



Introduction
As policymakers around the globe struggle with the COVID-19 pandemic, vaccines offer an effective tool to tackle the severity and spread of the underlying viral disease (SARS-CoV-2). Promoting vaccine uptake is a crucial component of government policies and public health endeavors (Chen et al., Reference Chen, Trump, Hall and Le2020). These efforts focus on protecting both vaccinated individuals and the community at large. Therefore, government agencies need to develop easy-to-implement tools that can be rapidly deployed and scaled up to increase immunization coverage (Milkman et al., Reference Milkman, Patel, Gandhi, Graci, Gromet, Ho, Kay, Lee, Akinola, Beshears, Bogard, Buttenheim, Chabris, Chapman, Choi, Dai, Fox, Goren, Hilchey and Duckworth2021b, Reference Milkman, Gandhi, Patel, Graci, Gromet, Ho, Kay, Lee, Rothschild, Bogard, Brody, Chabris, Chang, Chapman, Dannals, Goldstein, Goren, Hershfield, Hirsch and Duckworth2022).
Governmental vaccination campaigns are one significant way to achieve this goal (Krpan et al., Reference Krpan, Makki, Saleh, Brink and Klauznicer2021). They aim to convince members of the public that vaccinations are both saving individual lives and contributing to herd immunity (Lunn et al., Reference Lunn, Belton, Lavin, McGowan, Timmons and Robertson2020; Loomba et al., Reference Loomba, de Figueiredo, Piatek, de Graaf and Larson2021; Patel, Reference Patel2021). Hence, activating resources to communicate vaccination opportunities to residents and motivate them to get vaccinated remains a core challenge (Milkman et al., Reference Milkman, Beshears, Choi, Laibson and Madrian2011; Lovari et al., Reference Lovari, Martino and Righetti2021).
However, government agencies, especially at the local level, are not always well-equipped to communicate effectively with the public. Scholars have highlighted the relevance of governmental communication while also emphasizing existing deficits (Liu et al., Reference Liu, Horsley and Yang2012). In the context of the COVID-19 pandemic, ineffective communication may come at the cost of individuals’ lives and threaten overall public health by undermining herd immunity (Schwarzinger et al., Reference Schwarzinger, Watson, Arwidson, Alla and Luchini2021). Thus, scholars call for action, indicating that, ‘we need to start learning now how best to “nudge” people to receive their vaccinations. [ … ] Now is the time to generate, collect and share evidence on which approaches work and which do not’ (Patel, Reference Patel2021, p. 185).
Extant research across the behavioral sciences presents insights that offer simple ways to improve government agencies’ information campaigns (Belle & Cantarelli, Reference Belle and Cantarelli2021; Milkman et al., Reference Milkman, Gandhi, Patel, Graci, Gromet, Ho, Kay, Lee, Rothschild, Bogard, Brody, Chabris, Chang, Chapman, Dannals, Goldstein, Goren, Hershfield, Hirsch and Duckworth2022). For instance, simple reminders can positively affect whether residents get vaccinated (Chen et al., Reference Chen, Trump, Hall and Le2020; Milkman et al., Reference Milkman, Patel, Gandhi, Graci, Gromet, Ho, Kay, Lee, Akinola, Beshears, Bogard, Buttenheim, Chabris, Chapman, Choi, Dai, Fox, Goren, Hilchey and Duckworth2021b). Furthermore, laboratory and survey experiments show that emphasizing the importance and usefulness of herd immunity can induce prosocial vaccination behavior to protect others (Betsch et al., Reference Betsch, Böhm, Korn and Holtmann2017; Korn et al., Reference Korn, Böhm, Meier and Betsch2020; James et al., Reference James, Bokemper, Gerber, Omer and Huber2021). However, communicating about contributions to herd immunity might not be compelling to all target groups (Isler et al., Reference Isler, Isler, Kopsacheilis and Ferguson2020) and even invite free-riding behavior. Indeed, individuals can profit from the protection provided by a well-vaccinated society without contributing to herd immunity themselves. This dysfunctional mechanism results from the dispersion of individual responsibility for this public good (Ostrom, Reference Ostrom1990; Peck et al., Reference Peck, Kirk, Luangrath and Shu2021).
Recent consumer and marketing research offers a theoretical approach proposing the psychological ownership mechanism to potentially increase residents’ vaccination intentions (Peck et al., Reference Peck, Kirk, Luangrath and Shu2021). Focusing on self-interest and promotion, psychological ownership is defined as ‘feelings of ownership for a variety of objects, material and immaterial in nature’ (Pierce et al., Reference Pierce, Kostova and Dirks2003, p. 84). Emphasizing psychological ownership can trigger individual contributions to public goods (Jami et al., Reference Jami, Kouchaki and Gino2021; Peck et al., Reference Peck, Kirk, Luangrath and Shu2021; Zhang et al., Reference Zhang, Liu, Zhang, Xu and Cheung2021).
This study implemented a local government public health information campaign to increase individual ownership of the COVID-19 vaccine. Building on previous research focusing on patients in from a healthcare system (Dai et al., Reference Dai, Saccardo, Han, Roh, Raja, Vangala, Modi, Pandya, Sloyan and Croymans2021), we suggest that increasing psychological ownership for COVID-19 vaccines will increase vaccination uptake in the general population. Based on a pre-registeredFootnote 1 cluster-randomized field experiment in cooperation with a German municipality, we test the efficacy of a subtle psychological ownership intervention in letters from the municipality's mayor. The goal is to increase residents’ COVID-19 vaccination intentions. Vaccination intentions are measured as unique link clicks on a specifically developed municipal website. On this website, residents can schedule a COVID-19 vaccination appointment (supplemented by vaccination-relevant information).
Thereby, we offer two distinct contributions. First, this study provides a novel way to foster individual contributions to public goods, applicable in various contexts. One essential contribution of our study is that we probe the external validity of prior scholarship on the relationship between psychological ownership and COVID-19 vaccination intentions (Dai et al., Reference Dai, Saccardo, Han, Roh, Raja, Vangala, Modi, Pandya, Sloyan and Croymans2021; Peck et al., Reference Peck, Kirk, Luangrath and Shu2021) among the entire adult population of a German town. We show how a low-cost intervention eliciting a feeling of individuals’ ownership can be beneficial when facing dysfunctionalities in providing public goods. Second, the study provides a ‘real-world’ test of behavioral interventions to increase the number of residents intending to make vaccination appointments. The present approach offers policymakers a practical, low-cost and easy-to-implement approach. Psychological ownership interventions can increase the number of people getting life-saving vaccines and contribute to herd immunity.
Theoretical background
Using psychological ownership to increase desirable behaviors
Research on psychological ownership focuses primarily on how individuals experience ownership and their relationships to owned entities (e.g., consumer goods). This research focus intends to predict individuals’ emotions, cognitions and behaviors toward owned entities (Peck & Shu, Reference Peck, Shu, Peck and Shu2018; Pierce et al., Reference Pierce, Kostova and Dirks2001, Reference Pierce, Kostova and Dirks2003). In general, psychological ownership is a cognitive-affective construct reflecting an ‘individual's awareness, thoughts, and beliefs regarding the target of ownership’ (Pierce et al., Reference Pierce, Kostova and Dirks2003, p. 86).
Individuals use their possessions during the development and display of their identity. Psychological ownership, thus, explains why and how individuals integrate objects in behaviors and expressions, such as during conversations (Jami et al., Reference Jami, Kouchaki and Gino2021). Psychological ownership constitutes possessive feelings toward material and immaterial objects manifested in expressions such as my, mine, and our (Pierce et al., Reference Pierce, Kostova and Dirks2001, Reference Pierce, Kostova and Dirks2003). In this sense, psychological ownership can include a range of different targets – material (a car) as well as abstract (an idea), or in the form of persons (a friend) or social constructs (a family). Empirical studies show how psychological ownership affects attitudes, values and behaviors related to the specific entity (Peck & Shu, Reference Peck, Shu, Peck and Shu2018), such as endowment effects (Beggan, Reference Beggan1992), the higher perceived value of an object (Dommer & Swaminathan, Reference Dommer and Swaminathan2013; Kricheli-Katz & Posner, Reference Kricheli-Katz and Posner2020) and increased emotional attachment (Shu & Peck, Reference Shu and Peck2011). Van Dyne and Pierce (Reference Van Dyne and Pierce2004) show that feelings of ownership can increase personal sacrifice, the assumption of risk on behalf of the entity, and greater responsibility for and stewardship of the target entity. Bakr et al. (Reference Bakr, Afsar-Manesh, Raja, Dermenchyan, Goldstein, Shu and May2020) show that a psychological ownership intervention in a letter can foster patients to engage in clinical tests. Peck et al. (Reference Peck, Kirk, Luangrath and Shu2021) extended these findings from private possessions to public goods. They show that psychological ownership can evoke cognitions and behaviors beyond those directed toward the owned entity. A feeling of ownership (e.g., seeing a ‘welcome to YOUR park’ sign) can encourage community members to better care for public goods (e.g., collecting trash or donating money) motivated by stronger feelings of responsibility.
Psychological ownership may benefit the provision of public goods by reducing free-riding. Even if people are not the owner in a strictly legal sense recent research finds that increasing psychological ownership can increase an individual's feelings of responsibility for the public good (or components of it) and lead to stewardship behavior (Peck et al., Reference Peck, Kirk, Luangrath and Shu2021). Put differently, an increased sense of individual ownership might help prevent the problems associated with shared ownership and diffused responsibilities.
The psychological ownership mechanism
Preventing the spread of vaccine-preventable diseases such as COVID-19 benefits the overall population. This effect occurs regardless of whether they directly contributed to the eradication effort. Herd immunity constitutes a public good because it is both non-excludable and non-rivalrous in consumption (Buttenheim & Asch, Reference Buttenheim and Asch2013; Johnson et al., Reference Johnson, Dawes, Fowler and Smirnov2020; see also Samuelson, Reference Samuelson1954). As a public good, it suffers from dysfunctionalities such as free-riding, which plays a relevant role in vaccination decisions (Agranov et al., Reference Agranov, Elliott and Ortoleva2021; Yong & Choy, Reference Yong and Choy2021), albeit not the only one.
The theoretical mechanism of psychological ownership indicates that felt ownership should reduce free-riding and, thus, increase individuals’ vaccination intentions (Dai et al., Reference Dai, Saccardo, Han, Roh, Raja, Vangala, Modi, Pandya, Sloyan and Croymans2021). The proposed mechanism works as follows: Psychological ownership facilitates alignment of the interests of the public good (here: herd immunity through COVID-19 vaccination) with individuals’ intention and actual behavior. Individuals will develop a feeling of ownership, strengthening their connectedness to the vaccine. Hence, they will be more likely to contribute to the public good and focus on arranging a vaccination appointment. This effect results from the awareness that individual vaccine uptake will contribute to the public good (Peck et al., Reference Peck, Kirk, Luangrath and Shu2021), and the increased individual self-esteem triggers prosocial behavior (Jami et al., Reference Jami, Kouchaki and Gino2021).
First, individuals should care more about public goods once they feel ownership of relevant constituting goods (here: vaccines). The increased perceived value can exist for public goods just as it does for individually owned objects. Even effortful behaviors for the benefit of the public good, such as picking up trash, can be triggered by psychological ownership (Peck et al., Reference Peck, Kirk, Luangrath and Shu2021). Following this line of argumentation, we suggest that psychological ownership can elicit behaviors that contribute to the public good of herd immunity by getting vaccinated. Previous research shows that psychological ownership can have an effect similar to that of legal ownership and increase the perceived value of an object (Shu & Peck, Reference Shu and Peck2011).
Second, triggering psychological ownership should positively affect individuals’ self-esteem (Jami et al., Reference Jami, Kouchaki and Gino2021), which should elucidate prosocial behavior aiming to contribute to the public good. Self-esteem is dependent on others’ perceptions and evaluations, and possessions play a relevant role in the perception of social positions (Dittmar, Reference Dittmar1992). Previous research argues that the boost in self-esteem due to felt ownership can trigger prosocial behavior (Jami et al., Reference Jami, Kouchaki and Gino2021). We expect individuals experiencing higher psychological ownership should exhibit a higher self-efficacy to get vaccinated and contribute to herd immunity. Previous studies support this argument, indicating a negative relationship between self-esteem and anti-social behavior (Graf, Reference Graf1971; Liang et al., Reference Liang, Liu, Tan, Huang, Dang and Zheng2016). Furthermore, prosocial behavior can help people maintain their boosted self-esteem, given that prosocial behavior is often admired and valued (Jami et al., Reference Jami, Kouchaki and Gino2021). Overall, we hypothesize:
H1: Emphasizing vaccine-related psychological ownership in a mayor's letter to residents (compared to a business-as-usual letter) increases residents’ intent to get vaccinated.
Data and methods
Experimental procedure and intervention
To test the effectiveness of a psychological ownership intervention on residents’ intention to receive a COVID-19 vaccination, we conducted a cluster-randomized field experiment in cooperation with the German municipality Bad Nauheim. The experimental design was developed in close consultation with officials of the municipality's administration to ensure high external and ecological validity (McConnell, Reference McConnell2021). We conducted a between-group design integrated into an official mailing campaign. The campaign included personalized letters sent to every resident in the respective municipality to raise awareness about COVID-19 vaccines and the possibility of setting up a vaccination appointment. We designed a letter that included all necessary information about the vaccine, the need to reach herd immunity, and how to schedule vaccination appointments. The letter was then formatted and typeset by the municipal administration. The letter was signed by the municipality's Mayor and two public health officials to further emphasize the matter's urgency. The control letter outlines the personal benefits of getting vaccinated against SARS-CoV-2, similar to previous nudging approaches (Milkman et al., Reference Milkman, Patel, Gandhi, Graci, Gromet, Ho, Kay, Lee, Akinola, Beshears, Bogard, Buttenheim, Chabris, Chapman, Choi, Dai, Fox, Goren, Hilchey and Duckworth2021b).
Compared to the control letter, the treatment letter contains a psychological ownership manipulation, i.e., subtle changes to the written text and the headings to emphasize individual ownership of the vaccine. We introduced explicit references to the ownership status by referring to ‘Your’ vaccine, ‘Your’ vaccine appointment and ‘Your’ personal contribution. These subtle changes were intended to increase the felt ownership related to the vaccine. The control letter simply referred to vaccination and vaccination appointments without reference to individual ownership status. The complete letters can be found in the Supplementary Appendix.
All letters included a personalized link and corresponding QR code to the municipality's information website. This website included links to the digital scheduling software for vaccination appointments and information about the COVID-19 vaccines. Furthermore, the website offered a list of general health practitioners offering vaccinations in the municipality.
Trial design and sample
The research design is a cluster-randomized controlled trial, including randomization of two different versions of a letter. Addresses were treated as cluster units. We randomized residents at the address level to avoid potential spillover effects among household members. Thus, every individual (n = 27,306) within the same address (n = 6,442) received the same letter on the weekend of 21–23 May 2021. We furthermore block randomized allocation to letters based on different cluster sizes (i.e., the number of individuals within addresses) to ensure a proportional distribution of control and treatment letters within clusters (Middleton & Aronow, Reference Middleton and Aronow2015). This approach allows using a conventional difference-in-means estimator within blocks without risk of bias (Gerber & Green, Reference Gerber and Green2012, p. 82). Randomization was performed in stata 16 using a reproducible seed.
The sample size is a census of all vaccine-eligible residents of the municipality, including those aged 18 and above (n = 27,306) nested in 6,442 addresses. We draw on Betsch et al. (Reference Betsch, Böhm, Korn and Holtmann2017) to presume a baseline click rate of about 10% in the control letter for sample size calculations. This baseline reflects the proportion of letter recipients that would follow the individualized link (dichotomous outcome: page visit yes/no). For our pre-study power calculations, a bracketed interclass correlation of between 0.01 and 0.3 provided a minimum detectable effect (MDE) between 1.1 and 1.5 percentage points at 80% power. We updated these figures after study completion. The observed baseline click rate of 7.62% and interclass correlation of 0.0002 at 1-week post-intervention (8.62% and 0.0001, respectively at 4-weeks post-intervention) resulted in an MDE of 0.92 percentage points (0.98 at 4-weeks post-intervention) at 80% power. In other words, our study is well powered to detect a minimal effect of a 0.92 percentage points difference between control and treatment letters at 1-week post-intervention and 0.98 percentage points at 4-weeks post-intervention.
The research design embodies a so-called encouragement design (Gerber & Green, Reference Gerber and Green2012). We sent letters to all study participants but could not ensure that everyone read the letter. Thus, we estimate treatment effects based on the intention-to-treat (ITT). Such field experiments include the risk that some residents will not receive the letter, open it or give it much consideration. However, the comparison of control and treatment groups should be accurate. In particular, randomization results in equivalent portions of residents not receiving the letter or not paying attention. Hence, the ITT is a conservative approximation of the actual treatment effect among those who receive and open the letter.
Outcome measures
To obtain the outcome measures for our study, we used different independent data sources. First, the Mayor's office generated a list of all municipal residents with an address in the municipality. Following the cluster randomization, each resident aged 18 and above received an information letter via mail. The letters contained an individualized link that included so-called Urchin Tracking Module (UTM) parameters. Such parameters are used in online marketing to assess, among others, the effectiveness of advertising campaigns. The UTM parameters included a randomly created identifier with five letters or numbers (e.g., 123AB) in our research design. This procedure allowed identifying the individual click behavior (link was clicked vs link was not clicked) without revealing the unique identity. To ensure a convenient link in the letter, we used the web-based application ‘rebrand.ly’ to shorten the original links. This approach allows creating a branded URL that includes the identifier but removes the UTM parameters (i.e., link.com/123AB). The provider collects data for click traffic for each shortened link and provides them using a secure Application Programming Interface (API). Using this API, we collected the dependent variable data at two points: (1) 1-week post-intervention and (2) 4-weeks post-intervention. We primarily obtained ‘unique clicks’, indicating the number of individuals who performed at least one click on each link.
To probe the findings’ robustness, we also collected data using the UTM parameters of each link based on Google Analytics for the municipality's website (for more detail, see: https://support.google.com/analytics/answer/9268042?hl = en&ref_topic = 10331681). Google Analytics data also included whether and how often each individualized link was clicked. For the primary dependent variable, ‘Unique Clicks’, we recoded the original data to a binary structure. This approach was chosen because individuals were not limited in how often they could follow the individualized link. Thus, ‘outcome = 1’ indicates that the link was clicked at least once.
Finally, we also used data from the municipality's list of all residents. This dataset contained residents’ characteristics which we used for covariate adjustment to increase the precision of our estimates. We report models with and without covariate adjustment. First, we included the cluster size to account for our initial block randomization scheme. Second, we included demographic information for each resident in the sample that we assume will affect their intention to get vaccinated. We were able to obtain information about residents’ age (year of birth), gender (female/male), PhD (yes/no), marital status (divorced/single/unknown/married/widowed/marriage dissoluted) and type of residence (sole place of residence/principal domicile).
Statistical analysis
We used ‘R’ to estimate linear probability models with clustered standard errors at the address level to account for potential clustering effects. A binary variable for unique link clicks is the primary dependent variable, and we follow recent methodological advice to estimate treatment effects on binary outcomes with linear regression (Gomila, Reference Gomila2021). While our primary regression model included only the treatment effect, we calculated an additional model including covariate adjustment. We ran these models for both measurement points. Thus, models 1 and 2 specify the treatment effect 1-week post-intervention, while models 3 and 4 indicate the treatment effect 4-weeks post-intervention. This approach was chosen to examine the robustness over time.
Results
Descriptive analysis and balance tests
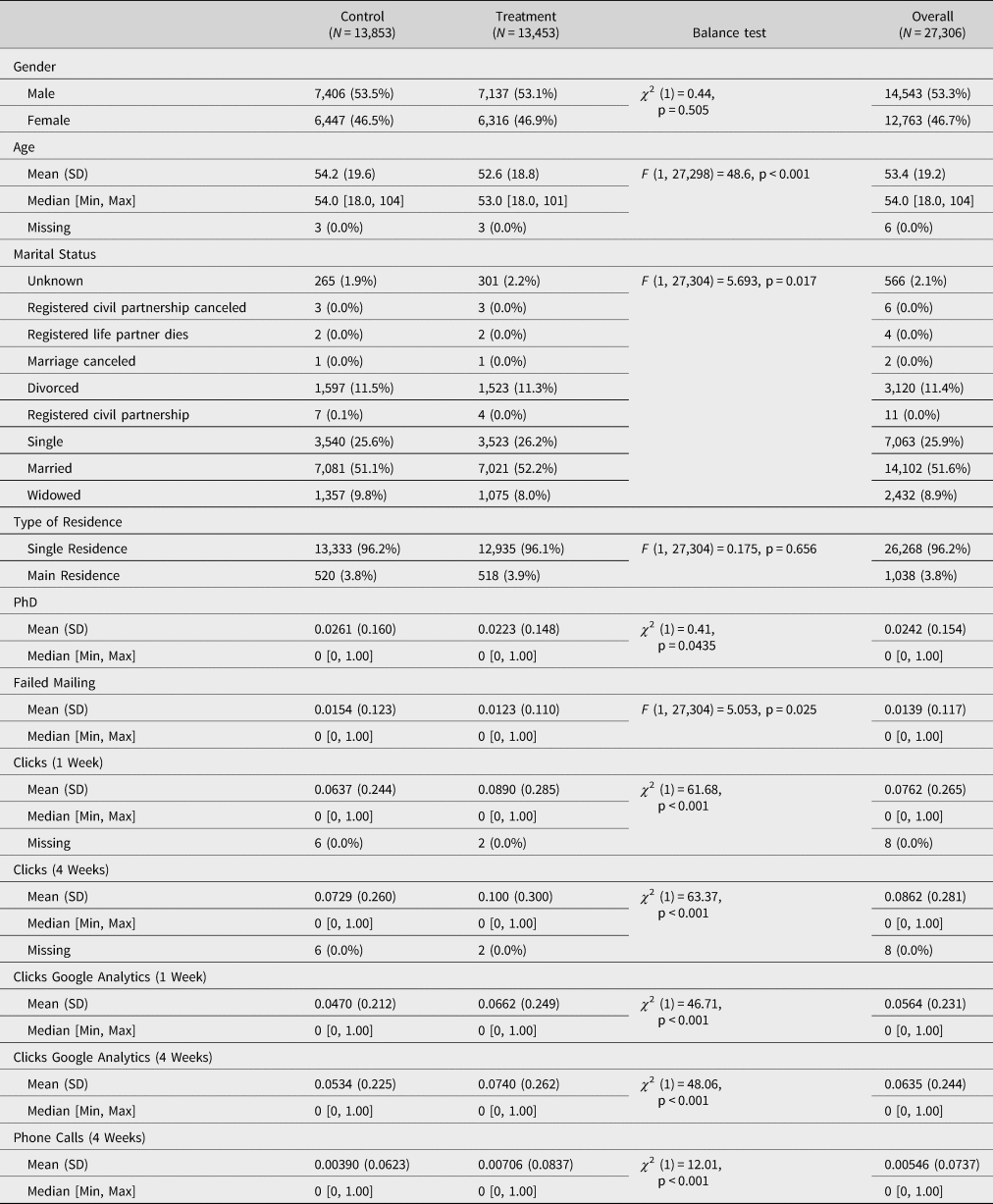
First, Table 1 indicates the distribution of demographic characteristics across experimental groups.Footnote 2 Our sample consists of 53.3% male participants, with a mean age of 54.2 years. While about half of our study population is married (51.6%), 26% are single and some are divorced (11.4%). Descriptive analysis of the outcomes measure shows that 2,080 participants (i.e., 7.62%) clicked the link during the first week following the mailing, while 2,353 (i.e., 8.62%) clicked the link after 4 weeks.
Table 1. Sample characteristics
Hypothesis testing
Table 2 and Figure 1 outline our primary analysis with individual link clicks as the main outcome. Regression models indicate the treatment effects on the percentage of individuals who clicked the link following the mailing. Thus, the regression coefficients can be interpreted as percentage point changes. Each model includes standard errors clustered by addresses to account for the hierarchical data structure.
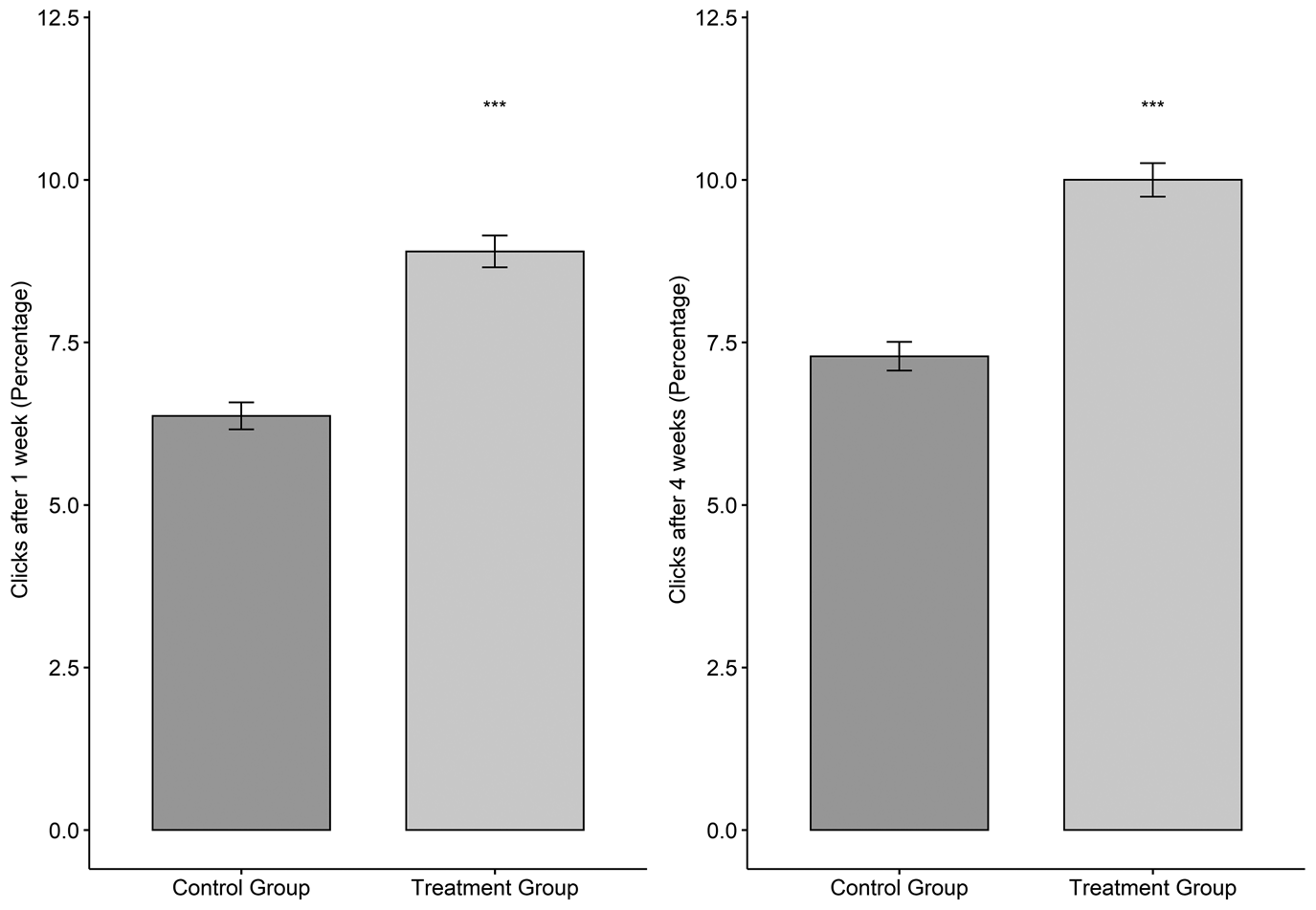
Figure 1. Treatment effects for individual click behavior (1 week & 4 weeks). Note: ***p < 0.0001.
Table 2. Linear probability models for individual click behavior

Linear probability model with clustered standard errors.
Model 1 presents the treatment effect of the psychological ownership intervention without covariate adjustment. As hypothesized, we can observe a positive effect indicating that participants in the treatment group were more likely to click the individualized link compared to the control group (b = 0.025, SE = 0.004, p < 0.0001). This effect amounts to a 2.5 percentage points increase in individual link clicks. To test whether this treatment effect sustains over a considerable time, we also analyzed participants’ click behavior 4-weeks post-intervention. Model 3 outlines the treatment effect without covariate adjustment. The effect for psychological ownership remains statistically significant (b = 0.027, SE = 0.004, p < 0.0001) and amounts to 2.7 percentage points. As shown in Figure 1, the treatment group exhibits a consistently higher share of participants who clicked the individualized link (8.9% after 1 week and 10% after 4 weeks compared to 6.4% and 7.3% in the control condition, respectively).
We further conducted exploratory heterogeneous subgroup analyses. First, age negatively relates to the likelihood of clicking (b = 0.001, SE = 0.000, p < 0.0001). Second, individuals with a main residence are more likely to click (b = 0.023, SE = 0.01, p = 0.0223) compared to sole residence.Footnote 3 Third, individuals with a canceled registered partnership (b = −0.071, SE = 0.012, p = 0.002) and those witha deceased registered civil partner (b = −0.058, SE = 0.015, p = 0.048) were less likely to follow the link compared to single individuals. Fourth, women were more likely to click the link compared to men (b = 0.012, SE = 0.003, p < 0.0001).
To further test the robustness of our findings, we obtained Google Analytics data from the municipality's website (Supplementary Appendices E and F). Due to the limitations of this measurement approach, the identification of click behavior is less reliable than the API data of the individualized links. However, both experimental groups should be equally affected. These additional robustness test yields similar findings compared to the original models. Indeed, the share of participants who clicked the link is 1.9 (1 week) and 2.1 (4 weeks) percentage points higher in the treatment group (1 week: b = 0.019, SE = 0.003, p < 0.0001; 4 weeks: b = 0.021, SE = 0.003, p < 0.0001). Finally, Supplementary Appendix G analyses the results regarding phone calls received in the 4 weeks following the mailing of the letter. It suggests that the positive impact of psychological ownership extends to the number of phone calls following the mailing campaign (4 weeks: b = 0.003, SE = 0.001, p = 0.0017).
To further strengthen our confidence in the findings’ robustness, we computed logistic regression models, adjusted p-values for multiple comparisons with Benjamini–Hochberg corrections (Benjamini & Hochberg, Reference Benjamini and Hochberg1995), and implemented randomization inference procedure (Young, Reference Young2019) for the treatment effects. The results for all three analytical approaches confirm the findings from the linear probability models.
Discussion
Our findings show that subtle textual amendments emphasizing psychological ownership can substantially boost people's intentions to make vaccination appointments. The applied psychological ownership treatment significantly outperformed the control group letter by 2.5 percentage points (39% increase) 1-week post-intervention. The empirical results are robust to using a different measurement instrument (i.e., Google Analytics) and precisely estimated as they are well above the MDE identified through power calculations.
Furthermore, we can observe a substantial treatment effect both 1-week and 4-weeks post-intervention. Compared to the treatment effect size of physical letters in other nudging contexts of 2.41 percentage points (DellaVigna & Linos, Reference DellaVigna and Linos2022), psychological ownership is an impactful approach to motivating individuals. Notably, we estimated our treatment effect in comparison to a control letter. In contrast, other nudging studies typically compare the intervention to a ‘business-as-usual’ condition, which often means no letter at all. Hence, our study produces a rather conservative estimate because our intervention will likely be even more impactful if we consider a situation in which residents receive no letter.
Based on the results, we estimate the downstream effect of the letter intervention on vaccination uptake. We presume that most individuals who clicked the link to set up a vaccination appointment will stick to it. This constitutes a strong assumption, and we caution not to take this thought experiment at face value. Instead, it is an optimistic upper bound of what is possible to achieve, in similar contexts, with low-cost nudge strategies based on psychological ownership (see, for example, Milkman et al., Reference Milkman, Gandhi, Patel, Graci, Gromet, Ho, Kay, Lee, Rothschild, Bogard, Brody, Chabris, Chang, Chapman, Dannals, Goldstein, Goren, Hershfield, Hirsch and Duckworth2022). Indeed, previous research indicates that revealed intentions, based on participants’ clicks, constitute strong predictors of actual behavior (Godin & Kok, Reference Godin and Kok1996; Webb & Sheeran, Reference Webb and Sheeran2006; de Bruin et al., Reference de Bruin, Sheeran, Kok, Hiemstra, Prins, Hospers and van Breukelen2012). Our expectation is also derived from previous research (Jensen et al., Reference Jensen, Ayers and Koskan2021), which indicates that up to 90% of individuals keep their vaccination appointments and actually show up (Dai et al., Reference Dai, Saccardo, Han, Roh, Raja, Vangala, Modi, Pandya, Sloyan and Croymans2021). Following this logic, we estimate that the control letter alone has led to about 908 actual vaccinations and the treatment letter to 1210 actual vaccinations. This would add up to roughly 300 additionally vaccinated individuals by simply adding personal pronouns to a mail-based vaccination campaign. Of course, factors influencing the uptake of vaccination appointments are plentiful and diverse for specific diseases.
In terms of the cost-effectiveness of our intervention, no additional costs arise because a regular information campaign is the status-quo. Emphasizing the psychological ownership of vaccinations in an existing information campaign offers considerable potential for public health practitioners. The total campaign costs were about 22,000 €, i.e., about 0.8 € per resident (n = 27,298). Following the above-calculated estimation of 2118 additional vaccinations, the local government invested approximately 12 € for an additional vaccination in the control group, compared to approximately 9 € in the treatment group.
Concerning behavioral public policy research debates (Hertwig, Reference Hertwig2017; Hertwig & Grüne-Yanoff, Reference Hertwig and Grüne-Yanoff2017; Banerjee & John, Reference Banerjee and John2021), it might be worth noting that the psychological ownership mechanism might be qualified as a nudge plus intervention. While nudges happen ‘automatically without much conscious thought on the part of the individual’ (Banerjee & John, Reference Banerjee and John2021, p. 1), a nudge plus incorporates ‘reflective strategy embedded into the design of a nudge’ (Banerjee & John, Reference Banerjee and John2021, p. 2). In turn, boosting works by fostering the competence of individuals to use their heuristics in a smart way (Hertwig, Reference Hertwig2017; Hertwig & Grüne-Yanoff, Reference Hertwig and Grüne-Yanoff2017). As outlined, the psychological ownership mechanism speaks to both active reflections of the public good's value and the emotional, relatively automatic reactions related to self-esteem. A psychological ownership intervention might be best described as a nudge plus based on these considerations.
Next to the specific vaccination setting of our study, we expect the mechanism should be applied in other policy areas where government agencies face similar challenges. Generating a feeling of individual ownership of public goods can benefit the provision of said goods and potentially reduce free-riding problems. In the context of COVID-19, psychological ownership may contribute to several practical aspects, such as contact tracing (Horvath et al., Reference Horvath, Banducci and James2022) or data sharing (Belle et al., Reference Belle, Cantarelli and Battaglio2021). Both problem settings include contributions to an intangible public good based on individualized action.
Apart from the ongoing pandemic, we suggest that psychological ownership may also contribute to the literature on coproduction, which often focuses on individuals’ contributions to public goods (James & Jilke, Reference James and Jilke2020). A variety of coproduction contexts, such as neighborhood patrols (Uzochukwu & Thomas, Reference Uzochukwu and Thomas2018) or lay judge services (Sievert, Reference Sievert2021), could benefit from psychological ownership interventions. Psychological ownership offers a complementary measure to ensure the persistence of coproduction (Steen & Brandsen, Reference Steen and Brandsen2020). These various aspects constitute urgent issues related to the provision of public goods. Future research on public goods provision may also benefit from testing the concept of collective ownership (‘OUR’ public good) as an intervention to improve essential outcomes (Pierce & Jussila, Reference Pierce and Jussila2010). Indeed, previous studies have indicated that shared or collective ownership can positively affect cooperative behaviors (Giordano et al., Reference Giordano, Patient, Passos and Sguera2020).
Overall, this study offers several important implications for practitioners. It presents a successful ‘real-world’ test of a behavioral intervention to increase people's intention to make a vaccination appointment. In line with prior studies (Dai et al., Reference Dai, Saccardo, Han, Roh, Raja, Vangala, Modi, Pandya, Sloyan and Croymans2021; Sprengholz et al., Reference Sprengholz, Eitze, Felgendreff, Korn and Betsch2021; Milkman et al., Reference Milkman, Patel, Gandhi, Graci, Gromet, Ho, Kay, Lee, Akinola, Beshears, Bogard, Buttenheim, Chabris, Chapman, Choi, Dai, Fox, Goren, Hilchey and Duckworth2021b, Reference Milkman, Gandhi, Patel, Graci, Gromet, Ho, Kay, Lee, Rothschild, Bogard, Brody, Chabris, Chang, Chapman, Dannals, Goldstein, Goren, Hershfield, Hirsch and Duckworth2022), the findings underline that active and direct communication of government agencies can lead to a significant increase in the desired behavior. Adding subtle textual amendments to trigger a feeling of ownership can boost desired behaviors. Such interventions offer public officials a practical, low-cost and easy-to-implement approach to decrease vaccine hesitancy (Betsch et al., Reference Betsch, Böhm, Korn and Holtmann2017; Randolph & Barreiro, Reference Randolph and Barreiro2020), at least in the early days of vaccine distribution (Thaler, Reference Thaler2021). The present study also adds to current discussions around vaccination policies. In particular, we propose a mild, unobtrusive measure worthy of attention in current policy discussions.Footnote 4 Still, caution is warranted as recent empirical results indicate that mere information cues about the vaccination appear ineffective (Dai et al., Reference Dai, Saccardo, Han, Roh, Raja, Vangala, Modi, Pandya, Sloyan and Croymans2021). Moreover, the tangible medium (letter vs text messages), trust in the messenger (Everett et al., Reference Everett, Colombatto, Awad, Boggio, Bos, Brady, Chawla, Chituc, Chung, Drupp, Goel, Grosskopf, Hjorth, Ji, Kealoha, Kim, Lin, Ma, Maréchal and Crockett2021) and the timing might play a role. For instance, other studies have shown null results for text messages targeting hesitant people (Rabb et al., Reference Rabb, Swindal, Glick, Bowers, Tomasulo, Oyelami, Wilson and Yokum2021). In addition to low-touch approaches such as behaviorally informed communication, there is a need for other methods like incentives and policy measures such as testing (Thunström et al., Reference Thunström, Ashworth, Shogren, Newbold and Finnoff2021). However, current techniques such as vaccine regret lotteries do not seem to deliver on their promises (Milkman et al., Reference Milkman, Gandhi, Ellis, Graci, Gromet, Mobarak, Buttenheim, Duckworth, Pope, Stanford, Thaler and Volpp2021a), and future research is needed.
We also note that ownership cues may not work for everybody. Indeed, vaccine hesitancy is strongly linked to people's partisan orientation and distrust in institutions (Gadarian et al., Reference Gadarian, Goodman and Pepinsky2021; Petersen et al., Reference Petersen, Bor, Jørgensen and Lindholt2021). Low-touch communication strategies will not persuade those who strongly oppose vaccinations. However, targeting individuals most amenable to motivational cues – such as those who want to get vaccinated but have not followed through – would be a reasonable possibility to increase vaccination rates further. That being said, the proportion of individuals that can be mobilized via nudges is highly likely inversely related to the timing of the vaccine rollout among a country's entire population. However, as policy debates about booster vaccinations become more salient (Callaway, Reference Callaway2021), the application of low-touch interventions to increase vaccine uptake will gain renewed importance. We have shown that psychological ownership interventions are likely an effective tool in this conjunction.
The present field experiment has strengths in terms of external validity but also limitations. A potential limitation is that we cannot differentiate whether the intervention mobilized people to get vaccinated who would otherwise not or whether some residents got vaccinated a few weeks or months earlier. Still, accelerating vaccination uptake is meaningful to public health and has clinical relevance. Hence, we argue that even earlier vaccinations have significant positive externalities and contribute to the public good of herd immunity. The second shortcoming is that we cannot single out the precise mechanism(s) behind the observed effect resulting from the psychological ownership intervention. Future research should help better understand the two theoretical mechanisms of the increased value of the public good and increased self-esteem and prosocial behavior and how they trigger a feeling of ownership. Arguably, lab-based experiments and qualitative interviews would be helpful to better understand the micro-level motivations behind psychological ownership and its effect on behavior.
Conclusion
This study has important implications for enhancing the uptake of COVID-19 vaccines and the provision of public goods more broadly. Our study shows that feelings of ownership, elucidated with subtle and low-cost textual amendments, positively affect people's intentions to make a vaccination appointment. These findings indicate that such behavioral enhancement applied to official communication constitutes an impactful approach. Promoting vaccinations at scale requires a range of strategic policy instruments. Still, it is promising to start with easy-to-implement, low-cost enhancements in government agencies’ communication campaigns.
Nonetheless, for currently unvaccinated residents, vaccine hesitancy can mainly be attributed to misinformation, political polarization and low trust in institutions. Consequently, designing nudge-type interventions and more high-touch interventions such as monetary incentives (Campos-Mercade et al., Reference Campos-Mercade, Meier, Schneider, Meier, Pope and Wengström2021) might be helpful in these cases. Noteworthy, practitioners are to profit from rigorously testing trials in the field and identifying the most effective interventions before deploying them at scale (Dai et al., Reference Dai, Saccardo, Han, Roh, Raja, Vangala, Modi, Pandya, Sloyan and Croymans2021). Overall, as policymakers and government agencies strive to develop communication strategies to foster benefit uptake and prosocial behavior, effective psychological ownership interventions can become part of their toolkit.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/bpp.2022.16.
Acknowledgments
The authors thank the municipal administration of Bad Nauheim, especially Mayor Klaus Kreß, Matthias Wieliki, Madeline Schuhmann, and Oliver Wolf, as well as the local healthcare officials Prof. Dr. H. Ardeschir Ghofrani (Kerckhoff-Klinik) and Prof. Dr. Dr. Friedrich Grimminger (Gesundheitszentrum Wetterau). The authors also thank Andreas Paech, Moritz Motyka, and Elena Moschinski for their instantaneous support before and during the data collection.
Financial support
The authors received no financial support for this article's research, authorship and/or publication.
Competing interest
The authors declare none.
Ethical standards
We received the ethical approval for this field experimental study of Zeppelin University, Friedrichshafen, Germany on April 15, 2021.






 Open access
Open access