


No CrossRef data available.
Published online by Cambridge University Press: 07 November 2024
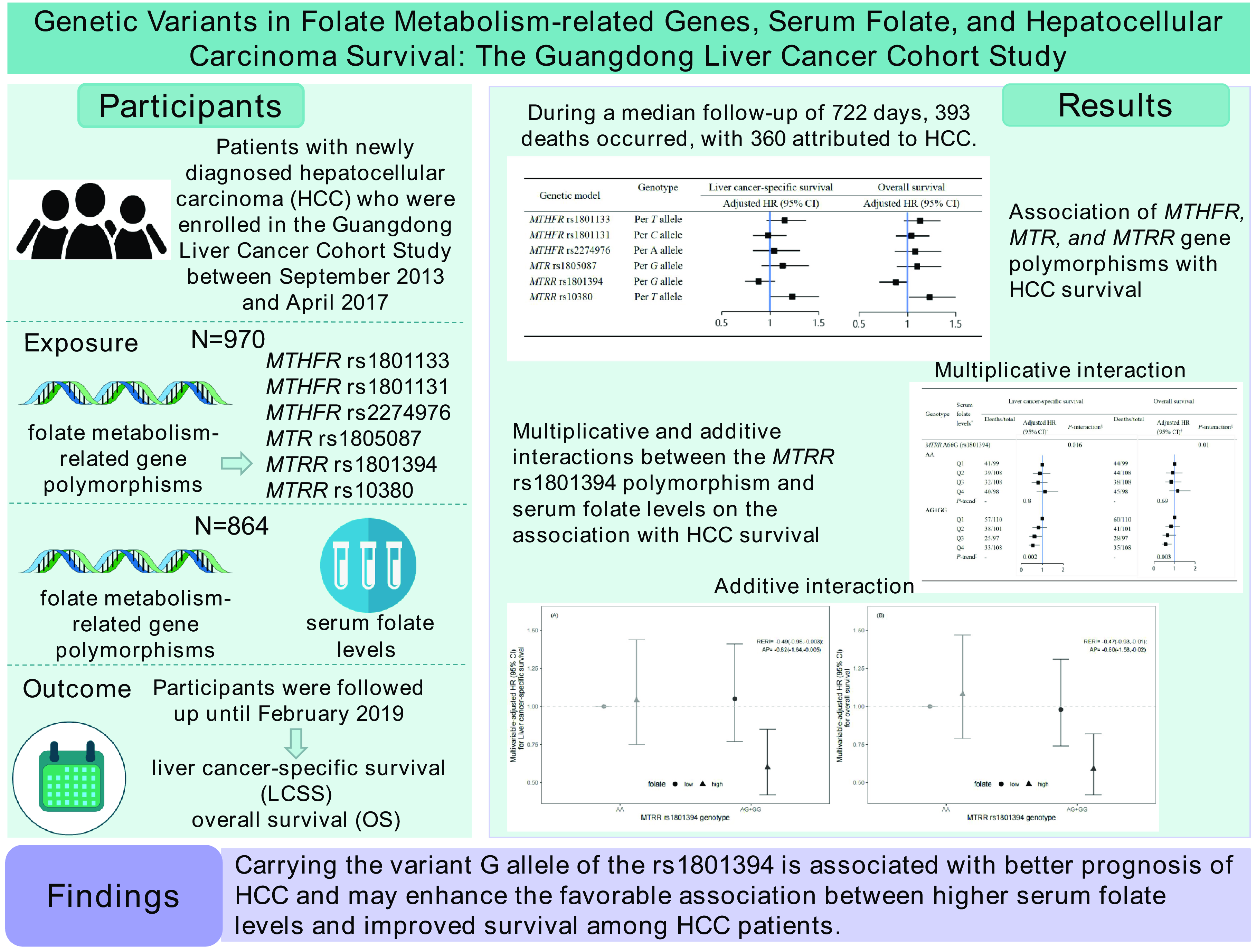
Folate metabolism is involved in the development and progression of various cancers. We investigated the association of single nucleotide polymorphisms (SNP) in folate-metabolising genes and their interactions with serum folate concentrations with overall survival (OS) and liver cancer-specific survival (LCSS) of newly diagnosed hepatocellular carcinoma (HCC) patients. We detected the genotypes of six SNP in three genes related to folate metabolism: methylenetetrahydrofolate reductase (MTHFR), 5-methyltetrahydrofolate-homocysteine methyltransferase reductase (MTRR) and 5-methyltetrahydrofolate-homocysteine methyltransferase (MTR). Cox proportional hazard models were used to calculate multivariable-adjusted hazard ratios (HR) and 95 % CI. This analysis included 970 HCC patients with genotypes of six SNP, and 864 of them had serum folate measurements. During a median follow-up of 722 d, 393 deaths occurred, with 360 attributed to HCC. In the fully-adjusted models, the MTRR rs1801394 polymorphism was significantly associated with OS in additive (per G allele: HR = 0·84, 95 % CI: 0·71, 0·99), co-dominant (AG v. AA: HR = 0·77; 95 % CI: 0·62, 0·96) and dominant (AG + GG v. AA: HR = 0·78; 95 % CI: 0·63, 0·96) models. Carrying increasing numbers of protective alleles was linked to better LCSS (HR10–12 v. 2–6 = 0·70; 95 % CI: 0·49, 1·00) and OS (HR10–12 v. 2–6 = 0·67; 95 % CI: 0·47, 0·95). Furthermore, we observed significant interactions on both multiplicative and additive scales between serum folate levels and MTRR rs1801394 polymorphism. Carrying the variant G allele of the MTRR rs1801394 is associated with better HCC prognosis and may enhance the favourable association between higher serum folate levels and improved survival among HCC patients.

