



Many clinical and parental observations report anxiety in children with high intellectual potential (HIP). We provide a service for children with HIP with emotional, behavioural and/or school problems at the National Center for Assistance to children and adolescents with High Potential (CNAHP) created in a French hospital-university department of child and adolescent psychiatry to identify and provide adapted care to these HIP youths with difficulties. More precisely, out of the first 338 children and adolescents referred to the CNAHP, a high proportion displayed school problems (78%), including school failure, and the following disorders according to ICD-101 and the DSM-52 diagnostic classifications: anxiety disorders (40.5%), intellectual disabilities (6.8%), conduct disorder (9.5%), depressive disorders (8%), personality disorders (3.5%), attention-deficit hyperactivity disorder (3.5%), obsessive–compulsive disorder (1.5%) and other problems (26.6% including, for example, family problems with sibling conflicts).Reference Guignard, Kermarrec and Tordjman3 Anxiety disorders are therefore the most frequent psychiatric disorders observed in this population. However, there have been relatively few studies of psychological and emotional disorders among children with HIP, and their results have been contradictory. Indeed, many studies on anxiety in children with HIP reported high levels of anxiety and the authors have suggested that high cognitive ability might be a vulnerability factor for psychiatric disorders.Reference Roberts and Lovett4,Reference Peyre, Ramus, Melchior, Forhan, Heude and Gauvrit5 However, some authors have failed to observe any significant difference in anxiety levels between children with HIP and their peers without HIP.Reference Guénolé, Louis, Creveuil, Baleyte, Montlahuc and Fourneret6–Reference Forsyth8 Finally, other authors have found that children with HIP were significantly less anxious than children of average intelligence, suggesting that children with HIP are better at coping with stressful situations and are somehow protected by their high cognitive abilities.Reference Terman9–Reference Zeidner and Shani-Zinovich13 It is noteworthy that the Martin et al meta-analysis highlighted lower levels of anxiety in individuals with HIP compared with individuals without HIP.Reference Martin, Burns and Schonlau14 It appears difficult to reach firm conclusions on the relationship between anxiety and HIP based on these contradictory results, which can be explained in part by methodological biases, such as different/absent definitions of HIP for the recruitment of participants to the studies,Reference Roberts and Lovett4,Reference Forsyth8,Reference Fouladchang, Kohgard and Salah12 small sample sizes,Reference Roberts and Lovett4,Reference Rost and Czeschlik7,Reference Forsyth8,Reference Tong and Yewchuk15,Reference Simoes Loureiro, Loventhal, Lefevre and Vaivre-Douret16 non-validated/adapted/specific tools for assessing anxiety and a single observational source for the evaluation of anxiety. Indeed, anxiety was assessed using mostly child's self-report evaluation,Reference Guénolé, Louis, Creveuil, Baleyte, Montlahuc and Fourneret6–Reference Forsyth8,Reference Scholwinsky and Reynolds10,Reference Reynolds and Bradley11,Reference Fouladchang, Kohgard and Salah12,Reference Tong and Yewchuk15 but also parental observation onlyReference Peyre, Ramus, Melchior, Forhan, Heude and Gauvrit5,Reference Simoes Loureiro, Loventhal, Lefevre and Vaivre-Douret16 or psychiatric evaluation.Reference Zeidner and Shani-Zinovich13 There are also studiesReference Guénolé, Louis, Creveuil, Baleyte, Montlahuc and Fourneret6 that did not compare individuals with HIP with individuals without HIP, raising questions therefore about the specificity of the results regarding high levels of intellectual functioning.
Given the discrepant results and methodological biases described above, the objective of the present study was to examine more thoroughly the relationships between high intellectual functioning and anxiety by comparing large samples of children with HIP and children without HIP, using clear definitions of HIP, with validated/adapted/specific assessment tools of anxiety in various and concomitant observational situations (parental evaluation, child psychiatric evaluation and child's self-report evaluation).
Method
Participants
The sample consisted of 608 children (mean age: 10.6 years, s.d. = 2.9, ranging from 6 to 16.1 years old, including 211 children with HIP (total IQ ≥130, 175 boys and 36 girls, mean age: 10. 7 years, s.d. = 3.0) and 397 children without HIP (total IQ <130, 333 boys and 64 girls, mean age: 10.5 years, s.d. = 2.8). They were all referred to the CNAHP, which provides a global psychological evaluation based on several tools, including cognitive, conative and socioemotional assessments given their problems (intellectual disabilities with school difficulties, emotional and/or behavioural problems). In addition, children and adolescents living near the CNAHP (1 h away maximum) are systematically referred to a child psychiatrist working in the CNAHP who becomes the medical referent in case of therapeutic follow-up after the psychological and psychiatric evaluation.
Written informed consent was obtained from all parents after explaining the study and its procedure to the parents and their children. The protocol was approved by the ethics committee of Rennes University Hospital.
Cognitive and anxiety assessments
Identification of HIP
Children's intellectual functioning was assessed by a psychologist using the Wechsler Intelligence Scale (WISC)-IVReference Wechsler17 validated for children and adolescents aged from 6 to 16 years, 11 months. The WISC-IV scale has been shown to have very good reliability and validity.Reference Wechsler17 Four composite scores were calculated based on ten subtests: the Verbal Comprehension Index (VCI), the Perceptual Reasoning Index (PRI), the Working Memory Index (WMI) and the Processing Speed Index (PSI). If a child had been already assessed using the WISC-IV less than 1 year ago, this child was not included in the study given that the reliability of the results from a new WISC-IV administration can be questioned.
Evaluation of anxiety
Anxiety was assessed according to three different observational sources: parents, child psychiatrist and child.
Parental evaluation
A parental questionnaire was used during a semi-structured phone interview (parental observation) conducted systematically for all parents by the same trained secretary when parents called to get an appointment for their child at the CNAHP. This interview includes questions about school, behavioural and/or emotional difficulties, such as anxiety problems, in order to check if the potential help provided by CNAHP is adapted to the parental request. Therefore, questions related to anxiety problems are asked consistently in the same way by the same professional for all parents.
Child psychiatric evaluation
The child psychiatric evaluation for ICD-10 and DSM-5 diagnostic criteria of anxiety disorders, based on psychiatric observation of the child or adolescent, provides a clinical psychiatric judgement. This psychiatric evaluation is performed only for children and adolescents living near the CNAHP and who could therefore benefit from regular therapeutic follow-up (as previously indicated in the Participants section).
Child's self-report evaluation
The Revised-Children's Manifest Anxiety Scale (R-CMAS)Reference Reynolds and Richmond18 is a self-report inventory for children from 6 to 19 years old. The R-CMAS, subtitled ‘what I think and feel’, is used to assess the level and nature of anxiety in children and adolescents. The R-CMAS provides a total anxiety score based on 28 anxiety items grouped in three subscales: physiological anxiety, worry/oversensitivity and social concerns/concentration. The physiological anxiety subscale is related to somatic symptoms associated with anxiety (such as sleep latency problems, nausea, fatigue, etc.). The worry/oversensitivity subscale is related to obsessional worries associated with fears of being emotionally hurt or isolated. The social concerns/concentration subscale is associated particularly with school problems and is related to social fears leading to attention or concentration difficulties.
The R-CMAS has been validated and used in research studies to measure anxiety in children with and without HIP.Reference Scholwinsky and Reynolds10 Also, there are nine lie scale items corresponding to social desirability. When these lie scores are too high, the other R-CMAS scores cannot be interpreted. In the present study, if a child got a score above 70 on the R-CMAS lie subscale, this individual was not included in the study. A R-CMAS total score between 60 and 70 corresponds to moderate anxiety levels and a R-CMAS total score above 70 corresponds to severe anxiety levels.
Concerning the assessment procedure, the R-CMAS self-report inventory was completed by the child at the CNAHP in the presence of a psychologist, who was available to answer the child's possible questions. Indeed, it appears it is important that the child neither completes the R-CMAS at home in the presence of parents, who might influence the child's responses, nor in a room alone given the potential emotional content of certain questions.
Statistical analyses
The relationships between anxiety (parental observation or child psychiatric diagnosis) and intellectual functioning (WISC-IV total IQ score and WISC-IV indices) were studied using either t-tests or χ 2-tests when the HIP group (IQ scores ≥130) was compared with the non-HIP group (IQ scores <130). The relationships between the R-CMAS anxiety scores (child's self-report evaluation) and levels of intellectual functioning (WISC-IV total IQ score and WISC-IV indices) were studied using t-tests when the HIP group (IQ scores ≥130) was compared with the non-HIP group (IQ scores <130).
Results
Descriptive analysis
To specify further the intellectual characteristics of the participants, we provide here the details of the WISC-IV scores for all the participants and the HIP and non-HIP groups (Table 1). It is noteworthy that the VCI is particularly high in the whole sample and the non-HIP group, and is the highest index in the HIP group.
Table 1 Descriptive analysis of Wechsler Intelligence Scale (WISC-IV) scores for the high intellectual potential (HIP) group (n = 211), the non-HIP group (n = 397) and all the participants (n = 608)

The child psychiatric evaluation was conducted for 324 out of 608 children given that, as explained in the Method section, only children living near the CNAHP area were systematically addressed to the child psychiatrist at the CNAHP for possible therapeutic follow-up. The parental evaluation and child's self-report evaluation were obtained from all parents and children (n = 608).
Based on psychiatric evaluation, anxiety disorders were observed in 162/324 (50%) of children attending the CNAHP and included mainly generalised anxiety disorder (143/324, 44.1%), but also phobic anxiety disorder (14/324, 4.3%) and separation anxiety disorder (5/324, 1.5%) according to DSM-5 and ICD-10 diagnostic criteria. Based on parental evaluation, the frequency of individuals with anxiety in the whole sample was 487/608 (80.1%).
Based on the child's self-report questionnaire (R-CMAS), anxiety was found in 145/608 (23.8%) of children, and about two-thirds of them (97/145, 66.9%) displayed moderate anxiety (R-CMAS total score between 60 and 70) and a third of them (48/145, 33.1%) displayed severe anxiety (R-CMAS total score above a threshold of 70).
According to the children's self-report evaluations, the distribution in the whole sample (n = 608) of the R-CMAS total anxiety score and the three different R-CMAS subscales scores were as follows: mean = 51.63 (s.d. = 12.87) (total anxiety score); mean = 51.83 (s.d. = 10.96) (physiological anxiety); mean = 49.67 (s.d. = 12.84) (worry/oversensitivity); mean = 52.92 (s.d. = 11.41) (social concerns/concentration).
Relationships between intellectual functioning and anxiety according to the parental, child psychiatric or child evaluation
The relationships between intellectual functioning and anxiety according to the child's self-evaluation, child psychiatric evaluation and parental evaluation are presented in Tables 2–4. There were no significant relationships between anxiety and intellectual functioning according to the child, child psychiatric or parental observational source when children were grouped with respect to the 130 cut-offs of intellectual giftedness for the WMI and PSI indices. Therefore, only total IQ, VCI and PRI levels are presented in Tables 2–4.
Table 2 Revised-Children's Manifest Anxiety Scale (R-CMAS) anxiety scores (child's self-report evaluation) in children (n = 608) grouped with respect to the 130 cut-off of intellectual giftedness for the total IQ score and the Verbal Comprehension Index (VCI) or Perceptual Reasoning Index (PRI) index

WISC-IV, Wechsler Intelligence Scale-IV.
Table 3 Relationship in children (n = 324) between anxiety (child psychiatric evaluation according to ICD-10 and DSM-5 criteria) and intellectual functioning for total IQ score, Verbal Comprehension Index (VCI) and Perceptual Reasoning Index (PRI)a
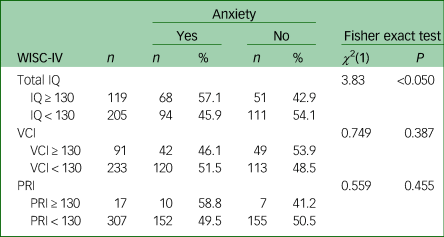
a. The results are expressed as the frequency of children with anxiety or without anxiety when children are grouped with respect to the 130 cut-off of intellectual giftedness for total IQ score, VCI and PRI.
WISC-IV, Wechsler Intelligence Scale-IV.
Table 4 Relationship in children (n = 608) between anxiety (parental observation) and intellectual functioning for total IQ score, Verbal Comprehension Index (VCI) and Perceptual Reasoning Index (PRI)a
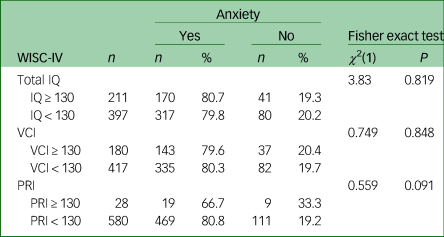
a. The results are expressed as the frequency of children with anxiety or without anxiety when children are grouped with respect to the 130 cut-off of intellectual giftedness for total IQ score, VCI and PRI.
WISC-IV, Wechsler Intelligence Scale-IV.
According to the child's self-report evaluation, when children were grouped with respect to the 130 cut-off of intellectual giftedness for the VCI index, the R-CMAS scores of total anxiety, physiological anxiety and worry/oversensitivity were significantly higher in the VCI ≥130 group compared with the VCI <130 group (Table 2). Inversely, when children were grouped with respect to the 130 cut-off of intellectual giftedness for the PRI index, the R-CMAS scores of total anxiety and worry/oversensitivity were significantly lower in the PRI ≥130 group compared with the PRI <130 group (Table 2). Also, it is noteworthy that VCI and PRI were significantly and positively correlated (r = 0.45, P<0.05).
Based on the child psychiatrist's evaluation, there was a significant relationship between total IQ scores and anxiety disorders according to ICD-10 diagnostic criteria. However, no significant relationship was observed between psychiatric diagnosis of anxiety disorders and any of the four WISC-IV indices (VCI, PRI, WMI or PSI index). The results are also presented for the VCI and PRI indices to allow the comparison with the child's self-evaluation (Table 3).
Based on the parental observation of anxiety, no significant relationships were found between intellectual functioning (total IQ score or any of the four WISC-IV indices) and anxiety (Table 4). The results are also presented in Table 4 for the VCI and PRI indices to allow comparison with the child's self-evaluation.
Finally, there was no significant relationship between the results compared across the three observational sources (parental, child psychiatric and child evaluations).
Discussion
Relationships between overall intellectual functioning and anxiety
A significant relationship was found between children's overall intellectual functioning (total IQ) and anxiety disorders diagnosed by the child psychiatrist according to the ICD-10 and DSM-5 criteria. This result confirms the findings of certain studies described in the introductory section reporting high levels of anxiety among children with HIP who have difficulties.Reference Peyre, Ramus, Melchior, Forhan, Heude and Gauvrit5,Reference Forsyth8 Children with HIP may exhibit anxiety because of their cognitive maturity and increased awareness leading to existential questions and associated anticipatory anxiety. Indeed, high overall intellectual functioning might lead to worries and therefore anxiety related to social preoccupations and questions about abstract concepts, not easily handled by some children given their young age and psychoaffective development. Inversely, anxiety corresponds to a state of hyperarousal with possible increased attention and alertness to environmental stimuli, which may contribute to high overall intellectual functioning.
There was no significant relationship between the children's overall level of intellectual functioning (total IQ) and anxiety, as assessed by either child's self-report evaluation (R-CMAS) or parental observation. It should be noted that anxiety was the most frequent psychological problem reported by parents (whole sample: 80.1%, HIP group: 80.7%, non-HIP group: 79.5%), and this high frequency, which reflects a problem of anxiety concerning most of the children recruited in the present study, might explain, because of a lack of discrimination of the sample, the absence of relationships observed between anxiety assessed by parents and total IQ scores or any of the four WISC-IV indices (VCI, PRI, WMI, PSI). In any case, our results underline the importance of using several different observational sources (parents, child and child psychiatrist evaluations) in order to assess more thoroughly anxiety behaviours, symptoms and disorders.
Relationships between anxiety and verbal ability or perceptual reasoning
Our study sheds light on the anxiety-related symptoms reported by children with high verbal potential (VCI ≥130) compared with children with poorer verbal skills (VCI <130). This significant association concerned not just the overall anxiety score, but also the physiological anxiety and worry/oversensitivity subscales. To our knowledge, this is the first study that assesses specifically anxiety among children with high and without high verbal potential. Our findings raise the issue that children and adolescents who invest in the cognitive sphere of verbal skills, choosing their words with care, using a wide vocabulary and talking like grown-ups from a very early age, may display some specific psychological characteristics.
Given the literature, several hypotheses can be proposed. First, some authors argue that high intellectual functioning, and more particularly verbal overinvestment, should be regarded as a mechanism for coping with anxiety.Reference Weismann-Arcache19 Overinvestment in language may reflect a need and an attempt for control to avoid being invaded and overwhelmed by emotions that are, by their very nature, difficult to control. However, these attempts to control emotions through verbal language overinvestment seem to fail given that in this study high anxiety is associated with high VCI. Inversely, it can be argued that these children encounter anxiety-provoking difficulties precisely because of their exceptional verbal skills. They may suffer from a wider gap between their advanced verbal skills and their physical (weight and height), psychomotor and emotional development than children who are gifted in other spheres and may experience more acutely this dyssynchrony.Reference Terrassier20 These children may be able to express their goals quickly and from an early age, but then they find themselves unable to attain them because of their youth and immaturity in other areas of development.
Moreover, parents of children with high VCI may value and nurture their verbal and academic prowess to the detriment of other areas that might allow them to achieve greater self-fulfilment. When too much emphasis is placed on verbal skills, children may engage less in play and creativity, thus losing the notion of pleasure. This may then lead to excessive striving for top marks at school which, when associated with perfectionism and fear of failure, may generate performance anxiety.
In addition, children with high verbal skills may sometimes have problems with relationships, because these skills are more salient in social situations than mathematical or spatial abilities,Reference Dauber and Benbow21 and set them apart from their peers, potentially resulting in anxiety and rejection.Reference Rousseau and Coulet22 Furthermore, high verbal potential reflected by a high VCI may be associated with high ability in verbal identification and expression of emotions, which can in turn increase awareness of emotions and lead to crystallisation with a reinforcement of these emotions. Therefore, expression of anxiety though verbal language might act not only as a mode of representation of anxiety but also as a reinforcement of anxiety contributing to higher anxiety scores on the self-report R-CMAS scale.
These different explanations may interact: whereas verbal overinvestment may initially constitute a means of warding off anxiety, this adaptive and defensive mode of functioning may subsequently place the child in a difficult position and foster the emergence of anxiety disorders. Finally, it cannot be ruled out that children with high VCI are more able than children without high VCI to identify and express verbally their emotions through a self-report inventory that is based on verbal identification and expression of anxiety. In this case, high R-CMAS anxiety scores in children with high VCI would not mean that these children are more anxious than children without high VCI but would rather reflect a methodological bias of assessment. It would explain why this result of an association between anxiety and high verbal potential is found in the child's self-report evaluation but not in the parental or child psychiatric evaluation, highlighting the need for multiple observational sources.
Our study also revealed a significant association between high PRI functioning (PRI ≥ 130) and anxiety reported on the R-CMAS. Children with high perceptual reasoning (PRI ≥ 130) were statistically less anxious (total anxiety score and worry/oversensitivity subscore) than children without high perceptual reasoning (PRI < 130). No previous study described psychological features of a high PRI population. The PRI measures fluid, as opposed to crystallised intelligence, and reflects generally the ability to find new solutions to new problems. As such, it measures respondents' ability to use their senses to structure their thinking and organise themselves. Children who are highly skilled in this area probably prefer what are sometimes rather solitary problem-solving activities to verbal activities. They are less concerned with existential questioning or social preoccupations, both potential sources of anxiety. Also, high perceptual reasoning might be used as a resource by children to solve stressful problems and keep emotions at a distance through reasoning, which may explain, in both cases, low anxiety scores observed in high PRI children. This can be related to the idea developed by Alfred KorzybskiReference Korzybski23 that rational thinking with reasoning process can decrease the negative effects of emotional reactions. Finally, it can be hypothesised that lower levels of anxiety may allow children to develop and express, thanks to a calm and secure internal environment, their perceptual reasoning potential and lower anxiety levels could therefore contribute to high PRI scores observed in these children.
Our results suggest that it would be useful to focus on individual cognitive indices, especially given that heterogeneous WISC-IV profiles are more frequent than homogeneous profiles in the clinical population coming to the Center but also in a general population.Reference Grégoire25 The definition of HIP is a theoretical definition with a predetermined cut-off threshold (total IQ ≥ 130 on the Wechsler scales according to the World Health Organization). Moreover, as the total IQ is a composite score, it can only be interpreted if it is based on broadly homogeneous indices to be representative of the child's intellectual capabilities. In the course of our clinical practice, we often come across children with no overall homogeneous intellectual potential, but rather a heterogeneous profile characterised by advanced skills in one or several domains. Most of these young individuals have high verbal skills (VCI scores considerably higher than the average score for children of their age). Verbal comprehension is a homogeneous index that measures crystallised intelligence. It is strongly linked to academic knowledge, and extremely sensitive to the learning opportunities available to children in their family environment; it is a reliable index, insofar as the examiner's subjectivity can have only a limited impact, given that the test is highly standardised.Reference Grégoire25 As well as being associated with anxiety, it is therefore highly predictive of learning and academic success. As such, we believe that the VCI is a useful measure for assessing children, as it has sound metric qualities and is of considerable clinical interest.
Several studies have indicated that the higher the total IQ, the greater the tendency for heterogeneous functioning and the weaker the correlations between the various subscales.Reference Detterman and Daniel26,Reference Lynn27 It is important to bear in mind that cognitive tests are not particularly sensitive at the extremes, making it difficult to gain a reliable picture of individuals with a particularly high IQ (i.e. total IQ ≥150).Reference Wechsler17 It is therefore legitimate to wonder whether the total IQ is a suitable measure for identifying HIP when it is used in isolation, without any other indices. Published in December 2016, the WISC-V is designed to improve profile accuracy precisely by adding new (ancillary) indices.
Based on our results, it appears that the VCI might be considered as a vulnerability factor for anxiety and PRI as a protective factor for anxiety (WMI and PSI indices were not significantly associated with anxiety scores). These opposing effects of two different aspects of intelligence might partly explain the discrepant relationships observed in the literature between intellectual functioning and anxiety; depending on the loading of the verbal component or reasoning component the results will differ. Furthermore, the directions of these effects can open interesting perspectives for further studies. It should also be noted, as indicated in the results section, that VCI and PRI scores are significantly and positively correlated. However, because these two dimensions of intelligence seem to have opposite effects on anxiety, they tend to nullify each other. This might explain why several studies using only a total IQ score did not find any effects of intelligence on anxiety assessed on self-report questionnaires.
Study limitations
Some limitations of the study should be acknowledged. First, the parental assessments of children's anxiety disorders, collected over the phone, were purely observational. As with all instruments based on observation, they were therefore dependent upon the observers' subjectivity. Although we use the same standardised and systematic interview grid for every child who attends the Center for an assessment, this tool has not been validated in clinical research. It might, therefore, be useful to supplement parental assessments with a properly validated instrument such as the Child Behavior Checklist. It is noteworthy that subjectivity cannot be ruled out either from the child psychiatrist's or child's evaluation. All observational sources are subject to subjectivity and should be therefore multiple to limit this bias. Second, although our control group was composed of children without HIP, there was a recruitment bias, given that they had all attended the CNAHP because of psychological and/or academic problems. This was therefore an atypical population probably not representative of the general population between the ages of 6 and 16 years. Thus, it would be useful to compare children with HIP who have difficulties attending the CNAHP with a sample of 6- to 16-year-olds drawn from the general population.
Implications
Anxiety in children with HIP was found in our study to be a very frequent parental preoccupation (80.7%) leading parents to bring their children to the CNAHP. Better understanding of the particularities and difficulties encountered by children with HIP, including anxiety, can improve their care and the development of their cognitive potential. Based on the results of this study, assessment of anxiety is highly recommended in children and adolescents with HIP who have school, behavioural and/or psychological difficulties. Early identification of anxiety disorders in this population can improve clinical practice by providing necessary therapeutic care.
This study highlights the importance of different observational sources of assessment. Indeed, children with high overall intellectual functioning (total IQ ≥130) who were referred to the CNAHP showed significantly more anxiety disorders than children without high overall intellectual functioning (total IQ <130) according to the child psychiatric diagnosis but not according to the parental observation or the child's self-evaluation. However, based on the child's self-evaluation, children with high verbal potential (VCI ≥130) perceived themselves as being significantly more anxious than those without high verbal potential (VCI <130), whereas children with high perceptual reasoning potential (PRI ≥130) perceived themselves as being significantly less anxious than those without high perceptual reasoning potential (PRI <130). These findings show the importance of studying different dimensions of cognitive functioning (such as the VCI and PRI), instead of focusing only on overall intellectual functioning (total IQ score). They offer interesting perspectives on children with HIP, based on their cognitive profile and regardless of their total IQ score, given that high verbal potential appears to be, in the present study, a factor of vulnerability for anxiety and that high perceptual reasoning potential may be a protective factor. Future research is needed to understand better the relationships between high intellectual functioning and anxiety, and their consequences for intellectual potential and talent development.
Funding
This study was funded by the CHGR (Centre Hospitalier Guillaume Régnier).
Acknowledgements
We thank the secretary, Cindy Menguy, who conducted the parental semi-structured phone interview and the psychologists of the CNAHP who participated in the cognitive assessments: Lisa Allain, Laura Blondel, Hélène Hardy, Marjo Lobach and Emilie Moguen.
Data availability
The structure of the data-set and the coding specification are available from the authors on request.
Author contributions
S.K., L.A. and S.T. conceived and designed the study. S.K. and S.T. recruited the children and evaluated anxiety. L.A., S.K., J.H.G. and S.T. performed the data analysis. S.K., L.A. and S.T. wrote the first draft of the manuscript, and all authors commented on the manuscript and revised the article.
Declaration of interest
None.
ICMJE forms are in the supplementary material, available online at https://doi.org/10.1192/bjo.2019.104.







 Open access
Open access
eLetters
No eLetters have been published for this article.