



Background
Digital addiction is an emerging global concern that refers to the compulsive and excessive use of digital devices, such as smartphones, computers and gaming consoles, which disrupt daily functioning and negatively affect well-being. This form of behavioural addiction is particularly prevalent among adolescents, who are more vulnerable because of their developmental stage and the increasing exposure to and integration of technology into everyday life. Digital addiction is manifest in an inability to restrain the use of digital devices and can lead to significant psychological, social and academic difficulties. Reference Kuss and Griffiths1 The rapid proliferation and penetration of digital technology have facilitated the development of addictive behaviours and prompted the critical need to understand and address this problem, especially within specific cultural contexts such as Bangladesh.
Digital device dependency, including smartphone addiction, gaming addiction and internet addiction, represents specific forms of digital addiction that have been extensively studied because of their widespread prevalence. Smartphone addiction involves the excessive use of mobile devices to the point where it interferes with everyday activities while facilitating the emergence of anxiety, depression and sleep disturbances. Reference Elhai, Levine and Hall2 Gaming addiction is another critical aspect of such a spectrum, whereby individuals, particularly adolescents, become engrossed in video games, leading to social isolation, poor academic performance and, in extreme cases, gaming disorder as recognised by the World Health Organization. 3 Internet addiction encompasses a broader range of online activities from social networking to compulsive browsing, resulting in significant impairments in personal, academic and social domains. Reference Kuss and Griffiths1 These forms of digital dependency highlight the diverse nature of digital addiction and underscore the need for comprehensive measures to screen, detect and manage these behaviours.
Literature review
Recent research has significantly advanced our understanding of digital addiction, focusing on various subtypes, such as smartphone, gaming and internet addiction. A recent meta-analysis revealed that 27% of people are addicted to smartphones, 14.2% to the internet and 6% to gaming. Reference Meng, Cheng, Li, Yang, Zheng and Chang4 Studies on smartphone addiction, particularly among adolescents, have shown prevalence rates ranging from 4.3% to 70%. Reference de Freitas, Gaíva, Bernardino and Diogo5 For instance, a study among Indian adolescents found that 64.6% were addicted to smartphones, with key drivers including urban residence, higher parental education, longer smartphone use and higher socioeconomic status. Reference Yogesh, Ladani and Parmar6 Among Filipino adolescents, a study found a 62.6% prevalence rate of smartphone addiction, which was negatively correlated with health-related quality of life. Reference Buctot, Kim and Kim7 In addition, usage patterns and psychological and behavioural factors were significantly found to be associated with smartphone addiction. Reference de Freitas, Gaíva, Bernardino and Diogo5
Gaming addiction has also been widely studied. A meta-analysis suggests that 4.6% of adolescents met the criteria for an internet gaming disorder, with higher rates in males. Reference Fam8 In China, 17% of adolescents were identified as suffering from internet gaming addiction, with significant associations found with neuroticism, conscientiousness, daily gaming time, having one or two long-term game partners, being male, relationship status and motivation for coping, sensation seeking and escaping. Reference Liao, Huang, Huang, Tan, Shao and Fang9 Moreover, gamers often experience higher levels of loneliness and psychological distress. Reference André, Broman, Håkansson and Claesdotter-Knutsson10 These findings suggest that gaming addiction is closely linked to several factors, including gender, family environment and psychological well-being. Internet addiction is another widespread form of digital dependency. A meta-analysis reported a global prevalence of 13.62% for excessive internet users, and internet addiction has been associated with various psychological, school-related and environmental factors and psychosocial issues. Reference Kuss and Griffiths1,Reference Fumero, Marrero, Voltes and Peñate11
Rationale for conducting the study
In Bangladesh, the issue of digital addiction has gained increasing attention, reflecting global trends. Several studies have illuminated the extent of this phenomenon and its impact on various aspects of life among different groups. For instance, internet addiction was reported in 27.1% of young adults using the Young Internet Addiction Test, a validated measure specifically assessing internet addiction through a comprehensive assessment of factors such as time spent online and interference with daily life, with significant risk factors including poor family relationships, lack of physical activity, cigarette smoking and excessive internet use. Reference Hassan, Alam, Wahab and Hawlader12 Research on gaming addiction among university students using the Game Addiction Scale Reference Sayeed, Rasel, Habibullah and Hossain13 which assesses gaming behaviours related to preoccupation, tolerance and withdrawal, revealing higher addictive behaviours among males, with excessive gaming leading to health issues such as headaches and ear discomfort. Reference Sayeed, Rasel, Habibullah and Hossain13 A study among 2157 university entrance test-takers found that 33.1% had digital addiction, using the Digital Addiction Scale developed for assessing general digital addiction, covering behaviours across various digital devices and activities. Reference Al-Mamun, Hasan, Mostofa, Akther, Mashruba and Arif14 Bangladeshi adolescents have also shown high levels of gadget addiction (46.9%) using the Problematic Media Use Measure Short Form, reporting significant associations with cognitive function, loneliness and anxiety. Reference Liza, Iktidar, Roy, Jallow, Chowdhury and Tabassum15 Another study reported that Bangladeshi adolescents spent an average of 6.67 h on the internet and 3.86 h on gaming daily. Reference Islam, Jahan, Amin Dewan, Pontes, Nahar Koly and Sikder16
These studies demonstrate the pressing need for culturally relevant tools that can accurately screen and assess digital addiction, particularly among teenagers. While specific forms of digital addiction, such as internet and gaming addictions, have been validated in Bangladesh, there remains a gap in the form of a validated tool specifically designed for general digital addiction in the teenager population. Previous studies have highlighted significant levels of digital addiction among various groups, including university entrance test-takers and young adults, with associated psychological and physical health impacts. Previous psychometric studies among Bangladeshi adolescents have included the Internet Gaming Disorder Scale- Short Form and Gaming Disorder Test among small adolescent samples (n = 428), Reference Islam, Jahan, Amin Dewan, Pontes, Nahar Koly and Sikder16 the Young Internet Addiction Test among university students (n = 177) Reference Karim and Nigar17 and the Digital Addiction Scale among prospective university students. Reference Al-Mamun, Hasan, Mostofa, Akther, Mashruba and Arif14
However, existing tools primarily focus on specific platforms (e.g. gaming, social media) or are designed for adult populations or university students, leaving a gap for validated measures tailored to teenagers. The Digital Addiction Scale for Teenagers (DAST) is a ten-item scale originally developed by Seema et al Reference Seema, Heidmets, Konstabel and Varik-Maasik18 to assess general digital addiction among Estonian teenagers, capturing behaviours across multiple digital platforms. It was initially validated among Estonian students and demonstrated strong internal consistency (Cronbach’s α 0.85) and a robust two-factor structure comprising digital attachment (items 1–6) and compulsive use (items 7–10). Reference Seema, Heidmets, Konstabel and Varik-Maasik18 Further psychometric evaluation in a Turkish sample examined the scale’s structure, with findings favouring a single-factor model, highlighting possible cultural variations in digital addiction levels. Reference Çelik, Tunç, Candemir, Kapkin İçen and Açar19
Although other validated tools exist in Bangladeshi populations, they focus on specific behaviours, such as gaming, social media addiction or internet addiction, rather than the broader spectrum of general digital addiction. The DAST addresses this gap by evaluating tolerance, withdrawal, fear of missing out and compulsive use, which are common across various digital activities. Moreover, it is specifically designed for teenagers, making it more relevant for understanding digital addiction in this age group. Hence, the present study aims to validate the DAST for use among Bangladeshi teenagers, examining its reliability, factor structure and convergent validity. In addition, identifying significant predictors of digital addiction will help one to understand the underlying causes and develop effective prevention and intervention strategies. This culturally adapted and validated tool will serve as a valuable resource for policymakers and healthcare providers, supporting targeted preventive actions and policies to address digital addiction among Bangladeshi adolescents.
Theoretical framework and hypotheses
This study employs the biopsychosocial model as a conceptual framework to understand and interpret the associated factors of digital addiction among adolescents, acknowledging how biological, psychological and social factors might contribute to addiction risk. However, it is important to note that this study is not introducing a new theoretical framework for the DAST itself, rather investigating how these factors are related to digital addiction. Biological factors include age and gender, recognising that younger adolescents and gender differences may influence addiction patterns. Reference Fam8,Reference Al-Mamun, Hasan, Mostofa, Akther, Mashruba and Arif14 Psychological factors encompass depression, anxiety and insomnia, suggesting that higher levels of these conditions may drive adolescents to excessive digital device use as a coping mechanism. Reference Al-Mamun, Hasan, Mostofa, Akther, Mashruba and Arif14,Reference Liza, Iktidar, Roy, Jallow, Chowdhury and Tabassum15,Reference Al-Mamun, Mamun, Prodhan, Muktarul, Griffiths and Muhit20 Social factors involve academic grade, location and the type of digital device used, highlighting how academic pressures, urban versus rural settings and specific devices (television, computer, smartphone, gaming console) contribute to addiction risk. Reference Pagano, Bacaro and Crocetti21 This approach provides a nuanced understanding of digital addiction, facilitating the development of targeted interventions and support strategies for affected adolescents. The current study proposes the following hypotheses:
-
(a) the Bangla Digital Addiction Scale for Teenagers (Bangla DAST) would demonstrate good psychometric properties (reliability and validity);
-
(b) age, gender, grade, location and types of digital devices used would show significantly different levels of digital addiction;
-
(c) depression, anxiety and insomnia would significantly associate with digital addiction.
Method
Study design, participants and procedure
This cross-sectional study, the MeLiSA study, was conducted among adolescents in the Shahzadpur sub-district of Sirajganj in November 2022. A two-stage stratified cluster sampling technique was employed. In the first stage, seven schools were randomly selected, with three from urban areas and four from rural areas, stratified by geographical location. In the second stage, students from the seventh, eighth and ninth grades at each selected school were randomly invited to participate.
Approval for data collection was obtained from school authorities and written informed consent forms were distributed to students for their parents or guardians to review and approve. During data collection, both the research team and class teachers were present in each classroom to assist students and answer any questions related to the questionnaire. The study included students who met the following criteria: (a) being present in the classroom during the survey period and (b) being enrolled in the seventh, eighth or ninth grade (i.e. ages 12–17 years). Students were excluded if they did not provide consent, had physical or intellectual disabilities or were absent at the time of the study. The response rate was 97.7% in the present study.
Measures
Demographic and digital device-related factors
The study gathered various sociodemographic data from the participants, including age, gender (male or female), grade (seventh, eighth or ninth) and location (urban or rural). In addition, information related to digital device usage was collected, such as whether participants slept alone in a room, watched television, used a smartphone, used a computer or used a gaming device. These questions were answered with a binary (yes/no) response.
Digital Addiction Scale for Teenagers
The DAST was assessed using a scale initially developed and validated for teenagers. Reference Seema, Heidmets, Konstabel and Varik-Maasik18 The scale consists of ten items, such as ‘I’m grumpy if I can’t use digital devices’ rated on a 7-point Likert scale ranging from ‘never’ to ‘very often’. The total score ranges from 7 to 70, with higher scores indicating higher levels of digital addiction. In this study, the reliability of the scale was assessed using Cronbach’s α. Previously, the scale demonstrated good reliability and validity. Reference Seema, Heidmets, Konstabel and Varik-Maasik18 For the present study, the scale was translated and validated following a forward and backward translation procedure outlined by Beaton et al. Reference Beaton, Bombardier, Guillemin and Ferraz22 Two independent bilingual translators, native speakers of Bangla, initially translated the original English questionnaire. These translations were compared and synthesised into a single version. A different bilingual translator, unaware of the original questionnaire, translated the Bangla version back into English. An expert committee reviewed this back-translation against the original to ensure accuracy, making necessary adjustments. The pre-final version was tested among 30 students to assess clarity, cultural relevance and comprehension. Feedback was used to make final adjustments. Pilot testing data were excluded from formal analysis. The psychometric properties of the scale, including reliability and validity measures, are detailed in the results section. The Bangla DAST is provided in the supplementary material available at https://doi.org/10.1192/bjo.2025.10.
Depression
Depression was evaluated using the Bangla Patient Health Questionnaire (PHQ-9). Reference Kroenke, Spitzer and Williams23,Reference Rahman, Dhira, Sarker and Mehareen24 This tool comprises nine items (e.g. ‘Little interest or pleasure in doing things?’) rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (more than half of the days). The total possible score ranges from 0 to 27, with a score of 10 or above indicating the presence of depression. In this study, the scale demonstrated good internal consistency, with a Cronbach’s α coefficient of 0.75.
Anxiety
Anxiety was measured using the Bangla Generalized Anxiety Disorder (GAD-7) scale. Reference Spitzer, Kroenke, Williams and Löwe25,Reference Faisal, Jobe, Ahmed and Sharker26 The scale includes seven items (i.e. ‘Feeling nervous, anxious or on edge’), rated on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day). The total score ranges from 0 to 21, with a cut-off score of 10 or higher indicating anxiety. Reference Spitzer, Kroenke, Williams and Löwe25 This threshold has been shown to have a sensitivity of 89% and a specificity of 82% for anxiety screening. Reference Spitzer, Kroenke, Williams and Löwe25 In this study, the scale demonstrated good internal consistency, with a Cronbach’s α coefficient of 0.79.
Insomnia
Insomnia was assessed using the Insomnia Severity Index (ISI-2). Reference Kraepelien, Blom, Forsell, Hentati Isacsson, Bjurner and Morin27 This version includes two items that address key aspects of insomnia: satisfaction with current sleep patterns and the impact of sleep on daily functioning. Responses are rated on a 5-point Likert scale, ranging from 0 (very satisfied) to 4 (very dissatisfied), yielding a total score between 0 and 8. A cut-off score of 6 or above was used to identify insomnia, with a sensitivity of 84% and specificity of 76%. Reference Kraepelien, Blom, Forsell, Hentati Isacsson, Bjurner and Morin27 The ISI-2 scale has been previously utilised in Bangladesh. Reference Hasan, Maliha, Rahman and Mamun28
Ethical consideration
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. The study obtained ethical approval from the University of South Asia in Dhaka, Bangladesh (Ref: IRB/2022/10(1)), ensuring adherence to ethical guidelines for research involving human participants. Before collecting data, the relevant school authorities, including school principals and class teachers, granted their approval, ensuring institutional support and ethical compliance. Students were provided with informed consent forms, which required their parents’ or guardians’ review and approval, making sure that their participation was voluntary and well informed. Both student assent and parental consent were required for participation, and students were made aware that they could withdraw from the study at any time without facing any penalty. Furthermore, no compensation was provided to the students for their participation, in line with ethical standards for recruitment practices.
Statistical analysis
Data were initially entered, cleaned and prepared for analysis using Microsoft Excel 2019 for Windows (Microsoft Corporation, Redmond, Washington, USA; https://www.microsoft.com). SPSS software version 27 for Windows (IBM Corporation, Armonk, New York, USA; https://www.ibm.com/products/spss-statistics) and R software 4.4.1 for Windows (R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org) were used for all the analyses. Categorical variables were summarised as frequency percentages, while continuous variables were presented as means and standard deviations. Skewness, kurtosis and histograms were used to assess the normality of the digital addiction scale. Given the assumptions of non-normality, Mann–Whitney and Kruskal–Wallis tests were conducted to examine mean rank differences between groups and the strength of the association was measured using effect size (<0.2 for small, <0.5 for moderate and >0.5 for strong). For item-level analysis, mean, standard deviation, skewness, kurtosis, corrected-item total correlation and McDonald’s omega if the item was deleted were reported. The reliability of the scale and its subscales were investigated using McDonald’s omega.
Confirmatory factor analysis (CFA) was conducted using the diagonally weighted least square method (DWLS) to examine the structural validity of the digital addiction components in the R software (‘lavaan’ package). The model fit was assessed using the comparative fit index (CFI), the Tucker–Lewis index (TLI), the root mean square error of approximation (RMSEA) and the standardised root mean square residual (SRMR). A satisfactory model fit was indicated by the CFI, and TLI values of >0.9, RMSEA of ≤0.06 and SRMR values of ≤0.08. Reference Hu and Bentler29,Reference Bentler30 Standard errors were adjusted using robust methods. Modification indices were performed to provide the best overall model fit to support the two-factor structural validity of the scale. The convergent validity was examined by investigating its relationship with other scales through Spearman’s rho correlation coefficient.
A multiple linear regression model was developed with the total DAST score as the dependent variable to identify the factors associated with digital addiction using the bootstrapping method with 5000 resamples. Assumptions for multiple regression were checked using variance inflation factor (VIF < 5), tolerance (>0.2), histogram and normal probability–probability (P–P) plot. The collinearity statistics and the normality of residuals, supported by the P–P plot and histogram, suggested that the data were appropriate for multiple linear regression analysis. All test results were considered significant at P < 0.05 with a 95% confidence interval.
Results
Characteristics of the study participants
Table 1 provides an overview of the participants’ characteristics. The majority of the participants were aged 12–14 years (72.1%), with a mean age of 13.91 ± 1.07 years. More than half were boys (53.94%), most were in the eighth grade (42.6%) and half resided in rural areas (50.9%). Regarding digital device use, 51.5% of participants slept alone, 68% watched television, 52.9% used a smartphone, 89.6% did not use a computer and 97.1% did not use a gaming device. In addition, 17.1% of participants exhibited depressive symptoms, 7.1% had anxiety and 2.4% were experiencing insomnia (Table 1).
Table 1 Distribution and differences between digital addiction and study variables
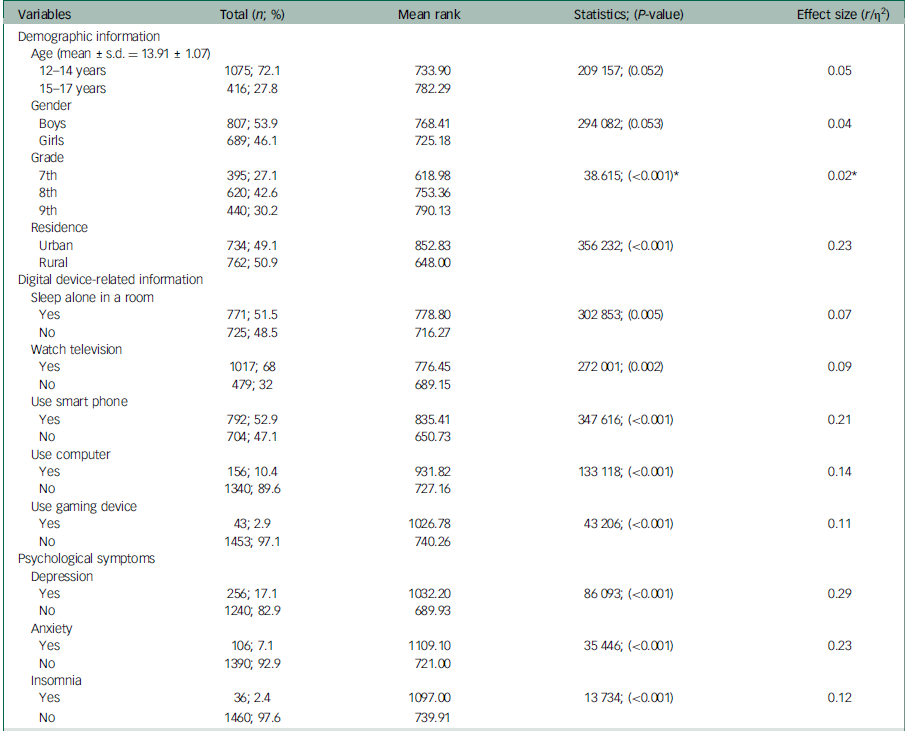
* Kruskal–Wallis test; effect size η2.
Internal reliability analysis of the Bangla DAST
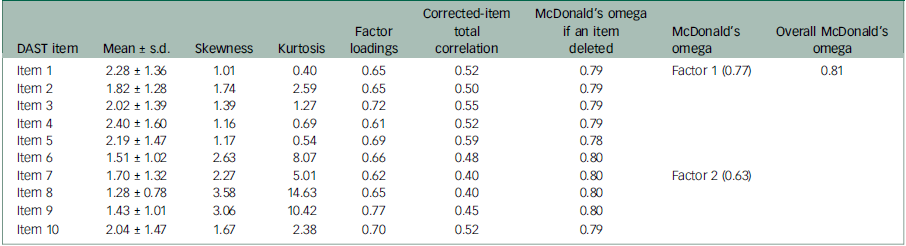
Table 2 presents the item-level analysis of the Bangla DAST. Confirmatory factor loadings for each item are shown in Table 2. All factor loadings were high (from 0.61 to 0.77), showing a strong relationship with the scale structure.Reference Kline31 Internal consistency was assessed using McDonald’s omega, indicating the values remained within the acceptable range when any single item was deleted. Factor 1 (attachment to digital devices) showed acceptable reliability, but the internal consistency for Factor 2 (compulsive use in different places) was moderate. In this study, the Bangla DAST demonstrated good internal consistency, with a value of 0.81 (Table 2).
Table 2 Internal reliability analysis of the Bangla Digital Addiction Scale for Teenagers (Bangla DAST)
Structural validity of the Bangla DAST
The structural validity of the digital addiction scale was assessed using the CFA. The results indicated that the two-factor model was moderately fitted, as evidenced by the following fit indices: CFI 0.97, TLI 0.95, RMSEA 0.06 [90% CI: 0.056–0.07] and SRMR 0.048.
Differences between digital addiction and study variables
Table 1 presents the differences in digital addiction scores across various study variables. The results indicate a significant variation in digital addiction scores by grade level, with ninth-grade students showing higher scores (η2 = 0.02, P < 0.001). Urban residents had significantly higher digital addiction scores compared to those from rural areas (r = 0.23, P < 0.001). Students who slept alone (r = 0.07, P = 0.005), watched television (r = 0.09, P < 0.001), used smartphones (r = 0.21, P < 0.001), used computers (r = 0.14, P < 0.001) or used gaming devices (r = 0.11, P < 0.001) had significantly higher digital addiction scores than those who did not. Furthermore, adolescents experiencing psychological symptoms such as depression (r = 0.29, P < 0.001), anxiety (r = 0.23, P < 0.001) and insomnia (r = 0.12, P < 0.001) also exhibited significantly higher scores of digital addiction compared to their peers without these symptoms (Table 1).
Spearman correlation between digital addiction and other variables
Table 3 reports the correlation coefficients between digital addiction and other variables. The two factors of the DAST were highly correlated with the DAST score. DAST Factor 1 and DAST Factor 2 were highly correlated with the overall DAST score, indicating that both factors significantly contribute to the measurement of digital addiction (r = 0.949 for Factor 1 and r = 0.754 for Factor 2, P < 0.001). Digital addiction was positively correlated with depression (r = 0.320, P < 0.001), anxiety (r = 0.282, P < 0.001) and insomnia (r = 0.328, P < 0.001), supporting the convergent validity of the digital addiction scale (Table 3).
Table 3 Spearman correlation among digital addiction, depression, anxiety and insomnia

DAST, Digital Addiction Scale for Teenagers.
**Correlation is significant at the 0.01 level (two-tailed).
Factors associated with digital addiction
Table 4 demonstrates a predictive model for digital addiction among adolescents. The model was statistically significant (F (12, 1442) = 36.019, P < 0.001) and explained 23.1% of the variance in digital addiction scores (R 2 = 0.231, adjusted R² = 0.224). This indicates that the factors included in the model account for a significant portion of the variance in digital addiction scores, providing a moderate model fit.
Table 4 Factors associated with digital addiction among adolescents
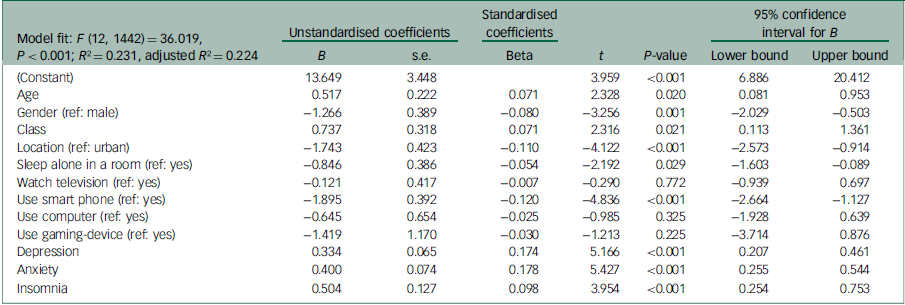
Results suggest that for each additional year in age, digital addiction scores increase by 0.51 units (b = 0.517, P = 0.020) and, for each increase in grade level, digital addiction scores rise by 0.73 units (b = 0.737, P = 0.021). Female participants had digital addiction scores that were significantly lower by 1.25 units compared to male participants. Also, not sleeping alone in a room (b = −0.846, P = 0.029) and not using a smartphone (b = −1.895, P <0.001) were significant predictors of lower digital addiction scores. For each additional unit increase in the depression, anxiety and insomnia scores, digital addiction scores increased by 0.334, 0.400 and 0.504 units, respectively (Table 4).
Discussion
The present study investigated the cultural validity of the Bangla DAST and its associated factors among Bangladeshi adolescents. The findings from this study provide robust evidence for the reliability and validity of the Bangla DAST. The scale demonstrated good internal consistency with a McDonald’s omega of 0.81, and CFA indicated a moderately fitted structure. Significant differences in digital addiction scores were observed across various demographic and behavioural variables, with higher scores among ninth-grade students, urban residents and those engaging in specific activities such as watching television and using smartphones, computers and gaming devices. Furthermore, adolescents experiencing psychological symptoms such as depression, anxiety and insomnia exhibited higher digital addiction scores. The predictive model revealed that age, grade level, gender, location, sleeping arrangements, smartphone usage, depression, anxiety and insomnia were all significant predictors of digital addiction, explaining 23.1% of the variance in digital addiction scores.
The Bangla DAST demonstrated strong reliability and moderate validity in this study, aligning with findings from other psychometric assessments of digital addiction instruments. The two-factor structure of the Bangla DAST comprises the following: (a) digital attachment, which includes aspects such as tolerance, withdrawal and a persistent preoccupation with digital devices (items 1–6) and (b) compulsive use, involving uncontrollable or problematic usage of digital devices in diverse settings (items 7–10). This two-factor structure captures distinct aspects of digital addiction, aligning with the conceptual model originally suggested by Seema et al Reference Seema, Heidmets, Konstabel and Varik-Maasik18 in their study with Estonian adolescents.
The internal consistency of the Bangla DAST is consistent with the original scale Reference Seema, Heidmets, Konstabel and Varik-Maasik18 and previous research validated the scale among Turkish secondary and high school students, indicating high reliability in both contexts. Reference Çelik, Tunç, Candemir, Kapkin İçen and Açar19 The Bangla DAST’s reliability also compares favourably with other Bangla versions of specific addiction scales, such as the Bangla Internet Gaming Disorder Scale–Short-Form (IGDS9-SF) and the Bergen Social Media Addiction Scale (BSMAS), both of which exhibited adequate levels of internal consistency. Reference Naher, Hiramoni, Alam and Ahmed32,Reference Islam, Jahan, Dewan, Pontes, Koly and Sikder33 The ACSID-11 (Assessment of Criteria for Specific Internet-use Disorders) is a recent digital addiction instrument validated across different language, although not yet available in Bangla. Reference Müller, Wegmann, Oelker, Stark, Müller and Montag34,35 Incorporating the ACSID-11 into future studies could further strengthen the comparative psychometric analysis across addiction scales. The two-factor structure CFA of the Bangla DAST indicated moderate structural validity. In contrast, a single-factor model was tested among Turkish students, showing acceptable fit indices, indicating that cultural differences may influence the perception and structuring of digital addiction. Reference Çelik, Tunç, Candemir, Kapkin İçen and Açar19 This finding is consistent with psychometric properties reported in other Bangla addiction scales, where CFA supported structural validity. Reference Naher, Hiramoni, Alam and Ahmed32,Reference Islam, Jahan, Dewan, Pontes, Koly and Sikder33 Overall, the Bangla DAST proved to be reliable, although it exhibited moderate structural validity, making it a valuable tool for assessing digital addiction among Bangladeshi adolescents. Future research could further explore the scale’s robustness across diverse populations and examine how the two-factor model functions in various cultural contexts.
The present study identified several significant factors of digital addiction among adolescents. Older adolescents exhibited higher digital addiction scores, a finding that is consistent with previous research indicating that digital addiction tends to increase with age because of greater autonomy and access to digital devices among older adolescents. Reference Gülü, Yagin, Gocer, Yapici, Ayyildiz and Clemente36 Older adolescents are more likely to use digital devices for social interaction, entertainment and academic purposes, which can contribute to higher levels of digital engagement and potential addiction. Reference Lee and Lee37 Male adolescents were found to have higher digital addiction scores compared to their female counterparts. This gender difference is supported by other studies, which have consistently reported higher rates of digital addiction among males. Reference Fam8,Reference Al-Mamun, Hasan, Mostofa, Akther, Mashruba and Arif14 One possible explanation is that males are more likely to engage in activities such as online gaming, which has been strongly associated with digital addiction. Reference Fam8 In addition, societal norms and expectations may encourage more digital engagement among males, particularly in gaming and technology-related activities.
Higher-grade students had significantly higher digital addiction scores. This finding is congruent with research suggesting that the transition to higher academic grades can be stressful, leading adolescents to seek digital distractions as a coping mechanism. Reference Al-Mamun, Hasan, Mostofa, Akther, Mashruba and Arif14 The increased academic demands and social pressures in higher grades may drive students to use digital devices more frequently for relaxation and socialisation, thereby increasing the risk of addiction. Urban residents were found to have higher digital addiction scores compared to their rural counterparts. This urban–rural disparity has been observed in other studies as well, whereby urban residents typically have greater access to digital devices and the internet. Reference Yasuma, Watanabe, Nishi, Ishikawa, Tachimori and Takeshima38 The higher availability and usage of digital technology in urban areas can lead to increased exposure and potential addiction. Moreover, urban environments often provide more opportunities for digital engagement through social media, online gaming and other digital platforms.
The present study identifies depression, anxiety and insomnia as significant factors of digital addiction among adolescents. Previous studies have consistently reported a strong relationship between these psychological factors and various forms of digital addiction. Reference Al-Mamun, Hasan, Mostofa, Akther, Mashruba and Arif14,Reference Liza, Iktidar, Roy, Jallow, Chowdhury and Tabassum15,Reference Al-Mamun, Mamun, Prodhan, Muktarul, Griffiths and Muhit20 For instance, depression and anxiety are known predictors of internet addiction, Reference Fumero, Marrero, Voltes and Peñate11 while a meta-analysis confirmed the strong link between sleep problems and internet addiction. Reference Alimoradi, Lin, Broström, Bülow, Bajalan and Griffiths39 The bidirectional relationship between mental health and digital addiction suggests that adolescents use digital devices as a coping mechanism for psychological distress, reinforcing dependency. Reference Elhai, Levine and Hall2 Insomnia, identified as both a cause and consequence of digital addiction, exacerbates the issue by disrupting sleep patterns through excessive screen time, particularly before bed. Reference Levenson, Shensa, Sidani, Colditz and Primack40 The findings from the current study align with this global trend, underscoring the need for targeted interventions to address the intertwined challenges of mental health and digital addiction, particularly in Bangladesh, where these issues are prevalent.
This study has several limitations, including its cross-sectional design, which limits the ability to infer causality between digital addiction and its associated factors. The reliance on self-reported data may introduce biases such as social desirability and recall errors, affecting the accuracy of the findings. In addition, the sample may not fully represent all Bangladeshi adolescents, which could limit the generalisability of the results. Furthermore, this study did not include measures of other forms of behavioural addiction, such as the BSMAS and IGDS9-SF. Without these established measures, it is challenging to determine the conceptual overlap between digital addiction as measured by the Bangla DAST and specific forms of behavioural addiction. This limits the study’s ability to compare findings with broader addiction constructs and reduces the study’s contribution to understanding the nuanced relationships among various behavioural addictions. Future research should address this limitation by comparing the DAST with these established tools to strengthen its criterion validity. The sample predominantly consisted of adolescents with limited exposure to certain digital devices, such as computers and gaming consoles. While the DAST captures broader patterns of digital overuse, the low prevalence of specific device usage may have biased the psychometric evaluation of the scale. Future studies should consider more diverse samples, particularly teenagers with greater exposure to digital technologies, to enhance the generalisability of the findings. Despite these limitations, the study has notable strengths. It addresses a significant research gap by focusing on digital addiction within the underexplored Bangladeshi adolescent population, providing culturally relevant insights. The study also employs a robust methodology that integrates psychological, behavioural and demographic factors, offering a comprehensive understanding of digital addiction’s factors. Furthermore, the psychometric validation of the Bangla DAST is a significant contribution, providing valuable information for future research in similar cultural contexts.
For future research, longitudinal studies are recommended to establish causal relationships between digital addiction and psychological factors such as depression, anxiety and insomnia. Expanding the sample to include a more diverse and representative group of adolescents across various regions of Bangladesh would enhance the generalisability of the findings. In addition, including other validated behavioural addiction scales, such as the BSMAS and IGDS9-SF, could facilitate a clearer understanding of how digital addiction overlaps with other specific behavioural addictions. Incorporating objective measures of digital usage, such as app usage data, alongside self-reported information could reduce biases and improve quantitative accuracy. Exploring additional factors such as family dynamics, school-related factors and peer influence could provide deeper insights into the predictors and consequences of digital addiction, allowing for more targeted interventions.
In conclusion, this study confirms the Bangla DAST appears to be a psychometrically valid tool for further studies to be carried out in Bangladesh. The scale will help to measure digital addiction among adolescents to identify individuals at risk of developing this problem. However, further research is needed to replicate the findings in the Bangladeshi context. In addition, the study found significant differences among various demographic, behavioural and psychological factors and digital addiction. The predictive model identified key contributing factors such as age, grade level, gender, sleeping arrangements and smartphone usage, explaining a substantial portion of the variance in digital addiction scores. These findings highlight the importance of considering demographic, behavioural and psychological factors in addressing digital addiction among adolescents.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1192/bjo.2025.10
Data availability
The data that support the findings of this study are available from the corresponding author, M.A.M., upon reasonable request.
Acknowledgements
The authors thank all the participants.
Author contributions
The study was conceptualised by F.A.-M. and M.A.M., and they collected the data. F.A.-M. analysed the data, interpreted the results and wrote the first draft. M.A.M. contributed to the preparation of the manuscript and edited the first draft. J.I. contributed to data collection, management and review. M.M.A. and M.M. supervised the project, and M.M.A., M.M. and D.G. reviewed and edited the manuscript. All authors approved the final version.
Funding
The present study received financial support from the University of South Asia, Dhaka, Bangladesh. In addition, M.M.A. acknowledges the funding support currently being received from Princess Nourah bint Abdulrahman University Researchers Supporting Project (PNURSP2025R563), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Declaration of interest
None.







 Open access
Open access
eLetters
No eLetters have been published for this article.