


Stroke is a main cause of death globally and the most common cause of permanent disability in adults in most regions( Reference Go, Mozaffarian and Roger 1 ). Primary prevention strategies are required to limit the growing burden of stroke. A recent meta-analysis study( Reference Myung, Ju and Cho 2 ) of randomised controlled trials (RCT) suggested that vitamin E supplementation demonstrated no beneficial effects in prevention of stroke or its subtypes. However, RCT have tended to have short duration, and to use high doses. Thus, the effect of long-term moderate dietary vitamin E intake on the incidence of stroke needs to be clarified.
Many observational epidemiological studies( Reference Del Rio, Agnoli and Pellegrini 3 – Reference Yochum, Folsom and Kushi 10 ) have examined stroke risk related to dietary vitamin E intake with a few studies( Reference Del Rio, Agnoli and Pellegrini 3 , Reference Voko, Hollander and Hofman 9 , Reference Yochum, Folsom and Kushi 10 ) suggesting a protective effect, but others studies( Reference Hirvonen, Virtamo and Korhonen 4 – Reference Ross, Yuan and Henderson 8 ) suggest that there is no effect. However, the results comparing vitamin E with stroke risk have, thus far, been inconsistent( Reference Marniemi, Alanen and Impivaara 7 , Reference Hak, Ma and Powell 11 – Reference Wright, Lawson and Weinstein 14 ). Given these conflicting results, we conducted this meta-analysis of prospective studies to clarify the associations between vitamin E intake and risk of stroke.
Methods
Literature search and inclusion criteria
We performed a literature search using PubMed (Medline), Embase, Scopus, the Cochrane library, Web of Knowledge and Google Scholar through to June 2018 using keywords related to vitamin E intake and cerebrovascular diseases. The keywords were as follows: ‘vitamin E’ or ‘tocopherol’; and ‘stroke’ or ‘cerebrovascular disorders’ or ‘cerebrovascular disease’ or ‘cerebrovascular event’ or ‘cerebrovascular accident’ or ‘intracranial haemorrhage’ or ‘brain haemorrhage’ or ‘transient ischemic attack’; and ‘diet’ or ‘dietary’ or ‘intake’ or ‘consumption’. Then, we reviewed the references from the retrieved articles to identify any additional relevant publications. No language restrictions were imposed.
Study selection
For inclusion, studies had to meet the following criteria: (1) a prospective cohort study or a nested case–control study; (2) evaluated the association between dietary vitamin E intake and stroke risk; (3) the outcome of interest was stroke and (4) the relative risk (RR) estimates or OR in nested case–control studies with 95 % CI were provided. We excluded RCT, non-human experimental studies and non-original research (editorials, reviews or commentaries).
Data extraction
The following data were extracted: the first author’s last name, publication year, study quality, study location, age of participants, stroke events and outcomes (fatal or non-fatal), number of participants, assessment of vitamin E intake, length of follow up duration, sources of vitamin E, RR and the corresponding CI of stroke for the maximum v. the minimum level, and variables that were controlled for in the analysis. The literature search and data extraction were conducted independently by two authors. Disagreements were resolved by discussion or consultation with a third author.
Assessment of methodological quality
We used the nine-star Newcastle–Ottawa Scale( Reference Stang 15 ) to evaluate the quality of the included studies. Studies were graded as high quality if they achieved a rating of >7 stars.
Main and subgroup analyses
We investigated the association between dietary vitamin E and cerebrovascular events. We also performed subgroup meta-analyses for vitamin E intake and stroke risk by type of stroke (ischaemic v. haemorrhagic), race (Non-East Asians v. East Asians), sex (female v. male), sources of vitamin E intake (foods or supplements), number of participants (≥20 000 v. <20 000), BMI adjusted (yes v. no).
Statistical analysis
Log RR of the highest compared with the lowest for cohort studies were weighed by the inverse variance method to obtain pooled RR, and the OR were deemed equivalent to RR. Although three studies( Reference Voko, Hollander and Hofman 9 , Reference Yochum, Folsom and Kushi 10 , Reference Ascherio, Rimm and Hernán 16 ) provided the RR of stroke from supplemental vitamin E intake, one of these studies( Reference Yochum, Folsom and Kushi 10 ) did not provide the available RR and its CI for stroke on the highest supplemental vitamin E intake. We contacted the authors to request data, but were unsuccessful in making contact with them. Thus, we did not include this study( Reference Yochum, Folsom and Kushi 10 ) in the meta-analysis of supplemental vitamin E intake and stroke risk.
Between-study heterogeneity was evaluated via the Cochran Q test and I 2 statistic. Heterogeneity was determined with a significance level of P<0·10 or an I 2 statistic >50 %, and we observed the presence of significant heterogeneity. A random effects model was applied when significant heterogeneity was observed; otherwise, a fixed-effect model was used( Reference Higgins and Thompson 17 , Reference Lau, Ioannidis and Schmid 18 ). We also pooled RR if the individual study reported risk estimates based on stroke subtypes.
We performed a dose–response meta-analysis using the method developed by Greenland & Longnecker( Reference Greenland and Longnecker 19 ) and Orsini et al.( Reference Orsini, Bellocco and Greenland 20 ) to estimate the trend from the correlated log RR across categories of dietary vitamin E intake. The amount of dietary vitamin E intake, distributions of cases and person years, and RR and 95 % CI were extracted using this method. The median or mean dietary vitamin E consumption in each intake category was used as the corresponding consumption dose. For studies that provided dietary vitamin intake using intake ranges, we estimated the midpoint for each category by using the average of the lower and upper bound. When the highest or lowest category was open-ended, we considered the bound to be the same as the closest adjacent category. We estimated a potential non-linear relationship between dietary vitamin E and stroke risk, using restricted cubic splines with three knots at percentiles 10, 50 and 90 % of the distribution( Reference Orsini, Li and Wolk 21 ). A P value for nonlinearity was calculated by making the coefficient of the second spline equal to zero.
We assessed publication bias was assessed using Begg’s funnel plot and Egger’s test. If publication bias exists, the Begg’s funnel plot is asymmetric or the Egger’s test P value is <0·05. Data analysis was performed using Review Manager 5.3 Software (version 5.3.5; The Nordic Cochrane Centre, The Cochrane Collaboration) and the R 3.2.2 software packages.
Results
Literature search
The initial search identified 3165 potential articles. A flow chart showing the details of study selection is shown in Fig. 1. Briefly, nine studies were identified and included in the analysis of the highest compared with the lowest dietary vitamin E intake and stroke risk. In all, eight studies( Reference Del Rio, Agnoli and Pellegrini 3 – Reference Yochum, Folsom and Kushi 10 ) on dietary vitamin E intake, three studies( Reference Voko, Hollander and Hofman 9 , Reference Yochum, Folsom and Kushi 10 , Reference Ascherio, Rimm and Hernán 16 ) on supplemental vitamin E intake, and two studies( Reference Yochum, Folsom and Kushi 10 , Reference Ascherio, Rimm and Hernán 16 ) on total vitamin E intake were included in the meta-analysis. In all, five studies were awarded seven stars, three studies were awarded eight stars, and studies with seven awarded stars were considered as high quality (online Supplementary Table S1).
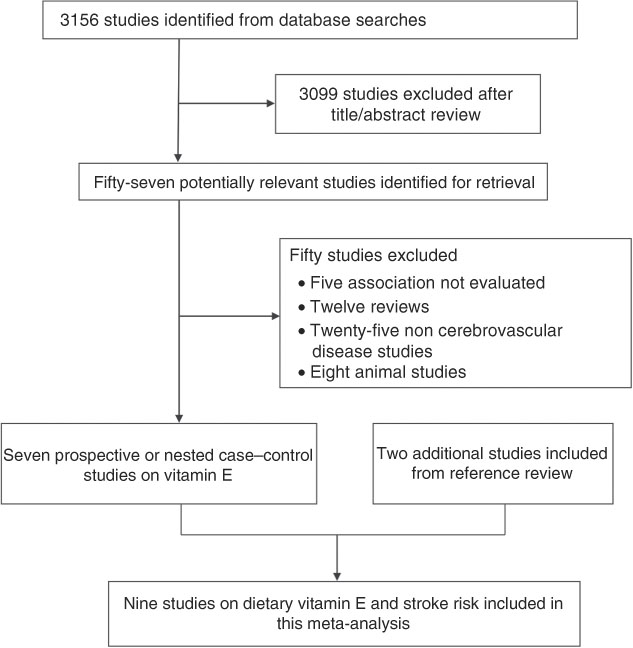
Fig. 1 Flow chart of articles included in this meta-analysis.
Study characteristics
Table 1 shows the characteristics of the nine studies on vitamin E intake. These studies had a total of 220 371 non-overlapping participants and 3284 stroke events. In the studies that reported age, the mean age of the participants ranged from 40 to 99 years. The year of publication of the included studies ranged between 1996 and 2012, spanning 16 years. In all, two studies( Reference Yochum, Folsom and Kushi 10 , Reference Ascherio, Rimm and Hernán 16 ) were conducted in the USA, two( Reference Keli, Hertog and Feskens 5 , Reference Voko, Hollander and Hofman 9 ) in Netherlands, two( Reference Hirvonen, Virtamo and Korhonen 4 , Reference Marniemi, Alanen and Impivaara 7 ) in Finland, one( Reference Del Rio, Agnoli and Pellegrini 3 ) in Italy, one( Reference Ross, Yuan and Henderson 8 ) in China and one( Reference Kubota, Iso and Date 6 ) in Japan. A total of four studies included males only, four studies included both males and females, one study included females only and the remaining one included a separate result for males or females. The follow-up duration ranged between 6·1 and 16·5 years.
Table 1 Characteristics of the included prospective studies on vitamin E intake and stroke risk (Relative risks (RR) and 95 % confidence intervals)

TS, total stroke; M, males; SBP, systolic blood pressure; IS, ischaemic stroke; HS, haemorrhagic stroke; MI, myocardial infarction; ICH, intracerebral haemorrhagic; SAH, subarachnoid haemorrhagic; DBP, diastolic blood pressure; F, females.
Vitamin E intake and stroke risk
A total of eight studies( Reference Del Rio, Agnoli and Pellegrini 3 – Reference Yochum, Folsom and Kushi 10 ) examined the association of dietary vitamin E intake with the risk of overall stroke. The summary RR for the high compared with low dietary vitamin E intake was 0·83 (95 % CI 0·73, 0·94) (Fig. 2). The effect of total vitamin E intake on stroke risk was reported in two studies( Reference Yochum, Folsom and Kushi 10 , Reference Ascherio, Rimm and Hernán 16 ), and the summary RR for the high-v.-low vitamin E intake was 1·13 (95 % CI 0·84, 1·51), with low heterogeneity (P heterogeneity=0·314, I 2=1·2 %). In all, three studies( Reference Voko, Hollander and Hofman 9 , Reference Yochum, Folsom and Kushi 10 , Reference Ascherio, Rimm and Hernán 16 ) including 770 stroke patients reported results for supplemental vitamin E intake. However, only two studies( Reference Voko, Hollander and Hofman 9 , Reference Ascherio, Rimm and Hernán 16 ) provided the available RR for supplemental vitamin E intake and stroke risk. The summary RR for the high-v.-low intake was 1·10 (95 % CI 0·85, 1·44), with no heterogeneity (P heterogeneity=0·74, I 2=0·0 %).
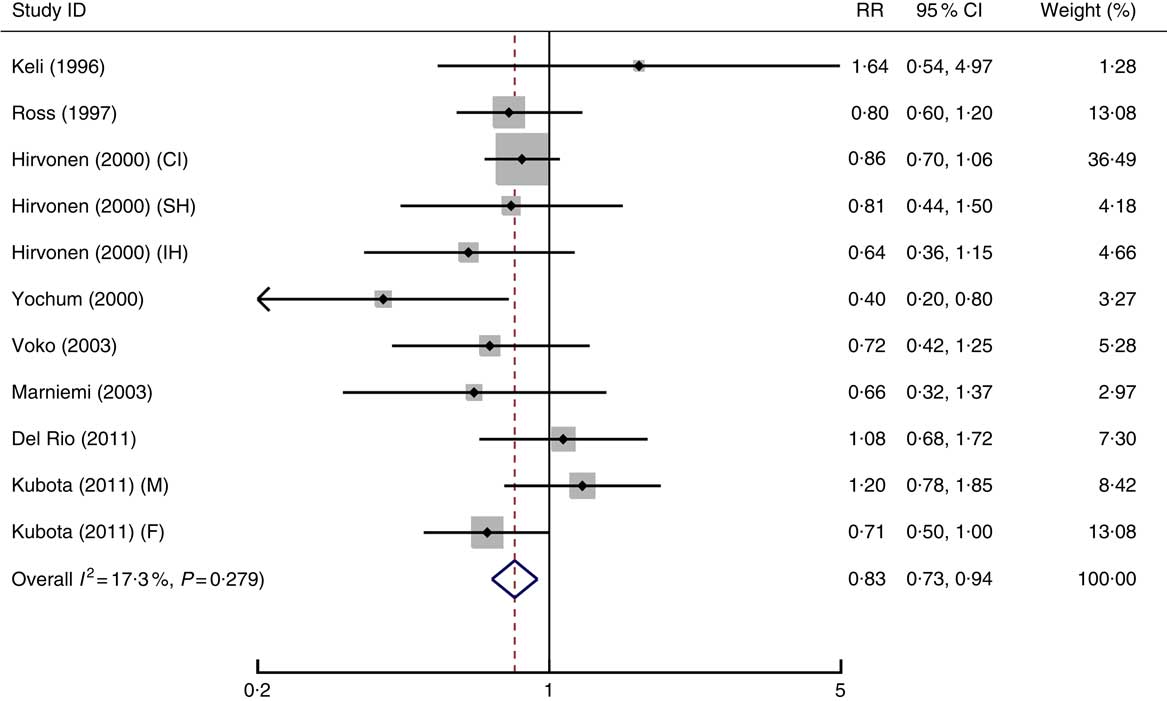
Fig. 2 Meta-analysis of dietary vitamin E intake and risk of stroke. CI, cerebral infarction; SH, subarachnoid haemorrhage; IH, intracerebral haemorrhage; M, males; F, females.
Dose–response meta-analysis
In all, six studies( Reference Del Rio, Agnoli and Pellegrini 3 – Reference Kubota, Iso and Date 6 , Reference Ross, Yuan and Henderson 8 , Reference Yochum, Folsom and Kushi 10 ) were included in the dose–response analysis, with a total of 2837 events among 180 231 participants. We found evidence of a non-linear association for dietary vitamin E intake (P=0·0249 for non-linearity) with risk of stroke (online Supplementary Fig. S1).
Subgroup and sensitivity analyses for vitamin E intake
The subgroup analysis showed that dietary vitamin E intake was associated with reduced risk of stroke for mixed stroke types (RR=0·80; 95 % CI 0·66, 0·97), for Non-East Asians (RR=0·82; 95 % CI 0·70, 0·95), females (RR=0·58; 95 % CI 0·34, 0·99), ≥20 000 participants in the cohort (RR=0·84; 95 % CI 0·73, 0·96), BMI adjusted (RR=0·83; 95 % CI 0·73, 0·95), and <10 follow-up years (RR=0·84; 95 % CI 0·72, 0·91) (Fig. 3). However, dietary vitamin E intake was not significantly associated with the risk of haemorrhagic stroke (RR=1·05; 95 % CI 0·49, 2·28). In addition, dietary vitamin E intake was not associated with stroke risk for East Asians (RR=0·84; 95 % CI 0·68, 1·04), males (RR=0·87; 95 % CI 0·75, 1·02), <20 000 participants in the cohort (RR=0·79; 95 % CI 0·61, 1·03), BMI non-adjusted (RR=0·78; 95 % CI 0·52, 1·17), and ≥10 years follow-up (RR=0·79; 95 % CI 0·53, 1·18; Fig. 2). In addition, omitting any single study did not remarkably alter the summary risk estimates (RR ranged between 0·80 and 0·84; Table 2).
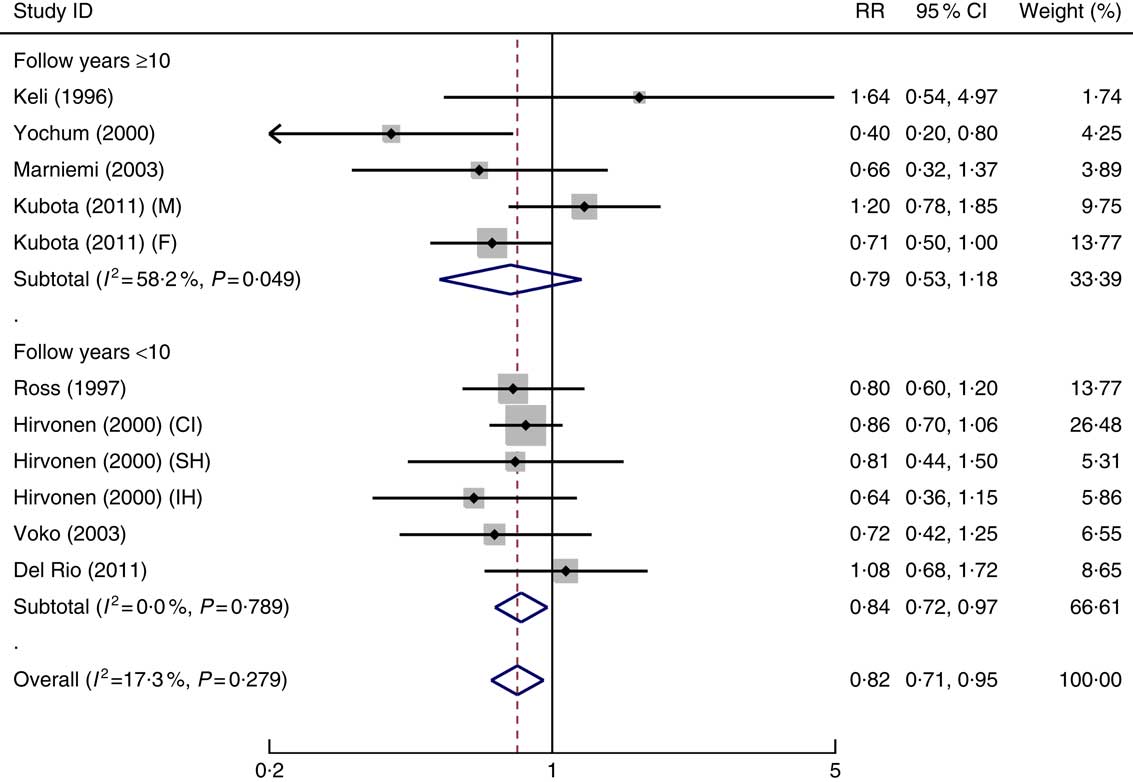
Fig. 3 Meta-analysis of vitamin E intake and stroke risk for follow-up years subgroups. M, males; F, females; CI, cerebral infarction; SH, subarachnoid haemorrhage; IH, intracerebral haemorrhage.
Table 2 Subgroup analyses of dietary vitamin E intake and stroke, high v. low intake (Relative risks (RR) and 95 % confidence intervals)

* P<0·05, statistical difference.
Meta-regression
We used meta-regression analysis to explore the potential sources of heterogeneity. However, stroke type, race, sex, participants, stroke events, BMI, publication year, or years of follow-up was not determined to be the source of heterogeneity in the meta-regression analyses.
Publication bias
The funnel plot was basically symmetrical, and there was no evidence of publication bias using Egger’s test (P Egger’s=0·843) (online Supplementary Fig. S2).
Discussion
Our meta-analysis supports an inverse association between dietary vitamin E and stroke risk. Compared with individuals who have less dietary vitamin E intake, those with high dietary vitamin E intake have 17 % reduction in the risk of stroke. Total or supplemental vitamin E intake was not significantly related to a reduced risk of stroke. As a lipid soluble antioxidant, vitamin E demonstrates its ability to inhibit lipid peroxidation via scavenging reactive oxygen species and to preserve cell membranes( Reference Clarke, Burnett and Croft 22 ). In addition, some evidence shows that vitamin E can improve atherosclerotic plaque stability and vasomotor function, and inhibit platelet aggregation and thrombus formation( Reference Saldeen, Li and Mehta 23 , Reference Liu, Wallmon and Olsson-Mortlock 24 ).
The role of dietary vitamin E intake in stroke prevention was found to be inconsistent in the previous studies. Results from four prospective studies( Reference Hirvonen, Virtamo and Korhonen 4 , Reference Keli, Hertog and Feskens 5 , Reference Marniemi, Alanen and Impivaara 7 , Reference Ross, Yuan and Henderson 8 ) agree that vitamin E has no overall effect on the prevention of stroke or its subtypes (ischaemic or haemorrhagic stroke). Several lines of evidence show that dietary vitamin E may have a protective effect against stroke mortality in postmenopausal women( Reference Yochum, Folsom and Kushi 10 ), and on ischaemic smoke in male smokers( Reference Voko, Hollander and Hofman 9 ), while another prospective study suggests that a high vitamin E intake may be positively associated with the risk of haemorrhagic stroke( Reference Del Rio, Agnoli and Pellegrini 3 ).
The subgroup results reveal that dietary vitamin E tends to be beneficial in prevention of stroke for Non-East Asians (six cohorts) but not for East-Asians (two cohorts), and a possible explanation is that vitamin E intake (39·45 mg/d) in the China cohort is higher than the amount in all the remaining studies, while vitamin E intake (6·4 mg/d for females and 6·6 mg/d for males) in the Japan cohort is lower than the amount in all the remaining studies. Conversely, the vitamin E intake (from 10·96 to 24 mg/d) tends to be beneficial in preventing stroke among the remaining cohorts. The dietary vitamin E intake ranges from 6·4 to 39·45 mg/d. It is of interest that the online Supplementary Fig. S1 shows a ‘break in the downward slope’ associated with RR at approximately 15 mg/d, this is the same value as the recommended intake in the USA( Reference Council and Council 25 ). Thus, based on this evidence and the results of our meta-analysis, dietary vitamin E intake between 15 and 39·45 mg/d appears to be beneficial in prevention of stroke. The proportion of participants in the population who eat insufficient vitamin E is approximately 75 %. Although nine studies involving 3284 events and 220 371 participants were included in the final analyses, the statistical power was still limited. Therefore, the recommended daily allowances for vitamin E in prevention of stroke needs to be further addressed.
Dietary vitamin E tends to be beneficial in the prevention of stroke for females but not for males. However, the biological mechanisms are not clear. When the analysis was performed in cohorts with a larger number of participants (≥20 000), the beneficial effect of vitamin E persisted. BMI is a factor affecting the incidence of stroke( Reference Strazzullo, D’Elia and Cairella 26 , Reference Cheng, Huang and Bai 27 ), and when the analysis was adjusted for this confounder, the beneficial effects of dietary vitamin E persisted. Based on our results, dietary vitamin E intake is associated with a reduced risk of stroke for follow-up <10 years but not for follow-up >10 years. Thus, there may be an optimal time window for dietary vitamin E intake in the prevention of stroke, this may be explained by the inconsistencies of a wider range for studies with follow-up ≥10 years (range, 10–16·5 years) compared with studies with follow-up <10 years (range, 6·1–8 years). There was low heterogeneity (17 %) between the included studies. However, the sources of heterogeneity could not be determined using meta-regression analyses and subgroup meta-analyses.
Our findings, however, are inconsistent with those of the previous meta-analysis( Reference Myung, Ju and Cho 2 ) of RCT, which suggested that vitamins E intake is not associated with stroke risk. In addition, the use of vitamin E supplements in RCT should not be considered to be equivalent to the intake of olive oils, nuts and vegetables in prospective cohort studies, because these contain various other nutrients. For example, olive oil is rich in MUFA, which is inversely associated with haemorrhagic stroke( Reference Cheng, Wang and Shao 28 ). Nuts have a low SFA content (4–16 %) and high MUFA content, as well as a variable amount of PUFA, such as linolenic acid( Reference Grosso, Yang and Marventano 29 ), which is inversely associated with ischaemic stroke, possibly through potential mechanisms of decreased blood pressure, reduced platelet aggregation, and enhanced deformability of erythrocyte cells( Reference Iso, Sato and Umemura 30 ). Vegetables are rich sources of K and antioxidants (such as vitamin C), which are significantly associated with lower rates of stroke( Reference D’Elia, Barba and Cappuccio 31 , Reference Chen, Lu and Pang 32 ). Based on the included studies, the main dietary sources of vitamin E are derived from consumption of fruits, nuts, vegetable oils, and vegetables, and the proportion of vitamin E in each food varies. Therefore, our results suggest that the beneficial effects of vitamin E on the risk of stroke might be obtained from a combination of a higher proportion of vitamin E and a specific proportion of other dietary components.
There are several limitations in the current study. First, heterogeneity is present among the included studies, but the meta-regression analyses did not reveal any source of heterogeneity. Second, the included studies used both the cross-check dietary history method and the FFQ to assess dietary vitamin E intake, and thus, the estimated consumption of vitamin E might not be accurate. However, vitamin E intake was cross checked or validated in most of the included studies. Moreover, although observational studies adjusted for several confounders, residual confounding is still an issue, and confounding factors in each study may not be consistent. However, adjustment for major confounding factors should reduce the potential bias. Third, the results of subgroup analyses may not be robust because of the limited number of studies included. Finally, most of the studies were from America and Europe, and few studies were conducted in East Asia. Therefore, more studies need to be included from other parts of the world such as Asia.
In conclusion, this meta-analysis provides evidence that a higher dietary vitamin E intake is associated with a reduced risk of stroke.
Acknowledgements
The authors thank Jodi Smith, PhD, from Liwen Bianji, Edanz Editing China (www.liwenbianji.cn/ac), for editing the English text of a draft of this manuscript.
This work was supported by the Natural Science Foundation of Heilongjiang Province (grant no. H2016087), Natural Science Program of Health and Family Planning Commission of Heilongjiang Province (grant no. 2016-280), Natural Science Program of Jiamusi University (grant no. JMSURCGG2016-004).
The authors’ contributions are as follows: P. C. and L. W. contributed to the study design, literature search, data extraction and data analyses; S. N., Z. L. and H. L. conducted the literature search; S. C. and J. Z. extracted the data and conducted the statistical analyses; P. C. and L. W. wrote the first draft of the manuscript and edited the manuscript. All authors read and approved the final manuscript.
None of the authors has any conflicts of interest to report.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114518002647





