



Introduction
While participation in various forms of unpaid activities (such as informal care-giving, formal volunteering in clubs or associations, informal volunteering beyond such organisations and domestic work) has long been identified as important for the welfare of society, getting a better understanding of how these activities influence each other remains important. In addition, while we know from previous research that societies differ in how far they encourage these activities, it remains to be understood which societal circumstances enable multiple engagement. Unpaid activities can take place in the private realm (e.g. providing informal care or giving help to relatives or neighbours) or in the public realm (e.g. formal volunteering in clubs or associations). This article focuses on two types of unpaid activities in the second half of life, namely formal volunteering in clubs and associations, on the one side, and informal help and care-giving, on the other side. Both types of activities are especially prevalent among the so-called ‘young old’ (see e.g. Hank and Stuck, Reference Hank and Stuck2008: 1281).
At the same time, we observe for both activities (informal help or care-giving and formal volunteering) a north–south gradient, with much higher involvement rates in Northern European countries than in Southern ones (for care-giving, see Brandt et al., Reference Brandt, Haberkern and Szydlik2009; for volunteering, see Hank and Erlinghagen, Reference Hank and Erlinghagen2010). Although it has been shown that both volunteering and informal care-giving in the second half of life are partly influenced by the same societal circumstances (such as government social spending; see Hank, Reference Hank2011), many studies rely on cross-sectional data and the comparative dimension in the relationship between the two is not yet well understood.
Both activities have much in common. They have been described as ‘productive’ (for a discussion of the term, see e.g. Van der Meer, Reference Van der Meer2006) and are (normally) unpaid, but they differ in important ways: while the provision of informal help or care for older adults mostly takes place within the private realm of the family and – to a much lesser extent – of friends and neighbours, formal volunteering is a public activity that takes place in clubs or associations. While the provision of informal help or care for older adults is mostly associated with a (moral) obligation to care for frail family members (Haberkern and Szydlik, Reference Haberkern and Szydlik2010), volunteering in clubs and associations is conceptualised as a decision that is taken freely (Wilson and Musick, Reference Wilson and Musick1997). Depending on the welfare state context, volunteering can mean different things, however: In the Anglo-Saxon context, volunteering is very often associated with help and support for needy groups; in the Scandinavian context, with its much more elaborated welfare state provision, volunteering is much more associated with leisure organisations in the field of sports, culture, hobby and recreation, on the one hand, and political and interest organisations, such as handicap organisations, patient organisations or unions, on the other hand (Henriksen et al., Reference Henriksen, Strømsnes, Svedberg, Henriksen, Strømsnes and Svedberg2018).
The question to be answered in this article is thus how the provision of informal help or care in the second half of life influences the likelihood of formal volunteering, and how this relationship is framed by a country's societal background, such as welfare state expenditure, family norms and female labour market participation. It is important to note, however, that we cannot empirically trace the mechanisms by which societal circumstances on the macro level impact on individuals’ decisions to become involved in formal volunteering.
The article proceeds as follows. In the next section, I summarise existing knowledge on the link between informal help/care-giving and formal volunteering in the second half of life at the individual level. I then present two theoretical approaches that attempt to explain this link. In the following section, I discuss previous literature referring to the question as to why we should expect the relationship between the two activities to vary between different country contexts. I then present the data that I use for my empirical analysis and my analytic strategy, as well as descriptive and multivariate results. The article ends with a discussion of how this study contributes to existing knowledge.
The nexus between providing informal care and volunteering in the second half of life
In this section, I first spell out my definition of formal volunteering and informal help and care-giving, before summarising the existing knowledge on the interrelation between care-giving and volunteering. Various authors have stressed the difficulty of defining volunteering and of distinguishing it from other helping activities (see e.g. Wilson, Reference Wilson2000). By formal volunteering, I refer to activities that are voluntary and unpaid, that are provided to people outside the family and that are organised by a club (or a stable group) for a certain period of time (for an overview of the term and how it is distinguished from other activities, see Wilson, Reference Wilson2000; Ehrhardt, Reference Ehrhardt2009; Henriksen et al., Reference Henriksen, Strømsnes, Svedberg, Henriksen, Strømsnes and Svedberg2018). Informal care, on the other hand, is provided mostly to older family members, such as a spouse (32%) or parent (36%), while a smaller proportion is provided to other relatives (18%) or friends (18%) (Colombo et al., Reference Colombo, Llena-Nozal, Jérôme Mercier and Tjadens2011: 90). Informal help comprises support with instrumental activities of daily living (IADL), such as cooking, shopping or cleaning; informal care-giving is understood as support with activities of daily living (ADL), such as washing, feeding, or dressing (Walker et al., Reference Walker, Pratt and Eddy1995). On average, informal care-giving is much more time-consuming than volunteering: while 46 per cent of informal care-givers in Europe report that they give care almost daily and another 34 per cent almost every week, only 18 per cent report volunteering almost daily, and 45 per cent almost every week. Informal help ranges in between with 26 per cent reporting helping almost daily and 42 per cent helping almost every week (Stuck, Reference Stuck2006).
Several studies have analysed the interrelation between different forms of (unpaid) activities among middle-aged and older adults, e.g. between intergenerational help and care (Brandt et al., Reference Brandt, Haberkern and Szydlik2009), or between volunteering, informal help and care-giving (Hank and Stuck, Reference Hank and Stuck2008). A number of studies report a positive relationship between informal care-giving and formal volunteering. Most of them state that among middle-aged and older women, care-giving does not reduce the frequency of participation in formal volunteering activities (Farkas and Himes, Reference Farkas and Himes1997). Instead, the share of volunteers is between one and a half (Sweden, Denmark, The Netherlands) and two times (Italy, Greece) higher among those who have helped or cared (Erlinghagen and Hank, Reference Erlinghagen, Hank, Börsch-Supan, Brugiavini, Jürges, Mackenbach, Siegrist and Weber2005). Similarly, Hank and Stuck (Reference Hank and Stuck2008) find a strong positive relation between different unpaid activities, including volunteer work and informal care-giving, that remains significant when controlling for other individual characteristics, such as age, employment status and health. The authors interpret the results as indicating an unobserved determinant of all three activities at stake (volunteering, care-giving, informal help), such as a general motivation to be active (Hank and Stuck, Reference Hank and Stuck2008). For the United States of America (USA), Burr et al. (Reference Burr, Choi, Mutchler and Caro2005) report that older adult care-givers are more likely to be volunteers than their non-care-giving peers. They conclude that this effect is stronger for care-givers with a high degree of involvement (in terms of annual care-giving hours) and for those providing care to non-relatives. Similarly, Jegermalm and Jeppson-Grassman (Reference Jegermalm and Jeppson-Grassman2009) show for Sweden that a substantial share of middle-aged and older adults are involved in both informal care-giving and volunteering activities. Other studies, however, report that female care-givers are less likely than non-care-givers to be engaged in (formal and informal) volunteering, while men's volunteering activities are not affected by their care-giving (Taniguchi, Reference Taniguchi2006; Choi et al., Reference Choi, Burr, Mutchler and Caro2007). Looking at the dynamics of care-giving, McNamara and Gonzales (Reference McNamara and Gonzales2011) report that care-giving responsibilities in relation to a parent did not appear to be associated with starting to volunteer. Instead, providing care to a parent or spouse represented a barrier to volunteering intensity and a facilitator in relation to ceasing to volunteer. This is also supported by qualitative research reporting that some older volunteers refer to other productive activities, such as care-giving, as a reason for stopping their volunteering activity (Tang et al., Reference Tang, Morrow-Howell and Choi2010).
Generally, one has to conclude that existing studies on the relationship between care-giving and volunteering mostly rely on cross-sectional data, or at most data with two points of measurement (note the exception of McNamara and Gonzales (Reference McNamara and Gonzales2011) who used five waves of the US Health and Retirement Study). Some studies are restricted in the sense that they deal only with women (Farkas and Himes, Reference Farkas and Himes1997) or spousal care-giving (Choi et al., Reference Choi, Burr, Mutchler and Caro2007). Although several studies discuss the issue of unobserved heterogeneity (see e.g. Burr et al., Reference Burr, Choi, Mutchler and Caro2005: S255), none uses the obvious strategy of estimating fixed-effect models. By focusing on within-person variability over time, these models control for time-constant unobserved influences, such as unmeasured personality characteristics which influence both care-giving and volunteering participation, as has been suggested by Hank and Stuck (Reference Hank and Stuck2008). By using fixed-effect models, we are thus able to identify an unbiased effect of care-giving on volunteering, net of time-constant unobserved heterogeneity, which allows us to make cautious interpretations regarding causal inference.
Moreover, most studies on the relationship between care-giving and volunteering rely on data from a single country – mostly the USA, but in one case Sweden. Only Hank and colleagues (Erlinghagen and Hank, Reference Erlinghagen, Hank, Börsch-Supan, Brugiavini, Jürges, Mackenbach, Siegrist and Weber2005; Hank and Stuck, Reference Hank and Stuck2008) use European comparative data (the first wave of the Survey of Health, Ageing and Retirement (SHARE)) to address the interrelation between care-giving and volunteering. Although they report different effect sizes in the relationship between care-giving and volunteering between countries, they do not develop hypotheses on moderating macro effects at the country level. I aim to address this additional research gap with my own analysis.
Theoretical approaches: why do care-givers volunteer more (or less) often?
When looking at the interplay between formal volunteering and informal care-giving, two opposite theoretical models are discussed. On the one hand, the role extension hypothesis claims that care-givers might be more likely to volunteer because their care-giver role brings them into contact with people and organisations that provide them with opportunities for volunteering (Choi et al., Reference Choi, Burr, Mutchler and Caro2007). The reason is that many care-givers receive assistance from other family members and/or professional organisations. This can be expected to be especially relevant for those who care outside their own household, e.g. for their parents, because they are usually part of a network of different formal and/or informal care-givers (Jacobs et al., Reference Jacobs, Broese van Groenou, Aartsen and Deeg2016), especially if their time investment is not too high. Instead, care-giving inside their own household often means partner care, which is associated with higher care intensity and is likely to be performed as solo care (Bertogg and Strauß, Reference Bertogg and Strauß2020) which does not provide possibilities for enlarging one's social networks. Apart from enlarging their social networks through their contacts with other members of a care-giving network, care-givers develop skills that are valuable for volunteering organisations, both practical knowledge in terms of performing care-giving activities as well as communication skills, knowledge about the medical and social security system, and (para-medical) knowledge about the needs of care recipients. They might thus be asked more frequently by other volunteers whether they want to join their club or association; such requests have been shown to be the most important reason for volunteering (Burr et al., Reference Burr, Choi, Mutchler and Caro2005).
Moreover, from the perspective of the informal care-giver, participation in volunteering activities may provide temporary relief from care-giving responsibilities. Thus, volunteering might not be seen as an additional burden, but instead be a valuable way to ‘break out’ of the private realm and help reduce the isolation or psychological strain that is often a side-effect of extensive care-giving (Choi et al., Reference Choi, Burr, Mutchler and Caro2007). A similar idea is put forward by theorists distinguishing between bridging (or encompassing) and bonding (or inward-looking) social networks (Putnam, Reference Putnam2000; Geys and Murdoch, Reference Geys and Murdoch2008). While formal volunteering has been associated with bridging social networks, informal care-giving is related to bonding social networks. This might also be the reason why we observe that older adults who engage in multiple productive activities concurrently, such as care-giving and volunteering, report a better state of health (Rozario et al., Reference Rozario, Morrow-Howell and Hinterlong2004). I assume, however, that this is a mechanism which can be expected mainly for sporadic help outside the household since this leaves enough time and energy to commit additionally to volunteering activities.
On the other hand, the role overload approach argues that care-giving for a disabled person is usually a stressful experience that often requires the commitment of a large amount of time and effort, and is both a physical and emotional challenge (Choi et al., Reference Choi, Burr, Mutchler and Caro2007). This should be especially prevalent for those with intensive care-giving obligations and care given inside an individual's own household because this type of care-giving involves mainly partner care, which is often provided without other formal or informal support (Bertogg and Strauß, Reference Bertogg and Strauß2020). Consequently, this perspective would anticipate that volunteers who are confronted with a relative's (or friend's) need for care are at risk of decreasing their voluntary engagement, or of ending it completely.
Even though these two theoretical approaches make different assumptions about care-givers’ resources, preferences and needs, they do not necessarily contradict each other. While the role extension hypothesis might apply better to care-givers who provide sporadic care outside their own household, the role overload hypothesis might apply better to those who provide care inside their own household as well as those who provide intensive care outside their own household. I therefore expect that
• individuals providing help/care inside their own household as well as those providing intensive help/care outside their own household are less likely to volunteer.
At the same time, i expect that
• individuals providing sporadic help/care outside their own household are more likely to volunteer.
Volunteering and care-giving from an international perspective
In addition to these individual-level arguments, the relationship between informal care-giving and volunteering could be influenced by the societal context in which they take place. Based on Esping-Andersen's (Reference Esping-Andersen1990) classical welfare state typology, Lamura et al. (Reference Lamura, Mnich, Nolan, Wojszel, Krevers, Mestheneos and Döhner2008) differentiate between four (to five) types of European care regimes: the Scandinavian model (e.g. Sweden), characterised by high public investments in home/residential care and a residual family role; the liberal, means-tested model (e.g. the United Kingdom), focusing on public care to those in need, implying a broader role for private care providers; the subsidiarity model (e.g. Germany) which allocates primary responsibilities to families, backed up by a long-term care insurance scheme funding care services provided by religious and non-governmental organisations; the family-based model (e.g. Greece and Italy) with limited public service provision, a central role being played by kinship networks; and the transition model (e.g. Poland), resembling the family-based countries, but facing more severe financial constraints (Lamura et al., Reference Lamura, Mnich, Nolan, Wojszel, Krevers, Mestheneos and Döhner2008). Previous research has shown how these welfare state regimes differ in regard to informal care-giving and help by family members (Brandt et al., Reference Brandt, Haberkern and Szydlik2009). In Northern Europe, help between parents and children is very common but typically consumes little time. In the South, to the contrary, we observe fewer support relations which are, however, very time-intensive. Central Western Europe lies in between with average transfer rates and intensities. Brandt et al. (Reference Brandt, Haberkern and Szydlik2009) conclude that with increased public transfers and social services, sporadic help is more likely (crowding in), and less time-consuming support between generations (crowding out) occurs. Hank (Reference Hank2011) similarly shows a positive effect of public social spending (as well as greater political and religious freedom) on volunteering as well as help and informal care-giving.
In order to explain this effect, the so-called ‘crowding-in’ hypothesis assumes that countries with high social expenditure encourage civic engagement through a variety of direct or indirect supportive interventions, such as programmes that provide incentives to volunteer, investment in education to prepare people for active ageing roles or local infrastructure that offers opportunities for volunteering (Hank, Reference Hank2011). Many empirical studies indeed find higher shares of socially engaged citizens in countries with high welfare expenditure (Salamon and Sokolowski, Reference Salamon, Sokolowski, Dekker and Halman2003; Motel-Klingebiel et al., Reference Motel-Klingebiel, Tesch-Roemer and Von Kondratowitz2005).Footnote 1 As informal care-givers, especially those who care outside their own household, have a higher likelihood of being part of a care-giving network of formal and informal care-givers, this should increase their chance of being asked to volunteer. I therefore assume that social expenditure ‘crowds in’ informal care-givers – especially those who care outside their own household – even more than non-care-givers.
In order to understand better the effect of social expenditure on the relationship between care-giving and volunteering, I further differentiate between two types of support for informal care-givers, namely cash-for-care and care-in-kind schemes. While care-in-kind schemes provide publicly funded – most of the times formal – home-care services, cash-for-care schemes provide cash allowances that are paid mostly to the care recipients who can use them (among other possibilities) to employ informal care-givers, such as family members (Da Roit and Le Bihan, Reference Da Roit and Le Bihan2010).Footnote 2 Cash-for-care schemes thus tend to promote informal care-giving arrangements. Above-average expenditures for care-in-kind can be found in Sweden and Denmark; above-average expenditures for cash-for-care are found in Italy, France, Austria, Slovenia and Germany (for an overview, see Figure A1a, b in the Appendix). The assumption is that publicly funded home care services (care-in-kind) are more likely to unburden households with care recipients and enable informal care-givers to participate in formal volunteering activities. This relationship should be especially prevalent for those care-givers who care outside their own household, since they are often part of a care-giver network which consists of different formal and informal care-givers, which increases their likelihood of being asked to participate in volunteering activities. Since the provision of care is organised by public or non-profit organisations where care is often provided by a team of professionals and volunteers (Sozanská et al., Reference Sozanská, Tošner, Frič, Zimmer and Priller2004), it is more visible in public than in countries relying on family care only. This should also increase the chances that members of the non-care-giving population get in contact with care-giving organisations which should in turn increase their volunteering likelihood.
Cash-for-care schemes, on the other hand, increase society's focus on the family as the main provider of welfare, which should stress informal care-givers’ focus on the private sphere. I therefore do not expect any influence of cash-for-care expenditures on the likelihood of non-care-givers’ volunteering. However, care-giving family members in countries that promote these private care solutions should have a higher chance of being part of a private care-giving network. These larger social networks should in turn increase their likelihood of being asked to participate additionally in volunteering. I therefore expect that
• higher expenditure on care-in-kind schemes increases the likelihood of care-givers volunteering to a higher degree than non-care-givers.
Moreover, I expect that
• higher expenditure on cash-for-care schemes increases the likelihood of care-givers volunteering; the likelihood of non-care-givers volunteering should, however, not be affected.
Another theoretical assumption is that in countries with a high level of informal social networks, especially family networks, as is the case in Southern (and some Eastern) European countries, we observe a lower participation in formal volunteering activities (Pichler and Wallace, Reference Pichler and Wallace2007). Although this theoretical expectation does not always find empirical support (Plagnol and Huppert, Reference Plagnol and Huppert2010), i argue that, for our specific sub-group of informal care-givers, the influence of family orientation in a country might even be stronger, since providing care for frail family members is a strong normative expectation. I therefore expect that a high average family orientation (measured as the share of adult children living together with at least one parent) in a country should lead to informal care-givers being involved in volunteering activities. I therefore expect that
• greater family orientation in a country (measured as the share of adult children living together with at least one parent) lowers the likelihood of care-givers being involved in volunteering activities; the likelihood of volunteering for non-care-givers should, however, not be affected.
My last theoretical assumption explaining country differences in the relationship between care-giving and volunteering is related to women's role in society. Thus, a high share of middle-aged women participating in the labour market is associated with women being more active in the public sphere. This assumption is supported by empirical evidence from a Scandinavian study which shows a historical convergence in volunteering between men and women in line with the trend towards women's employment participation (Boje et al., Reference Boje, Hermansen, Møberg, Henriksen, Strømsnes and Svedberg2018). In countries with a lower female labour force participation rate, women's focus on the private sphere of the family, including informal care-giving for family members, should therefore be more widespread. By contrast, in countries with a high share of middle-aged women participating in the labour market, female care-givers should also have a higher likelihood of participating in other activities pertaining to public life, such as formal volunteering in clubs or associations.Footnote 3 From these arguments I expect that
• the greater the middle-aged women's labour force participation in a country, the stronger the positive relationship between care-giving and volunteering participation for women.
Data and sample
To assess my theoretical assumptions empirically, i used data from SHARE, a country-comparative longitudinal study which has surveyed a representative sample of adults aged 50 years or older in a number of European countries repeatedly in the years 2004, 2006, 2010, 2013 and 2015. I restricted my sample to respondents aged between 50 and 80 years of age. Since not all countries have participated in all waves, I further had to restrict my sample. I only included countries which participated in at least three consecutive waves. This leaves me with the following 13 countries: Austria, Germany, Sweden, The Netherlands, Spain, Italy, France, Denmark, Switzerland, Belgium, Czech Republic, Slovenia and Estonia. The overall sample size at the individual level over all waves is about 86,000. Sample sizes in countries vary between about 4,150 in Switzerland and about 8,800 in Belgium. Since my method (see below) requires at least two observations per person, my sample is further reduced to about 35,500 individuals out of which most have two (63%) or three (26%) observation points. From this analytic sample, about 6,400 individuals are involved in volunteering, about 2,300 are care-givers in their own household and about 10,000 provide care outside their own household.
Measures
Information on my dependent variable (volunteering) was captured through a dichotomous variable indicating whether a person reported having participated in volunteering. A difficulty with this variable is that in the first two waves of SHARE, respondents were asked about their volunteering participation in the last month, while the question in the subsequent waves refers to volunteering in the past 12 months. This leads to a higher average volunteering rate in the last three waves (2010: 18.3%, 2013: 19.1%, 2015: 18.4%) than in the first two waves (2004: 14.3%, 2006: 15.2%). Since separate estimations with two sub-samples (including only the first two or only the last three waves) yielded similar results, I decided to pool all waves for my analysis in order to enlarge both my sample size (including the number of countries) and the number of repeated observations.
My main explanatory variable is a person's participation in informal care-giving. I differentiate between respondents who report having cared inside their own household and those who have given care outside their own household. Regarding the first, respondents were asked: ‘Is there someone living in this household whom you have helped regularly during the last 12 months with personal care, such as washing, getting out of bed or dressing?’, followed by a list of persons who might receive the care (to be selected). Regarding the second, they were asked: ‘In the last 12 months, have you personally given personal care or practical household help to a family member living outside your household, a friend or neighbour?’Footnote 4 The question can be answered with ‘yes’ or ‘no’. In the following, respondents who reported giving care outside their own household were asked how often they have given care to three different persons (which they named before). The answer categories are: about daily, about every week, about every month, less often. From these items, I generated a categorical variable indicating whether a person did not give any kind of care (0), whether he or she provided sporadic care (about monthly or less often) outside their own household (1), intensive care (weekly or daily) outside their own household (2) or care inside their own household (3). People who reported providing care both inside and outside their own household were coded as care-givers outside their own household.Footnote 5
At the individual level, the following control variables, which have been shown in previous research to impact on volunteering participation and care-giving, were covered. Age was included in the models as age in years at the time of interview. Health was measured as a self-assessment, with five answer categories ranging from very bad (1) to excellent (5). A person's employment status was captured with three categories: (1) retirement, (2) (self-)employment, and (3) non-employment (respondents being unemployed, permanently sick or disabled, or home-makers). Due to our analytical approach (see below), I did not include any time-constant variables, such as the respondents’ education or gender (for an overview of the distribution of my variables at the micro level, see Table 1).
Table 1. Descriptive statistics of individual variables

Note: SD: standard deviation.
At the macro level, I separately introduced the following four variables in my models: (a) an indicator for the share of adults aged 50 or older in a country who report living in the same household or building with at least one of their parents – this indicator was aggregated over the five waves from my analytic data-set; (b) the share of women aged between 50 and 64 in a country participating in the labour market; (c) public expenditure on old-age cash benefits as a percentage of a country's Gross Domestic Product (GDP); and (d) public spending on old-age in-kind as a percentage of a country's GDP. While the female labour force participation rate is retrieved from Eurostat data, data on social spending are provided by OECD Statistics. All macro indicators were included in the models as lagged effects, i.e. I included information from one year before the respective survey wave was conducted.
What i observe empirically is that countries do not only vary substantially in their level of care-in-kind expenses but that the development over time is also rather different: while countries with a high level of care-in-kind expenses, like Sweden or Denmark, have seen substantial cut-backs in the last years, other countries with rather low care-in-kind expenses, like Belgium or Austria, have seen slight increases over the past years; in other countries (Germany, Italy, Czech Republic) care-in-kind expenses remained low over the entire observation period (see Figure A1a in the Appendix). For cash-for-care expenditures, i see again interesting country differences not only regarding the level of expenses but also the development: thus, countries like Austria, France and Italy, which already had comparatively high expenses at the beginning of the 2000s have still increased their expenses; in other countries i also see an increase in expenses but on a lower level (Denmark, Belgium, Czech Republic); in a few countries (Germany, Estonia) i find a decrease in expenses or a continuous low level (Switzerland, The Netherlands) (see Figure A1b in the Appendix). I also see that the share of the adult population in a country that lives together with at least one parent is on a constantly low level especially in Northern European countries (Sweden, Denmark, The Netherlands), while some of the countries with generally high levels in this indicator have increased their share in the last years (Italy, Slovenia, Czech Republic) (see Figure A1c in the Appendix). As to the share of employed women aged 50–64 years, we see in all countries a steady increase, although on very different levels; however, for countries with very high participation rates the increase has flattened in the past years (Sweden, Switzerland, Estonia) (see Figure A1d in the Appendix).
Analytical strategy
As discussed in the literature review, it seems essential for my analytical strategy to control for time-constant unobserved heterogeneity. This should circumvent the limitations of earlier research, namely that it remains unclear whether care-giving per se influences a person's likelihood of volunteering or whether we observe instead a special group of ‘super helpers’ who, due to specific personality characteristics, are more likely to get involved in care-giving as well as in volunteering. I therefore decided to use conditional fixed-effect logistic regression models, which base their explanation on within-person changes only (see e.g. Andreß et al., Reference Andreß, Golsch and Schmidt2013). Countries, as well as individual variables which do not change over time, are thus fixed in my models. However, I incorporate information at the macro-level using time-varying variables. It is thus important to note that my macro-level variables do not reflect differences between countries but within countries over time. In order to find out whether these changes in contextual characteristics influence the likelihood of volunteering differently for different groups of (non-)care-givers, I include interaction terms between care-giving at the individual level and my macro-level indicators.
Although this approach limits the analysis to within-person changes over time, i consider it most suitable in order to address the issue of unobserved heterogeneity. An alternative modelling strategy would be random-effect multi-level models which take into account the clustered nature of the data (three levels: countries, individuals, time). Since the data are restricted at the macro level to a non-random selection of 13 European countries, which excludes countries of the liberal welfare state type, such as Great Britain or Ireland, I do not consider it appropriate to use multi-level random-effect models to calculate and identify country differences in the effect of care-giving on volunteering (for a discussion of this methodological argument, see Bryan and Jenkins, Reference Bryan and Jenkins2016).
Descriptive findings
Confirming previous studies, I find important differences between countries regarding the share of volunteers and care-givers inside and outside their own household in the 50+ population (Figure 1).

Figure 1. Share of volunteers and care-givers among 50+ population by country (%).
Note: hh: household.
Across countries, participation in volunteering ranges from very high participation rates, especially in Northern European countries (such as 34% in the Netherlands and 29% in Denmark) but also in Switzerland (28%) to countries with low volunteering participation, especially Southern and Eastern European countries (such as 5% in Spain, 7% in the Czech Republic and 8% in Estonia). When differentiating between intensive and sporadic help/care-giving outside one's own household, we see that Scandinavians are much more involved in sporadic help/care-giving (Denmark 28%, Sweden 24%) than Southern and Eastern Europeans (Italy 7%, Slovenia 6%, Spain 4%). As to intensive help/care-giving, we observe especially high participation rates in Belgium (21%), the Czech Republic (16%) and Germany (15%). Regarding care-giving inside the individual's own household, we see the highest participation rates in Southern and Eastern European countries, like Spain (8%), Estonia and Italy (both 6%) or the Czech Republic (5%). The rates for informal care-giving inside one's household are lowest in Northern European countries, such as Sweden, Denmark, but also in Switzerland (all about 2%). This supports earlier studies showing that sporadic support for parents is especially widespread in Northern European countries while intensive support for parents is more common in familialistic countries in Southern and Central Europe (Schmid et al., Reference Schmid, Brandt and Haberkern2012). This probably has to do with different household constellations: since it is much more common in Eastern European and Southern European countries for adults to live in the same household as their parents (in-law) (Isengard and Szydlik, Reference Isengard and Szydlik2012), care-giving inside the individual's own household is not restricted to partner care but more often also involves care-giving for parents (in-law).
As to my research question under which circumstances care-givers in their second half of life are additionally involved in volunteering, we see large country differences (see Figure 2).
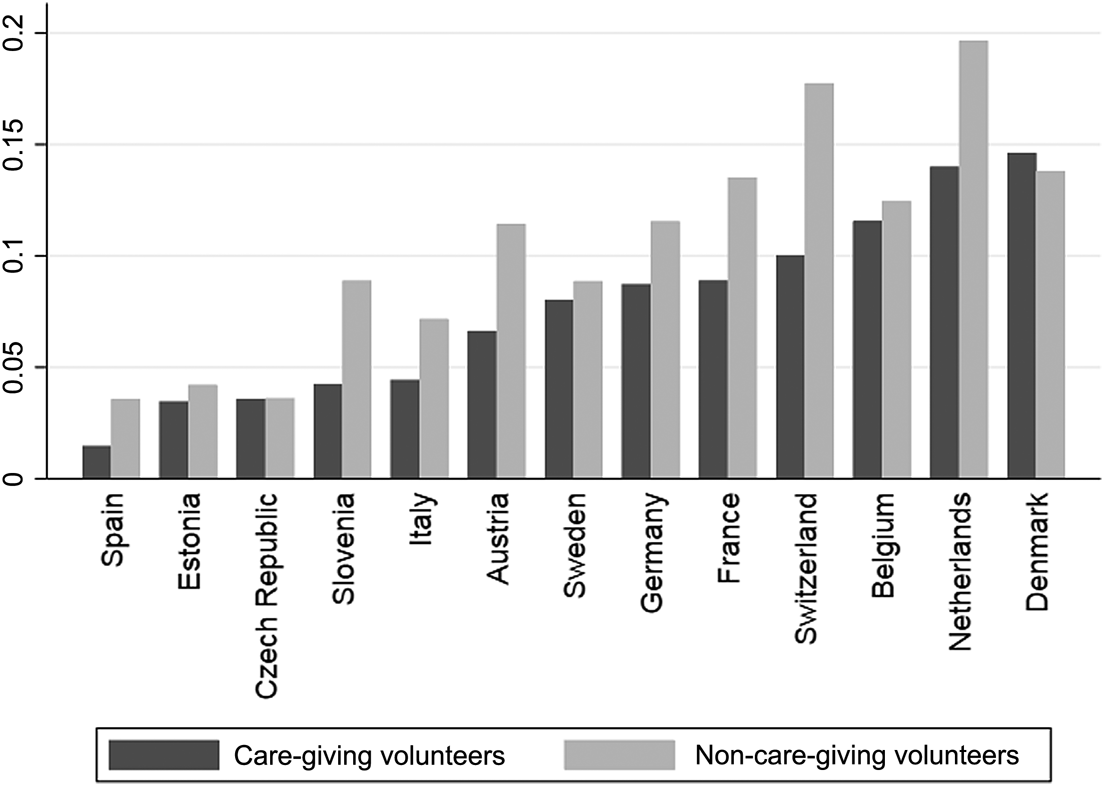
Figure 2. Share of care-giving and non-care-giving volunteers among 50+ population by country (%).
While in most countries (with the exception of Slovenia), care-givers are more involved in volunteering than non-care-givers, differences between the two groups are very small in some countries, like Switzerland or Italy, while care-givers are much more involved in volunteering in other countries, like the Netherlands, Denmark, Belgium or Sweden, than non-care-givers. This high involvement of care-givers in volunteering could have to do with the on average lower care-giving intensity in Northern European countries (Schmid et al., Reference Schmid, Brandt and Haberkern2012) which might leave more room for formal volunteering in the public sphere.
Multivariate results
The results of the multivariate analysis, which aims to assess my theoretical expectations, are presented in Table 2, depicting odds ratios and standard errors in parentheses.
Table 2. Conditional fixed-effect logistic regressions on likelihood of volunteering
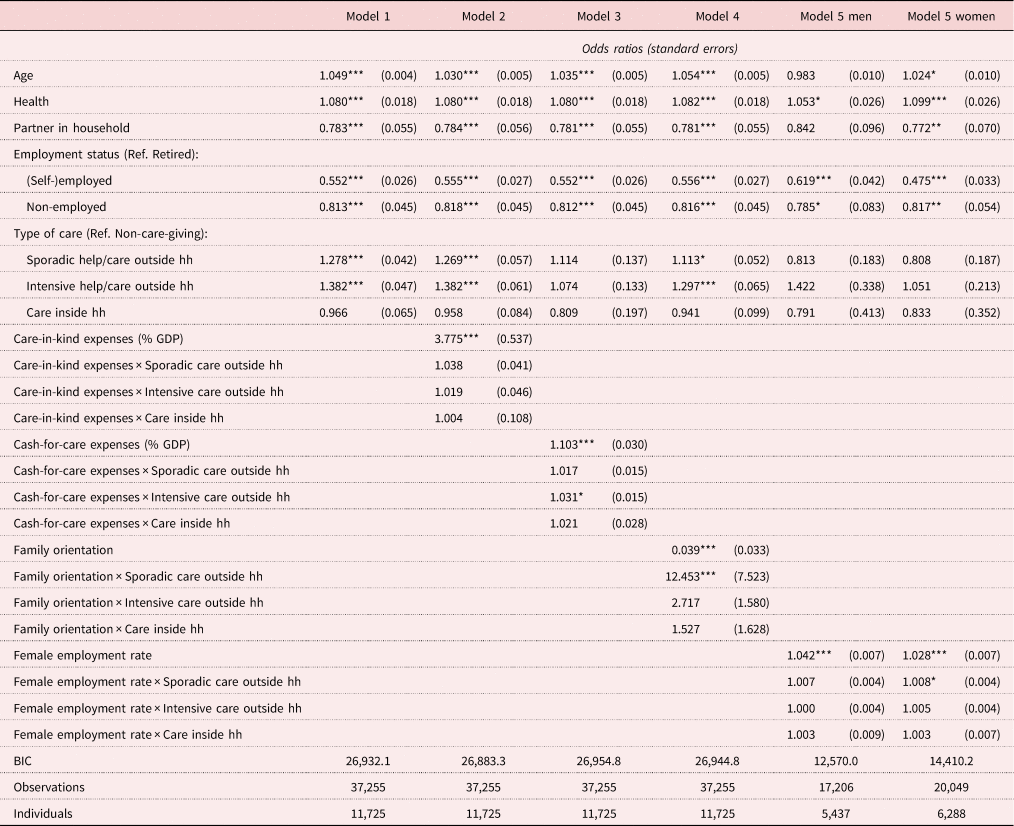
Notes: Fixed-effect regression models. Respondents aged between 50 and 80 years old. Ref.: reference category. hh: household. GDP: Gross Domestic Product. BIC: Bayesian information criterion.
Source: Survey of Health, Ageing and Retirement in Europe (SHARE), release 6.0.0, Waves 1, 2, 4, 5 and 6; Eurostat; OECD Statistics.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
Other than expected, intensive care-giving outside the individual's own household is positively related to volunteering; for care-giving inside their own household I find, however, no significant relationship with volunteering. My theoretical assumption of a negative effect of intensive help/care-giving outside the individual's own household and help/care-giving inside their own household on volunteering can thus not be confirmed. Regarding sporadic help/care-giving outside the individual's own household, I find, as expected, a significant positive effect and therefore can confirm my theoretical assumption. This finding supports earlier research which has also shown a close link between care-giving and volunteering (Burr et al., Reference Burr, Choi, Mutchler and Caro2005; Erlinghagen and Hank, Reference Erlinghagen and Hank2006; Choi et al., Reference Choi, Burr, Mutchler and Caro2007; Hank and Stuck, Reference Hank and Stuck2008). I can show that this relationship, however, only holds for (sporadic, as expected, but also intensive) help/care-giving outside the individual's own household. Moreover, my analysis is the first to show the effect of care-giving on volunteering using fixed-effect regression models. Earlier research could not be sure whether a time-constant factor, such as a person's tendency to help others, is the reason for his or her participation in informal care-giving and volunteering. Since my analytic strategy circumvents this problem by analysing within-person variance only, I have much more confidence in my conclusion that care-giving outside the household encourages participation in volunteering.
At the macro level, I find several factors that influence the relationship between care-giving and volunteering. A strong effect is found for care-in-kind welfare state expenses, which I expected to create a supportive infrastructure and networks that promote volunteering. Each percentage point increase in care-in-kind expenditure increases the odds of non-care-givers of volunteering by about 280 per cent (Model 2, odds: 3.775 ≈ 3.8). Although the effect is larger among care-givers than among non-care-givers, the interaction effects are not significant which is why I cannot confirm my theoretical assumption that care-in-kind welfare expenses increase the likelihood of care-givers volunteering to a higher degree than non-care-givers. Generally, however, the findings support my idea that care-in-kind expenses seem to provide a supportive infrastructure promoting volunteering. Regarding cash-for-care schemes, I find that they have a positive influence on those who give intensive care outside their own household, which confirms my theoretical assumption; other than expected I find, however, also a positive effect for non-care-givers. Each percentage point increase in cash-for-care expenditure increases the odds of intensive care-givers outside their own household of volunteering by 14 per cent (Model 3, odds: 1.103 × 1.031 ≈ 1.14) and of non-care-givers by about 10 per cent (odds: 1.103). Generally, I therefore cannot confirm my assumption that care-in-kind expenditures – by providing professional home-care support – unburden especially informal care-givers and thus enable them to volunteer additionally in the public sphere. Instead, care-in-kind expenses seem to generally create a supportive infrastructure for volunteering which serves not only care-givers but the entire population. As to cash-for-care expenses, they seem to serve especially those who give intensive care outside their own households and enable them – despite their heavy burden – to participate additionally in formal volunteering.
Confirming my theoretical assumption, I find a negative effect of family orientation, measured as the share of middle-aged adults in a country who live with at least one parent in the same household or building, on care-givers’ likelihood of volunteering; this effect, however, only holds for those who give sporadic help/care outside their own household. For those who give intensive help/care outside their household or help/care inside their household, the effects are also positive but not significant. However, against expectations, this effect of family orientation on care-givers also holds for non-care-givers. The effect is about 51 per cent for those who give sporadic care outside their households (odds: 0.039 × 12.453 = 0.486; 1 − 0.486 ≈ 0.51) and 96 per cent for non-care-givers (odds: 0.039; 1 − 0.039 ≈ 0.96). We thus see that family orientation is actually especially harmful for non-care-givers’ likelihood of volunteering while it has a little smaller but still substantial negative effect on sporadic care-givers. Intensive care-givers outside their own household and those who care inside their own household do not differ significantly from non-care-givers, i.e. their likelihood of volunteering is lowered to a similar degree as for non-care-givers.
Moreover, as expected theoretically, I find a significant effect of the employment rate of middle-aged women on the likelihood for volunteering for those women who give sporadic help/care outside their household. However, the effect can also be observed for men and women who do not provide informal care inside or outside their household. For women, however, i find a stronger effect for those who provide sporadic help/care outside their own household. Although the effect looks small (odds: 1.028 for non-care-giving women, 1.028 × 1.008 ≈ 1.04 for women providing sporadic help/care outside their household), when looking at a change of 10 percentage points in female employment in this age group, which about describes the difference between Germany and Estonia, i find that the odds of volunteering (versus non-volunteering) increases for (sporadically) care-giving women by 48 per cent (1.028 × 1.008 ≈ 1.04; 1.0410 = 1.48) and for non-care-giving women by 32 per cent (1.02810 = 1.32).
Discussion
In this article, I have focused attention on the linkage between two unpaid activities, one of which – formal volunteering – takes place in the public realm, while the other – informal care-giving – mainly takes place in the private realm of the family. The possibility for care-givers to participate additionally in volunteering might be important in order to enlarge their social networks from bonding connections among family members to social linking connections with other volunteers which might not only provide a sense of belonging but also be the source of social support (Lin et al., Reference Lin, Ye and Ensel1999). Moreover, additional volunteering might also improve informal care-givers’ state of health (Rozario et al., Reference Rozario, Morrow-Howell and Hinterlong2004). My findings confirm previous research, but also yield new insights. With regard to the former, I confirm that informal care-givers are more involved in volunteering than non-care-givers, even when controlling for unobserved heterogeneity by only analysing within-person changes over time. I thus conclude that it is not time-constant personality characteristics which increase the likelihood of care-giving and volunteering at the same time, as discussions around ‘super helpers’ or ‘doers’ suggest (see Burr et al., Reference Burr, Choi, Mutchler and Caro2005: S255; Jegermalm and Jeppson-Grassman, Reference Jegermalm and Jeppson-Grassman2009: 366). Rather, care-giving itself seems to indeed increase the opportunity of volunteering. This, however, only holds true for individuals providing care outside their households, be it sporadically or intensively. This finding is plausible in the light of previous research which has shown that a decrease in the share of family members in the social network increases the likelihood of volunteering participation (Ajrouch et al., Reference Ajrouch, Antonucci and Webster2016). Since care-giving inside an individual's own household mostly involves partner care that is frequently done without additional formal or informal support (Bertogg and Strauß, Reference Bertogg and Strauß2020), this type of care does not seem to have the same positive effect on volunteering as care-giving outside the household.
At the macro level, I find several factors that influence the relationship between care-giving and volunteering. A strong effect is found for care-in-kind welfare state expenses, which are thought to create a supportive infrastructure and networks that promote volunteering, not only among the care-giving population, as expected, but rather in the general population. Moreover, cash-for-care expenditures increase the likelihood of volunteering for those who care intensively outside their own household; non-care-givers’ likelihood of volunteering is, however, also increased by cash-for-care expenditures. For care-givers, it seems plausible that financial transfers unburden them from the need to participate in the labour market which leaves them with more time for unpaid volunteering. The finding that cash-for-care expenditures also increase the likelihood for volunteering in the general population supports the general previous finding that public social spending increases the likelihood for volunteering, the exact mechanisms for the non-care-giving population, however, remains unclear.
In addition, I also find significant effects regarding the role of family and women in a given society. First, I show that family orientation reduces the likelihood of volunteering. The effect is even stronger for non-care-givers than for sporadic care-givers (outside their household). This is interesting insofar as i find at the micro level that care-giving (outside the individual's own household), which is usually provided to family members (i.e. takes place in the private realm), does not hinder volunteering in the public realm; on the contrary, it even encourages it. At the societal level, however, a stronger family orientation weakens this effect to some degree. At the same time, I find that in societies with a strong emphasis on middle-aged women's labour market participation, the positive effect of care-giving on volunteering is even stronger for women. Again, I find this effect not only for those women who care sporadically outside their own household but also for non-care-giving men and women. It thus seems that a public role for women in the sense of continuous employment participation has the positive effect that middle-aged women do not reduce their activities to only those taking place in the private sphere, such as care-giving activities for relatives, but also stay engaged in the public, namely as volunteers in clubs or associations.
My study comes with a number of limitations. To begin with, the measurement of volunteering available in the SHARE data unfortunately does not allow for differentiating between volunteering in different types of organisations. The type of organisation in which care-givers volunteer could, however, give further interesting insights into the motives for engaging in the public sphere. For instance, if care-giving mainly increases volunteering in care-related organisations, this would support the idea that social networks are the explanatory mechanism, whereas an increase in non-care-related organisations would rather support the idea that volunteering is used as an escape from their straining engagement in the family.
Regarding the measurement of care-giving, this study is also restricted. Only for care-giving outside the household can I differentiate between sporadic and intensive help/care-giving. In order to circumvent biases related to country differences in the share of adults who live together with at least one of their parents, I decided not to limit my analysis to care outside the household but to include care-giving inside an individual's own household as a separate category. Moreover, I cannot differentiate for all waves between informal help, i.e. support with IADLs, such as cooking, shopping or cleaning, and informal care-giving, i.e. support with ADLs, such as washing, feeding or dressing, which is why I had to collapse both activities. I hope, however, that my differentiation between high- and low-intensity care-givers (outside their own household) captures much of this effect.
Having these limitations in mind, I am still convinced that my analysis takes us a step further in understanding the relationship between formal volunteering and informal care-giving for middle-aged adults in a country-comparative context. Moreover, it yields important insights for policy makers in times of population ageing who aim to encourage multiple engagement of the middle-aged in the private and the public sphere. The most important finding in this respect is that I can confirm the well-known finding that welfare expenses, be it care-in-kind or cash-for-care, ‘crowd in’ private engagement. For cash-for-care expenses, I also find that they increase the positive effect of (intensive) care-giving (outside the individual's own household) on volunteering. Additionally, fostering the public role of middle-aged women by encouraging their employment can increase the chance that women who are engaged in informal care-giving in the private sphere of the family will additionally contribute in the public sphere by being involved in volunteering activities.
Data
This paper uses data from SHARE Waves 1, 2, 4, 5 and 6 (DOIs: 10.6103/SHARE.w1.611, 10.6103/SHARE.w2.611, 10.6103/SHARE.w4.611, 10.6103/SHARE.w5.611 and 10.6103/SHARE.w6.611). The SHARE data collection has been primarily funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812) and FP7 (SHARE-PREP: No. 211909, SHARE-LEAP: No. 227822, SHARE M4: No. 261982). Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the US National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see www.share-project.org).
Acknowledgements
I would like to thank Ariane Bertogg for providing invaluable support with setting up the data for the project in general and commenting on an earlier version of this paper, as well as Maarten Buis for helping with the descriptive graphs. Moreover, I thank two anonymous reviewers and the editor for their helpful comments and suggestions.
Financial support
This work was supported by the German Research Foundation (DFG) (project number STR1322/2-1).
Ethical approval
Ethical approval was not required.
Appendix

Figure A1a. Development of care-in-kind expenditures by country over time (% of Gross Domestic Product (GDP)).
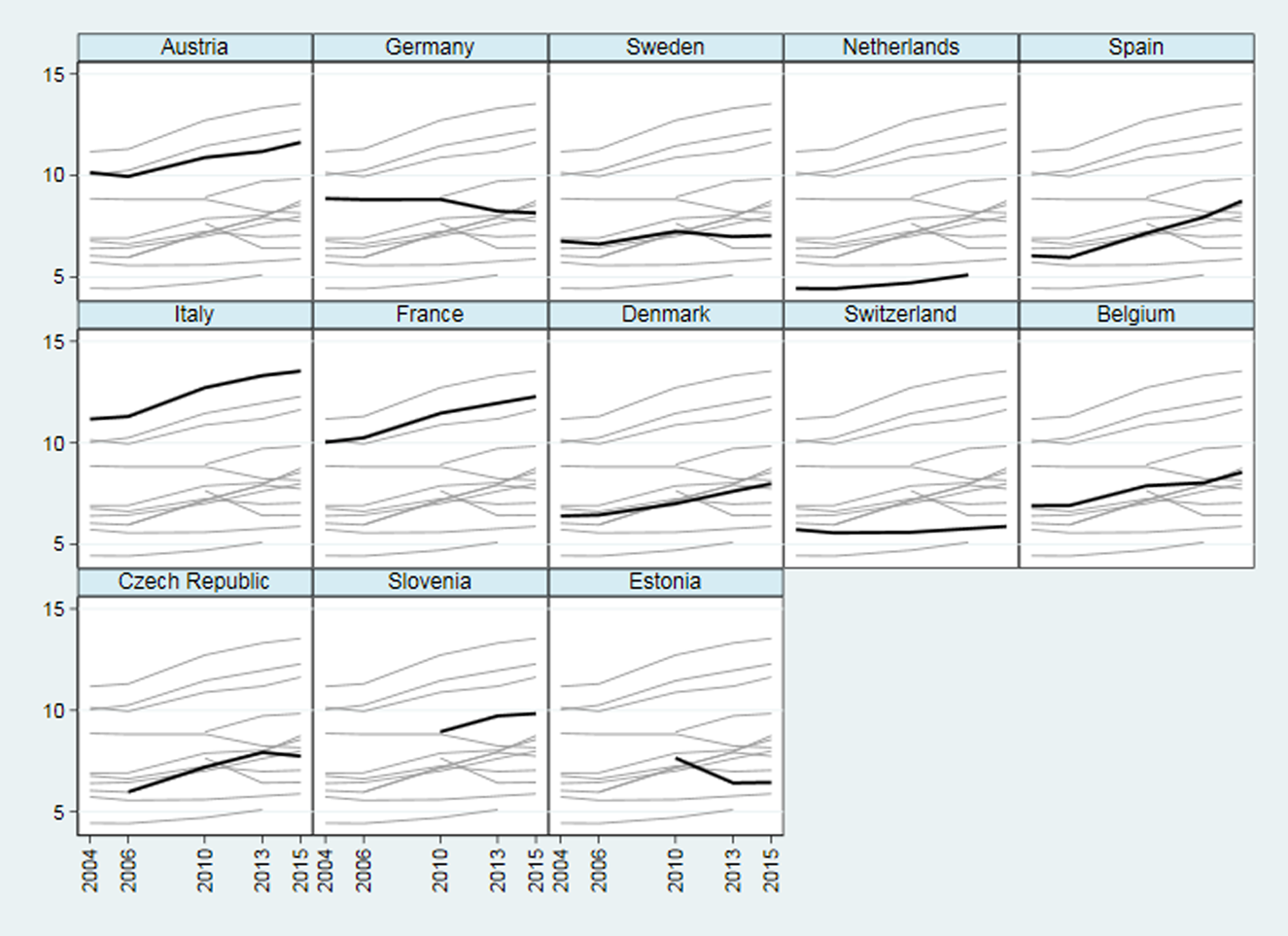
Figure A1b. Development of cash-for care expenditures by country over time (% GDP).

Figure A1c. Development of family norms by country over time (% adults living with at least one parent).
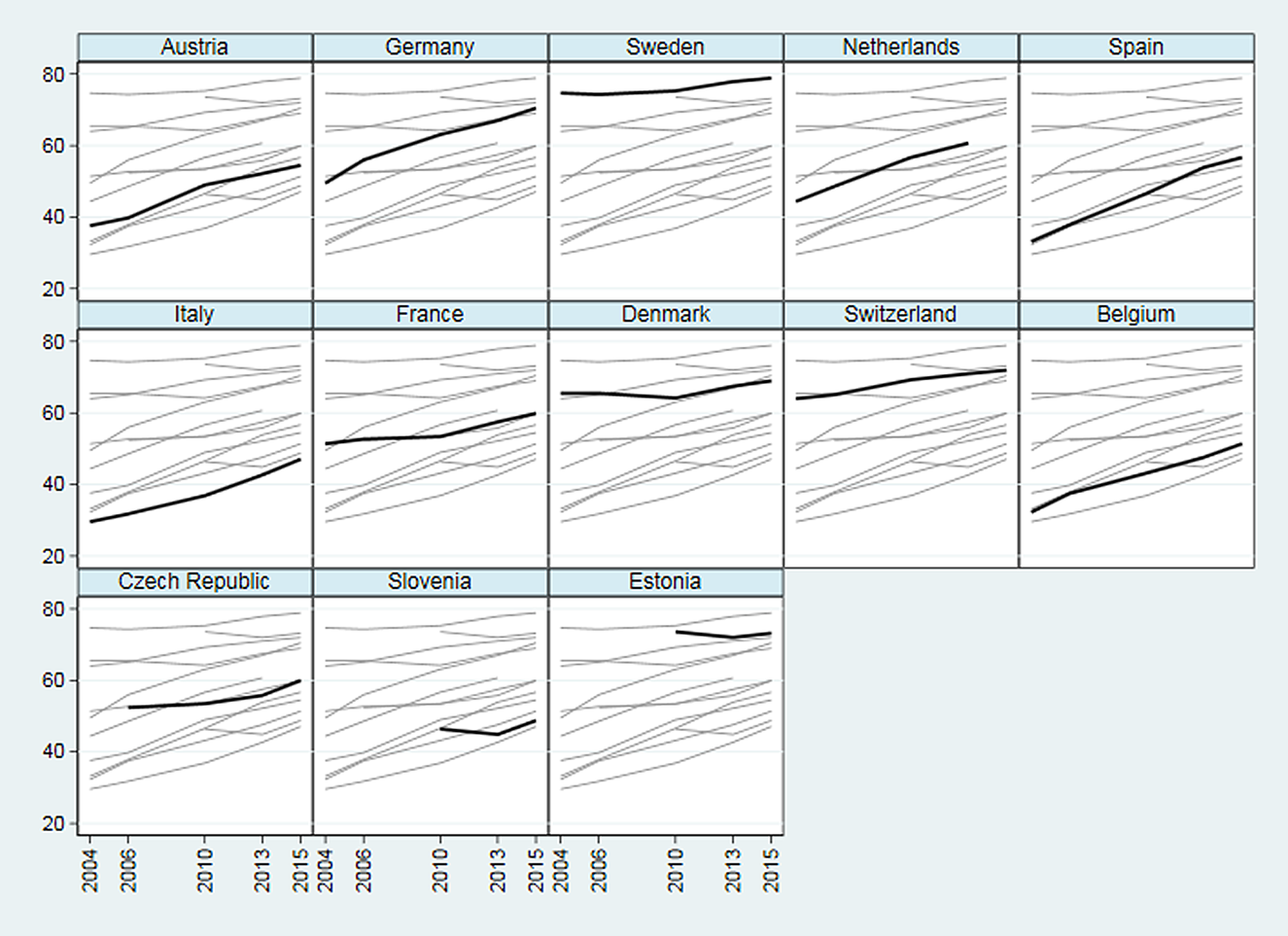
Figure A1d. Development employment rate of women aged 50–64 by county over time (%).









 Open access
Open access