



Humans are equipped with a highly sophisticated energy regulation system that provides signals about when to start and stop eating(Reference Broberger1,Reference De Graaf, Blom and Smeets2) . Although several environmental, genetic and developmental factors pose challenges to our everyday efforts to regulate eating(Reference Bilman, Van Kleef and Van Trijp3–Reference Birch, McPhee and Shoba5), some people do relatively well in listening to and acting upon these internal bodily signals in a confident, relaxed and enjoyable way.
Prior research has shown that the tendency to eat in response to physiological signals of hunger and satiation (i.e. internally regulated eating style) associates with lower BMI (small to medium effect sizes have been reported(Reference Keirns and Hawkins6,Reference Moy, Petrie and Dockendorff7) ), better psychological outcomes (e.g. higher body appreciation, self-esteem, emotional awareness, life satisfaction, psychological flexibility; lower depression, anxiety, perfectionism, dichotomous thinking, preoccupation with food) and better behavioural outcomes (e.g. lower restrained, emotional and external eating, unhealthy weight-loss practices, eating disorder symptomatology; higher eating self-efficacy, proactive coping, autonomy)(Reference Van Dyke and Drinkwater8–Reference Linardon and Mitchell14). Evidence from intervention studies further corroborates these positive findings(Reference Van Dyke and Drinkwater8,Reference Warren, Smith and Ashwell10,Reference Clifford, Ozier and Bundros15–Reference Schnepper, Richard and Wilhelm23) , although with respect to weight it seems that internally regulated eating mainly results in weight maintenance and to a lesser extent in weight loss (small effect sizes have been reported(Reference O’Reilly, Cook and Spruijt-Metz24)). The impact on energy intake, dietary quality and other physical indicators of health (e.g. blood pressure, lipids and glucose) is less clear, although improvements have also been documented in those domains(Reference Van Dyke and Drinkwater8,Reference Clifford, Ozier and Bundros15,Reference Schaefer and Magnuson16,Reference Goode, Kalarchian and Craighead21,Reference Ciampolini, Lovell-Smith and Bianchi25–Reference Greene, White and Hoerr31) .
Although we are still far from making firm conclusions about the effects of this eating style, this body of evidence suggests that it can have beneficial effects. Internally regulated eating style has received considerable attention in the literature but in a highly fragmented manner, as many research groups have tried to conceptualise this eating style from their own theoretical lenses. Concepts such as intuitive eating, eating competence, mindful eating, etc. have emerged in the literature and practice, which all refer to eating styles that are driven by internal hunger and satiation cues. For example, Tribole & Resch(Reference Tribole and Resch32) originally defined intuitive eating as the type of eating that is based on physiological cues of hunger and satiety rather than on emotional or external cues. They positioned intuitive eating as an eating style with a strong anti-diet mentality; connection with and responsiveness to internal signals of hunger, fullness and food selection; relaxed relationship with food; non-responsiveness to emotional hunger; body appreciation and appreciation of the food’s sensory qualities. Tylka and colleagues(Reference Tylka33,Reference Tylka and Kroon Van Diest34) brought the concept of intuitive eating forward by describing and measuring some key elements: unconditional permission to eat, eating for physical rather than emotional reasons, reliance on internal hunger and satiety cues and body-food choice congruence (the extent to which individuals match their food choices with their bodies’ needs).
Eating competence also falls within the boundaries of internally regulated eating. Eating competence is defined as being ‘positive, comfortable, and flexible with eating and matter-of-fact and reliable about getting enough to eat of enjoyable and nourishing food’(Reference Satter35). Individuals who score high on the eating competence self-report measure are those who have positive attitudes about food and eating, experiment with new food and learn to accept it, respond to internal signals of hunger and satiety and have good meal planning skills. Eating competence is built on two main pillars: permission (choosing and eating food that is liked in adequate amounts to satisfy hunger) and discipline (eating family-style meals at predictable times). Thus, it differs from intuitive eating in that it focuses more on responsiveness to satiation signals for meal termination and to a lesser extent on responsiveness to hunger signals for meal initiation. In fact, those who practice eating competence learn to tolerate hunger at reasonable levels to adhere to the social structure of meals and snacks.
A third prominent and increasingly studied concept related to internal regulation of eating is mindful eating. Mindful eating is based on the application of mindfulness techniques to regulate eating. The conceptual foundation for mindful eating was provided by a group of researchers who developed a treatment for binge eating disorder; Mindful-Based Eating Awareness Training(Reference Kristeller, Baer, Quillian-Wolever and Baer36,Reference Kristeller and Hallett37) . Based on this conceptualisation, cultivation of mindful eating incorporates bringing attention to the eating experience in a non-judgmental manner, savouring the food and appreciating its sensory qualities, being aware of hunger and satiety sensations and making food choices based on both liking and health(Reference Kristeller and Wolever38).
Finally, several intervention programmes promote internally regulated eating but do not fall under the three main research streams mentioned above. For example, Appetite Awareness Training(Reference Allen and Craighead20) aims to re-establish and enhance sensitivity and responsiveness to internal signals of hunger and satiety and to overcome self-perpetuating maladaptive cycles of overeating that result from dietary restraint, emotional and other situational cues. An extension of this programme also involves the reduction of reactivity to food cues that predict food intake(Reference Boutelle, Knatz and Carlson39). There is also a sensory-based nutrition intervention that, next to promoting eating in response to internal hunger and satiety cues, aims to build a non-restrictive relationship with food and to amplify, with sensory education, the pleasure that is associated with eating(Reference Gravel, Deslauriers and Watiez40).
As can be seen, the concept of internally regulated eating has gone into many directions and described by different terminologies, while limited efforts have been made to see this literature from a panoramic perspective(Reference Kerin, Webb and Zimmer-Gembeck41,Reference Winkens, van Strien and Barrada42) . Therefore, it is still not clear which are the key characteristics that enable individuals to stick to this internal, body-based eating style. While each of the previous attempts to understand the internally regulated eating style has shed light only on parts of the total picture, analysing them together at a more integrated level would do more justice to the full complexity of the concept.
In this paper, we synthesise the full breadth of characteristics that are necessary for the internally regulated eating style, we provide definitions for these characteristics, and we specify hypotheses about how they relate to each other and how they contribute to this eating style. We focus on individual-difference characteristics that form a general tendency (eating style) and not on particular behaviours that manifest as a result of this tendency. This is important because eating behaviours vary substantially depending on situational factors, while the dominant eating style of individuals is more stable over time and predictive of the broader pattern of someone’s eating behaviour(Reference Ajzen43). Thus, we position internally regulated eating style as a general tendency that is underpinned by five individual-difference characteristics, namely, sensitivity to physiological signals of hunger and satiation, self-efficacy in using physiological signals of hunger and satiation to determine when and how much to eat, trust on the body’s physiological processes for the regulation of eating and the tendencies towards food legalisation and food enjoyment. We believe it is necessary to understand the trait-like characteristics that work as preconditions for the internally regulated eating style and the mechanisms by which these characteristics support individuals in maintaining this eating style.
In achieving the aims above, we make the following scientific contributions: first, we contribute to the integration of a rather fragmented literature; second, we introduce a common language to the field by providing definitions for the full breadth of characteristics that define the internally regulated eating style and, third, we build a theoretical framework that does justice not only to the full spectrum of characteristics of the internally regulated eating style but also to the associations between them. This is important because concepts in this domain have not always been properly defined, and limited efforts have been made to hypothesise and justify the potential associations between them. This work highlights the characteristics that individuals should maintain or improve to be able to adhere to this eating style, and at the same time the areas that should be addressed by health professionals in order to promote this eating style among their clients. The theoretical framework presented here can be used to develop comprehensive measures of internally regulated eating style and to design lifestyle interventions for the promotion of physical and psychological health.
What is internally regulated eating?
Hormonal, neural and mechanical signals that are coordinated through the brain are translated into subjective sensations of hunger and satiation that signal when to start and stop eating. Hunger and satiation become noticeable not only with visceral sensations in the abdominal area (e.g. hollow sensation, growling sounds, gastric contractions and gastric distension) but also with more generalised physical (e.g. fatigue, weakness and discomfort), affective (e.g. desire to eat, decline in pleasantness or reward value of the food) and cognitive changes (e.g. lack of concentration, thoughts about food and lack of interest in food)(Reference Murray and Vickers44). These components can act synergistically to form an integrated feeling of hunger or satiation, respectively, but they can also influence our behaviour on their own. For example, patients whose stomach has been removed still report feeling hungry or full despite the lack of visceral cues(Reference Kamiji, Troncon and Suen45). Similarly, individuals may experience visceral symptoms of hunger without a desire to eat at that specific moment due to stress, negative emotions or because they are busy(Reference Murray and Vickers44).
Visceral and broader physical (bodily) sensations of hunger and satiation are particularly relevant for internally regulated eating. Individuals who regulate their eating internally determine when and how much they eat based on sensations of this kind, that is, they initiate eating when they experience moderate bodily signs of hunger and cease eating upon experience of moderate bodily signs of satiation(Reference Tanco, Linden and Earle19,Reference Tribole and Resch32,Reference Carrier, Steinhardt and Bowman46–Reference Omichinski and Harrison51) . This narrower control of eating prevents individuals from experiencing extreme states of hunger and fullness. Affective or cognitive signals can of course co-occur with physical ones when initiating or ending a meal; however, responding to the former in the absence of the latter is not compatible with internally regulated eating. It can be argued that sometimes it is difficult to distinguish physical from affective or cognitive signals. For example, palatable foods can impact appetite control and increase the sensation of hunger(Reference Erlanson-Albertsson52). However, it is important to consider that hunger is commonly measured with self-reports that capture a rather integrated feeling of hunger (e.g. how hungry do you feel at the moment?)(Reference Blundell, De Graaf and Hulshof53) rather than its physical component per se. Therefore, it remains a possibility that physical hunger is distinguishable from non-physical forms of hunger if it is explicitly evaluated. In the rest of the paper, we use the terms ‘internal’ or ‘physiological cues/signals’ to refer to the physical component (bodily sensations) of hunger and satiation.
Which are the key components of the internally regulated eating style?
The ability to sense/perceive and interpret the signals that the body generates in response to hunger and satiation is a central characteristic of the internally regulated eating style. Existing conceptualisations of internally regulated eating refer to this as ‘the ability to clearly recognise the physical signs of hunger, satisfaction, and fullness’(Reference Hawks, Merrill and Madanat54), ‘differentiation of physiological (stomach) hunger and psychological (mouth) hunger signals’(Reference Higgins and Gray50), ‘sensitivity to hunger and satiety cues’(Reference Boutelle, Knatz and Carlson39) and ‘bringing awareness to sensations of physical hunger and different types of satiety (stomach fullness and sensory-specific satiety)’(Reference Kristeller and Wolever38). We use the term sensitivity to physiological signals of hunger and satiation to refer to this competence.
In turn, individuals also need to be able to use physiological signals of hunger and satiation to decide when and how much to eat. We use the term self-efficacy in using physiological signals of hunger and satiation to refer to the perception of ease (or difficulty) in using internal signals of hunger and satiation to decide when and how much to eat. While previous research has focused heavily on the concept of responsiveness to internal signals of hunger and satiation, which is a behavioural characteristic (e.g. ‘responding to the internal regulators of hunger, appetite, and fullness’(Reference Satter35), ‘heightened responsitivity to internal cues, both hunger and satiety’(Reference Craighead and Allen48), readiness to eat in response to internal physiological hunger signals(Reference Tylka33)), we position self-efficacy as the individual-difference characteristic that is determinative for responsiveness.
Furthermore, individuals also need to have a sense of trust that the body can manage the regulation of eating itself without the need for external or cognitive control. This attitude supports individuals in resorting their eating decisions to their internal feedback. We use the term internal trust to refer to this attitude, which is in line with previous references to this characteristic (e.g. ‘trust these signals to guide their eating behaviour’(Reference Tylka33), ‘trust in their internal hunger and satiety cues and reliance on these cues to guide their eating behavior’(Reference Tylka and Kroon Van Diest34), ‘Relaxed self-trust about managing food and eating’(Reference Satter35), ‘self-reliance in the development of a nondieting lifestyle’(Reference Omichinski and Harrison51), ‘rely on signals of hunger and satiety from their own bodies’(Reference Tanco, Linden and Earle19)) (Self-efficacy and internal trust may look similar to each other; nevertheless, the two are conceptually distinct. Self-efficacy can be conceptualised as a competence (i.e. how easy it is for someone to use internal signals of hunger and satiation to decide when and how much to eat), while internal trust is an attitudinal characteristic (i.e. to what extent someone trusts his/her body to guide his/her eating)).
Another important feature of the internally regulated eating style is to have a relaxed relationship with food and particularly a relaxed attitude towards indulgent food. We use the term food legalising to refer to this attitude, a term that has also been used by other authors in the field (e.g. ‘“legalising” of all foods’(Reference Higgins and Gray50), ‘All food is legalized’(Reference Omichinski and Harrison51)). Food legalising has been conceptualised in various ways in previous research. For example, some refer to it as ‘there are no taboo foods or restrictions on eating’(Reference Hawks, Merrill and Madanat54), ‘refusal to label certain foods as forbidden’(Reference Tylka33) and ‘be “given permission” to eat previously forbidden foods’(Reference Tanco, Linden and Earle19), while others use more general terms such as ‘being comfortable with food behaviors’(Reference Satter35) and ‘spontaneity and the enjoyment of food without anxiety, guilt or concerns about compulsive or “out-of-control” eating’(Reference Higgins and Gray50).
The last characteristic that completes the profile of those who have the tendency to regulate their eating internally is the tendency to derive pleasure from eating by appreciating the sensory qualities of the food that is consumed. We use the term food enjoyment to refer to this characteristic, which has also been part of existing conceptualisations of internally regulated eating and has been referred to as ‘savoring and enjoying food’(Reference Kristeller and Wolever38), ‘Being able to pay attention to food and self during the process of eating’(Reference Satter35), ‘Identification of tastes in a variety of foods’(Reference Gravel, Deslauriers and Watiez40) and ‘looking at the food, holding the food, smelling the food’(Reference Boutelle, Knatz and Carlson39). An overview of the key characteristics of the internally regulated eating style can be found in Table 1.
Table 1. Key individual-difference characteristics of internally regulated eating style

Overall, we argue that some individuals are more sensitive, self-efficient, confident, relaxed and appreciative compared with others, but the intensity of these features can also vary within individuals depending on life changes and special circumstances. In the following sections, we discuss existing evidence on these characteristics, we explain why all are necessary conditions for the internally regulated eating style and we theorise about how they relate to each other and how they contribute to internally regulated eating style, providing supportive evidence when available.
Sensitivity to physiological signals of hunger and satiation
Individuals differ substantially in the sensations they experience when they are fed or fasted. While most people report gastric sensations before and after meals, some fail to do so(Reference Friedman, Ulrich and Mattes55–Reference Monello and Mayer57). Individual differences are also observed in the ability to detect visceral sensations associated with hunger and satiation, in how pleasant/unpleasant people find such sensations and in how they respond to changes in their visceral states. For example, Whitehead & Drescher(Reference Whitehead and Drescher58) measured sensitivity to stomach contractions in twenty healthy individuals and found that half of them displayed perceptual accuracy significantly better than chance. Besides, individuals who reported feeling both abdominal tension and abdominal sounds performed better in the visceral perception task compared with those who reported only one or none of these symptoms. Sepple & Read(Reference Sepple and Read59) found that seven out of ten healthy males had <20 % of a standardised meal in their stomach when self-reported hunger started to increase, while the rest started feeling hungry with fuller stomachs. This indicates between-individual variability in the hunger threshold. Similarly, Stephan et al.(Reference Stephan, Pardo and Faris60) showed that healthy, normal-weight individuals whose stomach was distended with a water-inflated gastric balloon reached the same subjective sensation of fullness with volumes ranging between 300 and 1175 ml. Comparable variability was reported by Van Dyck et al.(Reference Van Dyck, Vögele and Blechert61) who employed a water load task, instead of the classic barostat procedures, to assess the satiation threshold of individuals. Thus, some individuals are able to perceive subtle changes in their internal states of hunger and satiation faster than individuals who are less perceptive of their inner experiences.
Some scholars have expressed the view that increasing awareness of internal cues of hunger and satiation may pose a challenge to food intake regulation and lead to overconsumption because individuals may be unable to distinguish between homoeostatic (i.e. related to energy depletion) and hedonic (i.e. related to food cues) drivers of eating(Reference Martin, Espel-Huynh and Marando-Blanck62). This is supported by evidence showing that the homoeostatic system of energy regulation can be easily overridden by hedonic cues in the food and eating environment(Reference Lee and Dixon63). Nevertheless, there is an increasing body of evidence from experimental and intervention studies that indicates that increased attention to internal bodily sensations, while eating leads to reduced consumption of snacks(Reference Jordan, Wang and Donatoni64,Reference Marchiori and Papies65) and better compensation for previous consumption(Reference Van De Veer, Van Herpen and Van Trijp66). Ciampolini and colleagues have shown that training individuals to link their subjective feeling of hunger to an objective marker (blood glucose levels), with the purpose of re-learning to identify physical hunger and responding to it, leads to positive outcomes (e.g. reduced premeal blood glucose, insulin sensitivity, blood glucose peaks, energy intake and body weight)(Reference Ciampolini, Lovell-Smith and Bianchi25,Reference Ciampolini, Lovell-Smith and Sifone26,Reference Ciampolini and Bianchi67) . Furthermore, obese individuals and those with eating disorders (e.g. bulimia, binge eating disorder) show a reduced ability to detect hunger and satiation signals as indicated by the fact that their hunger and fullness ratings are not consistent with changes in the size of preloads they consume in laboratory experiments(Reference Craighead and Allen48,Reference Hadigan, Walsh and Devlin68,Reference Sysko, Devlin and Walsh69) . Results from neuroimaging studies also show a negative association between BMI and brain activity relevant for perception of mechanical distention in the stomach, suggesting that obesity associates with insensitivity to satiation signals(Reference Wang, Tomasi and Backus70). Evidence from the interoception literature further confirms that obesity and eating disorders are characterised by significant interoceptive deficits(Reference Jenkinson, Taylor and Laws71–Reference Klabunde, Collado and Bohon73). Taken together, the above evidence suggests that sensitivity to internal hunger and satiation signals, which can be seen as a domain-specific type of interoception (i.e. the ability to perceive/sense changes in the internal state of the body), is an adaptive competence that associates with improved health outcomes.
Self-efficacy in using physiological signals of hunger and satiation
Based on the theory of planned behaviour, self-efficacy (i.e. perceived behavioural control) is an important determinant of intention to perform a behaviour and of behaviour per se (Reference Ajzen74). Self-efficacy in the eating domain has mainly been studied from the perspective of perceived competence with losing weight or sticking to dieting goals(Reference Clark, Abrams and Niaura75,Reference Glynn and Ruderman76) , and several studies have confirmed that eating self-efficacy is a reliable predictor of weight loss behaviour(77). To our knowledge, self-efficacy in using internal signals of hunger and satiation has not been studied in the existing literature. Extrapolating the above evidence, we suggest that if individuals find it is easy to rely on their internal signals to self-regulate their eating, they are more likely to do so. Some preliminary evidence suggests that higher eating self-efficacy is associated with higher scores on intuitive eating(Reference Young78), and self-efficacy has been found to be a predictor of non-dieting behaviour(Reference Leske, Strodl and Hou79). Furthermore, we expect that there are individual differences in how easy it is for people to start eating only when feeling physically hungry and to stop eating when feeling comfortably satiated. The individual differences that have been documented for behavioural tendencies such as disinhibited eating(Reference Stunkard and Messick80) or eating in the absence of hunger(Reference Tanofsky-Kraff, Ranzenhofer and Yanovski81) suggest that some people tend to chronically override their hunger and satiation signals, while others manage not to do so.
Several pieces of evidence indicate that coupling eating with internal signals of hunger and satiation has positive effects on food intake regulation and weight outcomes. Individuals who said their habitual eating was not related to hunger or fullness sensations scored higher on disinhibited eating and showed lower meal-induced changes in hunger/fullness sensations after consumption of fixed meals in the laboratory compared with individuals whose eating was habitually related to hunger and fullness sensations(Reference Barkeling, King and Näslund82). Similar evidence has been documented for children. In a laboratory study with pre-schoolers, it was found that only children who were prompted to eat based on internal cues of hunger and satiety managed to respond to the energy density cues of preloads and to compensate for prior intake, while children who were prompted to eat according to schedule and to clean their plates to receive rewards did not show evidence of energy compensation(Reference Birch, McPhee and Shoba5). Finally, the literature on appetitive traits that associate with weight has identified satiety responsiveness as a food avoidance appetitive trait, which associates inversely with energy intake and BMI(Reference Carnell and Wardle83).
Internal trust
To regulate eating internally, individuals need to have a sense of trust on the body’s physiological processes for eating regulation. This trust should underlie both decisions about starting eating (i.e. trusting that the body has physiological processes to self-regulate the initiation of eating to avoid the aversive state of hunger) and stopping eating (i.e. trusting that the body has physiological processes to self-regulate the cessation of eating to avoid the aversive state of fullness). We call this tendency ‘internal trust’ because the individual has to shift the focus internally and trust that the body can manage the regulation of eating itself, without the need for cognitive or external rules (In some cases, using cognitive or external control over eating may be an attempt to compensate for pre-existing deficits in perception of hunger and satiation(Reference Klabunde, Collado and Bohon73). In these cases, external or cognitive control may help individuals to regulate their eating.).
Individuals who reported trusting their bodies to tell them how much to eat were less likely to engage in unhealthy and extreme weight control behaviours (e.g. skipping meals and inducing vomiting) as measured with self-reports in a cross-sectional study with 2287 adults(Reference Denny, Loth and Eisenberg84). Furthermore, reliance on internal cues to drive eating associates negatively with eating disorder symptomatology, body shame, poor interoceptive awareness and BMI, while positive associations have been documented with measures of psychological health such as satisfaction with life, self-esteem, optimism and body appreciation(Reference Tylka33,Reference Tylka and Kroon Van Diest34,Reference Madden, Leong and Gray85) . More general, body trust, an important dimension of interoceptive awareness, associates positively with measures of body awareness and negatively with measures of anxiety, body dissociation and difficulties with emotional regulation(Reference Mehling, Price and Daubenmier86). Taken together, these results provide support for the adaptive nature of a self-trusting attitude not only in the domain of eating but also in more general terms.
Food legalising
Due to our innate preference for sweet and energy-dense foods that is evolutionary advantageous in periods of food scarcity, it is difficult for many individuals to resist highly palatable foods that are easily encountered in modern societies(Reference Lowe87). In fact, the heightened responsiveness to hedonic cues is recognised as an important contributing factor to obesity(Reference Lowe and Butryn88). Consequently, several scholars and health practitioners promote the idea of cognitive self-control as a means of managing cravings for palatable food and maintaining a balanced and healthy diet. For example, it has been found that focusing on the long-term health outcomes of unhealthy eating associates with inhibition of reward activity in the brain(Reference Hare, Malmaud and Rangel89). Cognitive self-control is effective for some individuals(Reference Wing and Hill90). Nevertheless, for other individuals, it is ineffective and may even have adverse effects. For example, it has been shown that the attempt to stick to restrictive intake norms (i.e. imposed rules governing eating behaviour) can have a counter-regulatory effect by ultimately leading to overconsumption(Reference Herman and Polivy91–Reference Birch, Fisher and Davison93). This effect – also called Abstinence Violation Effect(Reference Curry, Marlatt and Gordon94) – has been documented in studies with restrained eaters(Reference Woody, Costanzo and Liefer92,Reference Herman and Mack95) and is attributed to the feeling that the diet has been violated due to either the energy content of the food that breaks the diet or to the mere consumption of a forbidden food. However, similar effects have been observed also among other population groups. Mann & Ward(Reference Mann and Ward96) have shown that prohibiting the consumption of a food, making it look like a ‘forbidden fruit’, leads to stronger desires for that food among college students. Similarly, Raynor & Epstein(Reference Raynor and Epstein97) found that short-term food deprivation increases the reinforcing value of food among non-restrained female adults. This response pattern can be explained not only by the reactance theory, which suggests that individuals react negatively (i.e. they desire the forbidden fruit) when they feel their freedom is constrained in some way(Reference Brehm98), but also by the commodity theory, which poses that decreasing the availability of a stimulus increases its perceived value(Reference Brock, Greenwald, Brock and Ostrom99).
To prevent individuals from exerting maladaptive coping strategies as a means of compensating for indulgent consumption, internally regulated eating paradigms take to a small or larger extent a libertarian stand to food. All foods, healthy or unhealthy, are allowed, and there are no taboo foods to be avoided. In addition, indulgent consumption is treated as an overwhelming experience filled with satisfaction rather than as a regretful situation followed by guilt(Reference Tribole and Resch32). This relaxed attitude is assumed to represent a more balanced and healthy relationship with food and eating. An unrestrained relationship with food may seem counterintuitive, considering that palatable foods activate the reward system and prolong consumption through a delay in the experience of satiety(Reference Erlanson-Albertsson52). However, there is evidence that this dédiabolisation of unhealthy or indulgent food may gradually lead to habituation with these foods, that is, decrease in behavioural and physiological responses after repeated exposure to the same food(Reference Epstein, Carr and Cavanaugh100,Reference Epstein, Temple and Roemmich101) . Through this process, even palatable foods do not seem so exciting or tempting after a while because the individuals know that they can consume them any time they want(Reference Tribole and Resch32). Thus, legalising food may eventually lead to weaker desires for potentially tempting food. In this way, food legalising can fit within contemporary views of self-control, which posit that successful self-control may not always result from effortful inhibition of desires but can be rather attributed to effortless processes such as experiencing the temptation (e.g. to eat a palatable but unhealthy food) as less overwhelming or tempting in the first place(Reference Gillebaart and de Ridder102). For example, Hofman et al. (Reference Hofmann, Baumeister and Förster103) showed that individuals with high self-control reported weaker desires for temptations compared with individuals with low self-control.
Furthermore, it has been found that less relaxed attitudes about food and eating (e.g. eating-related guilt and preoccupation with food) and the coping behaviour that usually accompanies such attitudes (e.g. effortful monitoring of the diet) increase cognitive load and limit the amount of available cognitive resources(Reference Green, Elliman and Rogers104). This is important because disruptions in cognitive function (e.g. working memory capacity and attention) associate with problems with appetite control and weight gain(Reference Higgs and Spetter105,Reference Gunstad, Sanborn and Hawkins106) . Instead, a carefree relationship with food, in which individuals are unencumbered by food preoccupations and avoidance efforts, could actually prevent individuals from wasting cognitive resources and assist them in using the available ones to attend and respond to their internal signals of hunger and satiation.
Interventions that have been supplemented with food legalising-like components have shown improvements in attitudes about food, responsiveness to food cues in the environment (i.e. external eating), eating disorder symptoms, self-control, depression, anxiety, body shape concerns, body image, spiritual well-being, food obsessions, flexibility and variety of food choices(Reference Tanco, Linden and Earle19,Reference Higgins and Gray50,Reference Young78,Reference Richards, Crowton and Berrett107) . In addition, a correlational self-report study found that giving oneself an unconditional permission to eat whatever food one desires at any moment is associated not only with lower BMI, disordered eating, body shame and body surveillance, but also with higher self-esteem and body appreciation(Reference Tylka and Kroon Van Diest34). Finally, in the study of Kuijer & Boyce(Reference Kuijer and Boyce108), it was found that participants who associated chocolate cake with celebration (compared with those who associated it with guilt) reported higher perceived behavioural control over eating and were more successful in maintaining their weight over a period of 18 months. Thus, taking a flexible approach to eating may prove to be an important determinant of healthy eating(Reference Swan, Bouwman and Aarts109).
Food enjoyment
Today’s modern societies are characterised by busy lifestyles whereby eating may go unnoticed several times during the day. Under such circumstances, people may frequently eat quickly or distractedly and therefore not fully appreciate the sensory qualities of the food and the pleasure that accompanies the eating occasion. In more extreme instances, people who struggle with eating-related problems (e.g. anorexia) may even view food as an enemy rather than as a source of pleasure. Internally regulated eating paradigms embrace the idea of food enjoyment, as they emphasise the importance of pleasure and satisfaction in eating that can be achieved by savouring the food while attending to and appreciating its sensory qualities(Reference Tribole and Resch32,Reference Satter35,Reference Kristeller and Wolever38,Reference Gravel, Deslauriers and Watiez40,Reference Omichinski and Harrison51) .
Mindfulness-based experiments and interventions that use strategies such as present moment awareness targeted at the sensory qualities of food being consumed have reported positive consequences on food intake, cravings for highly palatable foods, eating behaviour (e.g. emotional and external eating) and psychological variables such as body appreciation(Reference Schnepper, Richard and Wilhelm23,Reference Arch, Brown and Goodman110–Reference Mason, Epel and Aschbacher114) . For example, in a series of experiments, Arch and colleagues showed that tuning into the sensory experience leads to higher enjoyment and lower energy intake of unhealthy foods(Reference Arch, Brown and Goodman110). In contrast, eating under distraction (e.g. while watching television) consistently leads to higher energy intake in the same but also in subsequent meals(Reference Robinson, Kersbergen and Higgs113). Furthermore, self-reported eating with awareness has been associated with lower BMI(Reference Framson, Kristal and Schenk115). Various mechanisms have been proposed to explain the effects of focused attention to the food while eating on food intake, including the enhanced impression of the eating episode in episodic memory, the reduction in eating automaticity or the prioritisation of sensory-specific satiation (i.e. decline in pleasure we obtain from eating a particular food as we eat) over physical satiation(Reference Tapper116). The focus on sensory stimulation as a means of deriving pleasure from eating seems to be crucial for the positive effects mentioned above, since food enjoyment independent of sensory amplification, as captured, for example, by the enjoyment of food subscale of the Adult Eating Behaviour Questionnaire, is identified as a food-approach trait that associates positively with energy intake(Reference Carnell and Wardle83).
A theoretical framework of internally regulated eating style
When individuals lack either sensitivity to or self-efficacy in using internal signals of hunger and satiation, they cannot engage in internally regulated eating. These are core competences that are needed for the internally regulated eating style. Sensitivity is a prerequisite for self-efficacy. Sensitivity and self-efficacy are, nevertheless, distinct competences because there may be other factors that prevent highly sensitive individuals from using their bodily sensations to self-regulate their eating (e.g. time constraints, unavailability of food and limited trust on the effectiveness of these signals). In turn, self-efficacy may impact sensitivity through reciprocal interaction and feedback. For instance, a person who finds it easy to use internal signals of hunger and satiation to determine when and how much to eat may routinely engage in such behaviour and this may aid the connection with the inner experience and improve sensitivity to internal, bodily signals(Reference Gravel, Deslauriers and Watiez40,Reference Bush, Rossy and Mintz111,Reference Bacon, Stern and Van Loan117–Reference Stunkard and Fox120) .
Internal trust is another prerequisite for the internally regulated eating style because it directs attention to the body and its internal processes. If individuals do not trust their bodies’ self-regulatory abilities for eating, they may be inclined to draw their attention towards outside of the body and resort to cognitive or external rules to guide their eating behaviour. The lack of internal trust may further impact sensitivity and self-efficacy. In support to this, it has been found that body trust, a more generalised version of trust, associates negatively with body dissociation and positively with attention regulation (i.e. the ability to sustain and control attention to body sensations)(Reference Mehling, Price and Daubenmier86). Thus, lacking internal trust may be accompanied by the feeling of being dissociated from the body and the signals it produces, while heightened internal trust may shift attention towards inside the body and make individuals more attentive to changes in their internal states. The perceptual accuracy hypothesis of the self-awareness theory, which posits that self-focused attention increases the capacity to perceive bodily signals, further supports our assertion(Reference Gibbons, Carver and Scheier121). In turn, sensitivity and self-efficacy may gradually increase internal trust through positive learning mechanisms. Finally, internal trust may even have a moderating role between sensitivity and self-efficacy because the lack of internal trust could act as a barrier to responding to internal signals that an individual accurately perceives.
Food legalising is another necessary condition for the internally regulated eating style. In the absence of a relaxed attitude towards indulgent food, individuals may be inclined to impose cognitive or external control on their eating as a means of avoiding indulgent consumption or in order to compensate for it. Thus, a different eating style would emerge (e.g. restrained eating). As we discussed previously, food legalising provides a permissive environment for the effective perception and responsiveness to internal signals of hunger and satiation by saving cognitive resources that could be wasted otherwise (e.g. when having a cognitively controlled strategy to eating). In this way, food legalising supports sensitivity to and self-efficacy in using internal signals of hunger and satiation.
Finally, we suggest that food enjoyment aids individuals to stay in tune with the eating experience and the accompanied sensations, leading, thus, to a more precise regulation according to internal signals. It has been shown that sensory characteristics of the food (e.g. thickness and creaminess) interact with the food’s energy content in determining its satiating capacity(Reference Yeomans122). This is because sensory cues create expectations about the satiating capacity of the food, which prepare the appetite system for the ingested nutrients, and when such expectations are confirmed by internal feedback, there is an increase in the efficiency of nutrient processing(Reference Yeomans and Chambers123). This highlights the inter-connectedness of the sensory experience while eating with the ingestive processes that take place in the body and corroborates our argument for the important role of food enjoyment in the internally regulated eating style.
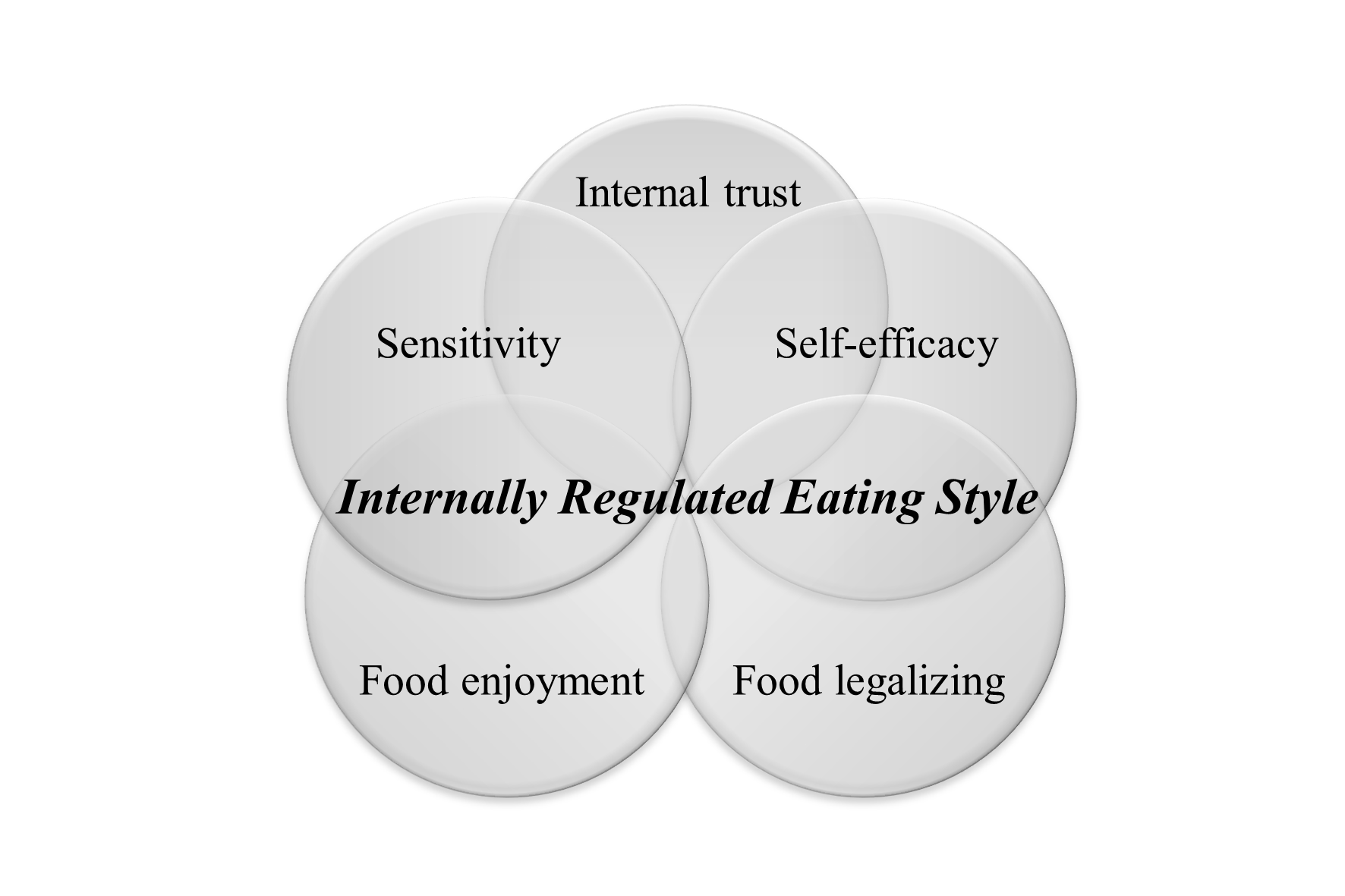
To wrap up, a set of five individual-difference characteristics work as necessary and only jointly sufficient conditions for the internally regulated eating style. We hereby propose the following inclusive definition of internally regulated eating style, which builds on earlier definitions of related constructs(Reference Tribole and Resch32,Reference Tylka33) . Internally regulated eating style is the general tendency to eat in response to physiological signals of hunger and satiation, which is underpinned by a specific set of individual-difference characteristics, namely, sensitivity to physiological signals of hunger and satiation, self-efficacy in using physiological signals of hunger and satiation to determine when and how much to eat, trust on the body’s physiological processes for the regulation of eating, and the tendencies towards food legalisation and food enjoyment (Fig. 1).
The theoretical model presented above is particularly relevant for adults, although it is consistent with models that have been developed for children such as the trust model proposed by Satter(Reference Satter124). The model is applicable for individuals who have at least some basic connection with their internal signals of hunger and satiation. Those with diminished ability to perceive such signals (e.g. individuals with eating disorders) should first be subjected to training to relearn and reconnect with their own bodily sensations. With respect to states of energy balance, the internally regulated eating style is particularly relevant for weight maintenance and prevention of further weight gain, although weight loss can also be achieved if individuals stabilise their eating behaviours at an energy intake level that is lower than their current energy needs(Reference Clifford, Ozier and Bundros15,Reference Schaefer and Magnuson16) . Thus, internally regulated eating can facilitate the prevention and to a lesser extent the treatment of obesity. Nevertheless, the stabilisation of eating behaviours and particularly the reduction of maladaptive behaviours such as eating in the absence of hunger or disinhibited eating that can be achieved with internally regulated eating(Reference Schaefer and Magnuson16,Reference Proffitt Leyva and Hill125–Reference Miller, Kristeller and Headings127) are relevant not only for obese and overweight individuals but also for those with binge eating disorder who may have normal weights. Finally, the eating pattern that emerges with internally regulated eating, that is, frequent small meals, can also be helpful for individuals with specific medical conditions such as those with gastrointestinal disturbances or diabetes(Reference Wheeler, Lawrence and Chae128).
How does internally regulated eating fit within existing theories of self-regulation and eating behaviour?
Dual-system theories that make a distinction between a rational system that requires effortful deliberation and an intuitive system that operates automatically and effortlessly have been used extensively to understand eating behaviour and self-regulation failure(Reference Loewenstein129–Reference Hofmann, Friese and Strack132). These theories take the general stance that effective regulation of eating can be achieved when individuals manage to resist short-term impulses (e.g. not eating the cake) for the sake of their long-term health goals (e.g. weight loss). Thus, they promote top-down strategies for the regulation of eating behaviour with an emphasis on cognitive control. According to these models, visceral urges (e.g. hunger, pain and pleasure) are disruptive influences for self-regulation(Reference Yang, Carmon and Kahn133).
On the other hand, emerging theories of self-regulation, such as the theory of embodied cognition, propose that all cognitive processes are fundamentally grounded in their physical context and that bodily states play an important role in cognition and decision-making(Reference Petit, Basso and Merunka134). This theory supports the notion of embodied self-regulation, namely that bodily states facilitate (instead of inhibit) self-regulation and that people should take them into account to help them achieve their long-term goals. Likewise, contemporary models of appetite control suggest that the distinction between a hedonic and a homoeostatic system of energy regulation should be abandoned and that we should focus on the inter-connectedness of metabolic, reward and cognitive processes that impact appetite regulation and food intake(Reference Higgs, Spetter and Thomas135,Reference De Araujo, Schatzker and Small136) . These models underline the important role that metabolic signals have on appetite control, either via their effects on cognitive processes such as memory, attention and learning(Reference Higgs, Spetter and Thomas135), or via neural processes that take place at an unconscious level(Reference De Araujo, Schatzker and Small136). This stream of literature sets the scene for better understanding internally regulated eating. Our hypothesised mechanisms, by which the characteristics of the internally regulated eating style facilitate cognitive processes that are important for the effective regulation of food intake (internal trust increasing attention to the body and its signals, food legalising preventing cognitive resources from being wasted, food enjoyment increasing episodic memory of meals), are in line with these models.
More specifically, we use the boundary model of eating, introduced by Herman & Polivy(Reference Herman and Polivy137), to describe how internally regulated eating leads to effective regulation of food intake. The boundary model suggests that food intake is regulated within two boundaries: one that corresponds to hunger and one to satiety (Herman & Polivy(Reference Herman and Polivy137) use the term satiety (i.e. the process that leads to the inhibition of eating between meals) in the original paper, although the term satiation (i.e. the process that leads to meal cessation) is more accurate because the satiety boundary is relevant for meal termination. In this paper, we use the original term as proposed by the authors, but we acknowledge the difference between the two processes. Furthermore, the boundary model illustrates hunger and fullness in the same continuum, which can be misinterpreted as hunger and fullness were different sides of the same process. While we want to keep with the original representation of the model, we want to clarify that we do not support this notion and we acknowledge that hunger and fullness are distinct processes, as indicated by existing literature(Reference Blundell, De Graaf and Hulshof53)). Biological pressures drive individuals to eat in order to keep within these boundaries and prevent the aversive states of hunger and fullness. The area between the boundaries is called ‘zone of biological indifference’, and this is where appetitive pressures – that is, social, cognitive and other psychological influences (food palatability, social pressures, etc.) – mainly determine food intake.
Various eating styles can be conceptualised using the boundary model of eating. For example, it has been suggested that restrained eating can force the hunger and satiety boundaries apart (wider zone of biological indifference) because the person eats in response to something other than the body’s signals (e.g. self-imposed or externally imposed eating rules) and this makes the individual gradually less sensitive to such signals(Reference Herman and Polivy137). In support to this, Koch & Pollatos(Reference Koch and Pollatos138) have shown in a prospective study with children that a diminished ability to detect bodily sensations (i.e. interoceptive deficits) is an outcome of obesity and dysfunctional eating tendencies such as external eating. This means that individuals become insensitive to internal signals if they do not use them in structuring their eating behaviours. While the hunger and satiety boundaries are still relevant for restrained eaters, they are less relevant for patient groups such as those with anorexia nervosa or binge eating disorder, as the former tend to override the hunger boundary (when engaging in extreme fasting) and the latter override the satiety boundary (when engaging in disinhibited eating). Similarly, when eating in the absence of hunger (i.e. a form of disinhibited eating), individuals override the hunger or satiety boundary (or both) as they tend to initiate eating while being in the zone of biological indifference or continue eating despite being in the aversive state of fullness(Reference Tanofsky-Kraff, Ranzenhofer and Yanovski81). Emotional eating and external eating have a similar pattern because individuals initiate eating or overeat in response to emotional and environmental cues either in the presence or absence of hunger(Reference Van Strien, Frijters and Bergers139). Thus, there are several eating styles that violate either one or both the hunger and satiety boundaries.
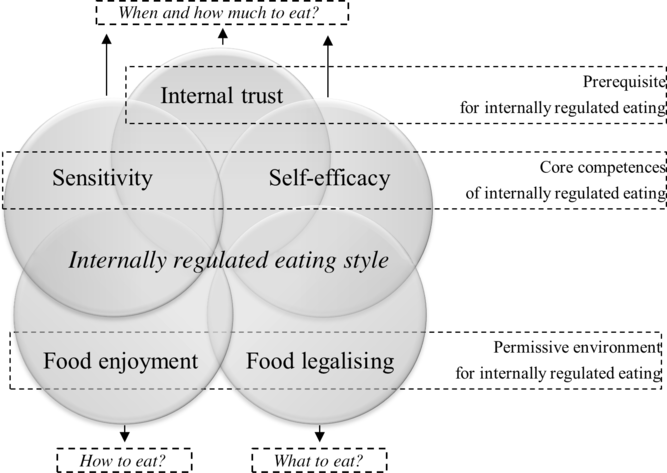
Fig. 1. Theoretical framework of internally regulated eating style. Five individual-difference characteristics comprise the internally regulated eating style. Sensitivity to physiological signals of hunger and satiation and self-efficacy in using physiological signals of hunger and satiation are core competences of internally regulated eating, food legalising and food enjoyment provide a permissive environment for listening and responding to internal signals of hunger and satiation, and internal trust is a prerequisite for engaging in this internal, body-based eating style.
In turn, we propose that internally regulated eating brings the hunger and satiety boundaries closer together (Fig. 2) because individuals who have this as their dominant eating style are inclined to initiate eating in response to early, moderate signals of hunger (the hunger boundary is displaced to the right) and to terminate meals in response to early, moderate signals of satiation (the satiety boundary is displaced to the left). In the same way that individuals lose touch with their bodily signals when they consistently ignore or override them(Reference Koch and Pollatos138), connection with those signals can become stronger if individuals consistently pay attention and respond to them(Reference Gravel, Deslauriers and Watiez40,Reference Bush, Rossy and Mintz111,Reference Bacon, Stern and Van Loan117–Reference Stunkard and Fox120) . Importantly, responding to moderate and not extreme internal signals is a critical element for the effective regulation of food intake. For example, with respect to hunger, it has been found that the longer the fasting the greater the activation of reward valuation of palatable food in the brain(Reference Stice, Burger and Yokum140), which may lead to overconsumption(Reference Stice, Yokum and Burger141,Reference Berridge142) .
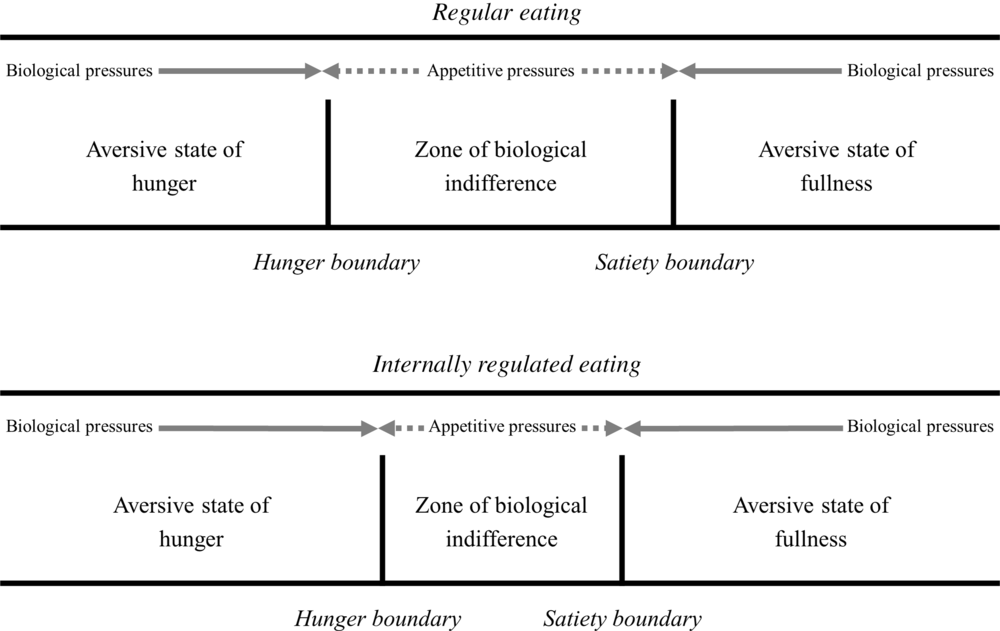
Fig. 2. The boundary model adjusted for internally regulated eating. Internally regulated eating brings the hunger and satiety boundaries closer together because the individual is more strongly inclined to initiate eating in response to early, moderate signals of hunger (the hunger boundary is displaced to the right) and to terminate meals in response to early, moderate signals of satiation (the satiety boundary is displaced to the left). This results in a narrower zone of biological indifference and, in turn, in a smaller latitude for appetitive pressures to exert their influences.
More specifically, we propose that the individual-difference characteristics we identified in this research enable individuals to maintain a narrow zone of biological indifference. Heightened sensitivity reduces the thresholds for perceiving hunger and satiation signals, which means that these can be perceived at early stages before their intensity increases. In addition, individuals with heightened self-efficacy should be able to initiate meals at early stages of hunger and terminate meals at early stages of satiation. Thus, sensitivity and self-efficacy work together in maintaining a narrow zone of biological indifference. Through attentional and other cognitive processes (discussed above), internal trust, food legalising and food enjoyment further support the maintenance of a narrow biological indifference zone, through their effects on sensitivity and self-efficacy. In this narrower control of food intake, the biological pressures that keep consumption within the two boundaries are more prominent and determinative for food consumption, leaving thus, a smaller latitude for appetitive pressures to exert their influences. This is not to say that internally regulated eaters are not susceptible to the effects of emotional or environmental factors that impact eating behaviour and food intake (e.g. negative emotions and food temptations). Such factors are challenging for everyone. Instead, we take the position that despite occasional fluctuations, those individuals are generally less responsive to such cues(Reference Warren, Smith and Ashwell10,Reference Clifford, Ozier and Bundros15–Reference Ulian, Aburad and da Silva Oliveira17) . The five individual-difference characteristics they have (particularly food legalising) support them in getting back on track after deviations.
Discussion
Internally regulated eating is a concept that has been receiving increasing attention in the literature and health practice over the last decades, but in a highly fragmented way. In this paper, we identified and delineated the key individual-difference characteristics that form the internally regulated eating style, considering streams of literature that had not been sufficiently integrated that far. Next to providing definitions and available scientific evidence for each of these characteristics, we formulated hypotheses about their inter-relationships and about the mechanisms by which they contribute to this eating style. The theoretical framework presented in this paper suggests that the internally regulated eating style leads to a more precise tuning of food intake within the states of hunger and satiation by listening and responding to moderate hunger and satiation signals in a confident, relaxed and enjoyable way. This superordinate conceptualisation of internally regulated eating style may be the starting point in finding the common ground between different streams of literature that share the main underlying concept and in facilitating the alliance of forces to promote a healthy and sustainable eating style.
In our model, a set of five individual-difference characteristics that support each other form the internally regulated eating style. Sensitivity to physiological signals of hunger and satiation is a prerequisite for self-efficacy in using such signals to determine when and how much to eat and these two competences associate positively with each other. Internal trust is also necessary because it directs attention towards inside the body and its processes, has a bi-directional relationship with sensitivity and self-efficacy and is further assumed to work as a moderator between them. Food legalising is another critical element as it provides a permissive environment for the effective perception and responsiveness to internal signals of hunger and satiation. Finally, food enjoyment completes the profile of the internally regulated eating style as it sets the scene for a more precise regulation according to internal signals. Thus, all five characteristics have their particular roles and are all necessary for the internally regulated eating style. This is a novel conceptualisation that adds to what is already known in the literature because it highlights the inter-connectedness of the internally regulated eating style characteristics.
Next to this main hypothesis regarding the inter-connectedness of the five characteristics, in this paper, we generated several hypotheses that can be tested with empirical research. For example, we hypothesised that food legalising prevents cognitive resources from being wasted and in this way provides a permissive environment that allows individuals to focus on their bodily sensations and use them in their eating-related decisions. To test this mechanism, researchers could conduct causal-chain experiments to examine how food legalising impacts the amount of available cognitive resources and, in turn, how the availability of cognitive resources impacts the perception and responsiveness to internal signals of hunger and satiation. In a similar way, it could be tested whether the effects of internal trust on perception and responsiveness to internal signals are mediated by attention processes.
The novel conceptualisation of internally regulated eating style also opens new avenues for the measurement of this eating style. Currently, there is no adequate scaling instruments to assess the characteristics we have identified in this research. The development of measures to capture these characteristics would not only improve our understanding of the concept and its correlates but will also open the field for experimentation. The use of quick and inexpensive measures of individual-difference characteristics to identify and classify individuals may work as a starting point in the study of eating behaviour, followed by a more elaborate exploration of actual behaviour (which, in turn, is more variant and not always representative of the individual’s dominant eating style). Once such instruments are available, researchers can use them to explore the interrelations between the characteristics of the internally regulated eating style and the extent to which they are predictive of health outcomes.
Finally, the main practical contribution of this paper is that it portrays the most important areas to intervene in order to promote the internally regulated eating style. Strategies like coupling subjective sensations of hunger and satiation with objective markers can be used to enhance sensitivity to and self-efficacy in using these signals to regulate food intake(Reference Ciampolini, Lovell-Smith and Bianchi25,Reference Ciampolini, Lovell-Smith and Sifone26,Reference Ciampolini and Bianchi67) . This could be done in combination with strategies aimed at increasing the awareness and reducing the responsiveness to external or emotional cues of food intake(Reference Boutelle, Knatz and Carlson39,Reference Provencher, Begin and Tremblay143) since such cues can have an important influence on food intake. Strategies that cultivate independence and self-reliance can be used to enhance internal trust, food habituation strategies, like repeated exposure to indulgent food, can be used to reduce the hedonic responses to such foods and prevent counter-regulatory behaviours that usually follow their consumption(Reference Epstein, Carr and Cavanaugh100), and mindful eating strategies like present-moment awareness during eating can be used to cultivate food enjoyment(Reference Kristeller and Wolever38).
There is abundant room for further progress in understanding internally regulated eating. Potential pathways for future research could be to investigate the psychobiological factors that influence the development and maintenance of the internally regulated eating style, to explore moderating factors that facilitate or prevent individuals in/from engaging in internally regulated eating, and to fully elucidate the long-term consequences of internally regulated eating on physical, psychological, behavioural and dietary outcomes. The current paper may provide a theoretical basis for future investigations on this topic.
Acknowledgements
The authors would like to thank the Wageningen School of Social Sciences (WASS) for funding the PhD project of A. P., within which the present research was conducted.
All authors contributed equally to the conception of the theoretical framework presented in this paper. A. P. reviewed the literature and drafted the original manuscript. E. v. K., E. d. V. and H. v. T. supervised this research. All authors reviewed the manuscript and approved its final version.
There are no conflicts of interest.



