



LEARNING OBJECTIVES
After reading this article you will be able to:
• list a selection of shorter cognitive tests
• identify the situations in which they can be best used
• describe the various cognitive domains underlying assessment of fitness to plead.
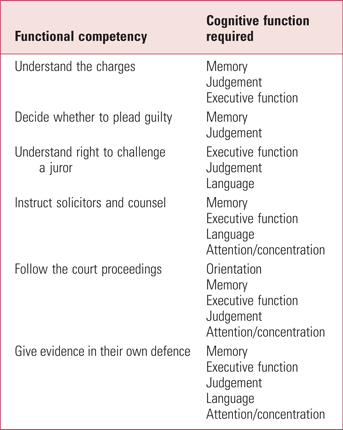
In England and Wales, the legal test of fitness to stand trial was originally set out in the case known as Pritchard (R v Pritchard 1836), but more recent case law, particularly R v John M [2003], has set out the test in the six parts illustrated in Table 1, which relates these to particular cognitive functions. It is important to note that these are a guide to help the clinician think about the areas that may be affected. They are not, as is the case in all cognitive testing, a replacement for clinical judgement. Almost all cognitive tests assess memory, attention and concentration, the Mini-Mental State Examination (MMSE) measures language in addition, and the Addenbrooke's Cognitive Examination (ACE) and Montreal Cognitive Assessment (MoCA) (with verbal fluency) can assess frontal lobe function to some extent.
TABLE 1 The six cognitive competencies of the legal test of fitness to plead and to stand trial in England and Wales
Many kinds of psychiatric disorder can affect fitness to stand trial. In younger people, psychosis, severe depression and intellectual disability can be factors. In older people, dementia and sometimes delirium may also be important. Cognitive function can be affected by any of these disorders. Tests of cognitive function have an important role in many areas of psychiatry when assessing patients who may have cognitive problems. The results of such tests should be used as a guide to inform a clinical judgement and are not an absolute measure that may indicate the presence or otherwise of significant cognitive impairment, and in themselves cognitive tests do not determine fitness to stand trial.
Cognitive tests
The assessment of cognitive testing in psychiatry started in the early 1950s with studies by Martin Roth which showed that people who had organic mental illnesses scored lower on tests of cognition than people with functional mental illnesses.
In 1968, Gary Blessed and the Newcastle group developed the Blessed Dementia Scale (Blessed Reference Blessed, Tomlinson and Roth1968), of which the cognitive section was the Information, Memory and Concentration test. This was a test that assessed knowledge of general information (such as orientation), short-term memory (remembering a name and address) and concentration (counting backwards from 20 down to 1). The Blessed Dementia Scale recorded the number of errors, hence the higher the score the worse the impairment.
A variant of that measure is the Mental Test Score, which was originally scored out of 34. This long version was quickly honed down to a ten-item version: the Abbreviated Mental Test Score (AMTS, also known as the Abbreviated Mental Test, AMT) (Hodkinson Reference Hodkinson1972) (see Supplementary Appendix 1, available at https://dx.doi.org/10.1192/bja.2024.17). The AMTS is greatly loved in the general hospital setting because it is very brief to administer. It is used in many of the major assessments of delirium. A further simplified four-item version asks the person to tell you their age, what year it is, where they are and their date of birth.
In 1975, the Mini-Mental State Examination (MMSE), probably the most widely used cognitive test in the world, was published (Folstein Reference Folstein, Folstein and McHugh1975). The original rationale was to give doctors and others working in the general hospital setting a ready tool to assess cognitive function in their patients. It tests orientation, language, attention, memory and praxis. It is scored out of 30. A few years ago it became subject to a charge for its use under copyright (www.parinc.com/Products/Pkey/237) and as other free tests are available it is now used less than in the past. A standardised version, with specific scoring instructions, is available (Molloy Reference Molloy and Standish1997).
A number of other tests have been developed. The Montreal Cognitive Assessment (MoCA) (https://mocacognition.com) is also scored out of 30. The test starts with the trails test, copying a cube and drawing a clock, which many older people find difficult – a tenet of cognitive function is to ease people into what essentially can be a conversation rather than them failing at the first hurdle. The MoCA is widely used, and several sets of normative data are available, which allows a comparison of a particular person's score with those of a large sample of people of similar age and educational background, two factors that can have marked effects on test scores.
The Mini-Cog (https://mini-cog.com) is a very brief assessment scale where the assessor says three words, asks the person to draw a clock and put the hands to show ten past eleven and then to remember the three words. There are many ways in which it can be interpreted but, essentially, if the person can only remember one of the three words that is an indication for more testing. If they recall one or two words, the clinician uses the clock drawing test as a tie-breaker. If the clock is perfect, then there is probably no need to do further tests. If the clock is abnormal, more detailed inquiry is merited. For a test that is so brief, one could not possibly say that it does anything more than screening for the possible presence of cognitive impairment.
The Addenbrooke's Cognitive Examination (ACE) (Hodges Reference Hodges2017) is a commonly used assessment in clinical practice in memory clinics in the UK. It is currently in its third edition (the previous version included the MMSE score and was later dropped because of copyright issues). It is scored out of 100 and usually takes only 10–15 min to administer but gives a very thorough score on memory, attention, verbal fluency, language and visuo-spatial function. It provides a more comprehensive assessment than shorter tests.
The Repeatable Battery for the Assessment of Neuropsychological Status Update (RBANS Update) is more extensive and has the advantage of giving a score in relation to a percentile of a population, but must be purchased from the publisher (www.parinc.com/Products/Pkey/237).
The Frontal Assessment Battery (Dubois Reference Dubois, Slachevsky and Litvan2000) can give a measure of frontal lobe function as well. Some of this is contained is contained within the ACE (the verbal fluency and clock drawing subtests) but asking about similarities (for example, in what way are a table and a chair alike) and carrying out the Luria test (asking the person to copy a sequence of fist, palm and side of the hand movements) can be helpful in identifying frontal lobe problems.
The Cognitive Estimation Test (Taylor Reference Taylor and O'Carroll1995) is a measure of someone's ability to give an approximate answer to a question for which there is often no exact figure. Common examples include: How many miles is it from Manchester (can be adapted for any city) to London? How long would it take to blow up a party balloon? How old is the oldest person in Britain? What is the height of the Blackpool Tower? How many camels are there in Belgium? If someone gives an answer that is likely to be approximately correct, that suggests reasonable judgement even when on questions that may be alien to them. For example, a correct answer to ‘How many camels are there in Belgium?’ would be ‘about 20’ – there will be a few in zoos and some in private collections. If someone says 100 000 or none, then that is wide of the mark.
A recently developed test is the Free-Cog (Burns Reference Burns, Harrison and Symonds2021) (Supplementary Appendix 2). The scale, scored out of 30, is designed to be administered in a conversational way and combines cognitive and executive function tests. The secret is in the name and the idea is that the scale can be used widely and is freely available. The cut-offs have been well described.
What to use and when
Cognitive tests do not directly measure fitness to plead, nor diagnose any specific mental disorder, such as dementia, although they can be an important part of such assessments. The measures simply give an assessment of cognitive function, cognitive abilities or cognitive impairment. Measurement of cognitive function is not an exact science and scores on tests can be affected by circumstances unrelated to changes in the brain, such as: the time of day the test takes place (people can have impaired attention, which can affect tests administered immediately after lunch or late in the afternoon); drugs – including alcohol – which may affect concentration and attention; and the presence of pain, which can cause people to pay less attention. The ability to answer questions accurately can also be affected by simple things such as whether a person has their correct reading glasses or a functioning hearing aid. There is sometimes a tendency to over-rely on an actual measure on a scale.
Of course, one does not need to use one of the set clinical tests, and often a description of whether someone is oriented, what their general knowledge is like, whether they are able to remember three words and whether they can draw a clock face can be helpful. In fact that was one of the rationales for the introduction the Free-Cog, in that it was something that flowed and made sense to people. For example, the Mini-ACE consists of a number of excellent questions, but some individuals can find the questions rather pointless and irrelevant.
The appropriate test to use depends on the clinical or forensic question that needs to be answered. For a quick screen of cognitive function in a general forensic setting, it would make sense to use something like the AMTS or the Mini-Cog.
If there is a bit more suspicion of cognitive impairment in an individual, then either the MMSE (with appropriate copyright permission) or the MoCA (there is a requirement now for training in its use before it can be downloaded) or the Free-Cog can be very helpful.
If a clinician is very suspicious of the presence of cognitive impairment, it would be appropriate to use the ACE. This, and the other tests mentioned, can be supplemented with tests such as the Cognitive Estimation Test and the Frontal Assessment Battery. If more than that is needed, it would be appropriate to ask for expert neuropsychology advice.
Executive function refers to the ability to integrate a number of psychological functions and cognitive capabilities to formulate new plans or actions and to align these to achieve a desired goal. So, the person has to form an intention to achieve the goal, make plans to monitor progress towards it, be flexible to overcome difficulties and be able to decide when the goal has been achieved. An essential component of executive function is judgement. Executive function has been described as the air traffic control centre of the brain.
For example, to get your car successfully out of a car park, you first have to remember where you parked it but then you would need your executive function to work out how to start it up, negotiate out of the parking space, find the exit and pay the parking fee in order to exit. In this example, just forgetting where the car was would not be sufficient for a diagnosis of dementia. It is easy to mix up memory and executive function. For example, one sometimes hears families say ‘My mother has forgotten how to cook a meal’. In reality it is not that the person has forgotten how to cook but the complexity of coordinating and sequencing ingredients needs intact executive function, which may be impaired in people with dementia.
Conclusion
In summary, there are a number of cognitive tests that can be used to assess the degree of impairment. This in turn may inform (but cannot take the place of) an assessment of fitness to plead and fitness to stand trial. Our next article in this issue (Series Reference Series and Burns2024) looks specifically at the value – and hazards – of using cut-offs in such tests.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bja.2024.17.
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Author contributions
A.B. is the primary author of this article. H.S. developed the original idea in collaboration with A.B. and was instrumental in crafting the final version through several drafts.
Funding
This work received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.
MCQs
Select the single best option for each question stem
1 Cognitive testing:
a on its own can determine a person's ability to stand trial
b was first used in the 1930s
c is the only thing needed to diagnose dementia
d scores are unaffected by mood
e scores can vary at different times of the day.
2 Which of the following is suitable for a very brief assessment of cognition?
a ACE
b MoCA
c MMSE
d Mini-Cog
e RBANS Update.
3 The ACE:
a is a brief test
b covers only memory
c is scored out of 80
d can only be used with special expertise
e covers a range of cognitive functions.
4 Executive function:
a can be identified by one single test
b does not involve planning and organisation
c impairments can affect fitness to stand trial
d is very easy to assess
e is always normal in dementia.
5 Of the following cognitive domains, the one most unlikely to affect fitness to stand trial is:
a memory
b praxis
c language disturbance
d executive function
e attention.
MCQ answers
1 e 2 d 3 e 4 c 5 b




 Open access
Open access
eLetters
No eLetters have been published for this article.