



Changes in dietary patterns, such as higher consumption of ultra-processed foods and drinks, and lower consumption of traditional foods, which by nature are less processed, are important determinants of obesity and related chronic diseases(Reference Monteiro, Moubarac and Levy1–Reference Poti, Braga and Qin4). Ultra-processed products have been dominating the current food systems(Reference Monteiro, Cannon and Moubarac3), influencing family purchase decisions(Reference Poti, Mendez and Ng5) and home food availability(Reference Monteiro, Moubarac and Levy1). Food advertising and aggressive marketing strategies of these products targeting parents and children, such as attractive packaging, health claims and the use of cartoon characters, have been observed(Reference Monteiro, Cannon and Moubarac3). Furthermore, as they are designed to be consumed anytime in any place, usually as snacks, drinks and ready-to-eat dishes, they may contribute to disarrange meals and displace cooking preparations at home(Reference Monteiro, Cannon and Moubarac3,Reference Lam and Adams6) .
Considering that ultra-processed foods are industrial formulations made mostly from a combination of various ingredients and substances, such as sugar, fat, salt and chemical additives to enhance their sensory qualities, they are commonly nutritionally unbalanced and hyper-palatable(Reference Monteiro, Cannon and Moubarac3–Reference Poti, Mendez and Ng5). Highly processed foods are in general energy-dense, high-fat and sweet tasting, which appear to be particularly related to addictive-like eating behaviour(Reference Schulte, Avena and Gearhardt7). They have been associated with a higher glycaemic response and with appetite triggering, leading to a low responsiveness to internal food cues and a higher responsiveness to external food cues(Reference Schulte, Avena and Gearhardt7). It has been suggested that ultra-processed foods may affect gastric and brain structures which regulate satiety, appetite and energy balance, prompting overeating and weight gain(Reference Schulte, Avena and Gearhardt7,Reference Fardet8) . Thus, their effects might be through their energy and/or from their additives. There is, however, little evidence to establish a rationale supporting energy intake as a mediator between ultra-processed foods and appetitive traits(Reference Schulte, Avena and Gearhardt7–Reference Small and DiFeliceantonio9).
Appetitive behaviours in children, mainly food-approaching traits (i.e. eating behaviours that imply movements towards food), are established as mediators to a later weight gain(Reference Albuquerque, Severo and Oliveira10–Reference Carnell and Wardle13). Although cross-sectional studies have shown positive associations of consumption of ultra-processed foods with BMI(Reference Louzada, Baraldi and Steele14) and other adiposity indicators(Reference Costa, Del-Ponte and Assunção2,Reference Costa, Pinto and Santos15) , there is still a need for longitudinal designs to better understand the relationships between ultra-processed food consumption and obesity among children and adolescents(Reference Costa, Rauber and Leffa16,Reference Leffa, Hoffman and Rauber17) . However, to the best of our knowledge, no studies have investigated the associations between ultra-processed consumption and appetitive traits in children.
In the present study, we hypothesised that ultra-processed food consumption influences appetitive behaviours in children, leading to increased later BMI. Our aim is to identify the diet contribution from food processing at 4 and 7 years of age and to assess the association of ultra-processed food consumption with appetitive behaviours at 7 years of age. We also seek to investigate whether appetitive behaviours at 7 years old are mediators to an increased BMI at 10 years old.
Methods
Study design and participants
The present study was conducted within Generation XXI, a prospective population-based birth cohort described elsewhere(Reference Larsen, Kamper-Jørgensen and Adamson18). A total of 8647 children and respective mothers were recruited between April 2005 and August 2006 at all the public maternity units in the Porto Metropolitan Area (Northern Portugal). These maternity units were responsible, at enrolment, for 91·6 % of the deliveries in the whole catchment population. Mothers were invited to participate 24–72 h after delivery, and 91 % of the invited mothers accepted to participate.
The three follow-ups of the entire cohort occurred between April 2009 and July 2011, April 2012 and April 2014, and July 2015 and July 2017, when the children were 4, 7 and 10 years of age (86, 81 and 76 % of the children were re-evaluated, respectively). The evaluations were performed by face-to-face interviews or by telephone with a shorter version of the questionnaire for those families not able to participate in-person (20, 15 and 16 % at 4, 7 and 10 years, respectively).
The present study involved a subsample of children evaluated at face-to-face follow-up evaluations at 4, 7 and 10 years old. We included data from 1407 children who provided at least 2-d food diaries at 4 and 7 years of age (even though 3-d food diaries correspond to the majority of the sample 96·5 and 96 % of the children, respectively by age) and information on the Portuguese version of the Children’s Eating Behaviour Questionnaire (P-CEBQ) at 7 and 10 years of age. We excluded twins, children with congenital anomalies or diseases that might influence dietary intake (coeliac disease, food allergy, food intolerance and phenylketonuria) and children who lacked data on variables of interest, achieving a final sample of 1175 children. Fig. 1 presents the flow chart of the study. Comparing the children included in the analysis with the remaining cohort, no statistical differences were found regarding children’s sex and BMI at 10 years of age. Mothers of children included in the study at baseline were slightly older (mean 30·5 (sd 4·74) v. 28·4 (sd 6·27) years, P < 0·001) and more educated (mean 11·9 (sd 4·26) v. 9·8 (sd 4·11) years of complete schooling, P < 0·001), even though the Cohen’s effect size was moderate (i.e. values of 0·36 for maternal age and 0·49 for maternal education level).
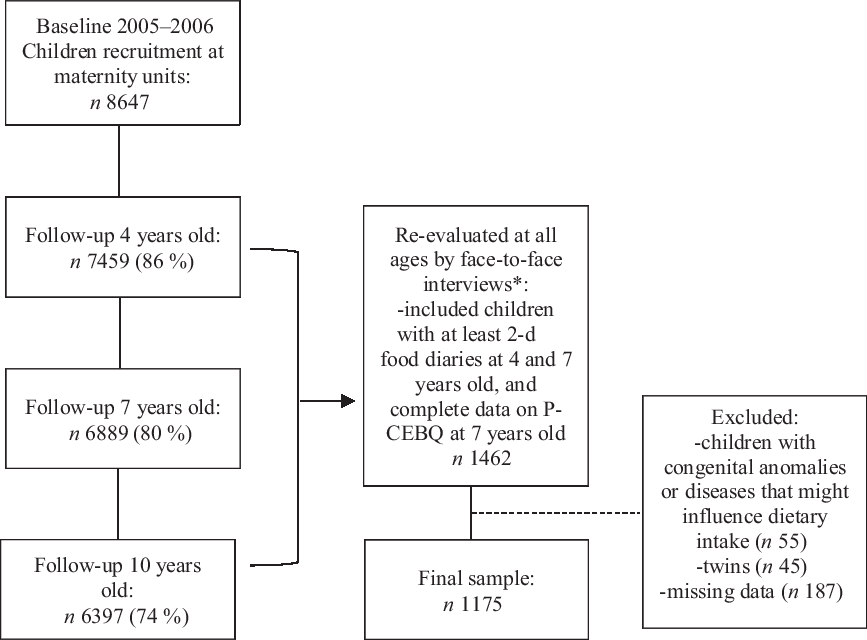
Fig. 1. Flow chart of the participants, Generation XXI birth cohort, Portugal. P-CEBQ, Portuguese version of the Children’s Eating Behaviour Questionnaire. * 70 % of all children at 4 years old, 68 % at 7 years old and 62 % at 10 years old.
The study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all the procedures involving human subjects were approved by the Ethics Committee of São João Hospital/University of Porto Medical School and by the Portuguese Authority of Data Protection. Parents or legal tutors of each participant received an explanation on the purposes and design of the study and gave written informed consent at baseline and follow-up evaluations.
Data collection
Data were collected by trained interviewers using structured questionnaires or by self-reported questionnaires filled out by the child’s main caregiver. They gathered information on socio-demographic, clinical and behavioural characteristics at 4, 7 and 10 years old.
Ultra-processed food consumption
Dietary intake of children at 4 and 7 years of age was measured by 2-d or 3-d food diaries (1 or 2 weekdays and 1 weekend day) filled by the mother and/or another adult caregiver, as previously described(Reference Vilela, Severo and Moreira19). Oral and written instructions were given for the correct completion of food diaries and for the quantification of food portions. Main caregivers were asked to report all foods and beverages consumed by the child and to provide detailed descriptions of each item, including the amount (in g, units or household measures), brand name, recipes (ingredients and methods of preparation) and location, whenever possible.
The codification process of food diaries was conducted by a team of trained nutritionists, using an age-specific food coding manual previously developed by the research team(Reference Vilela, Severo and Moreira19,Reference Moreira, Severo and Oliveira20) . Energy and nutrient intake was estimated using the software Food Processor SQL (2004–2005 ESHA Research), based on an adapted version of the Food Composition Table of the US Department of Agriculture(21). For typical Portuguese foods or culinary dishes, new codes were created with national nutritional information, as previously described(Reference Moreira, Severo and Oliveira20).
Food and beverage items were further classified into groups according to the nature, extent and purpose of industrial processing, based on the NOVA food classification system(Reference Monteiro, Cannon and Moubarac3) (Table 1). Groups 1 and 2 were grouped and consisted of unprocessed (i.e. natural foods having not undergone any kind of industrial processing), minimally processed (i.e. processed in ways that did not add substances or subtract edible parts), moderately processed foods (i.e. those that had an edible part subtracted, but no substance added, such as salt, sugar, oils or fats) and culinary preparations (i.e. handmade dishes made from these foods and basic culinary ingredients such as salt, sugar, honey, vegetable oils, butter and animal lards). Group 3 comprised processed foods (i.e. manufactured by adding salt, sugar, oil or fats to unprocessed, minimally or moderately processed foods), most foods having two or three ingredients and the industrial purpose to increase durability or to enhance sensory quality. Group 4 was composed of ultra-processed foods (i.e. industrial formulations typically with many ingredients and additives, most of them derived from foods or obtained with the further processing of foods constituents through chemical synthesis). Examples of the food items included in each group are presented in Table 1.
Table 1. Groups identified according to the nature, extent and purpose of industrial processing based on the NOVA food classification system(Reference Monteiro, Cannon and Moubarac3)

For each group, we calculated the total amount (in g or ml) consumed from each food or beverage items and expressed the consumption as a percentage of the total daily energy intake (for descriptive purposes) and in kcal (included in the statistical models, per 100 kcal, to enable readability of the estimates).
Appetitive behaviours
Children’s eating behaviours were assessed using the P-CEBQ, previously tested within the Generation XXI cohort(Reference Albuquerque, Severo and Oliveira10). Parents at the 7- and 10-year-old evaluations completed the questionnaire, being 96 and 91 % answered by mothers, respectively. The original CEBQ(Reference Wardle, Guthrie and Sanderson12) and the P-CEBQ(Reference Albuquerque, Severo and Oliveira10) measure appetitive traits in children and are composed of thirty-five items grouped into eight subdomains, four assessing food approach behaviours: ‘Enjoyment of Food’ (representing a general interest in food), ‘Food Responsiveness’ (measuring eating in response to external food cues), ‘Emotional Overeating’ (characterised by increased eating in response to negative emotions, such as anger and anxiety) and ‘Desire to Drink’ (evaluating the increased desire to have drinks); and four food avoidant behaviours: ‘Satiety Responsiveness’ (reflecting the ability to regulate the amount of food eaten, based on perceived fullness), ‘Slowness in Eating’ (measuring the speed of eating during the course of a meal and reflecting a gradually reduced interest in a meal), ‘Food Fussiness’ (measuring a lack of interest in food and unwillingness to try new foods) and ‘Emotional Undereating’ (characterised by decreased eating in response to negative emotions). The items were answered on a five-point Likert scale (‘never’, ‘seldom’, ‘sometimes’, ‘often’ and ‘always’), scored from 1 to 5. In accordance with the original scale, five of the items were reverse-scored due to opposite phrasing.
The CEBQ has demonstrated stability over time and good psychometric properties in diverse populations(Reference Wardle, Guthrie and Sanderson12,Reference Carnell and Wardle13,Reference Ashcroft, Semmler and Carnell22) including the current sample of children(Reference Albuquerque, Severo and Oliveira10). At 7 years old, the Cronbach’s alpha for the different subdomains of the P-CEBQ ranged from 0·74 to 0·85, attesting its good internal consistency, and the reliability assessed by the mean intraclass correlation was 0·73, attesting its good reliability(Reference Albuquerque, Severo and Oliveira10). At 10 years old, the Cronbach’s alpha of the P-CEBQ ranged from 0·76 to 0·84.
In participants with missing data in <50 % of the items, missing data (about 3 % at both 7 and 10 years old) were handled by imputation, replacing the average of the remaining questions within each subdomain(Reference Engels and Diehr23).
Additionally, at 4 and 7 years of age, problematic eating behaviours in children were assessed through single questions by a caregiver report. Caregivers were asked about specific perceived eating problems observed during the previous year and their level of concern (‘very concerned’, ‘somewhat concerned’, ‘not concerned’). The following questions were included in the analyses: ‘my child does not eat enough’, ‘my child eats very slowly’ and ‘my child eats too much’. As described previously(Reference Vilela, Hetherington and Oliveira24), these parental concerns were used as proxies of the subdomains of the CEBQ at 4 years of age, as at this age the P-CEBQ was not applied.
BMI
Participant’s anthropometric measurements were performed at the ages of 4, 7 and 10 years by a team of experienced examiners, according to standard procedures(Reference Gibson25). Children were weighed and measured barefoot and in light clothing. Weight was measured to the nearest 0·1 kg using a digital scale (Tanita®, Arlington Heights), and height was measured to the nearest 0·1 cm using a fixed wall stadiometer (SECA®). BMI was obtained by calculating weight/height2 (kg/m2). Age- and sex-specific BMI standard deviation scores (BMI z-scores) were computed according to the WHO criteria(26).
Potential confounders
Characteristics that may confound the association between ultra-processed food consumption, appetitive traits and BMI were considered. The following potential confounders were selected on the basis of previous literature and exploratory data analyses: maternal age, maternal education (number of completed schooling years) and BMI before pregnancy were recorded at baseline; exclusive breast-feeding for the first 6 months was recorded at 4 years old as ‘yes’ or ‘no’; parental concerns regarding child’s eating behaviour at 4 years of age (‘yes, ‘very/somewhat concerned/not concerned’ v. ‘no, ‘never happened’); the practice of regular physical exercise was collected at 4 years of age as a dichotomous response (‘non-practitioners’ v. ‘practitioners’); daily screen time (time spent in front of television/videos, computer or game devices) during both weekdays and weekends was also collected at 4 years of age and was categorised into <2 and ≥2 h/d.
Statistical analysis
Descriptive statistics were performed for maternal and child characteristics.
After checking normal distribution of food consumption data, Pearson’s correlation coefficient (r) and the intraclass correlation coefficient between the consumption of each of the NOVA food groups at 4 and 7 years of age were computed to assess tracking of dietary patterns. Intraclass correlation coefficient values between 0·81 and 1·00 were considered to represent almost perfect agreement, 0·61 and 0·80 substantial agreement, 0·41 and 0·60 moderate agreement, 0·21 and 0·40 fair agreement and values <0·21 slight agreement(Reference Landis and Koch27).
Associations between ultra-processed food consumption (group 4) at 4 years of age (exposure) and appetitive behaviours measured by the P-CEBQ subdomains (outcomes) at 7 years of age were evaluated through linear regression models (regression coefficients and respective 95 % CI). The following regression models were estimated: model 0 – crude (unadjusted); model 1 – adjusted for maternal characteristics (age, years of education and BMI before pregnancy) and model 2 – adjusted for maternal and child characteristics (exclusive breast-feeding for the first 6 months, parental concerning on eating behaviours, practice of physical exercise and daily screen time at 4 years of age).
The interaction of the child’s sex in these associations was investigated by including an interaction term into the fully adjusted models, but no modification by child’s sex was found in the linear regressions. Child BMI z-score was treated as a collider variable because it is believed to be ‘caused’ by both ultra-processed consumption and appetitive behaviours, and for that reason, it was not included as a confounder of the associations.
Another set of models was performed through the Haye’s PROCESS approach using 5000 bootstrap simulations to examine two potential mediators of the associations between the ultra-processed food consumption at 4 years and P-CEBQ subdomains at 7 years of age: energy intake from groups 1 + 2 and 3 (not ultra-processed foods) at 7 years of age (kcal/d), and ultra-processed food consumption at 7 years of age (kcal/d).
Additionally, we evaluated the mediating role of eating behaviours related to appetite in the associations between ultra-processed food consumption at 4 and 7 years of age and BMI z-score at 10 years of age: crude associations; model 1 (total effect) was adjusted based on theoretical considerations for variables associated with obesity (maternal education, BMI before pregnancy, exclusive breast-feeding, daily screen time and physical exercise), and direct and indirect effects of the subdomains of the P-CEBQ that showed associations with ultra-processed food consumption (parallel mediation); model 2 included the child BMI z-score at 4 years to isolate its effect. The indirect effect estimates for which the 95 % CI did not include zero were considered statistically significant, and thus evidence of potential mediations.
Sensitivity analyses were further performed to assess whether results would be substantively different using the exposure variable consumption of ultra-processed products (group 4) in percentage of total energy intake.
All the analyses were conducted using the statistical software package IBM SPSS® Statistics version 25 (SPSS Inc.), including the PROCESS macro version 3.5 for mediation analyses. Significance was defined as a P value of <0·05.
Results
Children and their mothers’ characteristics are described in Table 2. The study sample had 52 % of boys (data not shown). About 14 % were exclusively breastfed during the first 6 months of age. Over 91 % of children lived with parents, and 50 % had no siblings at 4 years of age. The majority of the children spent <2 h/d in front of a screen (67·2 %) and practiced regular physical activity (71·8 %) at 4 years of age. At the evaluations of 4, 7 and 10 years of age, 9·4, 13·7 and 17·2 % of children had obesity, respectively (data not shown).
Table 2. Participants’ characteristics (n 1175), Generation XXI birth cohort, Portugal (Mean values and standard deviations; numbers and percentages)

The children’s average reported energy intake from food diaries at 4 and 7 years of age was 6786 (SD 1214·2) and 7414 (SD 1242·2) kJ/d, respectively. Table 3 presents the tracking coefficients of food consumption from 4 to 7 years of age for the groups based on the NOVA food classification system. Ultra-processed food products (group 4) consumption corresponded to 27·3 % (1881·9 (SD 908·8) kJ/d) at 4 years old and 29·3 % (2204·5 (SD 961·1) kJ/d) at 7 years old. Group 4 exhibited stability coefficients slightly higher than groups 1 + 2 and 3, overall showing a fair level of agreement between measures at the two age frames.
Table 3. Tracking of food consumption groups based on food processing (the NOVA classification) from 4 to 7 years of age, Generation XXI birth cohort, Portugal (Mean values and standard deviations; correlation coefficients and 95 % confidence intervals)

r, Pearson’s correlation coefficient (two-tailed); ICC, intraclass correlation coefficient (computed for absolute agreement; two-way random model; single measures).
* P < 0·05, ** P < 0·001.
† Groups 1 + 2: Unprocessed, minimally and moderately processed foods, and culinary preparations. Group 3: Processed foods. Group 4: Ultra-processed food products.
The upper quartile of the ultra-processed food consumption (group 4) had the highest mean energy content (7744·6 (SD 1223·4) kJ/d) and a higher percentage of children following an ‘Energy-dense food’ (32·0 %) and ‘Snacking’ (31·8 %) dietary patterns (data not shown). These patterns were previously described in the literature as less healthy dietary patterns(Reference Durão, Severo and Oliveira28).
Significant positive associations between ultra-processed consumption at 4 years old and three subdomains of the P-CEBQ at age 7 were found in univariate analysis (Table 4, model 0): ‘Satiety Responsiveness’ (β = 0·022; 95 % CI 0·004, 0·039); ‘Food Fussiness’ (β = 0·034; 95 % CI 0·015, 0·054) and ‘Desire to Drink’ (β = 0·026; 95 % CI 0·005, 0·047). These significant associations persisted after adjustment for maternal confounders (Table 4, model 1), except for ‘Desire to Drink’. In the final adjusted models (further adjusted for child characteristics, Table 4, model 2), higher ultra-processed food consumption at 4 years old was significantly associated with later higher scores of ‘Food Fussiness’ (β = 0·026; 95 % CI 0·007, 0·045) at 7 years old.
Table 4. Associations between ultra-processed food consumption at 4 years of age‡ and appetitive behaviours at 7 years of age, Generation XXI birth cohort, Portugal§ (β Values and 95 % confidence intervals)

* P < 0·05
† Significant if the 95 % CI does not include zero.
‡ In kcal per 100 kcal/d.
§ Model 0: crude. Model 1: adjusted for maternal age, maternal education and BMI before pregnancy. Model 2: total effect – adjusted for maternal age, maternal education and BMI before pregnancy, exclusive breast-feeding for the first 6 months, parental concerns ‘my child does not eat enough’/‘my child eats very slowly’/‘my child eats too much’, daily screen time, and practice of physical exercise at 4 years. Mediation of energy intake from food groups 1 + 2 and 3 (kcal/d) at 4 years old: direct and indirect effects.
The consumption of ultra-processed foods at 4 years old had a significant direct effect on later increased ‘Food Responsiveness’ (β = 0·019; 95 % CI 0·007, 0·037), but no indirect effect (mediated by energy intake) was found (β = –0·002; 95 % CI 0·007, 0·002) (Table 4, model 2).
Energy intake was a mediator between ultra-processed consumption at 4 years old and both appetitive traits domains (Table 4, Model 2, indirect effect): ‘Satiety Responsiveness’ (β = –0·007; 95 % CI 0·003, 0·012) and ‘Food Fussiness’ (β = –0·007; 95 % CI 0·002, 0·012). Ultra-processed food consumption at 7 years old was not a mediator on the relationship between early ultra-processed consumption and appetitive behaviours at 7 years old (data not shown).
Ultra-processed food consumption at 4 years old was significantly associated with BMI z-score at age 10, after adjustment for maternal and child confounders (Table 5, model 2) (β = 0·028; 95 % CI 0·006, 0·051); and appetitive behaviours at 7 years old associated with early ultra-processed consumption (Food Responsiveness, Satiety Responsiveness and Food Fussiness) were not powerful mediators (Table 5, model 1 – indirect effect) (β = –0·002; 95 % CI –0·014, 0·011). Ultra-processed food consumption at 7 years old did not show an association with later BMI.
Table 5. Associations between ultra-processed food consumption at 4 and 7 years of age and BMI at 10 years of age, and the mediating role of appetitive behaviours, Generation XXI birth cohort, Portugal‡ (β Values and 95 % confidence intervals)

* P < 0·05.
† Significant if the 95 % CI does not include zero.
‡ Model 1: total effect – adjusted for maternal (age, education and BMI before pregnancy) and child (exclusive breast-feeding for the first 6 months, practice of physical exercise and daily screen time) characteristics. Mediation of appetitive behaviours at 7 years old associated with ultra-processed consumption (food responsiveness, satiety responsiveness and food fussiness): direct and indirect effects. Model 2: model 1 (total effect) + child BMI z-score at 4 years old.
Discussion
This study, to our knowledge, is the first to prospectively investigate, within a large population-based sample, the relationship between ultra-processed food consumption, appetitive behaviours and BMI in children. Higher ultra-processed consumption at 4 years of age was positively associated with food responsiveness (directly) and food fussiness and satiety responsiveness at 7 years of age (indirectly). For these two, energy intake mediated the relationship between early ultra-processed food consumption and food avoidant traits 3 years later. Furthermore, ultra-processed food consumption at 4 years of age was a predictor of higher BMI at 10 years old, and appetitive traits at 7 years old were not mediators of this relationship.
In the current study, the energetic contribution of ultra-processed products to the diet of pre-school and school-age children in Portugal (approximately 28 and 30 % of total energy, respectively) was lower than those found for other populations(Reference Costa, Del-Ponte and Assunção2,Reference Costa, Rauber and Leffa16,Reference Vandevijvere, De Ridder and Fiolet29) . Ultra-processed foods comprised about 42 % of total energetic intake at age 4, 48 % at age 8 in a Brazilian population sample(Reference Costa, Rauber and Leffa16) and 33 % in a Belgian population sample of children aged 3–9 years(Reference Vandevijvere, De Ridder and Fiolet29). Formerly, Portuguese households had shown a low availability of ultra-processed foods (10·2 %) and a high consumption of unprocessed or minimally processed foods (43·4 %), compared with that of other European countries over the period of 1991 and 2008(Reference Monteiro, Moubarac and Levy1). Despite this fact, dietary patterns high in energy-dense foods (such as sweets, soft drinks, salty pastry and processed meats) and low in foods typically consumed at main meals (such as vegetables, fish, meat, eggs, rice, pasta and potato) and intermediate in snacks were recently identified in Portuguese children at ages 4 and 7 years(Reference Durão, Severo and Oliveira28) and associated with a higher weight(Reference Ashcroft, Semmler and Carnell22). In the current sample, children with higher ultra-processed foods consumption (at the upper quartile) had followed more frequently these dietary patterns and had higher energetic intake.
Higher ultra-processed consumption at 4 years of age was positively directly associated with food responsiveness at 7 years old, which reflects the urge to eat when children see, smell or taste palatable food, such as ultra-processed foods. In a study with British and Australian pre-school children, food responsiveness was unrelated to liking fruits and vegetables, but was positively related to the preference for non-core foods (i.e. high in sugar and fat)(Reference Fildes, Mallan and Cooke30). Previous evidence suggests that highly palatable food-cues promote food-seeking behaviours even when in a state of satiety(Reference Schulte, Avena and Gearhardt7–Reference Small and DiFeliceantonio9) what is a risk factor for obesity(Reference Belfort-DeAguiar and Seo31).
Since ultra-processed foods and beverages are typically energy-dense(Reference Monteiro, Cannon and Moubarac3,Reference Hall, Ayuketah and Brychta32) , we tested the hypothesis that the association between the consumption of such products and appetitive traits was mediated, in part, by the energy intake. The usual method for adjusting ultra-processed food consumption for total energy intake in epidemiology studies is using total energy intake as a denominator. This method has the potential disadvantage of leaving some residual confounding regarding total energy content and, since total energy intake is associated with appetitive traits, it can induce an association in the opposite direction. For this reason, we used in the models the variable consumption of ultra-processed food and beverages in kcal/d instead of the percentage of total energy intake, even though it is most commonly used in other studies adopting NOVA classification(Reference Costa, Del-Ponte and Assunção2,Reference Louzada, Baraldi and Steele14,Reference Costa, Rauber and Leffa16,Reference Vandevijvere, De Ridder and Fiolet29) . It is worth to mention that sensitivity models using group 4 in percentage of total of energy intake were essentially similar to the models with kcal/d (results not shown). In fact, in this study, the energy intake was found to be a mediator of the relationship between high ultra-processed consumption at 4 years and food avoidant behaviours at 7 years of age, attenuating the total effects of ultra-processed foods in appetitive behaviours.
Increased consumption of ultra-processed products early in life was, surprisingly, associated with a later food avoidant eating profile comprising high food fussiness and satiety responsiveness. Food avoidant behaviours, in general, are related to insufficient food intake and lower energy intake(Reference Brown, Vander Schaaf and Cohen33). However, this does not mean that these children consume less energy-dense foods; preliminary data in this sample suggest that food fussiness, in particular, is negatively correlated with fruit and vegetables intake and positively correlated with ultra-processed food intake. The observed association may reflect food reward adaptations that result from increased consumption of ultra-processed products(Reference Small and DiFeliceantonio9). These products have higher amounts of sugar and fat, in combinations not encountered in natural foods, which seem to influence the fidelity of gut–brain signalling of food choices, that is, increased doses of those products increase food reinforcement(Reference Small and DiFeliceantonio9). In the current sample, mothers may have observed that children who eat more ultra-processed foods started to eat less of other foods, and thus reported higher food fussiness and satiety responsiveness among their children. Besides that, the early consumption of ultra-processed foods showed a direct effect (i.e. without mediating effect of energy content) on higher food responsiveness – a food approach behaviour – indicating that food properties other than energy density (e.g. combination of ingredients and other additives, orosensory properties), as well as the associated dietary patterns (e.g. snacking), may be implicated in satiety and food cue responsiveness in children and should be investigated further.
A high dietary share of ultra-processed products is associated with high content of added sugar, total and trans fatty acids, and low content of protein, fibre, vitamins and minerals(Reference Louzada, Baraldi and Steele14,Reference Rauber, Campagnolo and Hoffman34,Reference Cornwell, Villamor and Mora-Plazas35) . These cohort findings showed that the intake of ultra-processed foods and beverages was somewhat stable from 4 to 7 years of age. Dietary pattern stability throughout childhood corroborates other studies that observed some level of tracking in the same age span(Reference Vilela, Hetherington and Oliveira24,Reference Rauber, Campagnolo and Hoffman34,Reference Vilela, Severo and Moreira36) . Even though the Portuguese children’s ultra-processed consumption is relatively low in comparison with other child populations and has shown stability over the period analysed, the slight increase in consumption should be considered alarming because it may limit the consumption of homemade meals from unprocessed, minimally or moderately processed foods. Examining whether there is a displacement of food patterns as a result of increased ultra-processed consumption and if it extends to late childhood and adolescence warrant further research.
The present results revealed that higher consumption of ultra-processed products at 4 years of age was positively associated with higher scores in food fussiness at 7 years of age, regardless of child and maternal characteristics. This finding confirms previous evidences that children exhibiting less healthy dietary patterns early in life may later have some problematic eating behaviours related to appetite(Reference Albuquerque, Severo and Oliveira10,Reference Vilela, Hetherington and Oliveira24,Reference Vilela, Severo and Moreira36,Reference Cole, An and Lee37) . Fussy eating has been described as a common problem among young children(Reference Albuquerque, Severo and Oliveira10,Reference Vilela, Hetherington and Oliveira24,Reference Vilela, Severo and Moreira36–Reference Tharner, Jansen and Kiefte-de Jong39) , with a peak incidence at approximately 2 years of age, and that tends to decrease as the child grows older and is exposed to a wide variety of foods(Reference Ashcroft, Semmler and Carnell22,Reference Cole, An and Lee37,Reference Lafraire, Rioux and Giboreau40) . Vilela et al.(Reference Vilela, Hetherington and Oliveira24) observed in the same population-based cohort a general trend for a decrease in diet variety from 4 to 7 years of age. Considering that children are predisposed to prefer foods high in sugar and salt, and to reject bitter or sour tastes(Reference Taylor, Wernimont and Northstone38), in fussy children the intake of staple foods and fresh produce can be easily replaced by hyper-palatable processed foods(Reference Vilela, Hetherington and Oliveira24,Reference Vilela, Severo and Moreira36,Reference Cole, An and Lee37) , and it may be associated with destructured meals(Reference Powell, Farrow and Meyer41). Additionally, it is common that parents of fussy children, who are usually thinner, adopt mealtime strategies, such as offering commercially prepared nutrition supplement drinks and preparing special meals with well-accepted foods(Reference Hendy, Williams and Riegel42). Thus, children’s food preferences and counterproductive parents’ behaviours may increase the consumption of ultra-processed foods, limiting diet variety and intensifying food fussiness afterwards(Reference Brown, Vander Schaaf and Cohen33,Reference Tharner, Jansen and Kiefte-de Jong39,Reference Russell, Worsley and Campbell43) .
Increasing satiety responsiveness reflects a greater capacity of responsiveness to internal satiety cues; children feel fullness earlier(Reference Wardle11). In the current study, it was positively associated with prior higher consumption of ultra-processed foods. At short-term, ultra-processed products have been linked to lower satiety potential(Reference Schulte, Avena and Gearhardt7,Reference Fardet8) , and addictive-like eating behaviours, mainly as a result of the added fat through the activation of somatosensory brain regions, and of the refined carbohydrate content and high glycaemic load, which are involved in the activation of reward-related neural circuitry, craving and overeating(Reference Schulte, Avena and Gearhardt7). There is evidence that satiety responsiveness may have a strong genetic component(Reference Carnell and Wardle13) and may be associated with breast-feeding duration, weaning style(Reference Brown and Lee44), child emotional temperament(Reference Powell, Farrow and Meyer41) and lower child age(Reference Carnell and Wardle13,Reference Ashcroft, Semmler and Carnell22) . In Powell’s study (2011), mothers who reported higher satiety responsiveness of their children between 3 and 6 years old revealed the use of food as a reward, more pressure to eat, a less healthy food-related home environment and higher levels of dietary restraint themselves. Thus, behavioural factors within families(Reference Lam and Adams6,Reference Fildes, Mallan and Cooke30,Reference Tharner, Jansen and Kiefte-de Jong39) (e.g. poor food preparation skills by caregivers, infrequent habit of cooking, low preferences for vegetables and fruits) may also be linked to ultra-processed consumption, which appears to influence the child’s satiety responsiveness and may explain our results.
In the current study, when adjusting the models to child’s BMI at 4 years of age, we found ultra-processed food consumption at 4 years of age significantly associated with BMI at 10 years. Ultra-processed food consumption early in childhood has been linked to subsequent increases in the waist circumference(Reference Costa, Rauber and Leffa16), body fat(Reference Costa, Del-Ponte and Assunção2) and blood lipid levels(Reference Leffa, Hoffman and Rauber17,Reference Rauber, Campagnolo and Hoffman34) . In cross-sectional studies with adolescents, ultra-processed products were positively associated with the occurrence of obesity(Reference Louzada, Baraldi and Steele14) and the metabolic syndrome(Reference Tavares, Fonseca and Rosa45). The relationship between ultra-processed products and increased risk of weight gain and health-related problems has been shown(Reference Monteiro, Moubarac and Levy1–Reference Monteiro, Cannon and Moubarac3), but little is known about the mechanisms underpinning the association between such foods attributes and increased BMI in children, as well as the understanding of patterns of BMI changes across time. Recent studies have suggested that an increased contribution of ultra-processed foods in diets seems to cause a sustained increase in energy intake rate, and a subsequent longer-term overconsumption and weight gain in adults(Reference Hall, Ayuketah and Brychta32,Reference Forde, Mars and De Graaf46) . Besides being a result of the characteristics of ultra-processed foods (such as high energy density and lower satiety potential)(Reference Fardet8,Reference Forde, Mars and De Graaf46) , this increased energy intake rate can also reflect the individual’s appetitive drive to eat, particularly hyper-palatable foods.
The strengths of our study are its prospective design and the use of the NOVA classification as a prominent approach to identifying and tracking children’s dietary patterns based on the extent and purpose of food processing. Also, it adds to the literature by examining temporal relationships between ultra-processed consumption, appetitive traits and weight gain among children. There is a need for evidence exploring the determinants of appetitive characteristics in children(Reference Ashcroft, Semmler and Carnell22). The current study also has some limitations. First, we should consider that studies on children’s eating habits that involve caregiver’s report on child dietary intake and appetitive behaviours are particularly susceptible to misreporting and social desirability bias. Furthermore, children’s eating behaviours were assessed subjectively through caregiver’s report using the P-CEBQ, which can also be influenced by their emotional attitudes towards food. However, the CEBQ subdomains have shown good correlation with objective measures(Reference Carnell and Wardle13) and good psychometric properties in this population(Reference Albuquerque, Severo and Oliveira10). Moreover, the use of a self-administered questionnaire is likely to reduce social desirability bias. On the other hand, this could lead to low response rates. In the present analysis, we were able to recover missing data in cases with more than 50 % of the CEBQ items completed, which minimised the sample losses. In addition, the comparison between children included in the analysis and the remaining cohort suggests that participants have mothers with higher education, which may influence feeding practices and, consequently, children’s appetitive traits, being a potential study limitation. However, the magnitude of differences was not high and is likely due to the large sample size and not to systematic differences between participants. Another limitation was that we did not collect CEBQ data at 4 years of age. Nonetheless, parental concerns for problematic eating behaviour of children at 4 years were used as proxies of antecedent eating behaviour and were added to the models.
In conclusion, early ultra-processed consumption influences on later appetitive traits and BMI in childhood. The findings indicate that a higher consumption of ultra-processed foods at pre-school age children may lead to higher food approach behaviours, such as food responsiveness (direct effect), and food avoidant behaviours at 7 years old (indirectly through the mediation of energy intake). In addition, a higher consumption of ultra-processed foods at age 4 was prospectively associated with later increased BMI at 10 years of age, but appetitive behaviours at 7 years old did not mediate this relationship. Further studies should investigate mechanisms underlying the associations of the characteristics of ultra-processed products with dietary, metabolic, behavioural and environmental factors which lead to an increased risk of obesity and associated diseases.
Acknowledgements
The authors gratefully acknowledge the families enrolled in Generation XXI for their kindness, all members of the research team for their enthusiasm and perseverance and the participating hospitals and their staff for their help and support. We also acknowledge the support from the Epidemiology Research Unit (EPI-Unit: UID-DTP/04750/2013; POCI-01-0145-FEDER-006862).
Generation XXI was funded by the Health Operational Programme – Saúde XXI, Community Support Framework III and the Regional Department of Ministry of Health. This study was supported through FEDER from the Operational Programme Factors of Competitiveness – COMPETE and through national funding from the Foundation for Science and Technology – FCT (Portuguese Ministry of Education and Science) under the projects ‘Appetite regulation and obesity in childhood: a comprehensive approach towards understanding genetic and behavioural influences’ (POCI-01-0145-FEDER-030334; PTDC/SAU-EPI/30334/2017); ‘Appetite and adiposity – evidence for gene-environment interplay in children’ (IF/01350/2015) and through Investigator Contract (IF/01350/2015 – Andreia Oliveira). It had also support from the Calouste Gulbenkian Foundation.
The authors’ responsibilities were as follow: G. M. V. was involved in formulating the research questions, designing the study, analysing and interpreting the data, and writing the first draft of the paper; S. V. and M. S. were involved in analysing and interpreting the data and critically revising the paper; S. R. and C. L. were involved in interpreting the data and critically revising the paper; A. O. was involved in formulating the research questions, designing the study, analysing and interpreting the data, writing and critically revising the paper. All authors read and approved the final manuscript.
The authors declare that there are no conflicts of interest.






