


Anaemia is one of the most frequent nutritional diseases, and it is a widespread public health problem around the world, affecting the physical growth and mental development of young children and increasing perinatal morbidity and mortality in women( Reference Gordon 1 , Reference Eden 2 ). The pathophysiology of anaemia is multifactorial, and the contribution of their causes varies by regions. The most common cause of anaemia is micronutrient deficiency, with Fe deficiency being the most frequent of all( 3 ).
In the 2010 Global Burden of Disease report( 4 ), Fe deficiency anaemia was globally ranked as the third leading cause of disability, accounting for a substantial proportion of disease burden in Mexico and the rest of the Latin American and Caribbean regions. It was estimated that anaemia was responsible for 68·3 % of years lived with disability, accounting for 8 % of all disabilities. Women and pre-school children carried the highest burden( Reference Kassebaum, Jasrasaria and Naghavi 5 ).
Anaemia in children younger than 2 years is of great interest and concern because higher Fe intake is required at this critical stage of growth, and it is often not provided by the diet. Neurobehavioural effects are of greatest concern because their effects persist for a long time after treatment with Fe and resolution of anaemia( Reference Fernald, Neufeld and Barton 6 ).
In the most recent National Health and Nutrition Survey in Mexico in 2012 (ENSANUT 2012), the prevalence of anaemia in children <5 years of age was 23·3 %( Reference De la Cruz-Góngora, Villalpando and Mundo-Rosas 7 ), whereas the prevalence of Fe-deficiency anaemia was 16 %( Reference Villalpando, De la Cruz and Shamah‐Levy 8 ). This is a concern because anaemia has been linked to lifelong cognitive, behavioural and other negative health effects in offspring( Reference Goonewardene, Shehata and Hamad 9 , Reference Walter, De Andraca and Chadud 10 ). Fe deficiency in utero appears to have direct effects on brain maturation indicators in premature infants( Reference Radlowski and Johnson 11 ).
In San Luis Potosí (SLP), one of the thirty-two states in the Mexican Republic, the prevalence of stunting in children <5 years was 10·1 % and the prevalence of anaemia was 18·0 % in 2012( 12 ). We do not have data on Fe deficiency in SLP, so we do not present them.
To address the problem of anaemia, the state of SLP and the federal government implemented two separate food assistance programmes (FAP). Prospera (previously Oportunidades) is a cash transfer programme and also distributes enriched baby food containing one RDA of Fe, Zn and other micronutrients( Reference Levy 13 ). The other FAP is rescue from malnutrition with amaranth (RMA). It was created by the SLP’s Health Ministry to achieve nutritional recovery of the childhood population in that state( 14 ). Amaranth is a cereal with high protein content (14 %) that is being promoted for the prevention of undernutrition and anaemia in children.
Household food insecurity is very high in SLP according to ENSANUT 2012; almost one-third of households experienced moderate or severe food insecurity( Reference Mundo-Rosas, Shamah-Levy and Rivera-Dommarco 15 ). Some studies on experience-based scales have shown that household food insecurity is associated with a variety of adverse health outcomes including malnutrition, physical, mental and social health, as well as dietary intake( Reference Cuevas-Nasu, Rivera-Dommarco and Shamah-Levy 16 – Reference Baig-Ansari, Rahbar and Bhutta 20 ), but little is known about the relationship between food insecurity and childhood anaemia. Measures of food insecurity based on scales commonly do not capture the broader structural determinants of food insecurity (social, economic and agricultural policies)( Reference Ghattas 21 ).
The objective of this study is to establish an indirect pathway for the association between FAP and anaemia prevalence through dietary and socio-economic (SE) conditions in beneficiary children. Results could be used to show the potential effectiveness of FAP and to improve the program strategies for reducing the prevalence of anaemia with dietary and SE conditions as an intermediary factor.
Methods
Design and sample
Data were drawn from a cross-sectional study to assess the association between FAP and the nutritional status of beneficiary children in SLP. A comparative two-stage probabilistic sample was designed. In the first stage, a sample of Primary Care Health Centers (PCHC) was selected using a probability proportional to the number of FAP beneficiaries under 5 years of age. A sample of forty-three PCHC was selected from a total of eighty-two in SLP. In the second stage, simple random samples of 420 children <5 years who were beneficiaries of Prospera and 420 beneficiaries of RMA were selected. The 374 children for the comparison group were not beneficiaries of any program and were selected from the PCHC catchment area using residence locations, ages and sexes as matching criteria in order to improve comparison between groups. The study was conducted between February and April 2014.
Description of the application of food assistance program information, complements and supplements
Prospera is a social programme developed by the Mexican government with a food aid component. It supports those families whose low-income and SE conditions do not allow them to accomplish the minimal well-being conditions such as feeding, health and education. This programme provides diverse monetary aids such as feeding support and education subsidies among others. Furthermore, the programme offers a health and nutrition component. The latter consists of a nutritional supplement named Nutrisano ( Reference Neufeld, Mejía and Fernández-Gaxiola 22 ), delivered to children between 6 and 23 months of age and to children between 2 and 4 years of age with low weight (weight-for-age <−1 sd)( Reference Neufeld, Steta and Rivera 23 ). Since 2014, Prospera began a new nutritional component including one complement and one supplement: a fortified milk drink and a single-dose sachet (such as small sugar sachets) containing microencapsulated micronutrient powder, which is easily sprinkled onto any home-prepared food (Vitaniño). The Prospera beneficiaries were provided with only one of the three supplements at monthly medical examinations, according to poverty and availability of local facilities such as clean water and sewerage of their residence area; the intrinsic nutrient content of all complement foods and supplements provided in programmes are listed in Table 1.
Table 1 Nutritional content of Prospera and rescue from malnutrition with amaranth (RMA), food complements and supplements

ER, retinol equivalents.
Mothers were encouraged to feed their children with a daily portion of the supplement, complement or milk as complementary to their regular feeding. Prospera complements came in the form of a dry mix powder offered in different flavours that required hydration before consumption. They are distributed in 240 g packages containing about five daily portions (the recommended daily portion was 44 g of powder). Mothers were instructed to add 40 ml of boiled water to one portion of powder, which produces a purée, referred to in Spanish as papilla. The powdered milk (Nutrisano milk) required hydration before consumption. Mothers were instructed to make one portion by adding 30 g of powder in 250 ml of boiled water. For Vitaniño, the recommendation was one daily supplement dose equivalent to a 1 g pack. It should be mixed with about 30 or 40 g of any household food (vegetables, fruits, beans or, mashed, ground or triturated foods).
RMA provides a nutritional complement based on amaranth called Tortimyl (which contains 4·5 mg of Fe with some additional micronutrients) to underweight children less than 5 years of age (weight-for-age −1 sd) who attended a medical consultation and were not beneficiaries of Prospera ( 14 ). In addition, the programme monitors nutritional status through weight and height measurements and a medical evaluation, monthly. Mothers of beneficiary children receive training on amaranth preparation, as well as nutritional counselling, warning signs and symptoms of malnutrition and prevention of acute respiratory and diarrhoeal diseases.
The RMA instructions indicate a daily intake of 13 g of amaranth flour added to any food (masa, milk, egg, soup, beans and so on) because it has no flavour.
Variables
Outcome variable
The main outcome variable was childhood anaemia status. Capillary Hb levels were quantified by finger-prick and analysed using portable HemoCue photometers (HemoCue Inc.). This procedure was performed by trained field personnel, and it was standardised with conventional techniques. In accordance with WHO recommendations, anaemia was defined as Hb level <110 g/l for children <5 years( 24 ) at sea level. Hb levels were adjusted for altitude using the equation published by Cohen and Hass( Reference Cohen and Haas 25 ).
Food insecurity, dietary and socio-economic measurements
Household food insecurity is defined as the lack of access to a diet of sufficient quality and quantity for a productive and healthy life( 26 ). Household food insecurity was measured in accordance with the well-validated Latin American and Caribbean Food Security Scale (ELCSA by its Spanish acronym)( 27 ). Adequate psychometric behaviour of ELCSA in ENSANUT 2012 was confirmed with Rasch modelling( Reference Villagómez-Ornelas, Hernández-López and Carrasco-Enríquez 28 ). The scale includes fifteen questions that assess poverty-related food insecurity household experiences, ranging from being worried about not having access to enough food to going without food for a whole day during the 3 months preceding the survey. Eight separate questions on the scale apply to food insecurity affecting adults and/or the household as a whole, and the remaining seven questions refer to food insecurity affecting minors (<18 years of age). The questions were answered as yes, no, don’t know or refused. An additive score based on the number of ‘yes’ responses to the ELCSA questions was then used to classify households as either food secure or into three mutually exclusive food insecurity severity categories (mild, moderate or severe food insecurity) with the use of standard cut-off scores( 27 ). For homes with individuals <18 years of age, the standard cut-off scores are ‘household food secure’ (score=0), ‘mild household food insecurity’ (score=1–5), ‘moderate household food insecurity’ (score=6–10) and ‘severe household food insecurity’ (score=11–15). For homes with individuals >18 years of age, the standard cut-off scores are ‘household food secure’ (score=0), ‘mild household food insecurity’ (score=1–3), ‘moderate household food insecurity’ (score=4–6) and ‘severe household food insecurity’ (score=7–8).
A SE index was generated using a principal component analysis based on a polychoric correlation matrix. Variables included in this index are household construction materials in an ordinal scale (floor, walls and ceiling), number of rooms used for sleeping, provision of water, car possession, number of domestic appliances (refrigerator, washing machine and boiler) and number of electrical appliances (TV, Internet, radio, telephone, cellphone and computer). The first principal component is a weighted average of the individual variables included, and it was used as the SE index, with 53·9 % of the total variability with an eigenvalue (λ) of 4·3 for a total of eight variables( Reference Gutierrez 29 ); therefore, higher levels of the index represent better SE conditions. For descriptive purposes, the SE index was classified by quintile distribution. The previous information was furnished by the head of the family during the survey.
Covariates
Age was included as a count variable in the whole sample model (for each year of life 1, 2, 3, 4 and 5 years).
Data analyses
Basic characteristics of children including their SE status and food insecurity level are described between the FAP and comparison groups. For comparison between groups, the χ 2 Pearson test with survey design correction was used( 30 ). For comparative purposes, we used the non-corrected cell χ 2 contributions to identify significant differences.
A structural equation model (SEM)( Reference Mulaik 31 ) was used to study the association between FAP, dietary and SE conditions, and anaemia; the advantage of the SEM is the capability to estimate direct and indirect associations that classic regression models cannot do( Reference Loehlin 32 ). Initially, a theoretical graphic model was developed establishing connections between variables as measures of association of FAP, dietary and SE conditions and anaemia prevalence. Arrowhead lines represent direct associations or dependencies, and double arrowhead lines represent correlations.
SEM includes two statistical components: one is the confirmatory factor analysis in which latent factors are non-observed variables (without units of measure) built on observable measured variables, and the second is path analysis, which is used to describe dependencies or associations among a set of variables or latent factors.
In our model, the latent factor is dietary and SE conditions, represented by a circle (Fig. 1); it was constructed using two measured variables: SE index and household food insecurity at two levels (mild and severe) using dummy variables, which are represented by boxes with arrows from the latent variable. The latent factor coefficients in the model only shows the direction and strength of the contribution of the factor to each measured variable; all coefficients are in terms of changes in standard deviations from the mean.
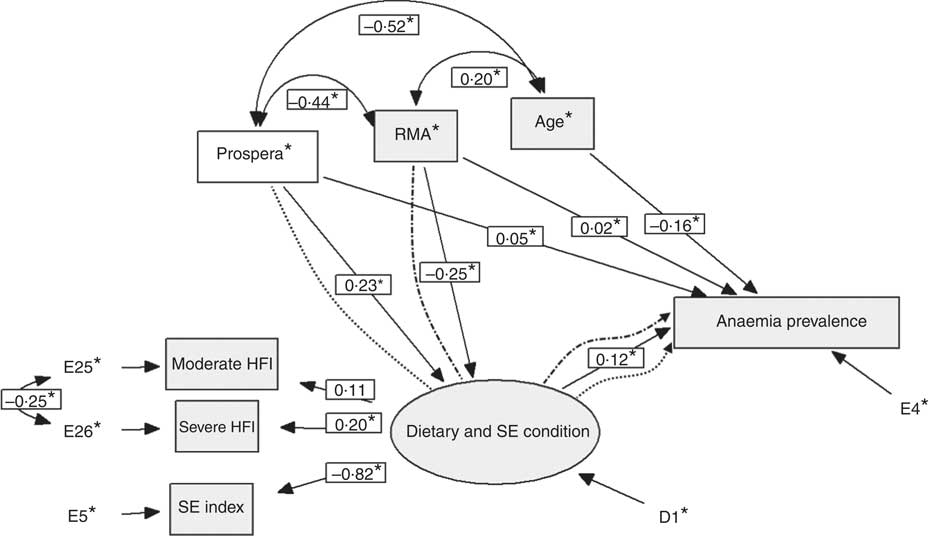
Fig. 1 This figure describes the paths followed by programmes to have an impact on the final variable: prevalence of anaemia. These in a direct manner go from Prospera and rescue from malnutrition with amaranth (RMA) to the prevalence of anaemia and are represented by solid lines. The other path represents an indirect manner; it goes first from programmes through dietary and socio-economic (SE) conditions to modify finally the prevalence of anaemia; it is represented by dotted lines in the figure. * Estimated parameters in the model fitting procedure. HFI, household food insecurity.
Path analysis is the representation of direct effects or associations among FAP, dietary and SE conditions and age on anaemia prevalence. Decomposition effect is a procedure to estimate the total effect of one variable on another composed by direct and indirect effects where alternative pathways exist. Direct effects are widely understood in common regression models, but indirect effects are rarely described and analysed. In this model, we highlight the indirect associations of FAP on anaemia FAP.
The final model included 1214 children (420 beneficiaries of Prospera, 420 beneficiaries of RMA and 374 in the comparison group) who had the full set of variables included in the final analysis. Prospera and RMA were included in the model as dummy indicator variables for beneficiary children. Significant association parameters were defined if a P-value was <0·05.
The analyses were conducted using Stata Statistical Software (release 13; StataCorp LP) and the SEM was built using the EQS 6 Structural Equations Program ( Reference Bentler 33 ).
Ethical considerations
The study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Research, Ethics, and Biosecurity Committees at the National Institute of Public Health in Cuernavaca, Mexico. Written informed consent was obtained from the parents of all participants.
Results
The basic characteristics of the whole sample, stratified by comparison groups, are described in Table 2. The distribution by sex was similar between the study groups; 45 % of Prospera beneficiaries, 34·0 % of RMA beneficiaries and 38 % of the comparison group lived in households moderately or severely food insecure, and only 18·5 % were food secure. Prospera had a higher proportion of children in severe household food insecurity than RMA and the comparison group. Children in the Prospera group had a lower SE index (Q1+Q2) (55·5 %) compared with 19·3 % for children in the RMA group.
Table 2 Percent distributions of descriptive characteristics by study groups (Numbers, percentages and 95 % confidence intervals)
HFI, household food insecurity; SE, socio-economic; Q, quintiles; RMA, rescue from malnutrition with amaranth.
* χ 2 Test.
One out of three children were anaemic; Prospera beneficiaries had a significantly higher prevalence of anaemia than the RMA group (P=0·001) (Table 2).
Fig. 1 shows the graphical SEM with standardised coefficients (in small boxes); this figure describes the paths followed by programmes to affect the final variable: prevalence of anaemia. These, in a direct manner, go from Prospera and RMA to the prevalence of anaemia and are represented by a solid line. The other path represents an indirect manner; it goes first from programmes through dietary and SE conditions to modify finally the prevalence of anaemia, and it is represented by dotted lines.
Standardised coefficients for direct associations in the model are shown in Table 3. FAP does not present significant direct associations with the prevalence of anaemia. Prospera had a significant negative association and the RMA programme showed a significant positive association with dietary and SE conditions (because latent factor has inverse scale in the model), meaning that Prospera targets populations with lower dietary and SE conditions and RMA targets beneficiaries with better conditions. Dietary and SE conditions showed a highly significant negative association with the prevalence of anaemia, indicating that high dietary and SE conditions are related to lower anaemia prevalence.
Table 3 Structural equation model coefficients for the path analysis diagram (direct effects)

RMA, rescue from malnutrition with amaranth.
* This factor has an inverse scale, and thus negative coefficients represent positive associations and vice versa.
The indirect associations of FAP on anaemia (Table 4) show a significant positive association for Prospera and a significant negative association for RMA on the prevalence of anaemia; this associative link goes through the food and SE conditions (represented by dotted lines in Fig. 1). This means that FAP is indirectly associated with anaemia through dietary and SE conditions, and thus in an impact evaluation study it will be expected that FAP could drive changes in anaemia prevalence through changes in dietary and SE conditions.
Table 4 Structural equation model indirect effects on anaemia prevalence
RMA, rescue from malnutrition with amaranth.
Latent factor coefficients are shown in Table 5; dietary and SE conditions had a significant negative association with the multivariate SE index and a significant positive association with the severity of the household food insecurity, and thus dietary and SE conditions had an inverse scale, as mentioned above; this means that a high level of this latent factor represents the worst situation. Prospera and RMA are not included as manifest variables of the dietary and SE conditions; both programmes are represented as independent factors with a direct influence on the latent factor (arrows are in the opposite direction with respect to manifest variables).
Table 5 Coefficients for the confirmatory factor analysisFootnote *

HFI, household food insecurity.
* Coefficient set to 1 to avoid model over specification.
** This factor has an inverse scale, and thus negative coefficients represent positive associations and vice versa.
Age as an important covariate has a significant negative association on the prevalence of anaemia and is negatively correlated to Prospera and positively to RMA, because Prospera is mainly focused on children under 2 years old and RMA focuses on older children. The negative correlation of Prospera and RMA represents a non-overlapping of both programmes in the sample, because beneficiaries of both programmes selected are mutually exclusive, and thus beneficiaries of Prospera should not have RMA and vice versa.
The fitted SEM had a comparative fit index of 0·98 and a root mean square error approximation of 0·045, meaning that the model has a good representation of the relationships among the observed variables. The whole model χ 2 statistic is 30·17 based on 8 df, and a P<0·001.
Discussion
The results of our study show an association between food and SE conditions and the prevalence of anaemia in FAP beneficiary children in SLP, Mexico. FAP partially mediates the association between lower dietary and SE conditions and a greater prevalence of anaemia( Reference Mazur, Marquis and Jensen 34 , Reference Fox, Hamilton and Lin 35 ). These results provide a novel theoretical approach for understanding the relationship between FAP and anaemia. The children with low dietary and SE conditions may experience greater food insecurity( Reference Lowe and Butryn 36 ), and the lack of effectiveness of FAP is associated with greater food insecurity in children in SLP. These associations may be mediated by dietary intake and may warrant further investigation.
It has been suggested that in children the prevalence of anaemia is caused mainly by an inadequate diet, poor social and economic conditions( Reference Galloway 37 , Reference Galloway 38 ) and other variables such as the stunting status of children, Fe supplement intake, food insecurity and the level of education and employment of the mother( Reference Pasillas-Torres and Rodríguez-Ortega 39 ).
It is possible that food social programmes may explain why these measures have not improved dietary quality and may increase the risk of anaemia among populations with low dietary and SE conditions; such is the case for RMA. It has been documented that food choice depends on reinforcing nutritional value, food accessibility( Reference Epstein, Leddy and Temple 40 ) and FAP focalisation. Nutritional assistance improves access to healthier options, but people tend to find less healthy foods, and chronic deprivation characterised by food insecurity may enhance this preference( Reference Raynor and Epstein 41 ). This suggests that food reinforcement and nutrition education may have the biggest effect on food security.
Several factors such as SE index, age and parents’ education, among others, have been associated with childhood anaemia. A study in India revealed that, in children between 6 and 59 months of age, anaemia has a strong negative association with the parent’s literacy status and wealth( Reference Bharati, Pal and Chakrabarty 42 ). In Mexico, those associations have been documented through an estimated logistic regression model for pre-school children using data from the 2012 National Health and Nutrition Survey (ENSANUT 2012) adjusting for SE status, BMI, residence and geographical region, FAP and security health services as covariates. It was reported that despite the decrease in the prevalence of anaemia in children between 1 and 4 years in the past 13 years, it is still of great concern, especially in indigenous children who live in the poorest areas( Reference De la Cruz-Góngora, Villalpando and Mundo-Rosas 7 ).
Another analysis from our study shows that 29·3 % of the children from households with food insecurity suffered anaemia, and the probability of being anaemic increases if the children are stunted. Households with anaemic children who did not receive FAP were generally more food secure than those who were beneficiaries of such programmes (PROSPERA and RMA) (data not shown)( Reference Shamah-Levy, Villalpando and Cuevas-Nasu 43 ).
A study in Bangladesh, Ethiopia and Vietnam showed that household food insecurity is a recognised underlying determinant of child undernutrition. However, evidence of associations between food insecurity and child undernutrition is mixed. The authors found that household food insecurity was significantly associated with wasting in Bangladesh, and that the diversity of the child’s diet did not mediate the association between household food insecurity and undernutrition in any of the countries( Reference Ali, Saha and Nguyen 44 ).
Another study in Hispanic children in the fifth grade and their mothers showed that children from the most food-insecure households had significant decreases in energy intake and meat consumption( Reference Matheson, Varady and Varady 45 ). We hypothesised that household food insecurity may lead to anaemia among Mexican children through different diet-related pathways: first, poor dietary intake and/or absorption of Fe; second, through a diet lacking sufficient micronutrients that may facilitate Fe absorption and utilisation (such as vitamin C, vitamin A, folate, vitamin B12 and carotenoids); and third, by consuming foods rich in phytic acid (such as maize) that may decrease Fe absorption( Reference Fischer, Shamah-Levy and Mundo-Rosas 46 , Reference De la Cruz-Gongora, Villalpando and Rebollar 47 ).
Previous studies in the United States examining household food insecurity and micronutrient deficiencies using scales similar to ELCSA suggest that diets in food-insecure households are lower in Fe and other micronutrients and higher in carbohydrates and fat, which indicates a continuing need for successful interventions to reduce Fe deficiency anaemia among food-insecure children and to improve food security among children( Reference Kaiser, Lamp and Johns 48 , Reference Eicher-Miller, Mason and Weaver 49 ). Specifically in Mexico, some epidemiological studies suggest that anaemia is strongly linked to deficiencies in micronutrients that increase the bioavailability of Fe, namely vitamin A and vitamin C( Reference De la Cruz-Gongora, Villalpando and Rebollar 47 , Reference Shamah-Levy, Villalpando and Jáuregui 50 , Reference Morales-Ruán, Villalpando and García-Guerra 51 ).
Also in Mexico, the poorest children have access to a high energy intake content that is low in dietary Fe, with the exception of those who are beneficiaries of Prospera or the subsidised fortified milk distribution programme (Liconsa)( Reference Rivera, Sotres-Alvarez and Habicht 52 – Reference Rivera, Shamah and Villalpando 54 ).
Our study has some limitations regarding how the programmes affect the prevalence of anaemia. This issue cannot be addressed because it is only a cross-sectional study, and thus we referred to statistical associations in order to describe the relationships between variables of beneficiary children from SLP. The inclusion of the length of time of a subject as beneficiary of the FAP should be used in further impact research.
In conclusion, FAP may indirectly modify the prevalence of anaemia in young children from SLP, Mexico, with a direct improvement on dietary and SE conditions. The unexpected finding of an association between RMA, dietary and SE conditions and the prevalence of anaemia reflects differences in the focus of the programmes. The SEM is a better way to represent variable relationships including indirect effects involved in the phenomenon under study.
Integral strategies and actions are required to reduce the number of children with anaemia for protecting and promoting nutritional, rather than using only the targeted, efforts utilised this far. In addition, there is a need for more research to explain the prevalence of anaemia in households with a better SE than the poorest.
Acknowledgements
The present study was supported by FOMIX, SLP-COPOCYT. Project: FMSLP-213-CO2-208475.
The authors thank Miguel Gaytan for coordination in the field work for obtaining information. We also would like to thank the children and their mothers of San Luis Potosi for their support and for volunteering their time to answer questionnaires and provide blood samples. We also thank Jesus Martinez and Eric Rolando López for his contribution to the consolidation of databases and processing.
The authors’ responsibilities were as follows: T. S.-L. coordinated the data analysis and interpretation and wrote the manuscript and designed the research; I. M.-G-H. conducted the data analysis and provided statistical expertise; L. C.-N., S. V. and E. B. G.-P. helped with the interpretation and contributed to the writing of the manuscript. All authors read and approved the final manuscript.
All authors declare that there are no conflicts of interest.






