


Dismounted military personnel undertake land-based missions in austere environments, including high-altitude terrain( Reference Jones, Hoyt and Baker 1 ), the tropics( Reference Booth, Coad and Forbes-Ewan 2 , Reference Booth, Coad and Roberts 3 ), deserts( Reference Cline, Tharion and Tulley 4 ) and in sub-zero temperatures( Reference Margolis, Murphy and Martini 5 , Reference Edwards, Roberts and Mutter 6 ). Such missions require personnel to carry their own supplies, and vary in physical and cognitive intensity. The most arduous, such as those involving combat activities, are often superimposed with multiple physiological and psychological stressors( Reference Nindl, Castellani and Warr 7 ). These include prolonged periods of near-continuous physical activity (often with load carriage exceeding 50 kg( Reference Fallowfield, Delves and Hill 8 )) and sleep deprivation, while maintaining high levels of alertness, attention, executive function and ultimately, job performance( Reference Alemany, Nindl and Kellogg 9 – Reference Tikuisis, Keefe and McLellan 13 ).
Personnel display particularly high levels of total daily energy expenditure (TDEE) during field operations. The highest reported TDEE is 29·8 (sd 0·9) MJ( Reference Hoyt, Jones and Stein 14 ), which was measured over multiple days of mountain warfare training. This is comparable with the mean TDEE measured over the 5-d mountain stage of the Tour de France, of 28·4 MJ/d( Reference Saris, van Erp-Baart and Brouns 15 ). When training on base, personnel typically display lower levels of TDEE, between 14·4 (sd 2·9) and 17·2 (sd 3·1) MJ( Reference Bovill, Baker-Fulco and Tharion 16 ), and are likely to remain in energy balance as the environment is conducive to eating adequately( 17 ). On base, personnel typically experience shorter working hours, have ample opportunity to sleep in dormitories, and eat freshly cooked meals in dining halls( Reference Tharion, Lieberman and Montain 18 ). In contrast, the complex, stressful and demanding field environment impacts substantially on food intake( Reference Hirsch and Kramer 19 ). Combat rations (CR) are provided to troops during field operations when it is not practicable to establish a field kitchen to provide fresh foods( 20 ). CR contain packaged food and drink items including main courses, snack items and beverage powders( Reference Hirsch, Kramer and Meiselman 21 ). Personnel often carry personal rations to supplement or diversify their diet during times of CR use( Reference Baker-Fulco, Patton and Montain 22 ), and may also be provided with supplementary foods( Reference Booth, Coad and Roberts 3 , Reference Alemany, Nindl and Kellogg 9 , Reference Booth, Coad and Roberts 23 , Reference Tanskanen, Westerterp and Uusitalo 24 ).
When used exclusively, CR are designed to provide military personnel with appropriate nutrition( 20 ). However, their high levels of TDEE are almost always met with under-consumption of CR( Reference Hirsch, Kramer and Meiselman 21 , Reference Forbes-Ewan 25 ); for example, only approximately 50 % of the energy content of CR was consumed during a study by Lester et al. ( Reference Lester, Lesher and Salomon 26 ). Troops have reported having insufficient time to prepare meals to eat during combat activities, as well as the inability to carry sufficient food due to space and weight limitations as a result of prioritising combat equipment( Reference Popper, Smits and Meiselman 27 ).
As a result of the complex and demanding nature of field operations, personnel may be in large energy deficits (ED), and experience rapid reductions in body weight (BW) and deleterious changes in body composition (BC). Reductions in BW during CR use are largely due to losses in fat mass (FM); however, fat-free mass (FFM) has also been shown to decline to varying extents( Reference Consolazio, Johnson and Nelson 28 , Reference Schoeller, Field and DeLany 29 ). It is important to understand the types of field training or operations during which troops may be particularly susceptible to substantial losses in FFM.
Marked decreases in BW during military operations of <3 d duration are likely due to water losses or dehydration, rather than losses of FM and/or FFM( 17 ), with an average BW loss of <3 % in this time period ‘unlikely’ to impact performance( 17 ). Conversely, the Committee on Military Nutrition Research of the US Institute of Medicine (IOM) states that a 10 % or more reduction in BW during military training that lasts for up to 30 d is ‘very likely’ to impact physical and cognitive performance( 17 ). Providing troops with appropriate nutrition during field training and periods of deployment is therefore paramount in mitigating the impact of field missions on BW, BC, and in turn, physical and cognitive performance, and immune status( 20 , Reference Day, Young and Askew 30 ). Although, it is the policy of many North Atlantic Treaty Organization (NATO) nations for CR to be used exclusively for a maximum period of 30 d( 17 ), there may be emergency situations in which military personnel will be required to subsist on CR for a longer duration until fresh feeding can commence. To date, systematic evidence including a rigorous risk of bias and quality assessment has not been published regarding the effect that continual CR use for periods between 3 and 40 d may have on BC and BW.
CR, recovery feeding policies, and BW and BC monitoring policies must be designed to mitigate the impact of missions on the BW, BC and performance of troops, using comprehensive evidence. Consequently, this systematic review aims to investigate the effects of the continual use of CR for periods of 3–40 d on BW and/or BC (FM, percentage of body fat (%BF) and/or FFM) in dismounted military personnel engaged in military field training or deployment, through evaluation of empirical research.
Methods
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement checklist( Reference Moher, Liberati and Tetzlaff 31 ). The protocol was registered with the PROSPERO International prospective register of systematic reviews (CRD42016030141) and can be accessed at http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016030141.
Eligibility criteria
The participant, intervention, comparator, outcome, study design (PICOS) format was used to develop eligibility criteria for study inclusion (Table 1). The review was limited to studies where BW and/or BC was monitored in military personnel engaged in military training or deployment involving the continual use of CR for periods of 3–40 d.
Table 1 Participant, intervention, comparator, outcome, study design inclusion and exclusion criteria used to determine study eligibility
CR, combat rations; BC, body composition; BW, body weight.
Studies involving military personnel who were provided with packaged supplementary food (in addition to CR) were also eligible for inclusion, as were studies involving participants who were permitted to eat personal rations.
Original peer-reviewed research of any study design and relevant grey literature (e.g. government reports, conference proceedings and theses) were eligible for inclusion, whilst review articles, abstracts and non-empirical research were excluded.
Search strategy
A search was conducted of the following electronic databases: Scopus, Ovid MEDLINE, Proquest Central, Cumulative Index of Nursing and Allied Health Literature (CINAHL) Plus, EMBASE, Web of Science, SPORTDiscus, Cochrane Library (Trials), National Technical Information Service (NTIS), in addition to the Defense Technical Information Center (DTIC), from their inception until December 2015. All databases were searched using a uniform combination of search terms (Table 2) derived from background reading and relevant Medical Subject Headings (MeSH). The search of the DTIC database was limited to the first ten pages of results, sorted by relevance. The title, abstract and keyword fields were searched in all of the databases. Searches were limited to studies published in English. After finalising the manuscript, searches in all databases were performed using the same search strategy for the period from December 2015 to October 2016.
Table 2 Search terms and search strategy
* Truncated term.
Study selection
A detailed overview of the study selection process can be found in the aforementioned protocol registered prospectively on PROSPERO.
Data extraction
The two authors independently extracted data from the included studies using a customised table. For studies that did not report the mean percentage BW change in participants, an approximate value was calculated using the mean initial and final BW values. When necessary, unit conversions were performed for energy, BW, BC, altitude and temperature data by one author according to the rates specified by the International System of Units guidelines. Data conversion checks were then performed on 100 % of the data. Data regarding the hydration status of participants was not extracted from the included studies, however it was assumed that participants were well hydrated at the beginning of field missions, and had opportunities to replace fluids losses after field missions before BW and BC measurements were made.
Several included studies were found to be published two or three times, in both the scientific literature and as government reports. In these instances, all publications are referenced in tables, however, they have been counted as one study in the final number of included studies. In the text, only the primary publications have been referenced.
In instances where a study reported that initial and final BW and/or BC measurements were taken but were not reported, the corresponding or first author was contacted for the missing data (where the authors were unable to find their email address, a subsequently listed author was contacted). This was also done in instances where the study protocol was unclear. Follow-up emails were sent to authors 2 weeks later when a response had not been received. Consequently, a study was excluded if the data had not been received.
In addition, the sex of participants was not reported in a number of studies. In these instances, if the study was conducted before 2013, the sex of the personnel was assumed to be male based on the type of personnel, as until then females had not been permitted to take part in the field training courses captured in this review.
Risk of bias, quality and synthesis of results
Both authors independently assessed each of the included studies for risk of bias and study quality using the Academy of Nutrition and Dietetics Quality Checklist( 32 ), with each paper rated as either positive, negative or neutral in quality. The design of each study was assessed by both authors independently using the Academy of Nutrition and Dietetics Research Design Algorithm( 32 , 33 ). Wherever a discrepancy was found, the authors reached a consensus through discussion.
The National Health and Medical Research Council (NHMRC) Evidence Hierarchy( 32 ) was used to designate a level of evidence (from II high to IV low) to each study according to its research question and study design( 32 ). In developing recommendations, greater weight was given to findings from studies providing high-level evidence.
Due to the differences in study protocols (e.g. duration of CR use, type of CR provided, type of military personnel, military activity and environmental conditions) and the lack of comparator, a meta-analysis could not be performed; results were thus tabulated and described narratively.
Results
Study selection
A total of 6490 records were retrieved from the database searches (Scopus=1495, Cochrane library (trials)=eighty-three, ProQuest Central=1248, SPORTDiscus=246, CINAHL Plus=265, Embase=837, Ovid MEDLINE=541, Web of Science Core Collection=1169, DTIC=100, NTIS=506), of which twenty-eight were included in the systematic review. One further article was obtained from backwards citation searching of the twenty-eight included studies, and one from a hand-search of the grey literature. In total, thirty studies( Reference Jones, Hoyt and Baker 1 , Reference Booth, Coad and Forbes-Ewan 2 , Reference Margolis, Murphy and Martini 5 , Reference Edwards, Roberts and Mutter 6 , Reference Alemany, Nindl and Kellogg 9 , Reference Booth, Coad and Roberts 23 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Lester, Lesher and Salomon 26 , Reference Consolazio, Johnson and Nelson 28 , Reference Schoeller, Field and DeLany 29 , Reference Owen, Turley and Casey 34 – Reference Hirsch, Meiselman and Popper 53 ) met the PICOS inclusion criteria and were included in the systematic review. Fig. 1 provides a detailed overview of the number of studies screened at each stage of the study selection process.

Fig. 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection.
Study characteristics
In twenty-nine of the included studies, all participants were, or were assumed to be, male( Reference Jones, Hoyt and Baker 1 , Reference Booth, Coad and Forbes-Ewan 2 , Reference Margolis, Murphy and Martini 5 , Reference Edwards, Roberts and Mutter 6 , Reference Alemany, Nindl and Kellogg 9 , Reference Booth, Coad and Roberts 23 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Lester, Lesher and Salomon 26 , Reference Consolazio, Johnson and Nelson 28 , Reference Schoeller, Field and DeLany 29 , Reference Owen, Turley and Casey 34 , Reference Jacobs, Van Loon and Pasut 36 – Reference Hirsch, Meiselman and Popper 53 ), however the most recently published study included two female participants( Reference Margolis, Murphy and Martini 35 ). The occupations of participants varied, with Infantry, Special Forces and Marines being among the most common occupations. The studies involved a range of specific military tasks, including combat training, field training and adventurous military training (see the online Supplementary Table S1 for a complete list of participant characteristics, military tasks and other key characteristics). Publication dates were in the period 1976–2016.
The duration of continual CR use varied between the studies, ranging from 3( Reference Margolis, Murphy and Martini 5 ) to 34 d( Reference Hirsch, Meiselman and Popper 53 ). Packaged supplemental food and/or drinks were provided in eleven of the included studies( Reference Jones, Hoyt and Baker 1 , Reference Edwards, Roberts and Mutter 6 , Reference Alemany, Nindl and Kellogg 9 , Reference Booth, Coad and Roberts 23 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Margolis, Murphy and Martini 35 , Reference Jacobs, Van Loon and Pasut 36 , Reference Nindl, Alemany and Kellogg 40 , Reference Edwards and Roberts 41 , Reference Morgan, Hodgess and Schilling 44 , Reference Crowdy, Consolazio and Forbes 45 ), and two studies also allowed personal rations to be consumed( Reference Owen, Turley and Casey 34 , Reference Siegel, Poole and Askew 46 ) (see the online Supplementary Table S1 for further details).
Quality assessment
The online Supplementary Table S2 lists quality ratings and levels of evidence for each of the thirty included studies. Four studies were rated positive in quality and were considered to be at low risk of bias( Reference Margolis, Murphy and Martini 5 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Shippee, Askew and Bernton 39 , Reference Johnson, Krzywicki and Canham 47 ). The majority of studies, twenty-five in total, were rated neutral in quality( Reference Jones, Hoyt and Baker 1 , Reference Booth, Coad and Forbes-Ewan 2 , Reference Edwards, Roberts and Mutter 6 , Reference Alemany, Nindl and Kellogg 9 , Reference Booth, Coad and Roberts 23 , Reference Lester, Lesher and Salomon 26 , Reference Consolazio, Johnson and Nelson 28 , Reference Schoeller, Field and DeLany 29 , Reference Owen, Turley and Casey 34 – Reference O’Brien, Freund and Sawka 38 , Reference Nindl, Alemany and Kellogg 40 – Reference Siegel, Poole and Askew 46 , Reference Kyrolainen, Karinkanta and Santtila 48 , Reference Gomez-Merino, Chennaoui and Drogou 50 – Reference Hirsch, Meiselman and Popper 53 ), with one further study rated negative in quality( Reference von Restorff, Diebold and Brezina 49 ). These studies were considered to be at risk of bias, with full details of methodological weaknesses listed in the online Supplementary Table S2. Levels of evidence ranged from high (II) to low (IV) according to the NHMRC levels of evidence hierarchy( 33 ) and are listed in the online Supplementary Table S2.
Outcomes
The included studies have been listed in Table 3 according to the duration over which they were conducted, from shortest (3 d) to longest (34 d) in duration. A reduction in the mean BW, FM and/or %BF of participants was a consistent finding amongst all included studies( Reference Jones, Hoyt and Baker 1 , Reference Booth, Coad and Forbes-Ewan 2 , Reference Margolis, Murphy and Martini 5 , Reference Edwards, Roberts and Mutter 6 , Reference Alemany, Nindl and Kellogg 9 , Reference Booth, Coad and Roberts 23 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Lester, Lesher and Salomon 26 , Reference Consolazio, Johnson and Nelson 28 , Reference Schoeller, Field and DeLany 29 , Reference Owen, Turley and Casey 34 – Reference Hirsch, Meiselman and Popper 53 ), with reductions in FFM seen in all studies except for in one sub-group in the Askew et al. study( Reference Askew, Munro and Sharp 52 ) and one sub-group of the Tanskanen et al. study( Reference Tanskanen, Westerterp and Uusitalo 24 ).
Table 3 Summary of results from included studies(Mean values and standard deviations; standard errors)
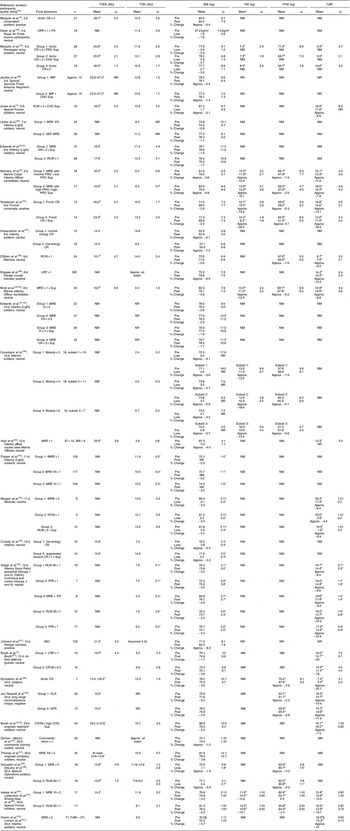
TDEE, total daily energy expenditure; TDEI, total daily energy intake; BW, body weight; FM, fat mass; FFM, fat-free mass; %BF, percentage body fat; CR, combat ration; Approx., approximately; NM, not measured; ORP, operational ration pack; PR, personal rations; PRO, protein; Sup, supplement; CHO, carbohydrate; IMP, individual meal packets; NR, not reported; RLW, ration, lightweight; MRE, meal, ready-to-eat, SEP MRE, Soldier Enhancement Program Meal, ready to-eat; RCW, ration, cold weather; LRP, long range patrol ration; EI, energy intake; IMRE, improved meal, ready-to-eat; FPA, food packet assault; MCI, meal, combat, individual; CRP, combat ration pack; SLR, special lightweight ration; GFR, German field rations; CR1M, combat ration one man; RLW-30, ration, lightweight-30 d.
aMeasured using doubly labelled water; bderived from skinfold thickness measurements; cestimated from continuous heart rate recordings and direct O2 uptake measurements; destimated using the intake/balance method; ecalculated from underwater weighing; festimated from food intake and weight loss; gmeasured using whole body dual-energy X-ray absorptiometry; hFM was calculated as BM−FFM, FFM calculated as total body water (measured with 2H dilution according to the Maastricht protocol)/0·732, and %BF as FM/BM×100; iestimated using the factorial method; jmeasured by the direct water displacement technique; kestimated from circumference measurement (s); lcalculated from the measured O2 consumption rates applied to the duration of each recorded activity; mbioelectrical impedance; nestimated using ‘OwnCal’ software (Polar Electro Inc.); omethod not specified; ptotal body water/0·73 (total body water based on 18O dilution space/1·01).
* se.
† sem.
‡ Whilst energy intake was NM, it was assumed that 100 % of the rations were consumed as very little energy was provided.
§ Measurements conducted during a 2-d period 9 and 10 d before the beginning of the field exercise when the soldiers were in barracks.
Discussion
This systematic review investigated the effects of the use of CR for continual periods of 3–40 d on BW and BC in dismounted military personnel engaged in training or deployment. A total of thirty studies that were conducted during training activities met the PICOS criteria. However, the search did not identify any studies that were conducted during deployment for the time period of interest.
Only six of the thirty included studies received a level II (high) evidence rating( Reference Alemany, Nindl and Kellogg 9 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Consolazio, Johnson and Nelson 28 , Reference Margolis, Murphy and Martini 35 , Reference Edwards and Roberts 41 , Reference Thomas, Friedl and Mays 51 ), with most of the included studies rated neutral in quality, thus indicating a moderate risk for bias. Whilst outcome data are considered less reliable from lower level evidence, military nutrition studies are almost exclusively undertaken during field training exercises scheduled for other purposes; thus it is often not possible to use gold-standard procedures for measuring BW, BC and human performance. Measurements which are suitable in field situations and can be undertaken quickly are often required.
This review captured studies with differing procedures for measuring BM and BC, with some not reporting measurement procedures in detail. Whilst these biases may have affected the magnitude of weight loss and changes in BC observed, it is a consistent finding across the thirty studies that decreases in BM, changes in BC and inadequate energy intake (EI) relative to energy expenditure occur during military training where personnel consume CR as their sole source of nutrition, thus useful conclusions can be drawn from the data.
Combat ration use and body weight
TDEE is known to be elevated during military field activities( Reference Margolis, Rood and Champagne 62 ) and large ED are often observed( Reference Alemany, Nindl and Kellogg 9 , Reference Hirsch, Kramer and Meiselman 21 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Nindl, Alemany and Kellogg 40 , Reference Johnson, Krzywicki and Canham 47 ). During short-duration CR use (3–7 d), large daily ED were observed, however the small resultant reductions in BW are considered unlikely to adversely affect performance( 17 ). However, personnel often undertake several short-duration missions during more prolonged training courses and deployments.
Seven studies were conducted during 8–10 d missions and the types and intensities of the missions in which CR were used covered a wide range, resulting in varying levels of ED( Reference Edwards, Roberts and Mutter 6 , Reference Alemany, Nindl and Kellogg 9 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Viswanathan, Prasad and Ramanuja 37 – Reference Nindl, Alemany and Kellogg 40 ). Large daily ED of approximately 9·3–10·0 MJ resulted in rapid BW loss during general purpose CR use, and were observed during 8-d field activities which, unlike the usual situation( 20 ), reportedly involved periods of near-continuous and strenuous physical and/or cognitive activity( Reference Alemany, Nindl and Kellogg 9 , Reference Shippee, Askew and Bernton 39 , Reference Nindl, Alemany and Kellogg 40 ). These included Infantry training, during which the mean BW of participants declined substantially, by 2·8 and 2·4 %( Reference Tanskanen, Westerterp and Uusitalo 24 ), approximately 3·8 and 4·8 %( Reference Alemany, Nindl and Kellogg 9 ). The largest daily ED was observed during a 10-d US Marine Infantry Officer course involving combat activities( Reference Hoyt, Buller and DeLany 42 ). In this study, the mean TDEE of participants was 22·5 MJ (measured using doubly labelled water) and mean TDEI was 5·58 MJ (from experimental CR containing only about 5·65 MJ). Participants had an initial mean BW of 81·0 kg and lost, on average, approximately 4·0 % BW. Personnel are likely to have the least amount of time to eat during these periods of near-continuous and strenuous activity, and it is likely that, in the 1st or 2nd day, the glycogen stores of personnel are depleted rapidly during such situations( Reference Jacobs, Van Loon and Pasut 36 ). This raises questions as to whether blood glucose levels are maintained at levels to support cognitive function and optimal energy metabolism for military tasks( Reference Taylor, Buskirk and BroŽek 63 ), particularly if there is insufficient time for meals to be eaten, or if the tactical environment has prevented a meal break for prolonged periods.
In contrast, substantially smaller ED during general purpose CR use resulted in slower reductions in BW during combat training lasting 8 d, such as Infantry defensive and assault activities( Reference Edwards, Roberts and Mutter 6 ). This contrast during 8–10 d of CR use is reflective of the broad range of environments and activities in which military personnel operate, and how these disparately impact on individuals’ ability to eat, on their TDEE, TDEI, and therefore, on BW. Furthermore, as indicated by the large standard deviations in BW loss, there are considerable ranges in the levels of BW loss among individuals undertaking the same missions( Reference Edwards, Roberts and Mutter 6 , Reference Alemany, Nindl and Kellogg 9 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Viswanathan, Prasad and Ramanuja 37 – Reference Nindl, Alemany and Kellogg 40 ).
Greater BW reductions were most commonly observed during special purpose CR use across all durations of CR use captured in this review. This is reflective of the more austere environments and hostile tactical situations for which special purpose CR are designed. Consequently, personnel display higher levels of energy expenditure and reduced levels of EI during special purpose CR use( Reference Forbes-Ewan, Waters and Coad 64 ). For example, the greatest mean BW reduction after an 8-d mission, of 6·0 %, was reported after use of the Long Range Patrol ration – a special purpose, lightweight CR suitable for troops who carry several days rations over long distances, when resupply of CR is often not possible due to the tactical situation( Reference Shippee, Askew and Bernton 39 ).
The most substantial decrease in mean BW was observed during 12 d of energy intake restriction during the jungle phase of a US Army Ranger course: from 71·3 to 65·4 kg( Reference Johnson, Krzywicki and Canham 47 ). This represents, on average, a BW reduction of approximately 8·3 %. However, previous phases during the Ranger course also involved inadequate EI, thus likely augmenting the BW losses observed during the jungle phase. By the conclusion of the 8-week course, BW losses averaged 9·4 %, with some individuals losing as much as 17·5 % of their initial BW. To our knowledge, this level of mean BW loss during 12 d of CR use has not been reported since 1976. CR have vastly improved since then, including becoming more convenient to eat in the field while providing better nutrition. Nevertheless, in the absence of additional data gathered during real-world operations involving non-stop combat activities, some groups may experience a mean BW loss of approximately 8·3 % over 12 d. According to the US IOM’s Committee on Military Nutrition Research, a BW loss of >3 % but <10 % during military training of 3–30 d duration is ‘unlikely’ to impact performance, whilst losses of >10 % are ‘very likely’ to impact performance( 17 ). However, a rapid loss of 6·2 % BM in a period of 1 week resulted in poorer cognitive outcomes including more tension, depression, anger, fatigue and confusion, in addition to poorer short-term memory in a group of collegiate wrestlers( Reference Choma, Sforzo and Keller 65 ).
During the more prolonged periods of CR use – those lasting 20–30 d – the mean levels of EI were closer to the mean levels of measured or estimated TDEE in most studies in which these were reported( Reference Booth, Coad and Roberts 23 , Reference Schoeller, Field and DeLany 29 , Reference Kyrolainen, Karinkanta and Santtila 48 , Reference Thomas, Friedl and Mays 51 ). In these studies, mean ED ranged between approximately 1·2 and 6·1 MJ/d( Reference Booth, Coad and Roberts 23 , Reference Schoeller, Field and DeLany 29 , Reference Kyrolainen, Karinkanta and Santtila 48 , Reference Thomas, Friedl and Mays 51 , Reference Askew, Munro and Sharp 52 ). However, the levels of TDEE were substantially lower compared with studies of lesser duration. The most pronounced levels of BW loss were seen during special purpose CR use: approximately 5·6 % BW during a 20-d arctic training exercise( Reference Kyrolainen, Karinkanta and Santtila 48 ), and approximately 6·3 % BW during a 30-d cold weather training exercise( Reference Askew, Munro and Sharp 52 ). Performance consequences of a similar level of BW loss were demonstrated in a study involving elite judo athletes that was conducted over a 4-week period( Reference Koral and Dosseville 66 ). This study showed that a mean BW decrease of 4·0 % resulted in significantly higher confusion and tension, and decreased vigour compared with the control group, which did not lose any weight.
The provision of supplementary foods in addition to CR was shown to be effective in mitigating BW losses, however, there were some limitations. Whilst experimental control was gained by providing the same CR to all study groups, the provision of supplement foods was only shown to be effective in reducing mean reductions in BW when participants were instructed that consumption of all supplement foods was mandatory( Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Jacobs, Van Loon and Pasut 36 ). Therefore, unless this condition is applied in field deployment or training, a beneficial effect may not be observed. Providing additional supplemental foods cannot overcome some of the barriers to nutritional intake that troops experience during training and operations in the field, such as limited load carriage capacity and limited time to eat( 20 , Reference Popper, Smits and Meiselman 27 ).
Combat rations use and body composition
BW losses primarily comprised of losses in FM, however, FFM also declined by varying levels during a number of studies( Reference Alemany, Nindl and Kellogg 9 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Consolazio, Johnson and Nelson 28 , Reference Schoeller, Field and DeLany 29 , Reference O’Brien, Freund and Sawka 38 , Reference Nindl, Alemany and Kellogg 40 , Reference Kyrolainen, Karinkanta and Santtila 48 , Reference von Restorff, Diebold and Brezina 49 , Reference Askew, Munro and Sharp 52 ). During short-term (8–10 d) CR use which resulted in fast BW reductions, there was a trend of FFM preservation in the study groups which consumed higher amounts of energy, despite having similar levels of daily ED, in the range of 9·3–10·0 MJ( Reference Alemany, Nindl and Kellogg 9 , Reference Tanskanen, Westerterp and Uusitalo 24 , Reference Nindl, Alemany and Kellogg 40 ). In a positive quality study by Tanskanen et al. ( Reference Tanskanen, Westerterp and Uusitalo 24 ), one study group lost, on average approximately 0·3 % of their FFM, and another gained approximately 0·7 FFM whilst consuming, on average, 10·9 and 13·3 MJ/d, respectively, and being in ED of 9·3 and 10·0 MJ/d, respectively. In contrast, substantially higher levels of FFM loss, of approximately 2·5, 2·2 and 1·9 %, were observed at similar TDEE of approximately 10·0 MJ/d but substantially lower TDEI of approximately 6·4–6·5 MJ/d( Reference Alemany, Nindl and Kellogg 9 , Reference Nindl, Alemany and Kellogg 40 ). Similarly, in a study conducted during a 30-d Special Forces field exercise, the extent of FFM loss was greater in the sub-group which had a lower TDEI( Reference Askew, Munro and Sharp 52 ). Collectively, these findings highlight that the extent of FFM loss during CR use is not solely dependent on the level of ED, and the level of TDEI during periods of high TDEE is of importance in the preservation of FFM. It is also probable that as the level of TDEI increases, the likelihood increases of consuming protein in the range 1·5–2·0 g/kg/d BW, as recommended by Pasiakos et al. ( Reference Pasiakos, Austin and Lieberman 67 ).
At very low levels of TDEI, increasing the protein content of the CR provided to personnel did not appear to provide any clear benefits to the preservation of FFM in personnel in one study undertaken over 8 d( Reference Alemany, Nindl and Kellogg 9 ). In this study, one sub-group of participants was provided with meal, ready-to-eat (MRE) containing approximately 0·5 g protein/kg BW and another was provided with MRE containing approximately 0·9 g protein/kg BW. Both sub-groups consumed similar levels of energy and had similar levels of ED. However, the higher levels of protein did not produce a measurable benefit to the preservation of FFM.
Collectively, these findings regarding the preservation of FFM are relevant to military personnel and also athletes aiming to make weight while maintaining or building FFM. It is often disputed whether or not it is possible to increase FFM whilst losing FM; however, a mean increase in FFM of 0·7 % was observed in the Tanskanen et al.( Reference Tanskanen, Westerterp and Uusitalo 24 ) study, despite an approximately 20·2 % reduction in FM. High levels of TDEE from near-continuous physical activities permit high levels of TDEI and optimal protein intake, in addition to losses of FM. Thus, a high level of TDEI is likely beneficial in preserving or increasing FFM during energy deficit.
The most substantial mean loss of FFM – approximately 3·6 % – was observed during a 20-d training exercise in Finland( Reference Kyrolainen, Karinkanta and Santtila 48 ). Throughout this exercise, the mean daily ED of participants fluctuated, and was likely to be particularly large in the first 7 d. Compared with all other studies, the participants in this study had the lowest levels of %BF: 7·4 (sd 3·1) % at the beginning, decreasing to just 5·5 (sd 2·0) % by the end of the study( Reference Kyrolainen, Karinkanta and Santtila 48 ). These low levels of BF are suboptimal for military personnel before periods of prolonged CR use, and may have contributed to the particularly large loss of FFM. A study undertaken by Friedl et al. ( Reference Friedl, Moore and Martinez-Lopez 68 ) suggested that the lower limit of BF in healthy men was 4–6 %, and those who exhibit BF at this level lose larger proportions of FFM and very little BF during weight loss compared with those with higher levels of BF.
The ramifications of decreases in FFM during combat and/or field training on performance has been previously demonstrated, with impaired performance during tasks which depend on elements of fitness such as lower body power output, as estimated by the vertical jump test( Reference Nindl, Alemany and Kellogg 40 ). A study comparing a general purpose CR (the MRE) with a lightweight ration designed for 30 d of continual use (the RLW-30) reported that the MRE sub-group lost BF alone, whereas the solders in the RLW-30 sub-group lost both FM and FFM. Consequently, those subsisting on the RLW-30 experienced decreases in isokinetic muscle strength and endurance, whereas the soldiers in the MRE sub-group did not. The RLW-30 sub-group also displayed greater decreases in aerobic capacity and reported more symptoms of impaired mental performance( Reference Askew, Munro and Sharp 52 ).
Limitations
Many of the studies included in this review did not report their procedures for measuring BW and BC in sufficient detail, thus indicating potential for measurement bias. In addition, many studies did not report that BW and/or BC was measured at a consistent time of day before and after CR use, and under standardised and well-controlled conditions (e.g. in the fasted, semi-nude, hydrated and voided state).
Limitations at the review level include language bias, as studies in languages other than English were excluded. A number of studies were identified which involved multiple study groups which received differing types of CR either with or without supplemental foods and/or permission to consume personal rations, however, reported the initial mean BW for all participants in all study groups as one figure. These studies were excluded if additional data could not be obtained from the authors, as it was not possible to accurately ascertain the BW changes in each sub-group across the study. In addition, during the database search, other missing data were not accessible for a number of relevant studies identified, thus the thirty studies included in this review do not reflect the entire breadth of BW and/or BC data which has been gathered during field and combat training involving the use of CR. In addition, this study did not obtain any data on the effect of repeated CR use with intervals of ad libitum fresh food access, as commonly occurs.
Implications for future research
To improve the reliability and validity of future research, more detailed reporting of study protocols is suggested, including inclusion and exclusion criteria, baseline demographics and methods of handling withdrawals. In addition, reporting of the procedures for measuring BW and BC should include details of the time of day of measurements and clarification of any factors which may introduce bias.
The largest daily ED were observed during very short-duration (3–7 d) and short-duration (8–10 d) CR use. There is limited published data on the cumulative effects of several bouts of short-duration CR use, which commonly includes periods of rest and recovery during more prolonged training courses and deployments. Future research should focus on assessing BW and BC changes during these periods. This will provide objective data as to whether BW and BC change to a similar degree as to during field and/or combat training. Consequently, this data can be used as a basis for research into feeding regimens which may assist in minimising the impact of missions on nutritional status, metabolic resilience and performance.
In addition, there is potential value in further exploring the use of supplemental food for both combat training and deployment scenarios, given the mixed results reported by the studies reviewed here. Although anecdotal evidence and one published report( Reference Siegel, Poole and Askew 46 ) suggests that soldiers carry appropriate types of personal rations during field training, it would be worthwhile to evaluate education that promotes the importance of high energy and nutrient dense items in mitigating deleterious levels of weight loss in the field.
With the exception of two female participants in the 4-d study undertaken by Margolis et al. ( Reference Margolis, Murphy and Martini 35 ), all of the research on BW and BC changes during CR use has been undertaken with males. With the commencement of females in combat roles, research is required to elucidate the magnitude of BW and BC changes they experience. It is possible that a lower level of BW and/or BC changes can be tolerated by females before health and/or performance decrements occur.
Recommendations
There is consistent high (II) level evidence of both positive and neutral quality that BW and BC changes occur during field activities involving CR use, and particularly where new types of CR are tested. Thus, BW should be measured where new types of CR are tested in all situations lasting 3 d and longer. BC should be measured in situations lasting 8 d and longer.
BW and overall nutritional status of military personnel should be stable before training and deployment involving CR use. Any intentional weight loss in the month immediately before CR use is not recommended, due to the potential for substantial reductions in BW during CR use.
There is high-level evidence (II) of neutral quality that there is potential for unnecessary reductions in the FFM in individuals with very low levels of BF (<10 %) during prolonged, low-intensity field activities. This suggests that personnel should have sufficient levels of BF to prevent unnecessary losses of FFM. Further research is required to clarify the satisfactory level of BF before CR use during differing types of missions.
There is also high-level (II) evidence of neutral quality showing that there is potential for rapid decreases in BW over 8–12 d of Infantry/Special Forces training courses involving near-continuous activities in the field. Thus, there is potential for impaired energy metabolism and performance as a result of depleted glycogen stores. Where practical, the BW of all personnel should be routinely monitored before and after similar activities of such duration. If an individual has rapidly lost >5 % of their BW, they should rest and recover with access to fresh foods, and not subsist solely on CR, until their BW returns to within 5 % of their initial BW. Where practical, including the use of methods appropriate to field environments, personnel undertaking Infantry and Special Forces activities in the field should have their BW measured after 14 d.
Nutrition education should be accessible by all military personnel undertaking particularly arduous field activities involving CR use, which may result in fast BW reductions. The messages should include the role of total EI, protein, carbohydrate and eating patterns in mitigating BW losses, adverse changes to BC, and in maintaining optimal energy metabolism during field activities.
As recommended by the IOM, any individuals who display particularly large losses of BW (>10 %) after a cumulative 30 d of CR use should rest and recover with access to fresh foods, and not subsist solely on CR, until their BW returns to within 5 % of their initial BW.
BC should also be monitored, where practical to do so, before and after more prolonged CR use (8+ d). Monitoring BF will provide an indication of whether an individual retains sufficient levels to aid the preservation of FFM. Any individuals who do not have BF levels of at least 10 % should not subsist solely on CR until their BF has reached optimal levels. Monitoring FFM may provide a means to evaluate whether soldiers are consuming protein at the recommended level of 1·5–2·0 g/kg per d and are maximally protected from FFM losses during field activities( Reference Pasiakos, Austin and Lieberman 67 ).
Conclusion
The data gathered from this systematic review process are the most comprehensive body of evidence to date regarding the effects of the continual use of CR for periods of 3–34 d on BW and/or BC (FM, FFM and/or %BF) in military personnel engaged in military training. The evidence suggests that the continual use of CR for durations within this time period leads to decreases in BW and often adverse alterations of BC, with the magnitude of losses depending largely on the intensity and duration of the mission being undertaken.
Given the arduous nature of combat training and deployment, and the deleterious impact that substantial decreases in body mass can have, where practicable, it is important to routinely monitor BW and BC during times of CR use during training and deployment, and take action to prevent performance decline. In particular, during specific types of Special Forces/Infantry activities, the rapidity of BW loss appears to have the potential to impair energy metabolism and consequently performance. Efforts should be made to closely monitor BW before and after such activities using field-appropriate methods, where practical.
The findings of this review suggest an importance of BC standards before prolonged and continual CR use (>7 d), including minimum levels of BF (>10 %). The findings also highlight the importance of minimising daily ED during training and deployment, to enhance metabolic and anthropometric resilience for the preservation of FFM and BF. Military nutrition research should continue to identify strategies to minimise daily ED and enhance energy metabolism during field training and deployment involving CR use, in order to mitigate the potential impact on the BW and BC of personnel.
Acknowledgements
The authors wish to thank their colleagues at Defence Science and Technology Group (DST Group) for providing support throughout the review process.
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
The review was conceived by B. A. B. Both authors contributed to formulating the PICOS, designing the review, conducting database and hand searches, screening titles and abstracts and full texts against the inclusion and exclusion criteria, extracting data from the included studies, assessing the included studies for risk of bias and rating their quality. B. A. B. assessed included studies for their level of evidence and E. C. T. critically reviewed the assessments. Both authors contributed to writing the introduction and critically reviewing it. E. C. T. wrote the methods and results and B. A. B. critically reviewed these sections. Both authors contributed to writing the discussion, limitations, implications for further research and conclusions sections and critically reviewing these sections. B. A. B. wrote the recommendations section and E. C. T. critically reviewed this section.
The authors declare that there are no conflicts of interest.
Supplementary materials
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114517000630






