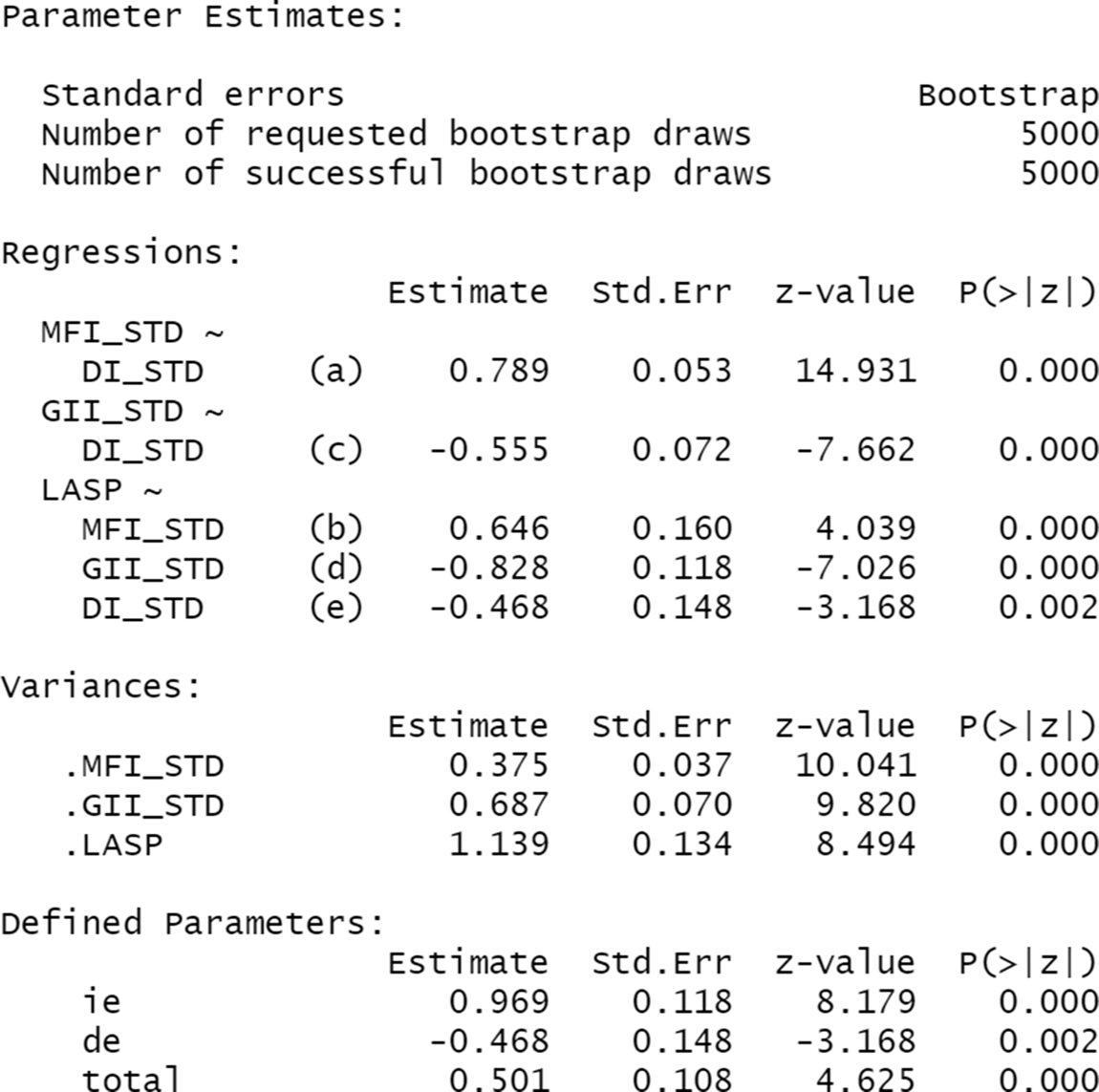
Alternative Model 2: Reversed Mediation Model 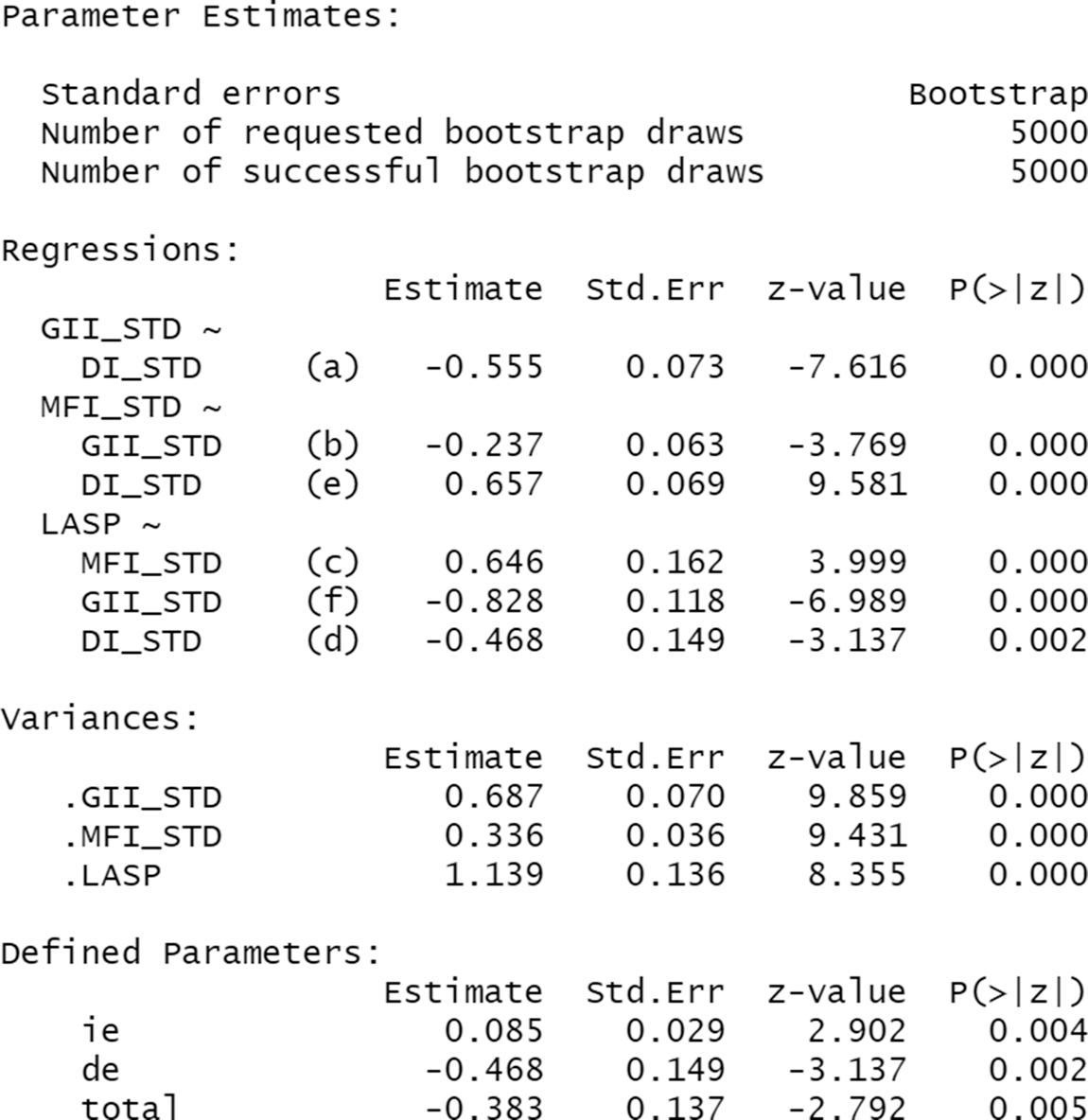
Alternative Model 3: Level of Abortion Services Provision as an Ordinal Variable 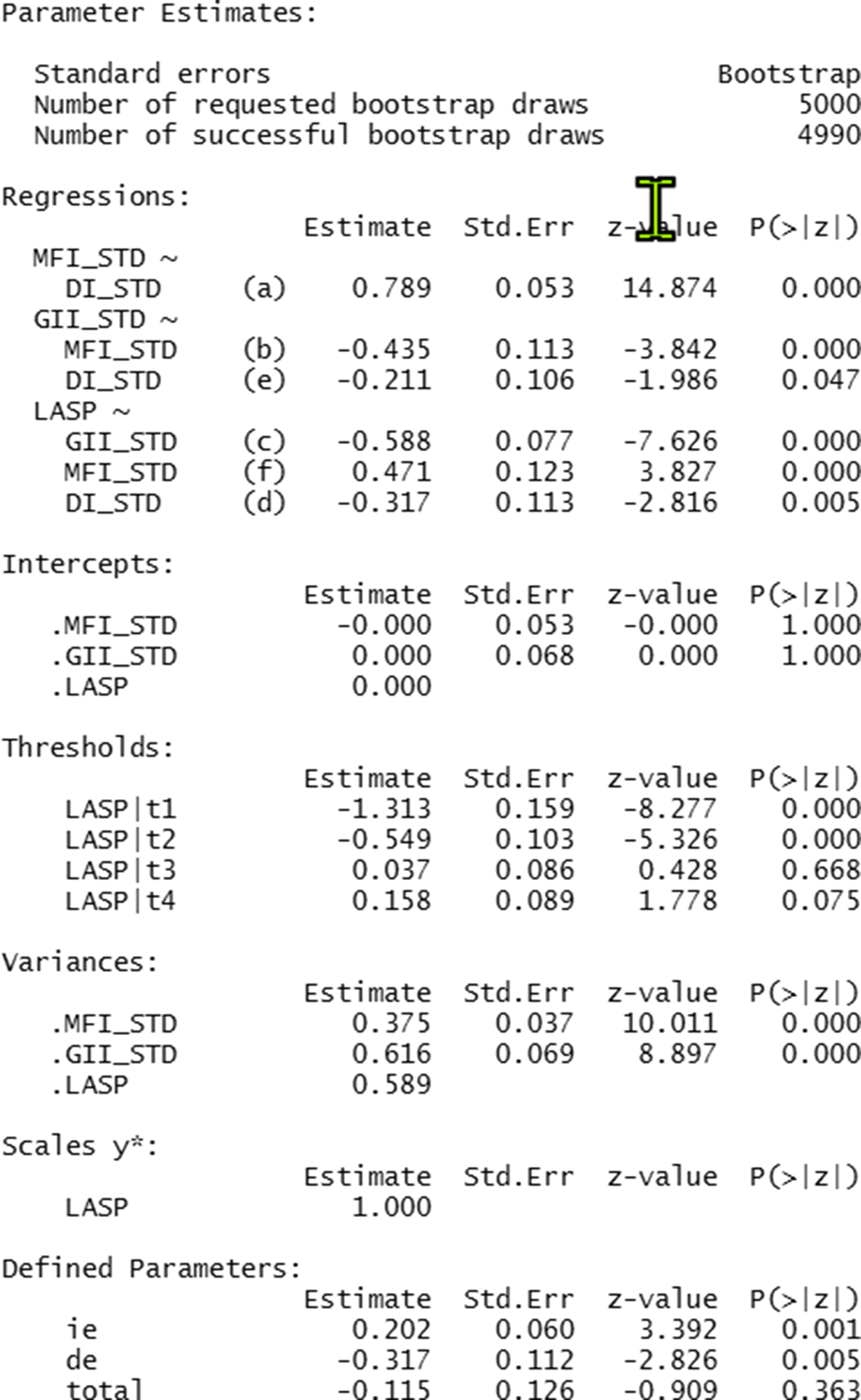









 Open access
Open access