



Introduction
Among university music student populations, the incidence of performance-related musculoskeletal disorders has been shown to be high, ranging from 62% to 88% (Árnason, Árnason, Briem, Reference ÁRNASON, ÁRNASON and BRIEM2014; Ingle, Reference INGLE2014), and this has been shown to be nearly twice as high as that of their peers studying towards academic degrees in subjects other than music (Kok et al., Reference KOK, NELISSEN and HUISSTEDE2015). Despite this, music students have been found to exhibit poor responsibility for self-health (Kreutz et al., Reference KREUTZ, GINSBORG and WILLIAMON2008; Ginsborg et al., Reference GINSBORG, KREUTZ, THOMAS and WILLIAMON2009; Perkins et al., Reference PERKINS2017), even while facing extremely high physical and psychological performance demands in a highly competitive higher education environment as they prepare for the professional world of music performance.
There appear to be several reasons to explain this apparent paradox of disengagement with health education. First, research shows that first-year students already show a high prevalence of prior music performance-related pain and injury at the entry point of tertiary courses (Brandfonbrener, Reference BRANDFONBRENER2009; Ballenberger et al., Reference BALLENBERGER, MÖLLER and ZALPOUR2018). Second, in the first year of tertiary training, the hours students spend practising and performing usually dramatically increases, with studies showing a subsequent deterioration in the health of students between the first and second year of university-level studies (Zander et al., Reference ZANDER, VOLTMER and SPAHN2010). Problems are not only physical, with first-year music students shown to face a high risk of developing mental health issues (Hildebrandt et al., Reference HILDEBRANDT, NÜBLING and CANDIA2012).
Music students, however, are often unaware of the health risks they face and lack effective strategies to help them to engage in health-promoting behaviours (Williamon & Thompson, Reference WILLIAMON and THOMPSON2006; Rickert et al., Reference RICKERT, BARRETT and ACKERMANN2015; Perkins et al., Reference PERKINS2017; Araújo et al., Reference ARAÚJO2020; Baadjou et al., Reference BAADJOU2019). Environmental factors, such as accessibility and availability of resources, and the contextual relevance of a given intervention strategy have been shown to be important in informing and shaping population-specific health behaviours and health literacy (McCormack et al., Reference MCCORMACK2004; McKenna et al., Reference MCKENNA, SIXSMITH and BARRY2018). Since music learning often begins in childhood, when habits and attitudes are formed, currently there is a significant imperative to address health education for student musicians (Young Musicians Health and Wellbeing Think Tank, 2022).
Traditionally, health information has not been integrated into the teaching of music performance at tertiary music institutions nor in pre-tertiary music teaching (Clark & Lisboa, Reference CLARK and LISBOA2013a). This has remained in stark contrast to other high-performance domains such as sports, despite decades-long calls for change (Quarrier Reference QUARRIER1993; Matei et al., Reference MATEI, BROAD, GOLDBART and GINSBORG2018; Fortington & Hart, Reference FORTINGTON, HART, Robertson and Maffulli2021). Worldwide, there is an apparent lack of accessible, evidence-based programmes that provide health education specific to the needs of musicians that may help music students to better manage the health risks they face (Wijsman & Ackermann, 2018). A majority of university students use the internet to access health information (Montagni, et al., Reference MONTAGNI2018); hence, digital health education has the potential to improve health and well-being for university-level music student populations.
When designing online education and health interventions for university-aged students, a formative evaluation process can assist in ensuring that such programmes are appropriately targeted for the specific group of students in the context best related to their studies (McKenna et al., Reference MCKENNA, SIXSMITH and BARRY2017; Montagni, et al., Reference MONTAGNI, LANGLOIS, WITTWER and TZOURIO2017). As part of that formative evaluation, a survey of Australian tertiary music students was carried out in 2010 to understand their attitudes and perceptions towards key health topics to inform the content of an online musicians’ eHealth programme: Sound Performers (Wijsman, Reference WIJSMAN2012).
Initially, the analysis of survey results focused on data that related primarily to the development of the online programme content, such as topic and delivery preferences. Following a three-year trial of the course, the process and outcome evaluations were carried out to refine and modify the presentation of original course content, such as simplifying health language and inclusion of more multimedia material and examples of practical applications of course concepts. Part of this process involved reviewing and reflecting on the variability of student engagement with different health topics that was evident in the trial of the health education programme. For example, while over 60% of students in the trial completed the programme, only 26% engaged with 100% of the programme topics. A majority of students (75%) engaged with the module, Body of Work, which focused on the physical characteristics of musical performers, while only 41% were interested in Performance Biomechanics, which focused on performance-related movement specifically for musicians. The topic that interested students the most was Muscles (78%), while paradoxically the topic that interested them least was the Practice Journal (43%). This led us to return to the dataset and undertake a more comprehensive analysis, taking into consideration how personal experience with physical and psychological health issues might be correlated with students’ answers concerning health topic preferences. Subsequent analysis of the entire dataset revealed important insights into the multiple factors that may help to explain this variability in music students’ attitudes towards health education topics.
This paper presents the survey design, analysis and results that reveal how this sample of music students’ personal health profiles and history may have influenced their attitudes and ratings of health education topics. The results have broader implications for designing effective health promotion strategies for tertiary music students and integration of musicians’ health education into the tertiary music curriculum.
Methods
The Australian Music Students’ Health Survey
The Australian Music Students Health Survey (AMSHS) was purpose-designed to assess students’ perceptions of the importance of a range of health topics as part of their education in Australian tertiary music institutions, as well as how this related to their performance health status. The broad topic areas the survey explored included anatomy, breathing, posture, injury prevention and management, performance biomechanics, psychological aspects of performance and exercise and nutrition. Additionally, their current and past state of health and possible correlations between these and their perceptions were investigated. The cross-sectional questionnaire developed for the AMSHS was a modified version of the performance health survey developed by the Australian Research Council-funded Sound Practice project, led by one of the co-authors (BA), studying the occupational health of Australia’s professional orchestral musicians (Ackermann et al., Reference ACKERMANN, KENNY, DRISCOLL and O’BRIEN2017).
The goal of the AMSHS was to explore in detail student attitudes towards these health topics, how important they perceived the integration of these to be within their courses of study and their willingness to attend classes. The health topics included in the survey were developed at the initial stage of the project by one of the authors (BA) based on extensive experience in providing musicians’ health education, as well as an extensive literature review of existing health education interventions for musicians. Additional consultation with the project’s 11-member reference group, comprised of an interdisciplinary mix of music educators, musicians’ health researchers and health experts, ensured that topics represented key health education priorities for music students (Wijsman, Reference WIJSMAN2012).
The survey questions used an 11-point Likert scale for responses, ranging from 0, representing no importance of the topic at all in relation to performance, to a maximum of 10, representing the topic would have the greatest possible effect on performance. Cross-sectional data regarding the self-reported physical and psychological health issues of this sample of student musicians were also collected to give a snapshot of their past and present health status. The survey data were analysed to probe more deeply the relationship between music student attitudes, health status, experiences and behaviours to assess how these may influence their engagement with health education.
Demographic information of participants
Demographic information was gathered for participants, including age, sex (male or female, reflecting data collection practices at the time), the length of time they had been learning, primary instrument and additional instruments (including voice), and their practice and performance habits (Table 1).
Table 1. Participant Demographic Data and Hours Practised (All Instruments)

Table 2. Pain Status * Psychological Status Cross-Tabulation

Following approval from the Human Research Ethics Committee of the University of Western Australia (UWA),Footnote 1 the survey was administered at three Australian tertiary schools of music. All participants completed a paper questionnaire and gave written informed consent. A total of 276 participants who completed the survey were recruited from three institutions: the School of Music at UWA (N = 80), the West Australian Academy of Performing Arts at Edith Cowan University (ECU) (N = 176) and the Sydney Conservatorium of Music (Sydney) (N = 20). At UWA and ECU, students were recruited through face-to-face contact in performance classes for a variety of instrument groups early in the academic year. Response rates at participating institutions among students who attended classes on the days in which the survey was distributed ranged between 92% (ECU) and 99% (UWA). While 74% of the students surveyed were in the first or second year of their studies (N = 199), this number represents approximately 34% (ECU) and 66% (UWA), respectively, of the total population of students enrolled in a performance studies unit at these institutions on the date of the survey.Footnote 2 At Sydney, students were recruited via personal contact by the Sydney-based project assistant, and though no data was available on total Sydney enrolment numbers for this study, this represents only a negligible percentage of students at this large tertiary music institution. Data for eight respondents who didn’t sign the informed consent form on the paper questionnaire, or who either did not answer questions about their current/past performance health or whose answers were unclear, were subsequently excluded. The data of 268 student musicians were included for the purposes of this study.
Instruments played and weekly time spent on instruments
The students surveyed were involved in a range of Western musical styles: classical, jazz and contemporary/popular. There was a fairly even number of responses from all instrument groups represented, including voice, keyboard, wind, brass, guitar, bowed strings and percussion. For the spread of participation across different instrument groups, see Table 1. Most students indicated that they had studied a second instrument (N = 178, 66.7%), of whom 88 (32.8%) were continuing with the second instrument at the time of the survey. In many cases, the reported second instrument had been played for longer than the first instrument, typically violin or piano, indicating that a change in instrument had occurred later in the musician’s training. 87 students (32.5%) also reported currently practising and performing on a third instrument. Students spent on average 26.3 h/week practising and performing on all instruments, of which an average of 17.5 h was on their primary instrument (Table 1).
Statistical analysis
IBM SPSS Statistics Version 24 was used for all statistical analysis. The distribution of data was tested for normality using Shapiro–Wilk test (Royston’s method) and were found to be non-normally distributed. Therefore, non-parametric tests were used. The Mann–Whitney U test for non-parametric data was used to test differences in the responses between sexes. When more than two groups were compared (i.e. pain status or psychological distress status: never experienced, only previous experience, both previous and current experience, current only experience) (Table 2), Kruskal–Wallis one-way Analysis of Variance (ANOVA) was used to compare the responses, and when significant ANOVA results were found, Mann–Whitney U test was used to identify specific differences between pairs of groups. Friedman’s ANOVA was used to compare the ratings among different topics, and when significant ANOVA results were found, Wilcoxon’s paired test was used to identify specific differences between pairs of topics. Spearman’s Rho was used to investigate associations between ratings and playing-related variables (practice and playing hours as well as ratings of perceived exertion during playing). An alpha level of 0.05 was set for all statistical tests.
Results
Effect of sex
Results of the Mann–Whitney U test analysis indicated that females rated understanding posture (p = 0.022), breathing (p = 0.002), nutrition (p = 0.007) and music performance anxiety (p = 0.003) as more important to performance than males. There were no differences between the ratings of males and females for all other topics (p > 0.270). Females indicated a greater likelihood of attending classes on anatomy (p = 0.001), posture (p = 0.001), breathing function (p < 0.001), nutrition (p = 0.006), injury prevention (p = 0.041) and music performance anxiety (p < 0.001). There were no differences between the rating of males and females on the likelihood of attending classes on body processes (p = 0.378), exercise and stretching (p = 0.082) and general physical health (p = 0.119).
Credit versus no-credit subject – likelihood of attendance
Using an 11-point Likert scale (0 = not likely, 10 = greatest likelihood), students were asked to indicate how likely they would be to attend performance health classes that were offered formally for credit and how likely they were to attend such classes as a non-credited option. Perhaps unsurprisingly, students indicated they would be most likely to attend classes if this was part of their credited course work with an average score of 8.10 compared to no credit with an average score of 6.81 (p < 0.001).
Rating of importance of topic information and likelihood of attending classes on a topic
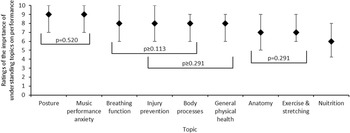
In general, students placed a high value on most topics, with the median of the lowest score for nutrition at 6.0 and the highest score for posture and music performance anxiety both at 9.0. This is summarised in Figure 1.

Figure 1. The median (± interquartile range) of the rating of perceived importance of different topics on playing performance ranked from most important to least important. Topics with similar ratings were grouped, while all other topics were significantly different to each other (p ≤ 0.036).
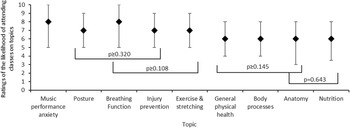
Students indicated a lower likelihood of actually attending classes, with the median of the lowest score for nutrition and anatomy at 6.0 and the highest score for music performance anxiety at 8.0. This is summarised in Figure 2.

Figure 2. The median (± interquartile range) of the rating of the likelihood of attending classes on the different topics ranked from most likely to least likely. Topics with similar ratings were grouped, while all other topics were significantly different to each other (p ≤ 0.046).
The final topics included in the eHealth curriculum Sound Performers are summarised in Appendix 1.
Physical health issues
There were 96 (36%) students who responded positively to the question: Do you suffer current pain or injury related to playing your instrument (i.e. pain or injury at present) that has been present for at least the past seven days? This subgroup included 60 females (63%), 30 males (31%) and 2 students whose gender was unspecified (2%). Of these students, the majority reported intermittent symptoms (67%) with the rest reporting constant symptoms. The average intensity of symptoms on an 11-point Likert scale (0 = no pain, 10 = severe pain) was 5/10 (range from 1 to 9), and 81% of these felt that symptoms were caused by playing (N = 78) and 5 were unsure, with 73% reporting that symptoms affected their playing. The majority of respondents (48%) reported the current pain had been present for >12 weeks (N = 46), with 20% reporting pain lasting between 4 and 12 weeks (N = 29) and the rest reporting symptoms lasting less than 4 weeks.
Psychological health issues
In response to the question: Do you suffer CURRENT psychological stress such as depression, anxiety or ‘stage fright’ related to playing your instrument that has been present for at least the past seven days?, 112 students responded affirmatively (41%). Of these students, the average effect of the severity of symptoms on an 11-point Likert scale (0 = no effect of symptoms, 10 = greatest possible effect) was 6 (with a range from 1 to 10), with 13 students (11.5%) reporting alarmingly high severity of effects scores from 9 to 10. In relation to frequency of symptoms, again on an 11-point Likert Scale (0 = no symptoms 10 = constantly present), the average score was 6 (range from 1 to 10), with 13 students (11.5%) reporting psychological symptoms were constantly present with a score of 10.
When these results were cross-tabulated, a correlation emerged between physical pain/injury and psychological stress, with 59% of students who reported past and current playing-related physical pain also reporting past and current performance-related psychological stress (Table 2).
Table 3. The Median and Interquartile Range of the Ratings of the Importance of Understanding and the Likelihood of Attending Various Topics for Different Pain Status Groups

Note: The p value provided is for Kruskal–Wallis one-way ANOVA.
* Indicates significantly different to having never experienced pain.
† indicates significantly different to having experienced previous pain only.
‡ Indicates significantly different to having experienced previous and current pain.
Effect of pain and psychological factors on perceived topic importance
Different pain status led to significant differences in the rating of the importance of understanding anatomy (p = 0.007), body processes (p = 0.028), injury prevention (p = 0.030) and the likelihood of attending body processes (p = 0.023), exercise and stretching (p = 0.001) and injury prevention (p = 0.003) with no difference in other topics (p > 0.063) (see Table 3).
Table 4. The Median and Interquartile Range of the Ratings of the Importance of Understanding and the Likelihood of Attending Various Topics for Different Psychological Status Groups

Note: The p value provided is for Kruskal–Wallis one-way ANOVA.
* indicates significantly different to having never experienced psychological distress.
† Indicates significantly different to having experienced previous psychological distress only.
In contrast, psychological stress status led to significant differences in the rating of understanding of music performance anxiety (p = 0.005) and the likelihood of attending classes on breathing function (p = 0.037), injury prevention (p = 0.047) and music performance anxiety classes (p < 0.001) with no difference in other topics (p > 0.098) (see Table 4). Psychological stress status did not affect the rating of the importance of understanding how the body works in relation to performing on an instrument (p = 0.223).
Finally, an analysis was conducted to evaluate whether the amount of hours students played and their self-perceived rating of average daily practice or playing effort had any association with their perceived importance or likelihood of attending health education. This is summarised in Table 5 and 6. Students’ interest in exercise and stretching and general health was weakly correlated with the number of hours they spent practising and performing on their primary instrument (r = 0.29 and r = 0.24; p < 0.001), and exercise and stretching were also weakly correlated with their rating of perceived exertion after an average day’s practice (r = 0.20; p = 0.003).
Table 5. Association Between Playing Hours and the Importance of Understanding Topics. The r Values Provided Are Spearman’s Rho

Note: Bold indicate significant Spearman’s Rho values.
Table 6. Association Between Playing Hours and the Likelihood of Attending Class. The r Values Provided Are Spearman’s Rho

Note: Bold indicate significant Spearman’s Rho values.
Discussion
The goal of the prospective programme design was to provide a resource to help educate and inform students on a broad range of topics to help prevent and mitigate health issues, supporting performance optimisation in the process. The Australian Music Students Health Survey and analysis of its data were valuable for refining the content and method of delivery of draft topics for the resulting online musicians’ health course, Sound Performers, in the formative evaluation phase. The survey results showed higher median scores for all topics that may appear more obviously relevant to students, such as posture. Topics that might have been perceived by students as less relevant to music performance, such as nutrition, rated relatively poorly. This accords with other research on a health education intervention in a British tertiary music school in which students prioritised health topics that they perceive as directly related to practising and performing on their instrument over those they may have perceived as less relevant (Matei et al., Reference MATEI, BROAD, GOLDBART and GINSBORG2018).
While a majority of the students surveyed responded that both understanding about performance health and receiving instruction about health topics as part of their course were important, our analysis of the data revealed some concerning findings. Past history of performance-related physical or psychological health issues was influential in determining the ratings for particular topics. Students with a history of psychological or physical issues showed a clear preference for topics they perceived as related to their past experience of a performance-related health issue (PRHI). For example, those with a history of psychological health issues showed a preference for topics such as music performance anxiety and breathing function, while students with a history of pain prioritised topics such as understanding anatomy and body processes, injury prevention and exercise and stretching. This suggests that the adverse impact of a PRHI on their ability to perform was more influential on students’ greater interest in accessing health-specific types of information than a desire to increase the breadth and depth of their performance health knowledge. This reactive, rather than preventive, behaviour suggests that students only become aware of such health risks once they have experienced a PRHI and may be ignorant of the physical and psychological demands they face, as observed in the past literature (Waters, Reference WATERS2019). The implication of this is that, at a minimum, early stages of tertiary music education should inform students about the well-identified risks associated with musical performance as well as provide effective practicable strategies to best mitigate these factors.
It is encouraging that students in this survey accorded relatively high scores to the importance of understanding most of the health topics; however, their scoring of the likelihood of attending such classes was rated somewhat lower for all areas, with the exception of music performance anxiety, for which the median scores were comparable (Figures 1 and 2). It also appears that while the importance of health is acknowledged by students, they do not always wish to commit time to further learning about these topics, unless they are playing a greater number of hours. It is notable that a positive correlation was observed between the total hours of practice and performance and the rating of the importance of understanding and attending classes on some topics that were planned for the anticipated musicians’ health education programme. It is possible these music students perceived that they may benefit from learning strategies that would support their relatively more intensive playing demands or that they were already experiencing PRHIs that made particular topics more relevant to them.
Some authors propose that preventative health programmes for musicians should be targeted to meet the specific varying needs of music students (Spahn et al., Reference SPAHN, NUSSECK and ZANDER2014), while other recommendations suggest that all relevant health topics for musicians should be covered in any musicians’ health programme (NASM, 2020). Our study reported a retrospective attitude on the part of students, where they showed interest in health topics based on past experience rather than awareness of their future needs. Therefore, in promoting awareness among Australian music students of the relevance of all health education to them, the music institutions where they study will be better positioned to exercise their primary duty of care in ‘providing adequate training, information and instruction to ensure students and staff are safe from injury and risks to health’ (Safe Work Australia, 2018).
The results of this survey show a lower prevalence of pain/injury or psychological problems in this group of music students than those in some other studies (Kreutz et al., Reference KREUTZ, GINSBORG and WILLIAMON2008; Brandfonbrener, Reference BRANDFONBRENER2009; Ballenberger et al., Reference BALLENBERGER, MÖLLER and ZALPOUR2018), and this sample also reported lower injury rates than more advanced Australian students or professional musicians (Ackermann et al., Reference ACKERMANN, DRISCOLL and KENNY2012; Rickert et al., Reference RICKERT, BARRETT and ACKERMANN2015; Ingle, Reference INGLE2014). This perhaps reflects higher workloads and pressured playing environments for these more experienced musician populations in Australia (Fry Reference FRY1987) and internationally (Quarrier Reference QUARRIER1993). This survey was administered prior to the events of the coronavirus disease 2019 pandemic, and therefore, the results do not reflect any impact of the pandemic on the health status or attitudes of this cohort of Australian music students.
In our sample, 50% of the students who participated were just starting their first year of a tertiary music course (N = 134), and this may have influenced the lower number of reported issues, before performance demands increased and intensified, which typically occurs during the first year of a musician’s training (Ballenberger et al., Reference BALLENBERGER, MÖLLER and ZALPOUR2018). However, these statistics point to the experience of physical injury and psychological stress in a significant proportion of this Australian student musician population. Interestingly, psychological PRHIs were more prevalent than physical PRHIs in this sample of music students, with a majority of respondents already reporting symptoms such as music performance anxiety. This accords with research on broader student populations showing increased mental health issues between the first and second years of study (Zander et al., Reference ZANDER, VOLTMER and SPAHN2010; Hildebrandt et al., Reference HILDEBRANDT, NÜBLING and CANDIA2012; Pedrelli et al., Reference PEDRELLI2015). The results from this study highlight the vulnerability of young students at this early point in their music studies and the vital importance of providing them with information and guidance early so that they can manage the risks they face as they proceed through their tertiary music studies.
Music institutions lag well behind other elite performance disciplines, such as sport and dance, in delivering education that embeds health promotion and injury prevention strategies using tailored educational models effectively for their music student populations (Clark et al., Reference CLARK, WILLIAMON and REDDING2013b, Cardinal et al., Reference CARDINAL, ROGERS and CARDINAL2020). More than 20 years ago, the National Association of Schools of Music (NASM) in the USA recommended that music administrators and teachers cannot, and must not, attempt to serve as health professionals, but they should have a basic understanding of health maintenance issues sufficient to inform their work as teachers and mentors to their students (NASM, 1991). For nearly 40 years, it has been known that there are risks associated with the education and training of musicians and a relatively large amount of research on this topic has appeared in Australia and worldwide over the past two decades. However, music education organisations in Australia have yet to take their role in providing a safe training environment seriously. Even though there has been a growth in resources and applied information to improve musicians’ health, the provision of substantive health information for tertiary music students by Australian universities has only marginally improved. Only one Australian tertiary institution currently provides musicians’ health education to its first-year music students as compulsory, formal course content, with others merely providing an induction session to incoming students, web pages and links to external information or elective units including performance health topics, some of which are embedded within more generic elective units of study. At one Australian institution, formal health education for musicians is reserved for graduate-level study, which we would argue is far too late in a musician’s education. The results of the current study suggest that undergraduate student musicians – especially first-year students – are not well-equipped to take responsibility for their own performance health and that music students are less likely to seek and access vital health information if it is not required as part of their studies. This is supported by the results of previous studies of Australian music students’ experience of PRHIs and their attitudes towards performance health (Ingle, Reference INGLE2014; Rickert et al., Reference RICKERT, BARRETT and ACKERMANN2015; Waters, Reference WATERS2019, Reference WATERS2020).
Music students have been shown to be vulnerable to performance health risk factors that they don’t expect nor understand (Perkins et al., Reference PERKINS2017; Waters, Reference WATERS2019). This may reflect low levels of health literacy in musicians concerning the health risks they face as performers (Baadjou et al., Reference BAADJOU2019). Health literacy is recognised by the World Health Organization (WHO) as essential for promoting good health behaviours (WHO), and high levels of health literacy empower people to ‘access, understand, appraise, and apply health information in order to make judgments and take decisions in everyday life concerning healthcare, disease prevention and health promotion to maintain or improve quality of life during the life course’ (Sørensen et al., Reference SØRENSEN2012, p. 3). However, the role of communities, organisations and governments in implementing effective strategies that promote individuals’ health literacy is also crucial (WHO 2022; Larsen et al. Reference LARSEN2015). Music education providers need to be proactive in developing and implementing effective health promotion strategies within their education programmes that will enable their students to access, understand, appraise and apply this information in their music practice and performance, thereby reducing their risk of a PRHI. As in sports training, this may involve a combination of engineering (e.g. ergonomic equipment, training environment, etc.), education (involving both teachers and students) and enforcement of health promotion policies (organisations and institutions) (Fortington & Hart, Reference FORTINGTON, HART, Robertson and Maffulli2021). Well-tested models of performance education, which integrate effective health promotion and injury prevention strategies into the curriculum, have also long existed in dance training (Cardinal et al., Reference CARDINAL, ROGERS and CARDINAL2020). Exploring the applicability of such models could help to reshape the delivery of music education and the content of the music education curriculum, even at the pre-tertiary level, to better support musicians’ health as well as career sustainability.
The top-down leadership responsibility for promoting healthy music teaching, performance and practice ultimately rests with the managers of music education organisations and music teachers, and there is an imperative to develop policies that ensure a culture of safety for vulnerable music students. The evidence from the current study suggests that the passive approach to educating students about music performance health taken by many tertiary music institutions in Australia needs to change. The authors of a recent study undertaken in the United Kingdom call for a systematic response to the available evidence and the involvement of managers and teachers to support students in not only understanding the importance of health education for optimising music performance and practice but in guiding their behaviour change to achieve better health outcomes (Matei et al., Reference MATEI, BROAD, GOLDBART and GINSBORG2018). Other research has similarly advocated for cultural change and shared responsibility at an institutional level as necessary prerequisites to improve music students’ health-promoting behaviours, such as investing time and resources in this vital, but neglected, aspect of the curriculum (Perkins et al., Reference PERKINS2017; Araújo et al Reference ARAÚJO2020; Baadjou et al., Reference BAADJOU2021). As in other performance domains, music education providers should provide comprehensive, evidence-based health information, with collaborative input from experts, as a foundational component of their students’ education, given the well-known very high physical and psychological demands intrinsic to music performance (Baadjou et al., Reference BAADJOU2021).
Health promotion for tertiary music students will remain a challenge if their awareness or interest in healthy behaviours occurs only as a consequence of negative experiences, as is suggested by the results of this research, rather than being seen as an essential strategy to prevent adverse health conditions from occurring in the first place and a pathway to performance optimisation. It is imperative to achieve the translation of health education into effective, health behaviour change for music students. This will support student musicians’ capacity to develop healthy, optimal and sustainable performance careers.
Funding statement
This project was supported by an Australian Government Office of Learning and Teaching Priority Projects Grant, PP9-1306 (2009–2012).
Competing interests
There are no conflicting interests to declare.
Appendix 1








 Open access
Open access