


The first 1000 d of a child’s life are paramount to the establishment of good health and good eating practices( Reference Barker 1 ). Current national survey data provide evidence at a population level that young children are at high risk of gaining excess weight, complemented with poor eating habits and inadequate physical activity. According to the 2007 Australian National Children’s Nutrition and Physical Activity Survey( 2 ), 21 % of boys and 18 % of girls, aged 2–3 years were classified as overweight and obese. In the Australian Health Survey 2011–2012 23 % of 2–4-year-olds were overweight/obese( 3 ). In addition, the AHS 2011–2012 assessed ‘discretionary foods’, such as cakes, soft drinks, ice cream, pies, hot chips and high fat take-away items contributed 30 % of total energy intake among 2–3-year-old children, with biscuits accounting for most. About 33 % of 2–3-year-old boys and 27 % of girls consumed sugary drinks the day before the interview.
There is convincing evidence that the family environment is important in influencing dietary behaviours( Reference Pearson, Biddle and Gorely 4 ). With the growing problem of childhood obesity, recent research has begun to focus on family and social influences on children’s eating patterns as these are strongly influenced by both the physical and social environment( Reference Patrick and Nicklas 5 ). The role of parents and the techniques used in the context of child feeding are critical in determining children’s weight status( Reference Stewart and Thompson 6 ). Hence, an understanding of the factors which influence food-habit formation in early life may help prevent the onset of predisposing obesity risk behaviours in children.
In an earlier study on 4-year-old Canadian children, only 17 % of children met recommended fruit and vegetable intakes, with approximately 50 % meeting milk requirements and 40 % exceeding meat intake( Reference Dubois, Farmer and Girard 7 ). In the Canadian study maternal immigration status, maternal education, household income and child’s sex predicted the likelihood of meeting recommended dietary guidelines; however, contributions of energy-dense foods were not included. In the ‘Growing up in Australia Study’( 8 ), it was reported that 89 % of 2–3-year-old children met Australian Guide to Healthy Eating (AGHE)( 9 ) recommendations of one serve of fruit per d and 49 % consumed two or more serves of vegetables per d. A third of 2–3-year-old children were having at least one or more serves of soft drink per d and one-fifth were having at least two or more serves of sweet energy-dense foods such as biscuits, chocolate, lollies and non-sweet energy-dense foods (such as meat pies, hamburgers, hot dogs, sausages or sausage rolls, hot chips or French fries). However, parental predictors of dietary intake were not assessed among 2–3-year-old children in that study. In Australia, the NOURISH and South Australian Dietary Intake studies, described dietary patterns of the 2-year-old cohorts as either: the ‘24-month core foods’ pattern, which included fruit, vegetables, dairy products, nuts/seeds, meat and water; or ‘non-core foods’ which included spreads, sweetened beverages, snacks, chocolate and processed meat. Lower maternal age was associated with higher ‘non-core food’ pattern scores at 14 months and maternal university education was associated with a higher ‘core food’ pattern at 14 and 24 months, but these associations were not significant( Reference Bell, Golley and Daniels 10 ).
More recent studies that have examined family correlates and eating behaviours have been carried out in older children (6–18 years)( 8 , Reference Van der Horst, Oenema and Ferreira 11 – Reference Pearson, Biddle and Gorely 13 ). Few studies have examined the same specific family correlates and eating patterns in young children, limiting the possibility of drawing strong or consistent conclusions. Hence this study aimed to: (a) provide a descriptive view of 2-year-old children’s eating patterns including both ‘healthy eating recommendations’ and contributions of ‘discretionary energy-dense’ foods, (b) examine maternal socio-demographic variables in predicting children’s dietary patterns and (c) determine if maternal and child dietary patterns are positively correlated and to what extent.
Methods
Study design
A cross-sectional analysis was conducted using data from the Healthy Beginnings Trial (HBT), a home-based randomised controlled trial that recruited 667 first-time mothers from one of the most socially and economically disadvantaged areas of south-west Sydney from 2007 to 2010( Reference Wen, Baur and Rissel 14 ). This study was conducted according to the guidelines laid down in the Declaration of Helsinki and was approved by the Ethics Committee of Sydney South West Area Health Service (RPAH Zone) (X04-0189, X10-0312 and HREC/10/RPAH/54). Details of the research protocol and outcomes of the HBT have been reported elsewhere( Reference Wen, Baur and Rissel 14 , Reference Wen, Baur and Simpson 15 ).
Participants
In total, 667 first-time mothers at 26–36 weeks of pregnancy were recruited to the trial from antenatal clinics at Liverpool or Campbeltown hospitals, located in south-western Sydney, New South Wales, Australia. First-time mothers who spoke English were eligible for inclusion in the trial. Once eligibility was established and consent obtained, mothers were asked to fill in their contact information to allow nurses to make arrangements for baseline data collection. For this analysis, only mothers who were allocated to the control group and whose children were aged 2 years (n 243) were selected to avoid any potential confounding effects of the intervention. Thus, participants were mother–child dyads in the HBT control group only.
Data collection and measures
Face-to-face interviews with each participating mother were conducted by two research assistants to collect mothers’ demographic information at baseline (26–36 weeks of pregnancy), and assess maternal and child’s dietary behaviours at 2 years.
Dietary behaviours of children aged 2 years and their mothers
Dietary behaviours were measured using short FFQ (sFFQ)( Reference Flood, Wen and Hardy 16 )questions from the New South Wales Child Health Survey. These were collected via face-to-face interviews. Mothers were asked to report their children’s intake of vegetables, fruit, water, milk, soft drinks, sugary drinks, processed meats, fast food, hot chips, confectionery, salty snacks and sweet snacks. Mothers’ own dietary behaviours were assessed with questions sourced from the New South Wales Health Survey Program in New South Wales, Australia. Both questionnaires have been validated in child( Reference Flood, Wen and Hardy 16 ) and adult populations( Reference Wen, Flood and Simpson 17 ), respectively, and the latter has been widely used in population health surveys in New South Wales( 18 ). Some examples of the questions used in the study are as follows:
-
(1) How many serves of vegetables (does your child/do you) usually eat each day? (Include fresh, dried, frozen and tinned vegetables. One serve=½ cup cooked or 1 cup of salad vegetables).
-
(2) How many serves of fruit (does your child/do you) usually eat each day? (Include fresh, dried, frozen and tinned fruit. One serve=1 medium piece or 2 small pieces of fruit or 1 cup of diced pieces).
-
(3) How many cups of soft drink, cordial, or sports drink, such as lemonade or Gatorade, (does your child/do you) usually drink in a day? (One cup=250 ml. 1 can of soft drink=1 ½ cups. 1×500 ml bottle of Gatorade=2 cups) (Do not include diet drinks).
-
(4) How often (does your child/do you) have meals or snacks such as burgers, pizza, chicken, or chips from places like McDonalds, Hungry Jacks, Pizza Hut, KFC, Red Rooster or local takeaway food places?
In addition, socio-demographic information was collected, including mother’s age, employment status, education level, marital status, language spoken at home and mothers’ country of birth using the NSW population health survey questionnaire( 18 ).
Variables of interest
Mother–child dietary intake
Cut-points for mother–child dietary comparisons were derived from the recommended number of servings in the dietary guidelines where appropriate. Child dietary cut-points were half that of mother’s, as based on the Australian Dietary Guidelines( 19 ); most core food dietary recommendations for children aged 2 years are half that of adults. Hence cut-points for vegetables, fruit, fruit juice, water and discretionary food items: sugary drinks and soft drink were halved for children compared with adults, except milk which forms a substantial component of a young child’s diet. For frequency of consumption questions pertaining to fast food, hot chips and processed meat, the same cut-points were used for both mother and child (online Supplementary Table S1).
Analysis
Statistical analyses were carried out using Statistical Package for Social Science (SPSS) for Windows version 19 (SPSS, Inc.). Descriptive statistics including means and standard deviations for various dietary variables were calculated. Consumption frequencies were then categorised and proportions were compared between groups for thirteen food categories: fruit, vegetables, water, milk, soft drinks, fruit juices, sugary drinks, hot chips, fast foods, processed meats, salty snacks, sweet snacks and confectionery using Pearson χ 2 tests for trend in proportions. One-way ANOVA was used to investigate differences in dietary consumption patterns of 2-year-old children based on maternal socio-demographics. Tests for normality were confirmed using probability plots. Kruskal–Wallis one-way test or Mann–Whitney U test was used when the variables were not normally distributed. Mothers’ intake for the foods: salty snacks, sweet snacks and confectionery was not assessed so these were excluded in comparative statistics but were included in the descriptive statistics for children’s intakes. Pearson’s correlation was used to examine the associations between mother/child intakes.
Binary logistic regression was used to examine the maternal predictors of children’s eating behaviours. Based on the literature, the following maternal and child characteristics were considered: child’s sex, mother’s marital status, mother’s country of birth, maternal BMI (healthy weight (BMI 18·5–24·9 kg/m2), overweight (BMI 25–29·9 kg/m2) and obese (BMI ≥30 kg/m2)), breast-feeding duration and number of children in the family. Food group intake was dichotomised to reflect adherence to dietary recommendations, that is consuming <1 serve fruit/d, fast food ≥2 times/week, processed meat ≥2 times/week and soft drinks >0·5 cups/d to determine odds of children to consume specific food groups based on comparable socio-demographic factor denominations, for example in older v. younger mothers. Dependent variables were child’s dietary intake and independent variables were covariate maternal factors such as maternal age, maternal education, household income <Australian $ (A$)40 000/annum, etc. Models were adjusted for confounding variables child’s sex, maternal age, maternal education, household income, mother’s country of birth, marital status, mother’s BMI at baseline, breast-feeding duration and number of children in the family.
Results
Mothers’ characteristics
Mothers’ age ranged from ≥16 to ≤47 years with a mean age 26 years (sd 6 months). Mothers’ characteristics are described in Table 1. Most were married or living with a partner, about a quarter had completed tertiary education and had a household income before tax of <A$40 000/annum. Almost half were classified as either overweight or obese based on BMI calculated from self-reported height and weight. Among the children included in this study (n 243), 54 % were girls, with an overall mean age of 2·0 years (sd 1 month).
Table 1 Characteristics of the 243 mothers in the Healthy Beginnings Trial (HBT) control group at children age 2 years (Numbers and percentages)
HSC, Higher School Certificate; TAFE, Technical and Further Education; A$, Australian dollars.
Consumption patterns of children
Most children (92 %) were reported to consume the AGHE( 19 ) recommendations of one serve fruit per d but only 20 % reported consuming the recommended 2·5 serves of vegetables/d, with mean serves of fruit of 2·2 (sd 1·2) and vegetables 1·7 (sd 1·2) (online Supplementary Table S2). In all, 30 % were reported to consume more than one sugary drink per d and 79 % were reported to consume fast food at least once per week. More than half (55 %) were reported to consume processed meat weekly or more frequently and ate confectionery such as chocolates and lollies more than twice a week, with 16·5 % consuming confectionery daily. A total of 20 % were reported to consume salty snacks such as cheese curls, potato crisps and corn chips and 26 % consumed sweet snacks such as doughnuts, sweet/savoury biscuits, muesli bars and cakes more than twice a week.
Predictors of dietary patterns
Univariate analysis was performed on maternal factors: maternal age, education, household income, total children and mothers country of birth (Table 2). Binary logistic regression with odds ratio was used to assess children’s likelihood to consume various food groups and associations with maternal factors stated above. Lower-income mothers (<A$40 000/annum), reported that their child was almost five times more likely to consume <1 serve fruit/d (adjusted OR (AOR) 5·83; 95 % CI 1·49, 22·8) compared with higher-income mothers (>A$40 000/annum). The latter reported their child was four times more likely to consume hot chips two or more times a week AOR 4·80 (95 % CI 1·28, 18·04) compared with higher-income mothers. Younger mothers (<25 years) reported their child consumed more soft drink (>0·5 cups/d) AOR 2·93 (95 % CI 1·03, 8·35) and sugary drinks (>0·5 cups/d) AOR 2·40 (95 % CI 1·12, 5·54) compared with older mothers (≥25 years) (P<0·05). Less educated mothers (≤Technical and Further Education/Higher School Certificate) and mothers with only one child, reported their child consumed more sugary drinks (>0·5cups/d) AOR 2·13 (95% CI 1·02, 4·44) and fruit juice (>0·5cups/d) AOR 2·31 (95% CI 1·14, 4·70) compared with more educated mothers (≥university) (P<0·05) and mothers with two or more children, respectively. Non-Australian-born mothers reported their child consumed more fruit juice (>0·5 cups/d) AOR 2·04 (95 % CI 1·02, 4·05), sweet snacks AOR 1·96 (95 % CI 1·02, 3·76) and fast food (≥2 times/week) AOR 3·67 (95 % CI 1·29, 10·43) compared with Australian-born mothers. For other child dietary variables: vegetables; water, milk, fast food, salty snacks, sweet snacks, processed meat and confectionery; no particular maternal variable was found to influence these associations after adjustments for confounding factors: child’s sex, maternal age, maternal education, household income, mother’s country of birth, marital status, mother’s BMI at baseline, total children in the family and breast-feeding duration.
Table 2 Maternal factors at baseline associated with children’s dietary intakeFootnote * (Adjusted odds ratios (AOR) and 95 % confidence intervals; n 243)
A$, Australian dollars.
* Adjusted for child’s sex, mother’s country of birth, marital status, mother’s BMI, mother’s age, mother’s education, household income, breast-feeding duration and the number of siblings.
† Reference group.
Consumption patterns of mothers and associations between maternal and child dietary intake
Approximately 50 % of mothers reported meeting the recommended serves of fruit but only 7 % met the recommended serves of vegetables with mean serves of fruit 1·6 (sd 1·1) and vegetables 2·3 (sd 1·3) (see online Supplementary Table S2). In all, 25 % reported consuming more than two sugary drinks per d and 53 % reported having fast-food take away at least once a week. Similar to children, approximately 50 % of mothers reported consuming processed meat more than twice a week. When mother–child dietary intakes were compared, we observed significant positive correlations for all dietary variables except milk, with the largest association for fast foods (Pearson’s r 0·52, P<0·001 and moderate associations for water, fruit, vegetables, sugary drinks and processed meat (Pearson’s r varied from 0·27 to 0·48, P<0·001) (Fig. 1).
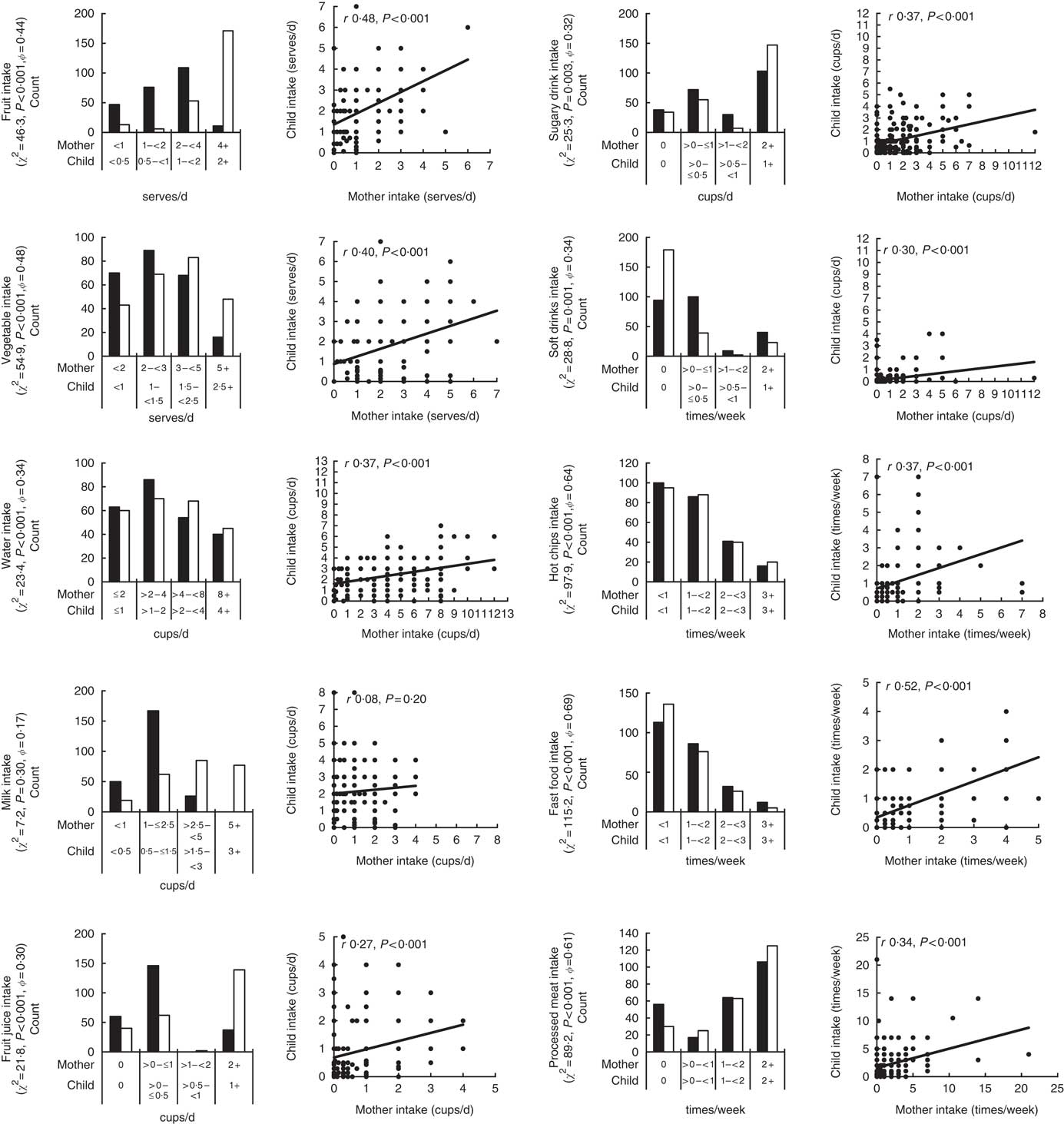
Fig. 1 Histograms and scatter plot of mother and child dietary intakes. χ 2, P value and ϕ coefficient (ϕ) values are provided on the histograms to provide a measure of agreement between the mother (■) and child (□) distributions. The Pearson’s correlation coefficient (r) and P values are provided on the scatter plots to indicate the level of association between mother and child dietary intakes.
Discussion
The present study investigated the association of maternal behaviours and socio-demographic on child eating practices. To our knowledge, this study is the first in Australia that has ascertained dietary intake among 2-year-old children of potential disadvantage (outside of the National Health Surveys), providing a descriptive view of 2-year-old children’s eating patterns and simultaneously examining maternal factors in predicting children’s diets. In our study, 2-year-old children’s dietary intakes were characterised by relatively low vegetable intake and high discretionary food intakes. This study shows that low maternal socio-economic status (SES) is associated with poor child food behaviours. Low household income (<A$ 40 000/annum), young maternal age (<25 years) and mother’s country of origin (born outside Australia) in particular seem to have the greatest association with children’s discretionary food intake.
Our study demonstrates that higher diet quality, in particular consuming recommended fruit intake, are less likely to be achieved by those with a lower household income. This has also been observed in several other studies in the preschool age group( Reference Darmon and Drewnowski 20 , Reference Pabayo, Spence and Casey 21 ). Another study reported that a two standard deviation increase in the area socioeconomic measure was associated with a 2·01-unit increase in fruit purchasing index (95 % CI 0·49, 4·50); however the corresponding associations for purchasing vegetables was lower at 0·60 (95 % CI −1·36, 2·56)( Reference Turrell, Blakely and Patterson 22 ), although these findings were not statistically significant. Studies investigating the proximity and provision of fruit and vegetable retail outlets in disadvantaged areas have found conflicting results such that living in socioeconomically disadvantaged urban areas may or may not mean fewer opportunities to purchase fruits and vegetables( Reference Winkler, Turrell and Patterson 23 , Reference Algert, Agrawal and Lewis 24 ). In our study, vegetable intake was not associated with any SES variable as most children (regardless of SES background) did not meet recommended intakes. It is hence likely that socioeconomic factors alone do not determine fruit and vegetable consumption choices, but maternal characteristics and individual choices appear to play a part.
In a recent US study, it was reported that 21 % of 1–5-year-olds eat out at least once a week( Reference Adams, Goffe and Brown 25 ). In our study at least 66 % of 2-year-olds were having fast food 1–2 times a week. Fast-food outlet density is higher in neighbourhoods of greater disadvantage with a study in Melbourne, Australia finding that people living in areas of more socioeconomic disadvantage were 2·5 times more likely to be exposed to fast food outlets than those in the suburbs with less socio disadvantage( Reference Reidpath, Burns and Garrard 26 ). In our study, lower-income mothers and mothers born outside Australia were almost 4–5 times more likely to have a child that consumed hot chips and fast food twice a week or more (P=0·02).
In this study sample, 8 % of 2-year-old children reportedly consumed more than one cup of soft drink per d, whereas 22 % of mothers consumed more than two soft drinks per d. However when fruit juice was included, providing an estimate of total sugary drink consumption, 74 % of 2-year-olds consumed more than one cup per d, whereas 60 % of mothers consumed more than two cups of sugary drinks per d. An earlier study among 2–3-year-old children reported that children who consumed one to two sugary drinks per d were two times more likely to remain overweight compared with children who consumed these less frequently( Reference Welsh, Cogswell and Rogers 27 ). In our study, young maternal age (<25 years) was a significant predictor of child soft drink intake with an almost 3-fold increased likelihood of a child drinking half a cup of soft drink per d, after adjusting for other variables. This is important to note, as eating practices in early childhood have a significant influence on longer-term eating behaviours( Reference Birch, Savage and Ventura 28 ).
Our study showed that mother–child intakes of most foods are highly correlated. Similarly, research on children’s intake of fruit and vegetables has shown positive relationships with parents’ intake of fruit and vegetables( Reference Wardle, Carnell and Cooke 29 ), and parents’ modelling of healthful dietary behaviours has been associated with low-fat eating patterns and lower dietary fat intake amongst children( Reference Tibbs, Haire-Joshu and Schechtman 30 ).
There are however several weaknesses in this present study. First, generalisability to whole diet intakes is limited as our questions were based on a sFFQ, hence several food groups were omitted such as wholegrain breads and cereals and a number of the questions were based on frequency of consumption rather than quantity. The sFFQ is limited in its ability to estimate absolute quantities of food in the diet. A previous validity study of the sFFQ has reported a tendency to over-report some foods, such as fruit and vegetables, and under-report other foods, such as biscuits and cakes( Reference Flood, Wen and Hardy 16 ). In addition, some questions may not provide a good indicator of mother’s dietary intake such as the milk question, where adults are likely to consume milk in hot beverages or breakfast cereals, rather than glasses of milk. Also relying on mothers to self-report their weight, height and dietary data of their children may be subject to some degree of mis-reporting. When determining predictors of child diet, we observed the confidence intervals were very wide. This could be due to our small sample size. To be more confident on the impact of maternal predictors in relation to child dietary practices, it would be prudent that any conclusions drawn from this study be replicated with a larger sample to confirm its veracity.
Conclusions
This study population comprises mothers and their children from socially and economically disadvantaged areas in Sydney, Australia. Our findings suggest that low maternal SES, in particular, lower maternal age (<25 years), low household income (<A$40 000/annum), and maternal country of origin (born outside Australia) are significant predictors of poor child diet quality. Most mother and child dietary behaviours are also highly correlated. Implications of this research suggest that as maternal factors are associated with child dietary behaviours and young children have similar dietary behaviours to their mothers, targeting young mothers (<25 years) of potential disadvantage before commencement of early feeding practices has the potential to improve children’s diets.
Acknowledgements
The study was funded by the Australian National Health and Medical Research Council (ID no. 393112).
The authors contributions are as follows: K. K. wrote the manuscript and analysed the data. K. K., M. H. and V. M. F. planned this study analyses. All authors contributed to the data interpretations and provided comments to drafts of the manuscript. L. M. W. was the principal investigator of the HBT and contributed to the study design and data collection. All authors read and approved the final version of the manuscript.
The authors declare that there are no financial or personal conflicts of interest.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114517003750





