



Athletes’ diets are one of several factors that influence their preparation for, performance in and recovery from competitive sport. The impact of diet on performance can be positive or negative(Reference Devrim-Lanpir, Hill and Knechtle1), but the margin between winning and losing efforts is also miniscule at times. Nutrition strategies for athletes include preparation for training and competition, as well as providing appropriate nutrients to support recovery(Reference Thomas, Erdman and Burke2,Reference Galiuto, Fedele and Vitale3) . Consuming a combination of macronutrients and micronutrients, in the appropriate amounts, at the right time can impact performance in training or competition as well as recovery and immune function(Reference Thomas, Erdman and Burke2,Reference MacKenzie, Slater and King4–Reference Venkatraman and Pendergast6) .
Previous research indicates that team-sport athletes’ dietary practices do not meet sport nutrition recommendations(Reference Jenner, Buckley and Belski7). Failure to meet recommendations can be detrimental to the health of the athlete and overall athletic performance(Reference Nepocatych, Balilionis and Hughes8); for example, not consuming appropriate amounts of protein can inhibit new protein synthesis(Reference Antonio9) or athletes not meeting energy requirements may experience unplanned weight loss(Reference Thomas, Erdman and Burke2), which may impact muscle mass as well as fat mass. It is therefore important to explore possible reasons why athletes might not meet these recommendations. Factors influencing dietary intake include gender, socioeconomic status, taste, convenience and possibly – the type of sport played, athletic level, nutrition support from sporting club, previous nutrition education and nutrition knowledge (NK)(Reference Heaney, O’Connor and Michael10,Reference Trakman, Forsyth and Middleton11) . Of these factors, NK has been explored frequently in recent peer-reviewed literature. A higher level of NK in the general population is associated with a greater intake of ‘healthy’ foods(Reference Worsley12), and there is evidence that there is a positive, but weak association between general NK and diet quality in athletes(Reference Birkenhead and Slater13,Reference Spronk, Heaney and Prvan14) .
General and sports NK can be assessed using several available tools(Reference Trakman, Forsyth and Hoye15–Reference Zinn, Schofield and Wall17), with new tools designed specifically for measuring NK in athletes developed in the past 5 years(Reference Trakman, Forsyth and Hoye18–Reference Tam, Gifford and Flood20). The current review focuses on tools developed in the past 5 years because it acts as an update to previous literature reviews, with the most recent having been published in 2016(Reference Trakman, Forsyth and Devlin21). As with all tools, validation must be completed to a sufficient degree to ensure results reflect outcomes being measured. Trakman(Reference Trakman, Forsyth and Devlin21) noted in a previous review that tools for measurement of NK were often not appropriately validated for use. Some tools used to measure NK may have undergone psychometric testing (i.e. have been validated) but may no longer be valid due to outdated information contained within the tool itself(Reference Trakman, Forsyth and Devlin21). Extensive modification of items within tools due to translation or changes to accommodate local diet trends may impact validation.
NK is thought to be poor amongst athletes. While there has been no set standard for what constitutes adequate NK, our previous literature review shows that mean percentage scores (i.e. percentage of correct responses) vary widely(Reference Trakman, Forsyth and Devlin21), with twenty-one of the included studies demonstrating scores below 60 %. Several studies have benchmarked the NK of athletes against other groups. A review found the NK of athletes to be equal to or greater than the NK of non-athletes(Reference Heaney, O’Connor and Michael10). One study comparing the NK of coaches, athletic trainers and strength and conditioning specialists from the National Collegiate Athletic Association (across all divisions and a wide variety of sports) found 9 % of athletes and 83·1 % of strength and conditioning specialists achieved a NK score >75 %(Reference Torres-McGehee, Pritchett and Zippel22).
A systematic review of athletes’ NK was published in 2016, providing equivocal results concerning the state of athletes’ NK at the time(Reference Trakman, Forsyth and Devlin21). A large number of studies have been published in this area since 2016. The recent development of current, validated tools has provided researchers with new tools with which to further study athletes’ NK(Reference Trakman, Forsyth and Hoye18–Reference Tam, Gifford and Flood20). This review differs from previous reviews in that it focuses on athlete NK and the relationship with athlete dietary intake(Reference Trakman, Forsyth and Devlin21,Reference Spronk, Kullen and Burdon23) with a systematic literature review study design(Reference Riviere, Leach and Mann24). These factors make it worthwhile to revisit a systematic review of athletes’ NK to determine if the previous conclusions on studies in this area are still applicable. The aims of this review are to summarise athletes’ general and sports NK scores reported in the past 5 years and to examine the quality of the tools used in the assessment of general and sports NK. The secondary aim of this review is to evaluate the association between athletes’ NK and dietary intake.
Materials and methods
This systematic review was conducted following the PRISMA guidelines(Reference Moher, Liberati and Tetzlaff25) and the protocol registered with PROSPERO (protocol registration ID CRD42020184263).
Search method
One reviewer (AJ) systematically searched the MEDLINE, CINAHL, Scopus, SPORTDiscus, Web of Science and Cochrane databases. For the Medline search, the terms Nutrition Knowledge and Athlete were mapped to the Subject Headings of Nutritional Sciences and Athlete, respectively (see online Supplementary Material for complete search). The following keywords were then added to the search: ‘Sport nutrition knowledge’ or ‘General nutrition knowledge’ or ‘Nutrition knowledge’ and Sport* or Athlete* (online Supplementary Material). References for all included studies were checked for further potential studies to be included in the final review.
Inclusion and exclusion criteria
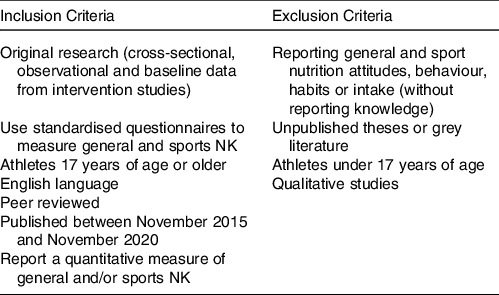
In order to be included in this review, studies were required to fulfil eligibility criteria as outlined in Table 1. Athletes were defined as any individual participating in an organised sport. Organised sport is defined as physical activity, involving competition and membership with sporting groups. For the purposes of this review, adolescents have been excluded due to the potential for age-related confounding factors.
Table 1. Inclusion and exclusion criteria
Screening process
Two reviewers (AJ and GT) independently screened all papers for eligibility by reviewing title and abstract, then full-text papers. Disagreements were addressed by discussion, or with a third reviewer (BD) where necessary. Three studies deemed eligible for inclusion through the initial screening process were not included because the full-text article could not be retrieved for data extraction.
Data extraction
A purpose-designed Google spreadsheet was used to extract data from the included studies. One reviewer (AJ) extracted the data from all included studies, and the second reviewer (GT) checked the extracted data for inconsistencies. Any inconsistencies were first discussed to attempt to reach consensus; if consensus could not be reached, the third reviewer (BD) was enlisted to decide. Data extracted with this form included author and date, basic study information (aim, location, setting, study design and recruitment methods), basic questionnaire information (questionnaire name, number of items and subsections included), secondary outcome measurement tool used and format, participant demographics (sample size, age and gender), primary outcome results (mean % score and range of the NK questionnaires) and secondary outcome results (dietary intake measures, either by macronutrient and/or micronutrient intake or food group intake), as well as correlation measures between NK and dietary intake where available.
Quality assessment
The quality of individual studies was assessed using the Joanna Briggs Institute Checklist for Analytical Cross Sectional Studies(Reference Moola, Munn and Tufanaru26), for assessment of all studies. This assessment tool was chosen as the most appropriate for the study design of studies included in the review. Guidelines for quality assessment were agreed upon among researchers.
Points were allocated for each question within the scale – ‘yes’ accounting for one point and ‘no’ or unclear receiving zero points for that question. Validity of the main NK assessment tool received a score out of two, with a tool requiring a minimum of three types of validity assessment to receive two points, and one or two types of validity assessment to receive one point. Due to differences in total possible points awarded to each paper, the final ranking for each paper was converted to a percentage to allow for comparison (online Supplementary Material).
Analysis
Due to the different NK assessment tools used across the reviewed studies, it was not possible to perform a meta-analysis on these results (see Table 2 for results). Synthesis for this systematic review is narrative – consisting of a descriptive comparison of results across studies. Where applicable, we also summate differences between genders, athletic ability, measurement tools and reported sports.
Table 2. Data extraction for NK in athletes
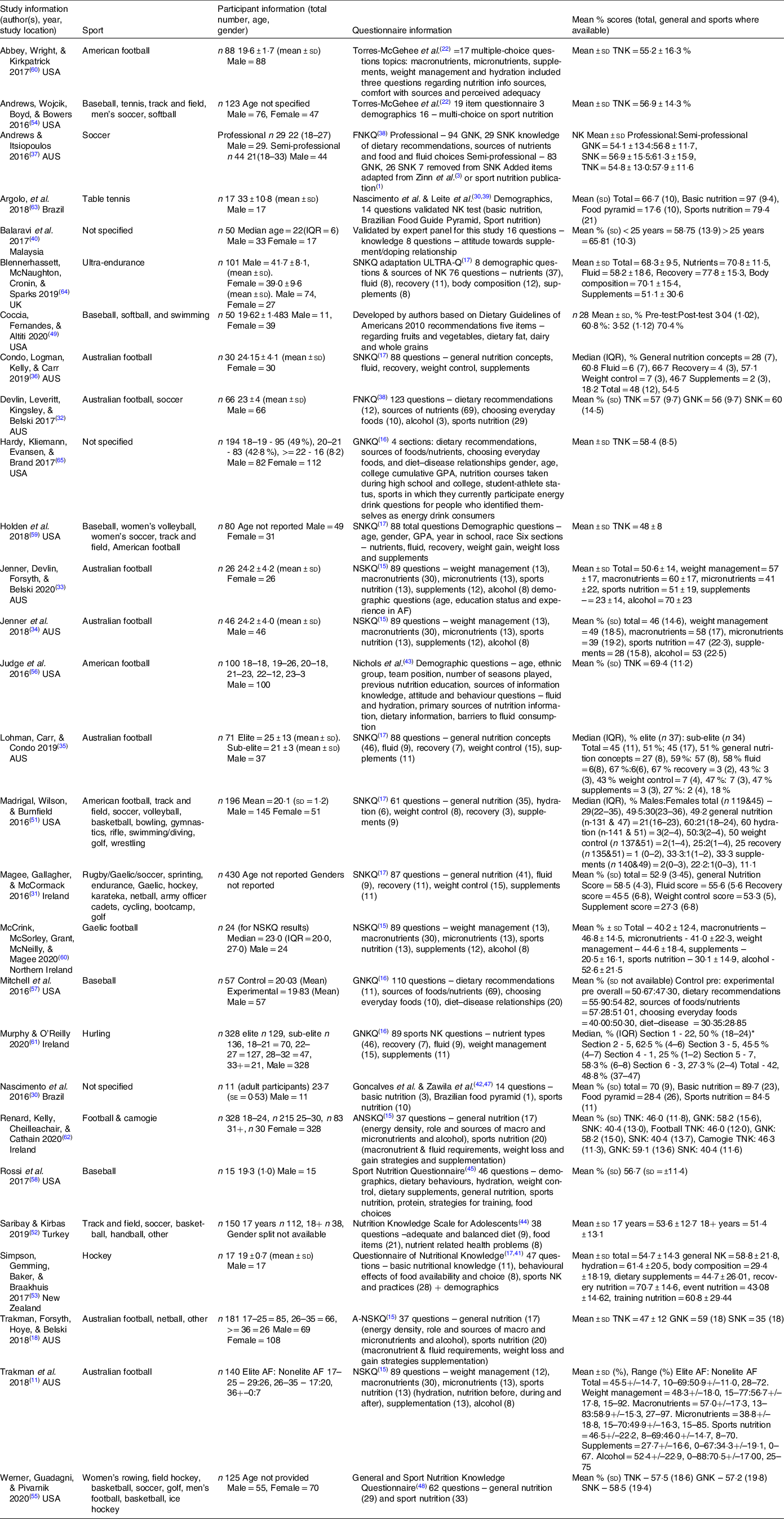
n, number of participants; sd, standard deviation; IQR, interquartile range; TNK, Total NK; GNK, General NK; SNK, Sports NK; AF, Australian football; FNKQ, Food and Nutrition Knowledge Questionnaire; SNKQ, Sports Nutrition Knowledge Questionnaire; GNKQ, General Nutrition Knowledge Questionnaire; NSKQ, Nutrition for Sport Knowledge Questionnaire; ANSKQ, Abridged Nutrition for Sport Knowledge Questionnaire.
* Reported as 18–14 in original paper, corrected values reported here.
Results
The initial search provided 1249 articles. After excluding articles that were published prior to November 2015 (n 100) and duplicated papers (n 312), there were 837 articles included in the abstract and title screening, with seventy articles eligible for full-text screening. Information on the selection process is presented below (Fig. 1). Three studies(Reference Elias, Saad and Taib27–Reference Dagcilar and Ozturk29) could not be retrieved for full-text screening through university subscription or contact with authors. Full-text screening resulted in twenty-eight studies included in the systematic review, with one additional paper identified through searching reference lists of included studies. One paper was removed during the data extraction process when it was identified as not meeting selection criteria for eligibility.
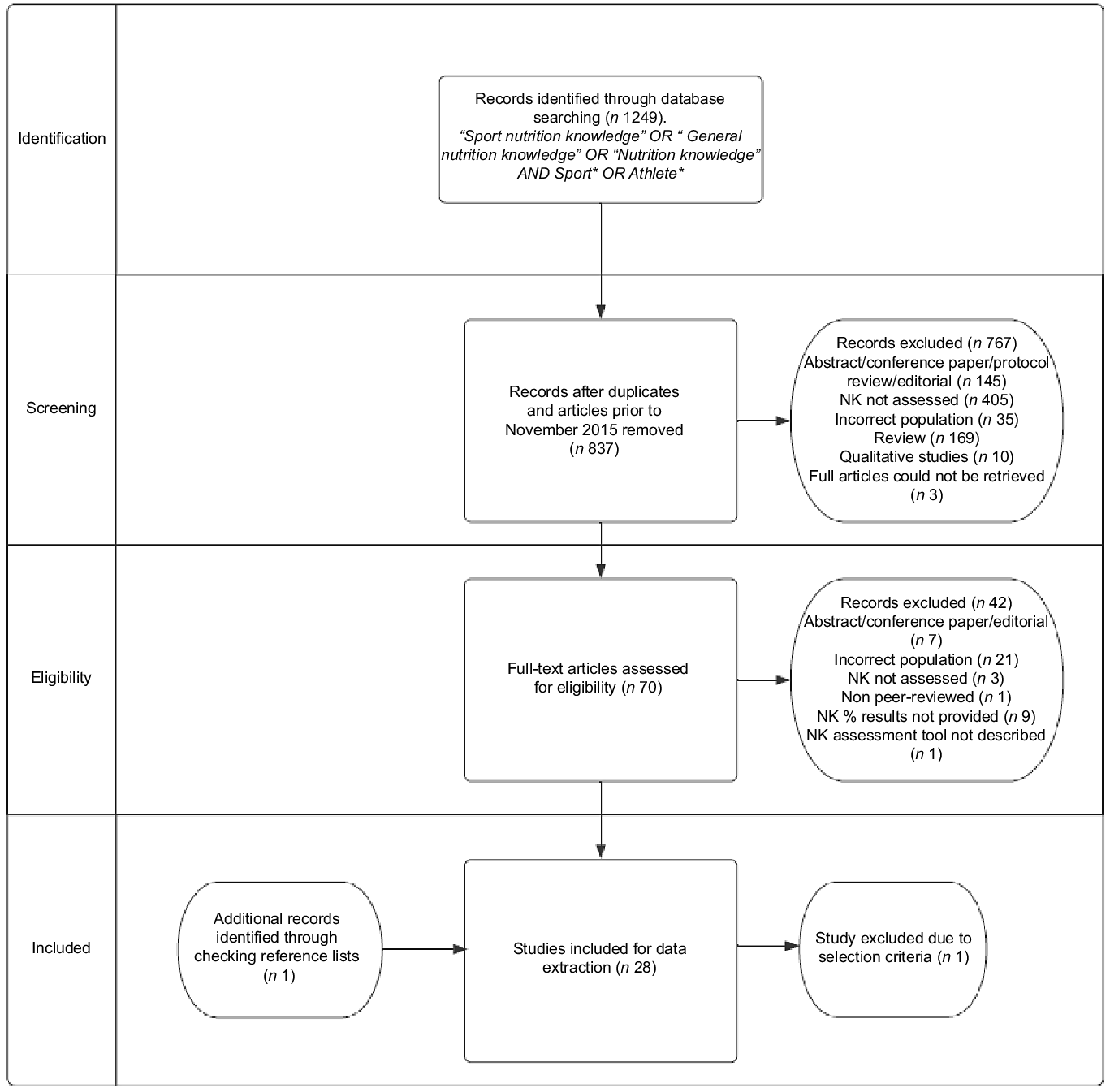
Fig. 1. Selection process flow chart. NK, nutrition knowledge; n, number of studies.
Study characteristics
The majority of studies (n 23) in this review utilised a cross-sectional design. The remaining five studies employed a quasi-experimental design, with education programme interventions. The results of included studies are presented in Table 2. These studies included 3117 participants in total, with eleven(Reference Nascimento, Silva and Ribeiro30) to 430(Reference Magee, Gallagher and McCormack31) participants per study. Nine countries were represented, with ten studies being conducted in the USA and eight studies conducted in Australia (Table 2). Thirty-four sports were represented in these studies, with Australian football, baseball and soccer being the most popular sports reported. Of the Australian studies (n 8), seven studies looked at Australian football(Reference Trakman, Forsyth and Middleton11,Reference Trakman, Forsyth and Hoye18,Reference Devlin, Leveritt and Kingsley32–Reference Condo, Lohman and Kelly36) , one paper also looked at soccer(Reference Devlin, Leveritt and Kingsley32), while another also included netball and ‘other’ participants(Reference Trakman, Forsyth and Hoye18); one Australian-based study looked exclusively at soccer(Reference Andrews and Itsiopoulos37).
Seventeen NK tools were used, in full or adapted by researchers, as the measurement tools across the included studies(Reference Trakman, Forsyth and Hoye15–Reference Zinn, Schofield and Wall17,Reference Torres-McGehee, Pritchett and Zippel22,Reference Nascimento, Silva and Ribeiro30,Reference Devlin and Belski38–Reference Coccia, Fernandes and Altiti49) . Due to the differences between NK measurement tools, it is not feasible to directly compare results from different tools as questions contained within tools can differ greatly. Where possible, we have made comparisons based on participant characteristics across studies that utilised the same tool.
Quality assessment
Raw quality assessment data for individual studies are available in Supplementary Material. Seven studies received 50 % or less for their quality assessment(Reference Coccia, Fernandes and Altiti49–Reference Werner, Guadagni and Pivarnik55). Fifteen studies scored between 51 and 80 %(Reference Nascimento, Silva and Ribeiro30–Reference Devlin, Leveritt and Kingsley32,Reference Jenner, Trakman and Coutts34–Reference Andrews and Itsiopoulos37,Reference Balaravi, Chin and Karppaya40,Reference Judge, Kumley and Bellar56–Reference Renard, Kelly and Cheilleachair62) . The remaining six studies scored between 81 and 100 %(Reference Trakman, Forsyth and Middleton11,Reference Trakman, Forsyth and Hoye18,Reference Jenner, Devlin and Forsyth33,Reference Argôlo, Borges and Cavalcante63–Reference Hardy, Kliemann and Evansen65) , with the highest rating of 100 % going to only one study(Reference Trakman, Forsyth and Middleton11).
Risks of bias within these studies mainly related to lack of validity of the NK tool in testing and generalisability of results. Sixteen of the included studies employed fully validated measurement tools; seven studies utilised partially validated measurement tools. This lack of validation for the measurement tools leaves the results produced by those studies open to measurement bias, making it difficult to ascertain athletes’ NK(Reference Trakman, Forsyth and Hoye15). While validated tools are available, these tools are not necessarily used appropriately by researchers. It is important to note here that validation does not speak to how up to date a tool may be and how current the information within it is.
Only seven of the included studies contained detailed information associated with the athletes’ training such as sport played, years playing sport, hours spent training per week or similar aspects related to athletic calibre. For the remaining twenty-one studies, the generalisability of results is difficult to ascertain. Other factors influencing the quality ratings of studies were lack of clear reporting of recruitment methods (n 14), response rates (n 23) and completion rates (n 19) of questionnaires.
Of note, recruitment of participants in many studies was reliant upon convenience sampling and study samples are often small; however, due to the small number of athletes involved in elite sports and heterogeneity of this group, small sample sizes may be representative of the target population.
Ten of the included studies examined correlation between NK and dietary intake; only six of these studies identified possible confounders and implemented a statistical strategy to deal with those confounding factors. This indicates an inappropriate use of statistical analysis within studies, potentially introducing statistical bias and misrepresentation of results.
Questionnaire
General Nutrition Knowledge Questionnaire (1999)
The General Nutrition Knowledge Questionnaire tool by Parmenter & Wardle(Reference Parmenter and Wardle16) was used in three studies in this review(Reference Mitchell, Holden and Forester57,Reference Murphy and O’Reilly61,Reference Hardy, Kliemann and Evansen65) . This tool was fully validated in a population of undergraduate students and contains 110 items with four subsections – dietary recommendations, sources of foods/nutrients, choosing everyday foods and diet–disease relationships. Total mean percentage scores for this tool ranged between 47·30 % (sd not available)(Reference Mitchell, Holden and Forester57) and 58·4 ± 8·5 %. Mitchell et al. (Reference Mitchell, Holden and Forester57) reported the scores for the subsections, which showed that the subsection with the lowest score was diet–disease relationships for both the control and experimental groups. The highest scores were in the subsection of sources of foods/nutrients for the control group and dietary recommendations for the experimental group.
Sports Nutrition Knowledge Questionnaire (2005)
Questionnaire use and validation
Six of the included studies employed the Sports Nutrition Knowledge Questionnaire (SNKQ)(Reference Zinn, Schofield and Wall17), which was fully validated for content, construct and test–retest validity in nutrition and business university students. One of these studies adapted and validated the SNKQ for use(Reference Blennerhassett, McNaughton and Cronin64), and this will be described below (ULTRA-Q Adaptation). Studies were in Australian football, baseball, volleyball, soccer, track and field, American football and a variety of collegiate sports(Reference Magee, Gallagher and McCormack31,Reference Lohman, Carr and Condo35,Reference Condo, Lohman and Kelly36,Reference Madrigal, Wilson and Burnfield51,Reference Holden, Forester and Smith59) . The SNKQ has a maximum eighty-eight items – subsections include general nutrition concepts, fluid, recovery, weight control and supplements. Three studies used this tool in full(Reference Lohman, Carr and Condo35,Reference Condo, Lohman and Kelly36,Reference Holden, Forester and Smith59) . The remaining two studies used eighty-seven and sixty-one items; the removal or alteration to items allowed for concepts to be updated to more recent recommendations, while maintaining the original subsection topics of the SNKQ(Reference Magee, Gallagher and McCormack31,Reference Madrigal, Wilson and Burnfield51) . Madrigal et al. and Magee et al. did not undertake or discuss tool validation after tool modification.
Results across studies and sub-section scores
Total percentage scores for studies using the SNKQ varied between 48 ± 8 % and 54·7 ± 14·3 %. Those studies that included results of subsections showed that participants often scored lowest in supplement sections(Reference Magee, Gallagher and McCormack31,Reference Lohman, Carr and Condo35,Reference Condo, Lohman and Kelly36,Reference Madrigal, Wilson and Burnfield51) . Performance varied across studies, with highest scores achieved in different subsections including nutrients(Reference Madrigal, Wilson and Burnfield51), fluids(Reference Lohman, Carr and Condo35,Reference Condo, Lohman and Kelly36) and recovery(Reference Simpson, Gemming and Baker53,Reference Blennerhassett, McNaughton and Cronin64) .
Comparisons across sports and athletic calibre
Due to the use of adapted or modified tools, the results of three of these studies could not be compared against those of other studies(Reference Magee, Gallagher and McCormack31,Reference Madrigal, Wilson and Burnfield51,Reference Blennerhassett, McNaughton and Cronin64) . The three studies able to be compared here looked at various sports: women’s Australian Rules football(Reference Condo, Lohman and Kelly36), baseball, women’s volleyball, women’s soccer, track and field, football(Reference Holden, Forester and Smith59) and elite and sub elite Australian football(Reference Lohman, Carr and Condo35). The three sports with highest scores for total NK were women’s Australian Rules football (Median = 60·8 %), and elite and sub-elite Australian Football (Median = 51 % and 51 %). The three sports with the lowest mean scores were American football (46 ± 7 %), track and field (48 ± 7 %) and women’s soccer (49 ± 1 %).
ULTRA-Q adaptation
The Blennerhassett et al. (Reference Blennerhassett, McNaughton and Cronin64) study investigated NK in ultra-endurance athletes. The tool used was a validated (for content validity and test–retest reliability) adaptation of the SNKQ, containing seventy-six items in the sections of nutrients (37), fluid (8), recovery (11), body composition (12) and supplements (8). Ultra-endurance athletes within this study had a total mean score of 68·3 ± 9·5 %. Results from this study are unable to be compared with studies utilising the SNKQ due to possible differences in the measurement tool caused by adaptation.
Torres-McGehee et al. (2012)
Questionnaire use and validation
Two studies(Reference Abbey, Wright and Kirkpatrick50,Reference Andrews, Wojcik and Boyd54) utilised adaptations of the partially validated (for construct validity) Torres-McGehee et al. tool(Reference Torres-McGehee, Pritchett and Zippel22), using either seventeen items or nineteen items within the questionnaire. Studies were in American football, baseball, tennis, track and field, soccer and softball. Andrews et al. (Reference Andrews, Wojcik and Boyd54) completed content validity testing and internal consistency testing using Cronbach’s α, making the tool partially validated. However, Abbey et al. (Reference Abbey, Wright and Kirkpatrick50) did not undertake any validation.
Results across studies and sub-section scores
The total mean nutrition scores were 55·2 ± 16·6 %(Reference Abbey, Wright and Kirkpatrick50) and 56·9 % sd = 14·3(Reference Andrews, Wojcik and Boyd54). Scores across sports have been compared; results show men’s soccer players achieved the highest score 59·4± %, followed by track and field (57·4 ± 11·3 %), tennis (56·7 ± 15·8 %), American football (55·2 ± 16·3 %), baseball (55·2 ± 15·0 %) and softball (54·4 ± 15·4 %). Abbey et al. (Reference Abbey, Wright and Kirkpatrick50) found that <50 % of participants correctly answered questions relating to athlete macronutrient balance, micronutrients, ergogenic aids, body composition and muscle mass, and >75 % of participants correctly answered items on fuel for exercise, creatine supplementation, rehydration and electrolyte loss(Reference Abbey, Wright and Kirkpatrick50).
No studies using this tool benchmarked athletic groups against other cohorts or compared results across athletic calibres.
Food and Nutrition Knowledge Questionnaire (2015)
Two studies(Reference Devlin, Leveritt and Kingsley32,Reference Andrews and Itsiopoulos37) utilised the Devlin & Belski tool(Reference Devlin and Belski38), which was originally developed as an amalgamation of the General Nutrition Knowledge Questionnaire tool and a sports specific knowledge assessment tool by Shifflet et al. (Reference Parmenter and Wardle16,Reference Devlin and Belski38,Reference Shifflett, Timm and Kahanov46) . Studies were in soccer and Australian football. This tool contains 123 items under the subsections of dietary recommendations, sources of nutrients, choosing everyday foods, alcohol and sports nutrition. This tool was not validated by Devlin and Belski(Reference Devlin and Belski38) in the original creation of this tool, nor was this validated by Devlin et al. (Reference Devlin, Leveritt and Kingsley32), although Andrews and Itsiopoulos(Reference Andrews and Itsiopoulos37) completed content validity testing on their modified version. Changes were made to the tool by Andrews and Itsiopoulos(Reference Andrews and Itsiopoulos37) when assessing the NK of semi-professional players, though the full tool was used to assess professional players in their study. The Andrews and Itsiopoulos(Reference Andrews and Itsiopoulos37) study found that semi-professional players had higher mean scores for all areas of the questionnaire than their professional counterparts – general NK (56·8 ± 11·7 % and 54·1 ± 13·4 %, respectively), sport NK (61·3 ± 15·9 % and 56·9 ± 15·5 %, respectively) and total score (57·9 ± 11·6 % and 54·8 ± 13·0 %, respectively). Devlin et al. (Reference Devlin, Leveritt and Kingsley32) reported a total NK score of 57 ± 9·7 %, General Nutrition Knowledge Questionnaire mean percentage score of 56 ± 9·7 % and sport NK score of 60 ± 14·5 %.
Nutrition for Sports Nutrition Knowledge Questionnaire (2017)
Six studies(Reference Trakman, Forsyth and Middleton11,Reference Trakman, Forsyth and Hoye18,Reference Jenner, Devlin and Forsyth33,Reference Jenner, Trakman and Coutts34,Reference McCrink, McSorley and Grant60,Reference Renard, Kelly and Cheilleachair62) employed the Nutrition for Sport Knowledge Questionnaire (NSKQ) or A-NSKQ(Reference Trakman, Forsyth and Hoye15,Reference Trakman, Forsyth and Hoye18,Reference Trakman, Brown and Forsyth66) . The NSKQ has eighty-seven to eighty-nine questions, broken into six subsections – weight management, macronutrients, micronutrients, sports nutrition, supplements and alcohol. Two studies utilised the abridged form of this tool, A-NSKQ(Reference Trakman, Forsyth and Hoye18,Reference Renard, Kelly and Cheilleachair62) , while the remaining four used the entire tool(Reference Trakman, Forsyth and Middleton11,Reference Jenner, Devlin and Forsyth33,Reference Jenner, Trakman and Coutts34,Reference McCrink, McSorley and Grant60) . The entire NSKQ tool was validated for content validity, construct validity and testing of item behaviour. The A-NSKQ(Reference Trakman, Forsyth and Hoye15,Reference Trakman, Forsyth and Hoye18,Reference Trakman, Brown and Forsyth66) was also validated for construct validity, internal validity and test–retest reliability and contains thirty-five or thirty-seven items in two subsections – general NK and sports NK.
The total mean percentage scores for the NSKQ ranged between 40·2 ± 12·4 % and 50·9 ± 11 %, while the A-NSKQ means were 47 ± 12 % and 46 ± 11·8 %. The studies that used the entire tool provided details of subsection results. The lowest scores across all studies were in the subsection of supplements, ranging between 20·5 ± 16·1 % and 34·3 ± 19·1 %. Female Australian football players (70 ± 23 %), Irish Gaelic football players (52·6 ± 21·5 %) and non-elite Australian Football players (70·5 ± 17 %) scored the highest results in the subsection of alcohol(Reference Trakman, Forsyth and Middleton11,Reference Jenner, Devlin and Forsyth33,Reference McCrink, McSorley and Grant60) . Elite and professional Australian Football players scored highest under the subsection of macronutrients (57 ± 17·3 % and 58·9 ± 15·3 %, respectively)(Reference Trakman, Forsyth and Middleton11,Reference Jenner, Trakman and Coutts34) . The studies using the shortened tool showed that athletes across the sports of Female Irish football and camogie players (GNK = 58·2 ± 15·6 %, SNK = 40·4 ± 13·0 %), Australian football players, netball players and ‘other’ athletes (GNK = 59 ± 18 %, SNK = 35 ± 18 %) scored higher in the general NK section of the questionnaire than the sports NK section(Reference Trakman, Forsyth and Hoye18,Reference Renard, Kelly and Cheilleachair62) . The results of the NSKQ and A-NSKQ cannot be compared due to the differences between the two tools.
The remaining studies used tools not used in any other study included in this review
Argolo et al. (Reference Argôlo, Borges and Cavalcante63) utilised an amalgamation of two questionnaires(Reference Nascimento, Silva and Ribeiro30,Reference Leite, Machado and Silva39) resulting in a fourteen-item tool containing sections on basic nutrition (3), Brazilian Food Guide pyramid (1) and sport nutrition (10), which was tested for discriminative validity, internal consistency and construct validity. For the table tennis players, the total percentage mean score was 66·7 ± 10 %. The area with the highest score was basic nutrition (97 ± 9·4 %). The area of lowest score was the food pyramid based on the Brazilian food pyramid (79·4 ± 21 %).
Balaravi et al. (Reference Balaravi, Chin and Karppaya40) generated a twenty-four-item tool for use in their paper containing sections on supplement NK (16) and attitudes towards supplement doping (8), which was partially validated by testing for content validity and internal consistency in Malaysian athlete populations. For the purposes of this study, the results of the supplement NK section of the tool will be reported. The results from this study showed that elite Malaysian athletes from various sports mean percentage scores of 58·75 % for athletes <25 years of age and 65·81 % for athletes over 25 years of age.
Coccia et al. (Reference Coccia, Fernandes and Altiti49) developed a five-item multiple choice tool for use in their paper that assessed NK related to fruits, vegetables, dietary fat, dairy and whole grains, which was not validated for use. The mean percentage score of the baseball, softball and swimming athletes was 60·8 ± 20·4 %.
Judge et al. (Reference Judge, Kumley and Bellar56) assessed NK in American football players using the seventeen-item tool developed by Nichols et al. containing items focused on hydration, which was tested for content validity in college athletes(Reference Nichols, Jonnalagadda and Rosenbloom43). The total mean percentage score from this study was 69·4 ± 11·2 %.
Nascimento et al. (Reference Nascimento, Silva and Ribeiro30) used a fourteen-question tool that was an amalgamation of two tools previously used(Reference Gonçalves42,Reference Zawila, Steib and Hoogenhoom47) containing sections on basic nutrition (3), Brazilian food pyramid (1) and sports nutrition (10). This study looked at athletes in various sports. Nascimento et al. (Reference Leite, Machado and Silva39) tested the resulting tool for validity, using construct validity test and item discrimination to achieve partial validation. Adults in this study had a mean percentage score of 70 ± 9 % for the overall questionnaire. Participants scored highest in the subsection of basic nutrition, 89·7 ± 23 % and lowest in the subsection on the Brazilian food pyramid, 28·4 ± 26 %.
Rossi et al.’s(Reference Rossi, Landreth and Beam58) study of baseball players utilised a partially validated, forty-six-item tool, which was an adaptation of the Sports Nutrition Questionnaire(Reference Reilly and Maughan45) containing sections on hydration, weight control, dietary supplements, general nutrition, sports nutrition, protein, strategies for training and food choices. The total mean percentage score for this study was 56·7 ± 11·4 %.
Saribay & Kirbas’s(Reference Saribay and Kirbaş52) adolescent athlete study used the thirty-eight-item tool developed by Oz et al. (Reference Öz, Aydin and Onsuz44) (Nutrition Knowledge Scale for Adolescents), which was tested for test–retest reliability and internal consistency; this tool contains subsections on adequate and balanced diet (9), food items (21) and nutrient-related health problems (8). Participants 18 years and older had a mean percentage score of 51·4 ± 13·1 %, and participants 17 years of age had a mean percentage score of 53·6 ± 12·7 %. No statistically significant difference was reported between age groups included in this study (14 years to 18 years and over).
Simpson, Gemming, Baker, & Braakhuis(Reference Saribay and Kirbaş52) employed an unvalidated, forty-seven-item tool adapted from Burkhart(Reference Burkhart41) and Zinn et al. (Reference Zinn, Schofield and Wall17) (Questionnaire of Nutritional Knowledge), which contains sections on basic nutritional knowledge (11), behavioural effects of food availability and choice (8) and sports NK and practices (28). The elite athletes in this study had an overall mean percentage score of 54·7 ± 14·3 %. Participants scored highest on questions related to recovery nutrition (70·7 ± 14·6 %) and lowest on questions related to body composition (29·4 ± 18·2 %).
Werner, Guadagni, and Pivarnik’s(Reference Werner, Guadagni and Pivarnik55) study of Division I collegiate athletes in the USA used the fully validated General and Sport Nutrition Knowledge Questionnaire, sixty-two-item tool first developed by Callela et al. (Reference Calella, Iacullo and Valerio48), which included subsections on general (29) and sport nutrition (33). The total mean percentage score was 57·5 ± 18·6 %.
Dietary intake
Twelve studies included data on dietary intake. Dietary intake was measured using a variety of methods: FFQ, food diaries, 24-h food recalls and 4-d semi-quantitative food records. Macronutrients were reported in various ways: grams per day, grams per kilogram of bodyweight per day, or percent of total energy intake. Comparisons between studies are limited due to varying methods of collecting and reporting diet intake data. Those studies including amounts of protein and carbohydrate measured in grams per kilogram of body weight per day(Reference Devlin, Leveritt and Kingsley32,Reference Jenner, Trakman and Coutts34–Reference Andrews and Itsiopoulos37,Reference McCrink, McSorley and Grant60,Reference Argôlo, Borges and Cavalcante63) had results varying between 1·1 g/kg.bw/d and 3·4 g/kg.bw/d of protein and 2·4 g/kg.bw/d and 4·6 g/kg.bw/d for carbohydrate. Daily carbohydrate intake recommendations for sport nutrition vary between 3 and 12 g/kg.bw/d, while daily protein intake recommendations for sport nutrition are between 1·2 and 2·0 g/kg.bw/d(Reference Thomas, Erdman and Burke2). Mean fibre values across studies (n 7) varied between 15 g and 45·8 g per d(Reference Jenner, Trakman and Coutts34–Reference Andrews and Itsiopoulos37,Reference Abbey, Wright and Kirkpatrick50,Reference McCrink, McSorley and Grant60,Reference Argôlo, Borges and Cavalcante63) . Studies reporting fat intake in grams per kilogram of body weight per day produced results between 0·9 g/kg.bw/d and 1·6 g/kg.bw/d(Reference Devlin, Leveritt and Kingsley32,Reference Jenner, Trakman and Coutts34,Reference Lohman, Carr and Condo35,Reference McCrink, McSorley and Grant60) . Saturated fat intake was reported as between 9·4 % and 13·4 % of total energy intake(Reference Lohman, Carr and Condo35,Reference Condo, Lohman and Kelly36,Reference McCrink, McSorley and Grant60,Reference Argôlo, Borges and Cavalcante63) . A summary of dietary intake data is provided in Supplementary Material.
A small number (n 5) of studies reported various micronutrient intakes. Na intakes ranged between 2063·3 mg and 9404·3 mg per d(Reference Condo, Lohman and Kelly36,Reference Abbey, Wright and Kirkpatrick50,Reference McCrink, McSorley and Grant60,Reference Argôlo, Borges and Cavalcante63) . Reported Ca intakes ranged from 648 mg to 1080·9 mg per d(Reference Jenner, Trakman and Coutts34,Reference Condo, Lohman and Kelly36,Reference McCrink, McSorley and Grant60,Reference Argôlo, Borges and Cavalcante63) . Potassium intakes fell between 3109 mg and 6298·1 mg per d(Reference Condo, Lohman and Kelly36,Reference Abbey, Wright and Kirkpatrick50,Reference McCrink, McSorley and Grant60) . Zinc intakes were between 8·8 mg and 11·7 mg per d(Reference Condo, Lohman and Kelly36,Reference McCrink, McSorley and Grant60,Reference Argôlo, Borges and Cavalcante63) .
Correlation between dietary intake and nutrition knowledge
Studies that examined correlations between dietary intake and NK (n 6) reported multiple associations, which are outlined in Supplementary Material. Andrews & Itsiopoulos(Reference Andrews and Itsiopoulos37) noted moderate positive correlations between sports NK and mean energy intake (r = 0·31, P = 0·04) in Australian soccer players, as well as between sports NK and carbohydrate intake (r = 0·35, P = 0·02). Argolo et al. (Reference Argôlo, Borges and Cavalcante63) found a negative correlation between Brazilian adult table tennis players’ total NK and their Na intake (r = –485, P < 0·05). Australian Football and soccer players displayed a weak, statistically significant, positive correlation between sport NK and both total energy intake and total carbohydrate intake (r 2 = 0·046, P = 0·014 and r 2 = 0·043, P = 0·039, respectively); a medium-large, statistically significant, negative correlation was also found in elite Australian football players between general and sports NK score and total protein intake (r 2 = 0·244, P = 0·026 and r 2 = 0·382, P = 0·016, respectively)(Reference Devlin, Leveritt and Kingsley32). A significant, negative correlation between NK scores in dietary recommendations and higher intake of caffeinated energy drinks was reported (r = 0·48, P < 0·001) in American student-athletes(Reference Hardy, Kliemann and Evansen65). A study of Australian football players(Reference Jenner, Trakman and Coutts34) demonstrated a moderate, positive association between NK scores and meeting estimated energy requirements (r = 0·325, P = 0·031), as well as NK scores being positively associated with protein, fibre and Ca intakes (r = 0·348, P = 0·021; r = 0·510, P = 0·001 and r = 0·428, P = 0·004, respectively). Murphy at al.’s(Reference Murphy and O’Reilly61) study of Irish hurlers found a weak to moderate positive association between NK and the Australian Recommended Food Score (a diet quality score validated for use in athlete populations) (r = 0·3, P = 0·007), with sub-elite players having a weak positive association (r = 0·26, P = 0·002) and elite players have a moderate positive association (r = 0·35, P = 0·006).
Discussion
NK amongst athletes is a popular topic, with twenty-eight studies published over the past 5 years included in this review. Thirteen of these included studies have also explored the dietary intake of athletes, and six studies reported correlations between NK and dietary intake. This review includes 3117 participants from nine countries, participating in thirty-four different sports.
According to evidence presented here, many athletes do not meet minimum NK requirements to ‘pass’ a NK test (based on the convention of 50 %, n 8), suggesting that they are unfamiliar with general and sports-specific dietary recommendations. Of the 10 studies that set a ‘pass’ mark for adequate NK, three studies using the NSKQ(Reference Trakman, Forsyth and Hoye15) for NK measurement achieved an ‘average’ or ‘medium’ score (non-elite AF players −50·9 ± 11 %, female AF players – 50·6 ± 14 %, variety of USA sports – 57·5 ± 18·6 %)(Reference Trakman, Forsyth and Middleton11,Reference Jenner, Devlin and Forsyth33,Reference Werner, Guadagni and Pivarnik55) . The remaining studies had poor or inadequate levels of NK(Reference Trakman, Forsyth and Middleton11,Reference Trakman, Forsyth and Hoye18,Reference Jenner, Trakman and Coutts34,Reference Abbey, Wright and Kirkpatrick50,Reference Andrews, Wojcik and Boyd54,Reference Holden, Forester and Smith59,Reference McCrink, McSorley and Grant60,Reference Renard, Kelly and Cheilleachair62) . Calculation of an overall mean score is not possible due to the use of different tools. Studies which had cut offs for ‘pass’ showed that athletes did not achieve passing marks. For other studies, mean percentage scores ranged between 40·2 % and 70 %. Because these were not benchmarked, it is difficult to say if these results are poor or not. These percentages seem low based on face value. Prior systematic reviews had a wider range of scores, with a low of 38·8 % and a high of 83·7 % in a 2016 systematic review(Reference Trakman, Forsyth and Devlin21) and scores between 34 and 71 % in a 2011 review(Reference Heaney, O’Connor and Michael10). This wide variety of potential scores may be related to the tools used to measure NK or the population in which NK is being tested. These results may indicate potential knowledge gaps in athletes that will enable athletic support staff to establish relevant nutrition education programs for athletes. It may be possible to use NK assessment tools to measure knowledge before and after the intervention to assess if the education program used was beneficial for the athletes.
Athletes’ poor NK could be due to a number of factors. Andrews et al. (Reference Andrews, Wojcik and Boyd54) suggest that the poor NK scores of collegiate athletes within their study may be due to a lack of emphasis on the importance of nutrition for athletic performance by coaches and trainers. A previous study of athletes, coaches, strength and conditioning specialists and trainers found that only 35·9 % of coaches, 9 % of athletes, 71·4 % of trainers and 83·1 % of strength and conditioning specialists had adequate NK(Reference Torres-McGehee, Pritchett and Zippel22), suggesting that coaches are not best placed to provide nutrition information to athletes and this task should be left to a team dietitian. Studies have reported mixed findings in relation to the association between having been given advice by a dietitian and NK, with researchers noting that a lack of an association may be because advice provided to athletes by team dietitians focuses more on practical food choice recommendations rather than the types of information assessed using NK tools(Reference Devlin, Leveritt and Kingsley32,Reference Andrews and Itsiopoulos37) .
As the recommended intake of protein and carbohydrate is dependent upon the type of sport and training the athlete is participating in, it is only possible to comment on these intakes when they either do not meet or exceed any recommended intakes. As such, it appears that athletes are below or meeting the requirements for carbohydrate intake for light intensity activities, when compared with current sport nutrition recommendations(Reference Thomas, Erdman and Burke2). The current sport nutrition recommendations for protein intake range between 1·2 and 2·0 g/kg.bw/d(Reference Thomas, Erdman and Burke2). However, the reported intake for protein indicates that some athletes are exceeding this range by 70 %, with a maximum mean intake of 3·4 g/kg.bw/d. A review examining protein intake in soccer players found that only two of the sixteen studies had participants with protein intake exceeding current sport nutrition guidelines (2·3 g/kg.bw/d), and in one study participants did not meet the recommendations (1·0 g/kg.bw/d)(Reference Burke, Loucks and Broad67). Burke et al.’s 2006(Reference Burke, Loucks and Broad67) review examined carbohydrate intake in soccer players indicated all soccer players included with the sixteen studies being reviewed consumed carbohydrate within the range for current carbohydrate recommendations (4·2–8·3 g/kg.bw/d). However, a 2019 review(Reference Steffl, Kinkorova and Kokstejn68) found a heterogeneous array of results for carbohydrate intake in soccer players (both junior and senior), with results between 2·9 g/kg.bw/d and 12·9 g/kg.bw/d, with senior players displaying a lower maximum carbohydrate intake than junior players (5·9 g/kg.bw/d and 12·9 g/kg.bw/d, respectively). Results of the current review indicate the athletes in the included studies consumed a much lower range of carbohydrate intake (2·4–4·6 g/kg.bw/d). The wider variety of sports included in the current studies should provide for greater variation in carbohydrate consumption due to differences in dietary requirements between sports. However, the smaller range of results may indicate a poor understanding of the benefit of carbohydrate consumption within the athletes included in the study or may be reflective of the popularity of low-carbohydrate diets in athletes in recent years.
The correlation between NK and dietary intake reported in this review demonstrates that those athletes with a higher level of NK are more likely to apply that knowledge to their dietary intake in a positive fashion. This includes moderate positive correlations between NK and other factors, including mean energy intake, carbohydrate intake, fibre, and Ca intakes, and negative correlations between NK and factors such as Na intake and energy drink intake. The relationship between NK and protein was examined in two studies(Reference Devlin, Leveritt and Kingsley32,Reference Jenner, Trakman and Coutts34) and found to be both positively correlated in professional Australian football players (r = 0·348, P = 0·021) and negatively correlated in elite Australian football players (r 2 = 0·244, P = 0·026 and r 2 = 0·382, P = 0·016, respectively). Spronk et al.’s(Reference Spronk, Kullen and Burdon23) systematic review found that higher NK in the general population was associated with greater intake of fruits and vegetables, cereals or fish, fibre, Ca and some core food groups, along with lower intake of fat and sweetened beverages, which could prove beneficial as small differences can be important in elite sports. This confirms that modifying NK is worthwhile when aiming to modify dietary intake. However, the difference in correlation between NK and protein intake suggests that further research is required to investigate this. Athlete protein requirements differ in relation to athlete goals, for instance increased protein intake in athletes wanting to increase muscle mass or those losing weight to minimise muscle loss. In these cases, it is possible that the high protein intake is impacted by an overall restriction of energy (including protein) to maintain lean physique; if protein intake is expressed as %E intake, a decrease in protein intake could reflect an appropriate increase in carbohydrate intake.
While NK has been found to have a weak, positive correlation with dietary intake in the general population(Reference Spronk, Kullen and Burdon23), NK is not the only factor that could potentially impact dietary intake. Birkenhead and Slater’s review(Reference Birkenhead and Slater13) placed these factors into the groups of ‘physiological and biological’, ‘lifestyle, beliefs and knowledge’, psychological, social and economic. To understand how a nutrition/dietetics professional may impact these factors, they have been classified into modifiable, semi-modifiable and non-modifiable factors(Reference Devlin69). No previous studies have examined relationships between the factors that are modifiable by nutrition/dietetic professionals (hedonic hunger, macronutrient balance, NK and body image and weight control) and dietary intake in athletes. A recent qualitative study of factors influencing dietary intake of professional Australian football players found four main categories of factors body composition assessment and goals, seasonal changes (preseason and competitive season), interpersonal factors related to peers, family and mood and NK and support(Reference Jenner, Belski and Devlin70). These factors closely relate to the factors of body image and weight control, macronutrient balance, hedonic hunger and NK(Reference Trakman71). Body composition assessment and goals are closely linked with body image and weight control, seasonal changes are related to alteration of macronutrient balance to achieve goals, the influence of peers and family is related to the availability of food and hedonic hunger and NK is a constant. This similarity between players’ understanding of influences on their dietary intake and factors that nutrition/dietetic professionals can influence the need to investigate these factors further.
Previous systematic reviews related to athletes’ NK have found that studies are flawed with inadequate statistical reporting, use of tools that are unvalidated(Reference Trakman, Forsyth and Devlin21) and a lack of benchmarking(Reference Heaney, O’Connor and Michael10), as well as use of tools that are outdated. The included studies in this review still exhibit a lack of complete validation with twelve studies not using fully validated tools for measuring NK; five studies used unvalidated tools(Reference Magee, Gallagher and McCormack31,Reference Calella, Iacullo and Valerio48–Reference Abbey, Wright and Kirkpatrick50,Reference Saribay and Kirbaş52) and seven studies used partially validated tools(Reference Nascimento, Silva and Ribeiro30,Reference Andrews and Itsiopoulos37,Reference Balaravi, Chin and Karppaya40,Reference Saribay and Kirbaş52,Reference Andrews, Wojcik and Boyd54,Reference Judge, Kumley and Bellar56–Reference Rossi, Landreth and Beam58) . Studies may fail to use appropriately validated tools because the methods of proving validity for a measurement tool can be time consuming and difficult to complete. Of note, where studies did use validated tools (n 16), eight studies utilised tools that were more than 15 years old(Reference Parmenter and Wardle16,Reference Zinn, Schofield and Wall17) . Due to the changes in practice and understanding around athlete nutrition within the past 15 years, it is unlikely that older tools reflect current recommendations. The questionnaires used in studies(Reference Trakman, Forsyth and Middleton11,Reference Trakman, Forsyth and Hoye18,Reference Jenner, Devlin and Forsyth33,Reference Jenner, Trakman and Coutts34,Reference Saribay and Kirbaş52,Reference Werner, Guadagni and Pivarnik55,Reference McCrink, McSorley and Grant60,Reference Renard, Kelly and Cheilleachair62) that utilised newer tools included the NSKQ (n 4)(Reference Trakman, Forsyth and Hoye15), the A-NSKQ (n 2)(Reference Trakman, Forsyth and Hoye18), The General and Sport Nutrition Knowledge Questionnaire (n 1) and an amalgamation of two tools that were validated for the study (n 1)(Reference Nascimento, Silva and Ribeiro30,Reference Leite, Machado and Silva39) . This selection indicates that there are a variety of tools available; it should be noted that this is not an exhaustive list of potential validated NK measurement tools for use. It is recommended that when selecting NK measurement tools, a tool that is validated within the research target population would be best or validation within the research target population should be carried out. In studies published since 2020, new, validated tools may not have been used extensively to date due to a possible delay in conducting studies (due to the COVID-19 pandemic) and publishing relevant results.
A recent systematic review by Capling et al. (Reference Capling, Beck and Gifford72) determined that there is substantial variability in dietary assessment methods in athletes. A variety of dietary assessment methods were used within the included studies, including FFQ (n 2), food record (n 1), 24-h food recall (n 1), 24-h dietary assessment tool (n 2), multi-pass 24-h food recalls (n 2), 3-day food diaries (n 2) and a 7-day food diary (n 1). While the dietary assessment methods used within these studies are validated and considered appropriate for use within the general population, there are some athlete-specific factors that these dietary assessment methods may not take into consideration. Because this is an emerging area of study, the validity of dietary assessment tools has been accepted as complete if it is a tool that has been validated for use within the general population.
There have been a number of reviews within this space. Spronk et al.’s 2014 review examined NK and dietary intake of community populations and athletes, with a larger focus on community population data(Reference Spronk, Kullen and Burdon23). Trakman et al.’s 2016 review examined the NK of athletes and coaches emphasising the knowledge gaps within these populations, without examining the dietary intake of athletes in relation to dietary intake(Reference Trakman, Forsyth and Devlin21). A recent narrative review examines NK of USA collegiate athletes and how sports dietitians impact NK and behaviours in those athletes, excluding athletes outside of USA collegiate sport(Reference Riviere, Leach and Mann24). Heaney et al.’s 2011 review combined NK and dietary intake in athletes; however, there has been a wide variety of research published between 2011 and 2020 requiring evaluation in this space(Reference Heaney, O’Connor and Michael10). It can be seen from the evidence here that an updated review of this area was required which examined the relationship between NK and dietary intake in athletes specifically.
Limitations
A limitation of this paper is the quality of the studies included in this review. The majority of studies included in this review were cross-sectional studies, or quasi-experimental studies, with many studies having small participant groups without mentioning power calculations, which may impact the generalisability of the studies to the wider target populations. Some of the tools used to assess NK are also limiting. Tools were not designed for assessment of athlete populations(Reference Parmenter and Wardle16,Reference Öz, Aydin and Onsuz44) were more than 10 years old and likely out of date (i.e. not reflective of current nutrition recommendations)(Reference Parmenter and Wardle16,Reference Zinn, Schofield and Wall17,Reference Gonçalves42,Reference Nichols, Jonnalagadda and Rosenbloom43,Reference Reilly and Maughan45–Reference Zawila, Steib and Hoogenhoom47) , or have not been fully validated(Reference Nascimento, Silva and Ribeiro30,Reference Devlin, Leveritt and Kingsley32,Reference Andrews and Itsiopoulos37,Reference Balaravi, Chin and Karppaya40,Reference Abbey, Wright and Kirkpatrick50–Reference Andrews, Wojcik and Boyd54,Reference Judge, Kumley and Bellar56–Reference Rossi, Landreth and Beam58) . Therefore, results must be interpreted with caution. A wide range of tools used to assess NK made comparison of results difficult between studies; therefore, a meta-analysis was not possible for this review. NK scores measured with tools that do not provide ratings or pass values have not been benchmarked against other population groups (e.g. nutrition experts or community populations), which provides results without context within the larger NK landscape. Dietary intake results are also heterogeneous, making comparisons difficult across all applicable studies. This review has examined the influence of NK on dietary intake, but other influences on dietary intake have not been investigated here.
A large portion of the included studies were conducted in American and European populations across a wide range of sports. All controls or comparators within the included studies were athletes. It should be noted that inadequate descriptions of sporting levels or calibres make comparing these results between studies problematic, as these descriptions may be different between countries and sports. No studies compared the NK of athletes to community populations.
Publication bias is possible as grey literature was not examined, and three studies could not be retrieved to be screened. There is also a possibility that studies in this field have not been published due to negative or inconclusive results. This review was limited to studies published in the English language and thus may have excluded some studies on the basis on language or region. This form of bias is not often an issue within this field, due to the smaller scale studies including relatively small sample sizes.
Conclusion
This review suggests that athletes have poor general and sports NK and often do not meet nutrition recommendations. However, inconsistent validation of tools used in these studies mean that these results must be interpreted with caution. NK and dietary intake were weakly associated in athletes. There are flaws in the measurement of NK, due to lack of validation. Newly created NK assessment tools are lending greater reliability to the results produced. It is necessary for future research to examine a population of athletes, across varying sporting levels, types, and regions, investigating NK and its correlation with dietary intake. It would be beneficial to also benchmark athlete general and sport knowledge and dietary intake against that of community populations. Finally, future studies should consider undertaking a holistic investigation of modifiable factors influencing athletes’ dietary intake by looking at NK in combination with other modifiable factors that may impact dietary intake.
Acknowledgements
This review has been completed as part of an Honours degree at La Trobe University, Australia.
No funding has been provided for this review.
A. J. completed independent screening, data extraction, quality assessment, and drafted the manuscript. G. L. T. completed independent screening, data extraction, quality assessment, and assisted with manuscript preparation. B. L. D. assisted in decision making regarding screening and data extraction and reviewed with manuscript. A. F. assisted with manuscript preparation.
There are no conflicts of interest.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114521004311





