


No CrossRef data available.
Published online by Cambridge University Press: 16 September 2024
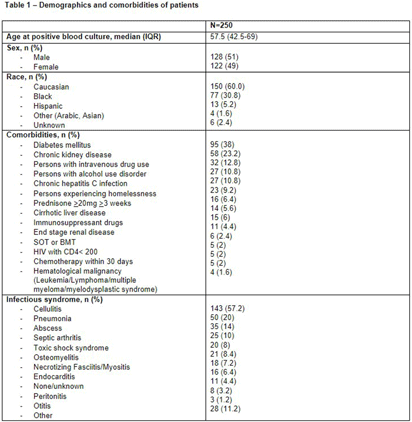
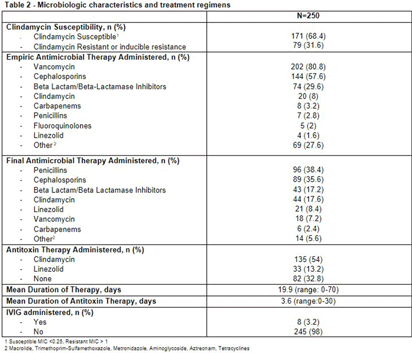
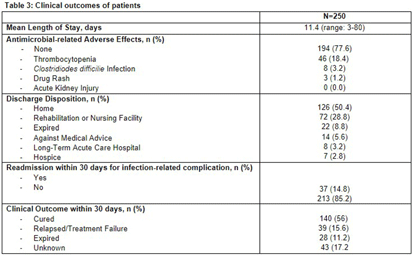
Background: Group A Streptococcus (GAS; Streptococcus pyogenes) is an important human pathogen that can cause life-threatening invasive disease, ranging from skin/soft tissue infections to infective endocarditis. In the fall of 2022, the Center for Disease Control & Prevention (CDC) issued an alert due to a global increase in invasive GAS infections, particularly among children and adults with co-morbidities. An increase in invasive disease was observed at our five-hospital healthcare system in Southeast Michigan. The objective of this study was to describe characteristics of patients with invasive GAS and characterize treatment and outcomes of disease. Methods: This was a retrospective cross-sectional study of patients from June 2013 to August 2023 with positive blood cultures for GAS. Patients were identified using a data query for positive blood cultures for GAS through Microsoft SQL Server. Patients with age < 1 8 years, polymicrobial bacteremia, incomplete data, or who were enrolled in hospice and/or died within 48-hours of admission were excluded. Collected variables included: demographics, infection characteristics (syndrome, duration of bacteremia), microbiological characteristics (antimicrobial susceptibility testing; AST), antimicrobial treatment (empiric and final, antitoxin therapy), and clinical outcomes (length of hospital stay [LOS], treatment-associated adverse events, 30-day mortality and infection-related readmission). Results: 250 patients were included (Table 1). More than half were male with median age of 57.5 years. Diabetes mellitus (38%) and chronic kidney disease (23%) were common comorbidities [Table 1]. Persons experiencing homelessness and persons who use injection drugs accounted for 9% and 13% of the cases, respectively. The most common infective syndrome accompanying bacteremia was cellulitis (57%). The majority of patients received vancomycin for empiric therapy (81%) and penicillin (38%) or cephalosporin (36%) for final regimen [Table 2]. A total of 79 GAS isolates (32%) were clindamycin resistant. Clindamycin was included in the empiric regimen of 20 (8%) patients, the final regimen in 44 (18%) of patients, and as antitoxin adjunct therapy in 135 (54%) of patients. A third (33%) of patients received no antitoxin. The average duration of antitoxin therapy was 3.6 days and antimicrobial therapy 19.9 days. The mean LOS was 11.4 days (Table 3). Thirty nine (16%) patients had treatment failure and 8 (3%) experienced C. difficile infection within 30 days of antimicrobial treatment. Thirty-day mortality was 11%; of these, 9% had in-hospital mortality. Conclusions: Invasive GAS infection confers significant morbidity and mortality, and ongoing research is needed to determine the best treatment regimens in the era of increasing clindamycin resistance.
 You have
Access
You have
Access
 Open access
Open access