



Crossref Citations
This article has been cited by the following publications. This list is generated based on data provided by Crossref.
Sedgi, Fatemeh Maleki
Hosseiniazar, Mohammadreza Mohammad
and
Alizadeh, Mohammad
2024.
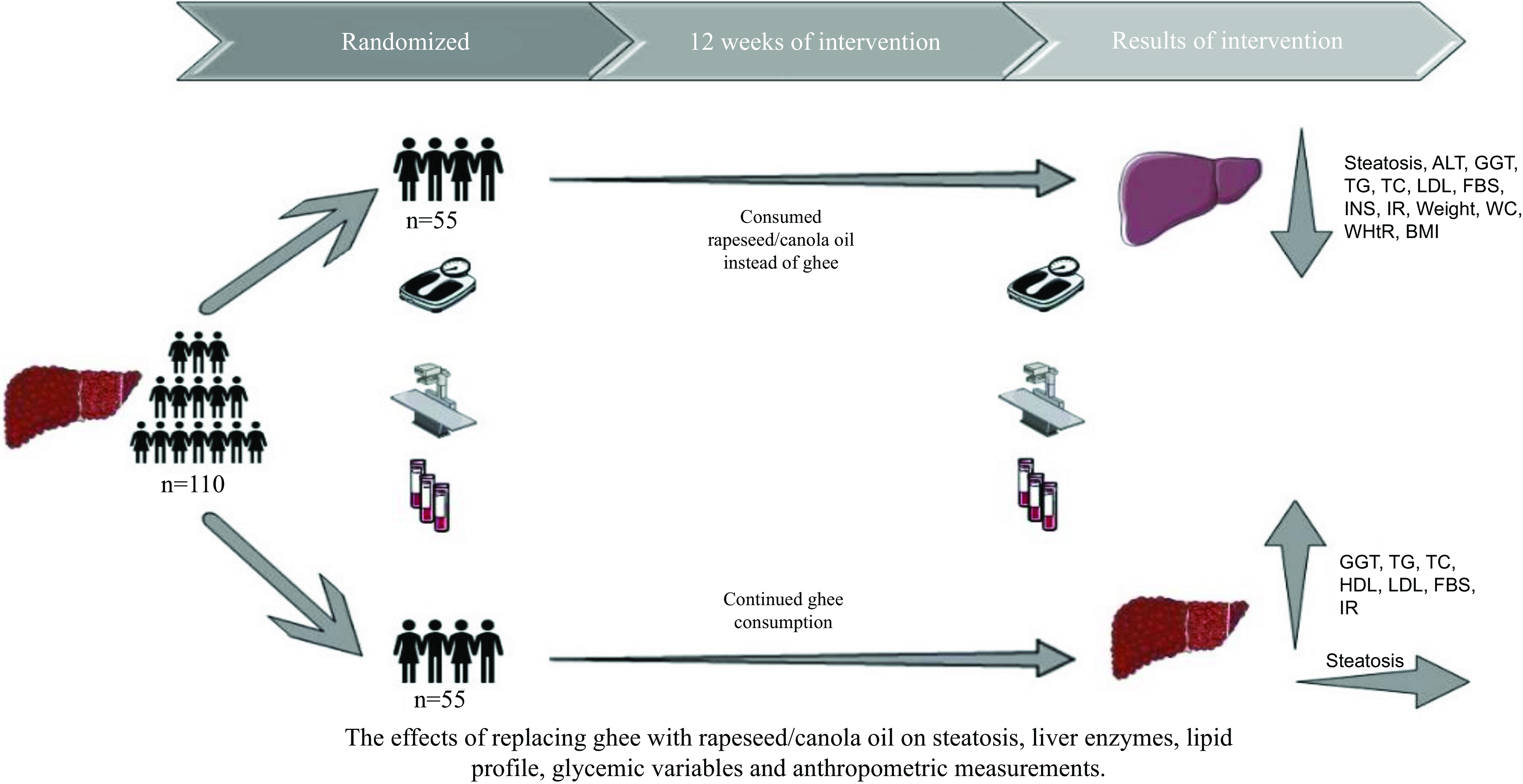
The impact of substituting clarified butter with canola oil on the components of metabolic syndrome, fatty liver index, and insulin resistance among individuals diagnosed with metabolic syndrome: a quasi-experimental study.
Journal of Diabetes & Metabolic Disorders,
Vol. 23,
Issue. 2,
p.
1977.
Misra, Anoop
Kumar, Ashish
Kuchay, Mohammad Shafi
Ghosh, Amerta
Gulati, Seema
Choudhary, Narendra Singh
Dutta, Deep
Sharma, Praveen
Vikram, Naval K.
Rastogi, Ashu
Shukla, Akash
Goyal, Alpesh
Gupta, Amit
Kulkarni, Anand V.
Chandra Anand, Anil
Arora, Anil
Mathew, Anu
Jagadeesha, Aravinda
Banerjee, Arijit
Ojha, Arvind Kumar
Luthra, Atul
Singh, Awadhesh Kumar
Saboo, Banshi
Saboo, Bharat
Makkar, Brij Mohan
Selvan, Chitra
Eapen, Chundamannil E.
Sanyal, Debmalya
Hasnani, Dhruvi
Kumar, Dinesh
Farishta, Faraz
Chhaya, Gaurav
Choudhuri, Gourdas
Sridhar, Gumpeny R.
Kesavadev, Jothydev
Sharma, Jugal Kishor
Natarajan, Kannan
Madan, Kaushal
Mehta, Ketan K.
Shah, Kiran
Das, Kunal
Premkumar, Madhumita
Wadhawan, Manav
Tiwaskar, Mangesh
Agrawal, Mayur
Verma, Nipun
Goswami, Parikshit
Kaur, Parjeet
Ranjan, Piyush
Agrawal, Prabhat Kumar
Sankar, Prasanth
Chawla, Purvi
Agrawal, Rajesh
Maiwall, Rakhi
Mehta, Rucha
Madhu, S.V.
Banerjee, Samar
Suri, Sandeep
Biradar, Sangram
Kalra, Sanjay
Bhadada, Sanjay Kumar
Agrawal, Saurav Shishir
Shalimar
Gulati, Seema
Shah, Shashank
Patil, Shubhashree Mangesh
Waghdhare, Swati
Chavda, Vipul
Mohan, Viswanathan
Gupta, Vitull K.
Saraswat, Vivek A.
and
Gupta, Yashdeep
2025.
Consensus guidelines for the diagnosis and management of metabolic dysfunction-associated steatotic liver disease in adult Asian Indians with type 2 diabetes.
Diabetes & Metabolic Syndrome: Clinical Research & Reviews,
Vol. 19,
Issue. 3,
p.
103209.
Lan, Yuxiang
Zhong, Chaohao
Li, Dujin
Chen, Haobin
and
Dai, Xu
2025.
Association between waist-to-height ratio and insulin resistance in patients with polycystic ovary syndrome: a meta-analysis.
Frontiers in Endocrinology,
Vol. 16,
Issue. ,